

Abstract
Background
Domain-specific physical activities may have different correlates and health effects, but few large studies have examined these questions, especially their separate associations with adiposity.
Methods
We analysed cross-sectional data of 466 605 adults without any prior chronic diseases, enrolled during 2004–8, from 10 diverse localities across China. Physical activity level in each of 4 domains (occupation, commuting, household, and active-recreation), calculated as metabolic equivalent (MET)-hr/day, was related to social-demographic factors and measures of adiposity (body mass index [BMI], waist circumference [WC], and bio-impedance derived percentage body fat), using multivariable linear and logistic regression models.
Results
The overall mean age was 50.8 years. The mean total physical activity was 21.7 MET-hr/day, mainly from occupation (62%) and household chores (26%), but little from active-recreation (4%), with women having a much higher household activity than men. Older participants had a lower level of occupational activity but a higher level of household and active-recreational activity, particularly after retirement. There was no linear association of occupational activity with adiposity, but working women tended to have a lower adiposity (e.g. 1.0 cm WC) than non-working women. In men, there was an inverse and apparently linear association between adiposity and levels of both commuting-related and household activities, with 3 MET-hr/day associated with -0.11 and -0.13 kg/m2 BMI, -0.42 and -0.62 cm WC, and -0.28 and -0.33 percentage points of body fat, respectively. In women, only household activity showed a linear, but weaker, association with adiposity. A higher adiposity was observed among men and women with higher levels of active-recreational activity.
Conclusions
In Chinese adults, physical activity mainly involves occupation and housework, with little from active-recreational activity. Domain-specific physical activities varied by socio-demographic factors and had different associations with adiposity.
Electronic supplementary material
The online version of this article (doi:10.1186/1471-2458-14-826) contains supplementary material, which is available to authorized users.
Keywords: Physical activity, Domain, Obesity, China, Biobank
Background
The health benefits of physical activity have been well recognized [1]. However, studies to date have focused primarily on active-recreational activities, in spite of a large contribution to total physical activity level of occupational, household and commuting-related activities, particularly in low- and middle-income countries, such as China [2–4]. Activities from different domains may differ in their determinants [5–7] and knowledge about them could help to inform the development of effective physical activity interventions at a population level. Several studies have examined associations of physical activity from different domains with socio-demographic factors, but these were mainly in Western countries where people in general have an urban-industrial lifestyle. In China, although there has been a large shift from a labour-intensive lifestyle to a more sedentary lifestyle over the past few decades, patterns of physical activity still differ greatly from those in the Western countries, with, for example, higher participation in leisure-time and household activity among older people in China [8], contrasting that seen in most Western populations [6].
A higher level of physical activity has been deemed as beneficial for preventing weight gain and obesity. Question remains, however, about the separate associations of domain-specific physical activities with adiposity and other health-related outcomes. Several studies have attempted to address these issues but the findings were inconsistent, with some showing inverse association between commuting-related activity and adiposity in various populations including Chinese [9], South Asians [10], and Americans [11] whereas others showing no association [12], an inverse association [2, 13], or a positive association [14] between occupational activity and adiposity. Large-scale epidemiological studies comparing simultaneously the associations of physical activity from four major domains with measures of adiposity are still lacking.
To fill this evidence gap, we report the findings of a cross-sectional investigation using data from the China Kadoorie Biobank (CKB), a prospective observational study of over 500 000 adults recruited from 10 diverse areas in China [15, 16]. The aims of this report are: 1) to determine the socio-demographic correlates of physical activity from occupation, commuting, housework and active- recreation; 2) to investigate the associations of domain-specific activity with different measures of adiposity including body mass index (BMI), waist circumference (WC) and percentage body fat.
Methods
Study design and participants
Detailed information about the CKB study design, survey methods and participant characteristics has been reported previously [15, 16]. In brief, all permanent residents aged 35–74 years in 10 geographically defined areas (5 urban and 5 rural) of China, identified through public registry records, were eligible to take part in the study. The areas were selected so as to cover wide spectra of risk exposures and disease patterns, and for logistical convenience, but were not intended to be representative of China as a whole. The baseline survey was conducted between June 2004 and July 2008. Invitation letters and study information leaflets were delivered door-to-door by local community leaders and health workers following extensive publicity campaigns. About one in three of the eligible residents (33% rural, 27% urban) participated. To encourage participation, those few individuals aged 30–34 or 75–79 years were not turned away [16]. In total, 512 891 participants (210 222 men and nearly all Han Chinese) were enrolled in the CKB.
For the current analyses, we excluded those who had a history of heart disease (n = 15 472), stroke (n = 8884), tuberculosis (n = 7660), chronic obstructive pulmonary disease (n = 13 289), and/or cancer (n = 2577); those who answered all questions in the physical activity questionnaire with zero (n = 81); those who reported spending more than 20 hours daily on all waking activities (n = 813); and those who gave implausible or conflicting answers to occupational and commuting-related questions (e.g. who reported not working but had non-zero commuting-related physical activity) (n = 1418). After these exclusions, 466 605 participants remained in this cross-sectional analysis.
The study was approved by the ethics committees of the University of Oxford and the Chinese Center for Disease Control and Prevention (CDC). In addition, ethics approval was obtained from the institutional research board at the local CDC in each of the 10 areas. Written informed consent was obtained from all participants.
Data collection
The baseline data collection took place in temporary assessment clinics specially set up in the local communities for this study. An interviewer-administered computerised questionnaire was used to collect information on socio-demographic factors (e.g. education, annual household income, and occupation), lifestyle factors (e.g. smoking, drinking, diet and physical activity), and medical history.
Detailed information on physical activity questions and methods used to derive domain-specific physical activity levels, in metabolic equivalents (MET)-hr/day, have been reported previously [17]. In brief, questions about physical activity were adapted from validated questionnaires used in several other studies in Western [18] and Chinese populations [19], with some additional modifications following a CKB pilot study. To quantify the amount of physical activity, metabolic equivalents (METs) from the 2011 update of a major compendium of physical activities [20] were used. Occupational activity included all physical activities performed during paid employment; commuting-related activity was the physical activity performed during the journeys between home and work, without including the transportation for other purposes; household activity included activities spent on household chores; and active-recreational activity included activities spent on sports during leisure time, but not sedentary leisure-time activities (mainly TV viewing) [17].
Body weight, standing height, WC and body fat percentage were measured by trained health workers while participants wore light clothes and no shoes. Standing height was measured to the nearest 0.1 cm using a stadiometer, and WC was measured with a soft non-stretchable tape at midway between the lowest rib and the iliac crest, also to the nearest 0.1 cm. Weight and percentage body fat were estimated using a bioelectrical impedance device (TANITA-TBF-300GS, Tanita Corp., Tokyo, Japan). BMI was calculated as the weight in kilograms divided by the square of standing height in meters.
Statistical analyses
For each of the four domains of physical activity, participants were first divided into two groups: performing no such activity or some activity; and the proportions of participants with no activity by socio-demographic factors were estimated separately for men and women using logistic regression models, adjusting for age (in 5-year intervals) and study area, where appropriate. Among those who had some activity from a specific domain, multiple linear regression models were used to estimate the age- and area-adjusted mean levels of activity by socio-demographic factors.
The adjusted mean levels (and 95% CIs) of adiposity measures in 4 groups of each domain-specific physical activity (zero, low, moderate or high) were estimated using multiple linear regression models with adjustment for age, study area (10 study areas), education (no formal education, primary school, middle or high school, and college or university), annual household income (<10 000, 10 000–19 999, 20 000–34 999, and ≥35 000 yuan), sedentary leisure time (hr/day), smoking (never, ex-regular, occasional and current smokers), alcohol intake (never, ex-regular, occasional and current drinkers) and other domain-specific activities (MET-hr/day). Analyses were performed separately for men and women and, if an approximately linear association was observed, differences in adiposity per 3 MET-hr/day of domain-specific physical activity were also examined using multiple linear regression with heterogeneity assessed by χ2 statistics, P values from Cochran Q tests, and I2 statistics (i.e. the variation in pooled estimates accounted for by heterogeneity rather than by chance) [21]. All statistical analyses were conducted using SAS 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Of the 466 605 participants included, the mean baseline age was 50.8 years, 40.4% were men, and 42.5% came from urban areas. Occupational activity was the largest domain, accounting for 76% and 52% of total physical activity in men and women respectively, and active-recreational activity was the smallest, accounting for less than 4% of total physical activity in both sexes. Nearly all women but only about 79% of men engaged in household work with the mean activity level in women being more than 2.5 times as high as in men (7.7 vs. 2.9 MET-hr/day). Women had higher mean percentage body fat (32% vs. 22%), higher mean BMI (23.8 vs. 23.4 kg/m2), but lower mean WC (78.8 vs. 81.9 cm) than men (Table 1).
Table 1.
Main characteristics of study participants
| Characteristics | Men (n =188 647) | Women (n = 277 958) | Total (n =188 647) |
|---|---|---|---|
| Age (years), % | |||
| 30 – 39 | 15.2 | 16.9 | 16.2 |
| 40 – 49 | 30.0 | 32.2 | 31.3 |
| 50 – 59 | 30.6 | 30.8 | 30.7 |
| 60 – 69 | 17.8 | 15.2 | 16.2 |
| 70 – 79 | 6.5 | 4.8 | 5.5 |
| Mean (SD) | 51.5 (10.7) | 50.3 (10.3) | 50.8 (10.5) |
| Residence, % | |||
| Urban | 42.6 | 43.3 | 43.0 |
| Rural | 57.4 | 56.7 | 57.0 |
| Occupational physical activity (MET-hr/day), % | |||
| 0 | 18.1 | 34.7 | 28.0 |
| 0.1– 10 | 18.0 | 20.7 | 19.6 |
| 10.1 – 20 | 25.5 | 23.1 | 24.1 |
| > 20 | 38.4 | 21.5 | 28.3 |
| Mean (SD) | 17.3 (14.9) | 10.9 (12.5) | 13.5 (13.9) |
| Commuting-related physical activity (MET-hr/day), % | |||
| 0 | 31.4 | 47.3 | 40.9 |
| 0.1 – 1.5 | 23.5 | 17.9 | 20.1 |
| 1.6 – 3.0 | 26.0 | 20.2 | 22.6 |
| > 3.0 | 19.1 | 14.6 | 16.4 |
| Mean (SD) | 1.9 (2.4) | 1.4 (2.2) | 1.6 (2.3) |
| Household physical activity (MET-hr/day) | |||
| 0 | 21.0 | 0.7 | 8.9 |
| 0.1 – 4.0 | 54.5 | 15.8 | 31.4 |
| 4.1 – 8.0 | 17.4 | 31.8 | 26.0 |
| > 8.0 | 7.0 | 51.8 | 33.7 |
| Mean (SD) | 2.9 (2.8) | 7.7 (3.9) | 5.7 (4.2) |
| Active-recreational physical activity (MET-hr/day), % | |||
| 0 | 79.0 | 80.4 | 79.8 |
| 0.1 – 2.0 | 6.9 | 5.8 | 6.2 |
| 2.0 – 4.0 | 6.8 | 6.5 | 6.7 |
| > 4.0 | 7.2 | 7.3 | 7.3 |
| Mean (SD) | 0.8 (2.2) | 0.8 (2.2) | 0.8 (2.2) |
| Total physical activity (MET-hr/day) | 22.8 (15.1) | 20.9 (12.8) | 21.7 (13.8) |
| Sedentary leisure time (hr/day) | 3.1 (1.5) | 2.9 (1.5) | 3.0 (1.5) |
| Body mass index (kg/m2)1 | 23.4 (3.2) | 23.8 (3.4) | 23.6 (3.3) |
| Waist circumference (cm) | 81.9 (9.7) | 78.8 (9.4) | 80.1 (9.6) |
| Percentage body fat (%)2 | 22.0 (6.2) | 32.0 (7.1) | 28.0 (8.3) |
SD: standard deviation.
12 participants with missing values.
2214 participants with missing values.
In both sexes, age was strongly and inversely associated with proportion of having and the mean levels of occupational activity. Due to retirement, the proportion of non-working people increased dramatically at 60–69 years for men (from 12.5% at 50–59 years to 49.3%) and 50–59 years for women (from 13.4% at 40–49 years to 45.6%). At the same time, mean levels of occupational activity, among those still working, greatly decreased (Table 2). An opposite trend was observed for active-recreational activity; those aged 70–79 years were ~3.6 times more likely to perform regular physical exercise than those aged 30–39 years. Their mean level of exercise was also higher than those younger than 60 years (for men) or 50 years (for women).
Table 2.
Levels of domain-specific physical activity by age and area 1
| Characteristics | n | Physical activity | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Occupational | Commuting-related | Household | Active-recreational | ||||||
| % no activity | Mean MET-hr/day (SD) 2 | % no activity 3 | Mean MET-hr/day (SD) 2 | % no activity | Mean MET-hr/day (SD) 2 | % no activity | Mean MET-hr/day (SD) 2 | ||
| Men | |||||||||
| Age, years | |||||||||
| 30 – 39 | 28 694 | 1.7 | 23.6 (12.8) | 17.8 | 2.5 (2.2) | 24.0 | 2.9 (2.6) | 88.4 | 3.1 (3.2) |
| 40 – 49 | 56 513 | 2.9 | 23.1 (12.8) | 16.7 | 2.6 (2.2) | 22.8 | 3.2 (2.6) | 87.5 | 3.2 (3.2) |
| 50 – 59 | 57 721 | 12.5 | 20.9 (12.8) | 15.2 | 2.9 (2.1) | 20.9 | 3.7 (2.6) | 79.7 | 3.9 (3.2) |
| 60 – 69 | 33 512 | 49.3 | 15.2 (12.9) | 15.6 | 2.8 (2.2) | 16.9 | 4.3 (2.6) | 62.7 | 4.5 (3.2) |
| 70 – 79 | 12 207 | 68.1 | 10.3 (12.8) | 16.4 | 2.6 (2.2) | 17.5 | 4.3 (2.6) | 58.1 | 4.4 (3.2) |
| Region | |||||||||
| Rural | 108 347 | 4.8 | 21.5 (13.6) | 19.4 | 2.9 (2.5) | 23.7 | 3.8 (2.6) | 91.9 | 2.7 (3.2) |
| Urban | 80 300 | 36.1 | 20.4 (13.7) | 10.5 | 2.4 (2.5) | 17.4 | 3.4 (2.6) | 61.4 | 4.3 (3.2) |
| Women | |||||||||
| Age, years | |||||||||
| 30 – 39 | 47 033 | 9.0 | 18.4 (10.3) | 19.4 | 2.6 (1.9) | 1.1 | 6.8 (3.6) | 90.5 | 3.0 (3.1) |
| 40 – 49 | 89 625 | 13.4 | 18.4 (10.3) | 19.1 | 2.8 (1.9) | 0.7 | 7.1 (3.6) | 87.2 | 3.6 (3.1) |
| 50 – 59 | 85 692 | 45.6 | 14.8 (10.3) | 18.9 | 2.8 (1.9) | 0.4 | 8.7 (3.6) | 76.6 | 4.5 (3.1) |
| 60 – 69 | 42 206 | 70.1 | 11.7 (10.3) | 21.2 | 2.7 (1.9) | 0.6 | 8.4 (3.6) | 66.2 | 4.3 (3.1) |
| 70 – 79 | 13 402 | 85.8 | 8.0 (10.2) | 21.3 | 2.6 (1.9) | 1.7 | 7.6 (3.6) | 68.4 | 4.0 (3.1) |
| Region | |||||||||
| Rural | 157 557 | 17.1 | 15.8 (11.7) | 21.7 | 2.9 (2.4) | 0.5 | 8.4 (3.7) | 93.9 | 2.8 (3.1) |
| Urban | 120 401 | 57.7 | 18.8 (11.8) | 13.8 | 2.5 (2.4) | 0.9 | 7.0 (3.7) | 62.7 | 4.4 (3.1) |
1Values were adjusted for age and study area (where appropriate). All P for heterogeneity across subgroups < 0.0001 for all.
2Least square means (standard deviations) among those participants who have that domain-specific physical activity.
3The proportion was calculated among working people only.
Compared with rural participants, urban participants were more likely to participate in all three non-occupational activities and had a higher mean level of active-recreational activity, but lower mean levels of commuting-related and household activity. On the other hand, mean level of occupational activity was higher in rural men and urban women as compared to their corresponding counterparts. Rural farmers do not have to retire at certain ages, therefore there was a much smaller proportion of non-working people in rural than in urban areas (Table 2). Across the 10 study areas, overall mean level of occupational activity was the highest in Zhejiang (a rural costal area) in both men and women, and the lowest in men from Haikou (an urban tropical area) and women from Henan (a rural inland area). Commuting-related activity was much higher in Gansu, a rural inland area in the west of China, than in other areas. With regard to mean level of household activity, the highest was found in women from Gansu and the lowest was in men from Henan (Additional file 1: Figure S1).
Factory workers had the highest mean level of occupational activity (25.9 MET-hr/day in men and 24.1 in women), followed by sales & self-employed (21.6 in men and 21.7 in women) (Table 3). Although mean level of commuting-related activity did not vary greatly across different occupations (2.1-2.9 MET-hr/day), proportion of non-commuting sales & self-employed was 9 times (in men) or 21 times (in women) as high as that of non-commuting farmers, and 3 times (in both men and women) as high as non-commuting factory workers. The mean levels of household and active-recreational activity were the highest in those not in paid occupation, including those retired and unemployed individuals and home makers. They also had a higher tendency to perform active-recreational activity, i.e. lower proportion of no such activity. For both men and women, sales & self-employed group had the lowest rate of household activity participating. In both sexes, education was associated inversely with mean levels of occupational, commuting-related and household activity but positively with proportion engaged in active-recreational activity. A lower proportion of non-working people was observed among those with a college or university education, particularly in women. A higher level of education was associated with a lower mean level of household activity, a higher proportion of men but lower proportion of women participating in household tasks. People with college or university education were 4 times more likely to perform regular physical exercise than those with no formal education. Household income was also positively, though to a lesser extent compared with education, associated with proportion of participating in active-recreational activity. However, no clear linear association of either education or household income with mean level active-recreational activity was observed. P values for heterogeneity for all of these associations were <0.0001 (Table 3).
Table 3.
Levels of domain-specific physical activity by socioeconomic factors 1
| Characteristics | n | Physical activity | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Occupational | Commuting-related | Household | Active-recreational | ||||||
| % no activity | Mean MET-hr/day (SD) 2 | % no activity 3 | Mean MET-hr/day (SD) 2 | % no activity | Mean MET-hr/day (SD) 2 | % no activity | Mean MET-hr/day (SD) 2 | ||
| Men | |||||||||
| Occupation | |||||||||
| Farmer | 84 124 | 1.6 | 19.6 (16.4) | 5.7 | 2.9 (2.9) | 20.7 | 3.6 (3.3) | 90.3 | 3.3 (4.5) |
| Factory worker | 38 389 | 0 | 25.9 (16.1) | 16.9 | 2.6 (2.8) | 19.0 | 3.3 (3.1) | 79.3 | 3.2 (3.7) |
| Sales & others4 | 19 450 | 0 | 21.6 (13.6) | 52.4 | 2.6 (2.3) | 28.2 | 3.2 (2.7) | 76.0 | 3.4 (3.3) |
| Professionals | 13 839 | 0 | 16.4 (13.7) | 27.2 | 2.1 (2.4) | 21.5 | 3.1 (2.7) | 61.5 | 3.4 (3.4) |
| Retired & others5 | 32 845 | 100 | - | - | - | 19.6 | 4.4 (3.1) | 58.7 | 4.6 (3.8) |
| Highest education | |||||||||
| No formal education | 16 387 | 11.4 | 22.5 (14.2) | 11.8 | 3.1 (2.4) | 22.2 | 3.8 (2.8) | 91.1 | 3.8 (3.3) |
| Primary school | 62 101 | 15.7 | 22.2 (14.0) | 14.4 | 2.9 (2.4) | 20.9 | 3.8 (2.8) | 85.7 | 3.8 (3.4) |
| Middle or high school | 95 869 | 21.6 | 21.0 (13.7) | 17.9 | 2.6 (2.3) | 21.0 | 3.5 (2.7) | 75.5 | 4.0 (3.2) |
| College or university | 14 290 | 13.0 | 14.8 (13.9) | 19.0 | 2.2 (2.4) | 19.8 | 3.2 (2.8) | 59.0 | 3.9 (3.3) |
| Annual household income (yuan) | |||||||||
| <10 000 | 48 718 | 20.0 | 21.8 (15.3) | 13.2 | 3.0 (2.6) | 18.1 | 4.0 (3.0) | 86.7 | 3.8 (3.4) |
| 10 000–19 999 | 53 248 | 21.3 | 22.3 (13.0) | 15.0 | 2.8 (2.2) | 21.6 | 3.7 (2.6) | 80.4 | 4.0 (3.2) |
| 20 000–34 999 | 48 151 | 16.3 | 21.4 (13.6) | 15.6 | 2.6 (2.3) | 21.0 | 3.5 (2.7) | 77.1 | 3.9 (3.2) |
| ≥35 000 | 38 530 | 13.6 | 18.6 (14.1) | 22.5 | 2.3 (2.4) | 23.9 | 3.2 (2.8) | 69.5 | 3.9 (3.3)6 |
| Women | |||||||||
| Occupation | |||||||||
| Farmer | 116 776 | 2.2 | 13.8 (12.5) | 3.6 | 2.8 (2.5) | 0.2 | 8.0 (4.4) | 92.3 | 3.4 (4.6) |
| Factory worker | 31 190 | 0 | 24.1 (12.2) | 25.1 | 2.7 (2.4) | 1.3 | 5.4 (3.9) | 83.4 | 3.1 (3.4) |
| Sales & others4 | 24 826 | 0 | 21.7 (11.6) | 74.3 | 2.8 (2.2) | 2.3 | 5.9 (3.7) | 83.4 | 3.2 (3.2) |
| Professionals | 11 304 | 0 | 15.0 (11.1) | 41.6 | 2.5 (2.2) | 1.6 | 5.5 (3.6) | 67.8 | 3.2 (3.3) |
| Retired & others5 | 93 862 | 100 | - | - | - | 0.5 | 9.1 (4.1) | 65.4 | 4.5 (3.4) |
| Highest education | |||||||||
| No formal education | 70 147 | 27.8 | 16.5 (12.5) | 18.2 | 3.0 (2.4) | 0.6 | 8.1 (4.4) | 90.7 | 3.7 (3.5) |
| Primary school | 87 196 | 35.2 | 17.4 (10.7) | 19.3 | 2.8 (2.0) | 0.6 | 7.9 (3.8) | 84.7 | 4.0 (3.3) |
| Middle or high school | 108 625 | 40.9 | 17.1 (11.7) | 20.2 | 2.6 (2.2) | 0.7 | 7.6 (4.1) | 72.4 | 4.3 (3.3) |
| College or university | 11 990 | 14.2 | 11.4 (11.4) | 18.3 | 2.3 (2.2) | 1.1 | 6.4 (3.9) | 61.8 | 3.9 (3.2)6 |
| Annual household income (yuan) | |||||||||
| <10 000 | 82 776 | 32.5 | 16.5 (12.3) | 19.8 | 2.8 (2.4) | 0.5 | 7.7 (4.2) | 86.6 | 4.0 (3.3) |
| 10 000–19 999 | 81 908 | 37.2 | 17.1 (10.4) | 17.7 | 2.8 (1.9) | 0.6 | 7.9 (3.7) | 81.8 | 4.1 (3.1) |
| 20 000–34 999 | 67 527 | 33.6 | 17.3 (11.3) | 17.0 | 2.7 (2.1) | 0.7 | 7.7 (3.8) | 78.1 | 4.1 (3.1) |
| ≥35 000 | 45 747 | 35.7 | 15.7 (11.3) | 24.4 | 2.5 (2.1) | 1.1 | 7.7 (3.9)6 | 70.3 | 4.1 (3.2)6 |
1Values were adjusted for age and study area, P for heterogeneity < 0.0001 for all domain-specific physical activities.
2Least square means (standard deviations) among those participants who have that domain-specific physical activity.
3The proportion was calculated among working people only.
4Including sales, self-employed and people in other un-specified occupations.
5Including those retired, un-employed and home makers.
6 P for trend across subgroups > 0.05, all other P < 0.0001.
Occupational activity was not linearly associated with any of the adiposity measures (Figure 1, Figure 2 and Figure 3). However, men with the highest level of occupational activity (i.e. > 20 MET-hr/day) had the lowest level of adiposity and women with the highest level of occupational activity also had the lowest percentage body fat. Working women were in general leaner than non-working women, in terms of all three adiposity measures, especially WC which was 1.0 cm smaller in working than in non-working women.
Figure 1.
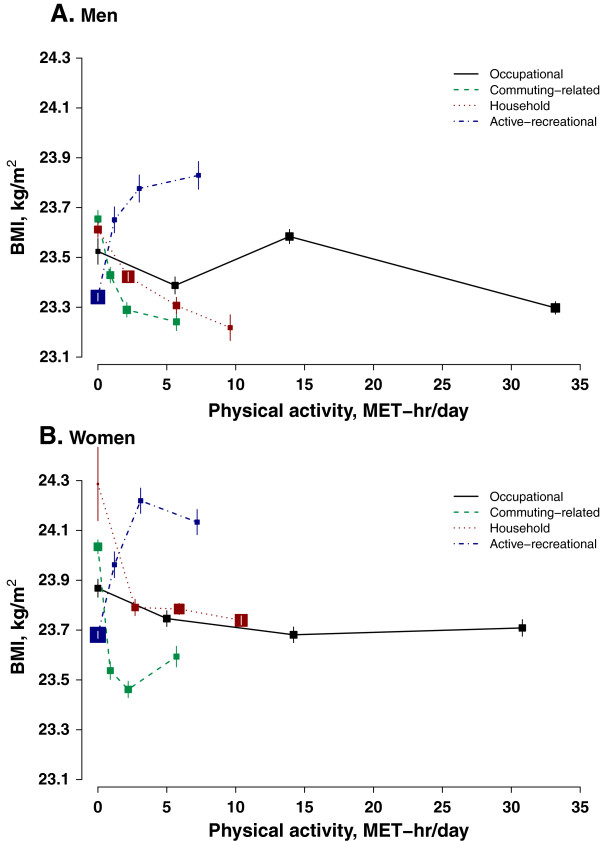
Body mass index in relation to physical activity from different domains. Analyses were adjusted for age (in 5-year intervals), study area, education, income, smoking, sedentary leisure time, and alcohol intake. Different domain-specific physical activities were mutually adjusted for each other. 2 participants with missing values on BMI were excluded from analyses. Sizes of boxes were inversely proportional to the standard errors of the point estimates. Panel A for men and panel B for women.
Figure 2.
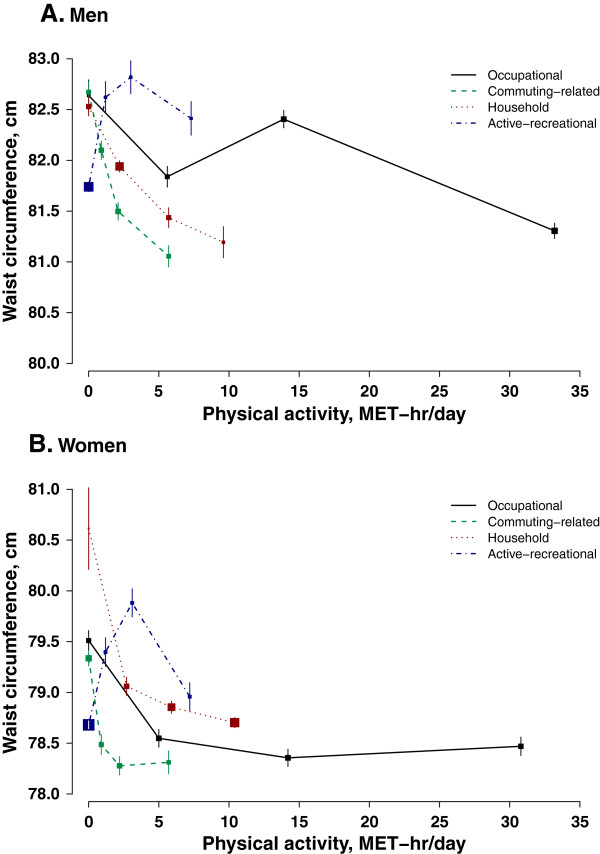
Waist circumference in relation to physical activity from different domains. Conventions as in Figure 1.
Figure 3.
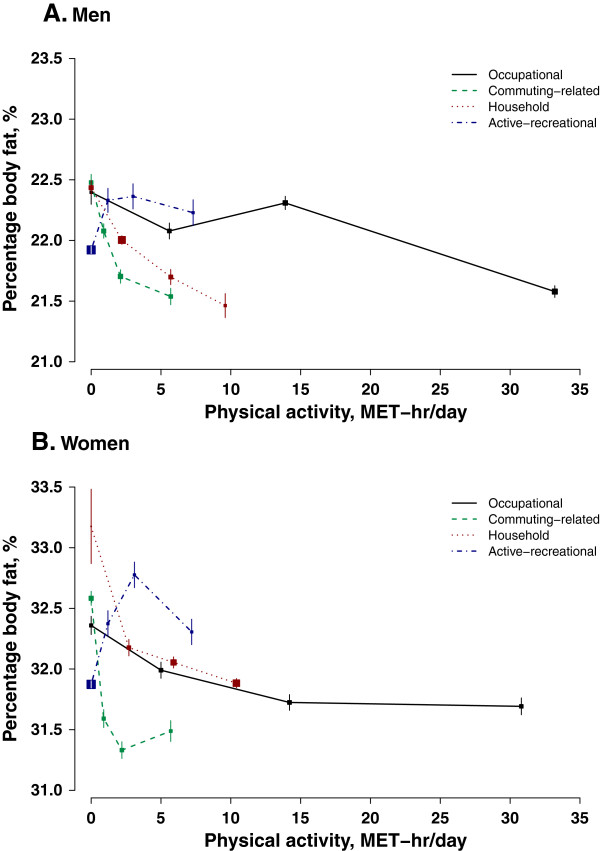
Percentage body fat in relation to physical activity from different domains. Conventions as in Figure 1. 214 participants with missing values on percentage of body fat were excluded from analyses.
In men, both commuting-related activity and household activity were inversely associated with adiposity regardless of how it is measured (Figure 1A, Figure 2A and Figure 3A). Men with high level of commuting (mean 5.7 MET-hr/day) had 0.4 kg/m2 lower BMI, 1.6 cm smaller WC, and 1.0% lower percentage body fat than those not commuting. Similar difference in adiposity was also seen in men between high (9.6 MET-hr/day) and no household activity: 0.4 kg/m2, 1.3 cm, and 1.0%, respectively. As shown in Additional file 2: Figure S2, per 3 MET-hr/day higher commuting-related activity was associated with 0.13 (95% CI: 0.11, 0.15) kg/m2 lower BMI, 0.62 (0.56, 0.68) cm smaller WC, and 0.16 (0.12, 0.20) percentage point less body fat. Household activity had a similar association with BMI and percentage body fat (3 MET-hr/day was associated with -0.11 (-0.10, -0.13) kg/m2 and -0.18 (-0.15, -0.21) percentage point), but its association with WC was much weaker compared to that of commuting-related activity (3 MET-hr/day was related to -0.42 (-0.38, -0.47) cm).
Female commuters overall had a much lower degree of adiposity than those who did not commute (0.5 kg/m2 BMI, 1.0 cm WC, and 1.1% body fat). However, there was a non- linear association between commuting-related activity and adiposity and women who had a moderate amount of commuting-related activity (1.6-3.0 MET-hr/day) tended to have the lowest level of adiposity (Figure 1B, Figure 2B and Figure 3B). In women, the inverse association between household activity and adiposity, though statistically significant, was much weaker than that in men. Restricting the analyses only to women who had some household activity (only 0.7% women were excluded), each 3 MET-hr/day higher household activity was associated with 0.02 (0.01, 0.03) kg/m2 lower BMI, 0.09 (0.06, 0.12) cm smaller WC, and 0.07 (0.05, 0.10) percentage point less body fat (Additional file 3: Figure S3).
In both men and women, those who reported performing some regular exercise during their leisure time tended to have a higher level of adiposity than those who did not (0.4 kg/m2 BMI, 0.9 cm WC and 0.4% body fat in men and 0.4 kg/m2 BMI, 0.7 cm WC and 0.6% body fat in women) (Figure 1, Figure 2 and Figure 3).
Discussion
This is the first well-powered and detailed study of domain-specific physical activity in relation to socio-demographic factors and adiposity among Chinese men and women from both urban and rural areas. With a much larger and more diverse population, our study confirms the findings reported in most previous studies based on people from China and other low- and middle-income countries [8, 22–24] in the following aspects: occupational and household physical activity are the two largest domains and women on average had a much greater level of household activity than men; older participants had a lower level of occupational activity but a higher level of household and active-recreational activity, particularly after retirement, due perhaps mainly to more available time for such activities. This study also found that the proportion of people performing active-recreational activity (22% of our participants) among Chinese adults is much lower than that typically seen in Western populations [25, 26], which may be attributable partly to less available time and partly to a lack of awareness about the importance of such activity, especially in rural areas [8, 22].
Although our study population is not intended to be representative of China as a whole or of any particular province [16], the associations observed, e.g. household activity in relation to adiposity, may still be generalisable to other settings or populations at large [27, 28]. The true association might even be stronger than that observed in this study since the 10 study areas probably do not include China’s full regional extremes.
An unexpected finding in our study was the lack of apparent association of occupational activity, the largest domain of total physical activity, with adiposity. Previous studies have provided mixed findings on this. For example, in two longitudinal studies, one involving ~3500 adults from the US National Health and Nutrition Examination Survey (NHANES) [13] and one on ~9400 adults in the China Health and Nutrition Survey (CHNS) [2], there was an inverse association between occupational activity and risk of obesity. But in a cross-sectional study of 12 044 people in the Spanish National Health Survey, neither BMI nor risk of obesity was significantly associated with level of work-related physical activity [12]. In another cross-sectional study of 1745 Swedish adults, there was a positive association of occupational physical activity with adiposity in women, but not in men [14]. Conversely, in a study among 1978 Vietnamese, an inverse association was observed only in men but not in women [29]. Disparities between these findings might be due to differences in study populations and methodologies used to assess occupational activity. Moreover, residual confounding by other factors, such as work-related stress and dietary habits, might also be an explanation for the lack of association between occupational activity and adiposity in our and other studies.
Another counterintuitive finding was that participants who engaged in regular active-recreational activities had higher, instead of lower, adiposity levels than those who did not. Reporting bias might be an explanation for this as it is known that people with a higher BMI tend to over-report the amount of exercise they performed to a greater extent than those with an ‘optimal’ body weight [30]. On the other hand, overweight and obese people may have started exercise more in order to control their body weight. However, this ‘reverse causality’ cannot be investigated reliably in the present cross-sectional analysis.
As in the present study, several previous studies have also reported an inverse association between household activity and adiposity in different populations [23, 31]. In a large national cohort study of over 70 000 Thai adults, the risk of being obese was 33% lower in participants who reported doing daily household activities than those who never or rarely did so [31]. In another study of 686 Malay participants, those with the lowest amount of household activity had double the risk of obesity compared to those with the highest amount [23]. In our study, women on average spent about 2.7 hours on household-related tasks, compared with only about 1 hour for men. If men could on average spend one extra hour daily on similar activities (2.8 MET-hr/day), i.e. switching from sedentary leisure time, then their adiposity indices would improve by 0.1 kg/m2, 0.37 cm and 0.17 percentage point lower respectively, independent of the effects of reduced sedentary leisure time [17].
As in other similar large-scale epidemiological studies, the present study used a questionnaire to assess levels of physical activity from all domains. Compared to more objective measures of physical activity (such as accelerometers) [32], questionnaire-assessed activities are more prone to measurement error due to recall bias (particularly among the elderly), social desirability bias, and difficulties associated with capturing low-intensity activities. In addition, misclassification might have occurred because the same MET value, from a compendium of MET values which mainly came from Western studies [33], being assigned to each type of activity regardless of between-person differences in intensity of performance. Physical activity questionnaires, however, remain as the most practical, feasible and cost-effective methods for quantifying habitual physical activity from different domains in large-scale epidemiological studies involving free-living participants [34]. Although no separate validation study has been conducted on our questionnaire, the observed associations between physical activity and socio-demographic factors in our study provide support for the validity of our physical activity questionnaire.
Conclusions
In Chinese adults, physical activity was derived mainly from occupation and housework, with active-recreational activity accounting for only a small proportion of total physical activity. Domain-specific physical activity varied by socio-demographic factors (such as sex, age, and socioeconomic status), and also had different associations with adiposity. Our findings may suggest that as well as total physical activity it is important to consider physical activity from different domains when assessing their health-related effects and recommending strategies for public health interventions. In particular, household and commuting-related activity (such as cycling) should be more widely publicized as effective ways for weight control. The continuation of the follow up for a wide range of health-related outcomes in the CKB participants will soon allow for the prospective assessment of the effects of total and domain-specific activities on risks of chronic diseases. Findings from prospective studies will further inform the development of public health policies on physical activity in China and other low- and middle-income countries where chronic disease burden is increasing.
Electronic supplementary material
Additional file 1: Figure S1: Levels of physical activity from different domains across 10 study areas. U: Urban areas; R: Rural areas. Levels of physical activity in each area was adjusted for age (in 5-year intervals). (PDF 20 KB)
Additional file 2: Figure S2: Commuting-related and household activity with BMI, waist circumference and percentage body fat in men. Associations were expressed as the regression coefficients (ß) for 3 MET-hr/day; Overall associations were estimated as inverse-variance-weighted averages. Analyses were adjusted for age, study area, education, income, sedentary leisure time, smoking, alcohol intake and other domain-specific activities. Only participants with some physical activity were included in analyses. (PDF 7 KB)
Additional file 3: Figure S3: Household activity with BMI, waist circumference and percentage body fat in 276 078 women. Conventions as in Additional file 2: Figure S2. (PDF 6 KB)
Acknowledgements
We thank Judith MacKay in Hong Kong; Yu Wang, Gonghuan Yang, Zhengfu Qiang, Lin Feng, Maigen Zhou, Wenhua Zhao and Yan Zhang in China CDC; Lingzhi Kong, Xiucheng Yu and Kun Li in the Ministry of Health of China; and Yiping Chen, Sarah Clark, Martin Radley, Hongchao Pan, Jill Boreham, and Sarah Lewington in the Clinical Trial Service Unit and Epidemiological studies Unit (CTSU), Oxford, for assisting with the design, planning, organization, conduct of the study and data analysis. The most important acknowledgement is to the participants in the study and the members of the survey teams in each of the 10 regional centres, as well as to the project development and management teams based at Beijing, Oxford and the 10 regional centres. CTSU acknowledges support from the British Heart Foundation Centre of Research Excellence, Oxford.
Members of China Kadoorie Biobank collaborative group are as follows:
International Co-ordinating Centre, Oxford: Zhengming Chen, Garry Lancaster, Xiaoming Yang, Alex Williams, Margaret Smith, Ling Yang, Yumei Chang, Iona Millwood, Yiping Chen, Sarah Lewington
National Co-ordinating Centre, Beijing: Yu Guo, Zheng Bian, Can Hou, Yunlong Tan
Regional Co-ordinating Centres, 10 areas in China:
Qingdao
Qingdao CDC: Zengchang Pang, Shanpeng Li, Shaojie Wang
Licang CDC: Silu Lv
Heilongjiang
Provincial CDC: Zhonghou Zhao, Shumei Liu, Zhigang Pang
Nangang CDC: Liqiu Yang, Hui He, Bo Yu
Hainan
Provincial CDC: Shanqing Wang, Hongmei Wang
Meilan CDC: Chunxing Chen, Xiangyang Zheng
Jiangsu
Provincial CDC: Xiaoshu Hu, Minghao Zhou, Ming Wu, Ran Tao
Suzhou CDC: Yeyuan Wang, Yihe Hu, Liangcai Ma
Wuzhong CDC: Renxian Zhou
Guangxi
Provincial CDC: Zhenzhu Tang, Naying Chen, Ying Huang
Liuzhou CDC: Mingqiang Li, Zhigao Gan, Jinhuai Meng, Jingxin Qin
Sichuan
Provincial CDC: Xianping Wu, Ningmei Zhang
Pengzhou CDC: Guojin Luo, Xiangsan Que, Xiaofang Chen
Gansu
Provincial CDC: Pengfei Ge, Xiaolan Ren, Caixia Dong
Maiji CDC: Hui Zhang, Enke Mao, Zhongxiao Li
Henan
Provincial CDC: Gang Zhou, Shixian Feng
Huixian CDC: Yulian Gao, Tianyou He, Li Jiang, Huarong Sun
Zhejiang
Provincial CDC: Min Yu, Danting Su, Feng Lu
Tongxiang CDC: Yijian Qian, Kunxiang Shi, Yabin Han, Lingli Chen
Hunan
Provincial CDC: Guangchun Li, Huilin Liu, Li Yin
Liuyang CDC: Youping Xiong, Zhongwen Tan, Weifang Jia
Funding
The China Kadoorie Biobank study is sponsored by the Kadoorie Charitable Foundation in Hong Kong, China, the Wellcome Trust in the UK, the UK Medical Research Council (MRC), the British Heart Foundation, Cancer Research UK, and the National Key Technology Research and Development Program in the 12th Five-Year Plan, Ministry of Science and Technology, People’s Republic of China (Ref: 2011BAI09B01). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The members of the steering committee and collaborative group of the China Kadoorie Biobank are listed in the Acknowledgement section
Abbreviations
- BMI
Body mass index
- CKB
China Kadoorie Biobank
- MET
Metabolic equivalent
- WC
Waist circumference.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HD performed the data analysis and wrote the manuscript; DB and PS helped with the statistical analyses and graphing; GW, DB and ZC contributed to the conception of this paper, helped with the interpretation of the results, and gave critical comments on the manuscript; LL, JC, RC, RP and ZC designed the study, obtained the funding, and contributed to the acquisition of data; and YG, ZB, YH, NZ, XZ, ZL and RH contributed to the data acquisition. All authors have read and approved the final manuscript, except for the deceased GW who had commented on the sub-final version of the manuscript. HD had full access to all of the data in the analysis and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Contributor Information
Huaidong Du, Email: huaidong.du@ctsu.ox.ac.uk.
Liming Li, Email: lmlee@vip.163.com.
Gary Whitlock, Email: gary.whitlock@ctsu.ox.ac.uk.
Derrick Bennett, Email: derrick.bennett@ctsu.ox.ac.uk.
Yu Guo, Email: guoyu@kscdc.net.
Zheng Bian, Email: Bianzheng@kscdc.net.
Junshi Chen, Email: junshichen@yahoo.com.
Paul Sherliker, Email: paul.sherliker@ctsu.ox.ac.uk.
Ying Huang, Email: huangying526@sina.com.
Ningmei Zhang, Email: zhangnmy@163.com.
Xiangyang Zheng, Email: 459225338@qq.com.
Zhongxiao Li, Email: lizhongxiao0408@163.com.
Ruying Hu, Email: ryhu@cdc.zj.cn.
Rory Collins, Email: rory.collins@ctsu.ox.ac.uk.
Richard Peto, Email: richard.peto@ctsu.ox.ac.uk.
Zhengming Chen, Email: zhengming.chen@ctsu.ox.ac.uk.
References
- 1.O’Donovan G, Blazevich AJ, Boreham C, Cooper AR, Crank H, Ekelund U, Fox KR, Gately P, Giles-Corti B, Gill JM, Hamer M, McDermott I, Murphy M, Mutrie N, Reilly JJ, Saxton JM, Stamatakis E. The ABC of Physical Activity for Health: a consensus statement from the British Association of Sport and Exercise Sciences. J Sports Sci. 2010;28:573–591. doi: 10.1080/02640411003671212. [DOI] [PubMed] [Google Scholar]
- 2.Monda KL, Adair LS, Zhai F, Popkin BM. Longitudinal relationships between occupational and domestic physical activity patterns and body weight in China. Eur J Clin Nutr. 2008;62:1318–1325. doi: 10.1038/sj.ejcn.1602849. [DOI] [PubMed] [Google Scholar]
- 3.Ng SW, Norton EC, Popkin BM. Why have physical activity levels declined among Chinese adults? Findings from the 1991–2006 China Health and Nutrition Surveys. Soc Sci Med. 2009;68:1305–1314. doi: 10.1016/j.socscimed.2009.01.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bauman A, Allman-Farinelli M, Huxley R, James WP. Leisure-time physical activity alone may not be a sufficient public health approach to prevent obesity–a focus on China. Obes Rev. 2008;9(Suppl 1):119–126. doi: 10.1111/j.1467-789X.2007.00452.x. [DOI] [PubMed] [Google Scholar]
- 5.Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380:258–271. doi: 10.1016/S0140-6736(12)60735-1. [DOI] [PubMed] [Google Scholar]
- 6.Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Med Sci Sports Exerc. 2002;34:1996–2001. doi: 10.1097/00005768-200212000-00020. [DOI] [PubMed] [Google Scholar]
- 7.Bauman A, Ma G, Cuevas F, Omar Z, Waqanivalu T, Phongsavan P, Keke K, Bhushan A. Cross-national comparisons of socioeconomic differences in the prevalence of leisure-time and occupational physical activity, and active commuting in six Asia-Pacific countries. J Epidemiol Community Health. 2011;65:35–43. doi: 10.1136/jech.2008.086710. [DOI] [PubMed] [Google Scholar]
- 8.Jurj AL, Wen W, Gao YT, Matthews CE, Yang G, Li HL, Zheng W, Shu XO. Patterns and correlates of physical activity: a cross-sectional study in urban Chinese women. BMC Public Health. 2007;7:213. doi: 10.1186/1471-2458-7-213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hu G, Pekkarinen H, Hanninen O, Yu Z, Guo Z, Tian H. Commuting, leisure-time physical activity, and cardiovascular risk factors in China. Med Sci Sports Exerc. 2002;34:234–238. doi: 10.1097/00005768-200202000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Millett C, Agrawal S, Sullivan R, Vaz M, Kurpad A, Bharathi AV, Prabhakaran D, Reddy KS, Kinra S, Smith GD, Ebrahim S. Associations between Active Travel to Work and Overweight, Hypertension, and Diabetes in India: A Cross-Sectional Study. PLoS Med. 2013;10:e1001459. doi: 10.1371/journal.pmed.1001459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gordon-Larsen P, Boone-Heinonen J, Sidney S, Sternfeld B, Jacobs DR, Jr, Lewis CE. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med. 2009;169:1216–1223. doi: 10.1001/archinternmed.2009.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gutierrez-Fisac JL, Guallar-Castillon P, Diez-Ganan L, Lopez Garcia E, Banegas Banegas JR, Rodriguez Artalejo F. Work-related physical activity is not associated with body mass index and obesity. Obes Res. 2002;10:270–276. doi: 10.1038/oby.2002.37. [DOI] [PubMed] [Google Scholar]
- 13.Steeves JA, Bassett DR, Jr, Thompson DL, Fitzhugh EC. Relationships of occupational and non-occupational physical activity to abdominal obesity. Int J Obes (Lond) 2012;36:100–106. doi: 10.1038/ijo.2011.50. [DOI] [PubMed] [Google Scholar]
- 14.Larsson CA, Kroll L, Bennet L, Gullberg B, Rastam L, Lindblad U. Leisure time and occupational physical activity in relation to obesity and insulin resistance: a population-based study from the Skaraborg Project in Sweden. Metabolism. 2012;61:590–598. doi: 10.1016/j.metabol.2011.09.010. [DOI] [PubMed] [Google Scholar]
- 15.Chen Z, Lee L, Chen J, Collins R, Wu F, Guo Y, Linksted P, Peto R. Cohort profile: the Kadoorie Study of Chronic Disease in China (KSCDC) Int J Epidemiol. 2005;34:1243–1249. doi: 10.1093/ije/dyi174. [DOI] [PubMed] [Google Scholar]
- 16.Chen Z, Chen J, Collins R, Guo Y, Peto R, Wu F, Li L. China Kadoorie Biobank of 0.5 million people: survey methods, baseline characteristics and long-term follow-up. Int J Epidemiol. 2011;40:1652–1666. doi: 10.1093/ije/dyr120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Du H, Bennett D, Li L, Whitlock G, Guo Y, Collins R, Chen J, Bian Z, Hong LS, Feng S, Chen X, Chen L, Zhou R, Mao E, Peto R, Chen Z. Physical activity and sedentary leisure time and their associations with BMI, waist circumference, and percentage body fat in 0.5 million adults: the China Kadoorie Biobank study. Am J Clin Nutr. 2013;97:487–496. doi: 10.3945/ajcn.112.046854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wareham NJ, Jakes RW, Rennie KL, Mitchell J, Hennings S, Day NE. Validity and repeatability of the EPIC-Norfolk Physical Activity Questionnaire. Int J Epidemiol. 2002;31:168–174. doi: 10.1093/ije/31.1.168. [DOI] [PubMed] [Google Scholar]
- 19.Matthews CE, Shu XO, Yang G, Jin F, Ainsworth BE, Liu D, Gao YT, Zheng W. Reproducibility and validity of the Shanghai Women’s Health Study physical activity questionnaire. Am J Epidemiol. 2003;158:1114–1122. doi: 10.1093/aje/kwg255. [DOI] [PubMed] [Google Scholar]
- 20.Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR, Jr, Tudor-Locke C, Greer JL, Vezina J, Whitt-Glover MC, Leon AS. Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;2011(43):1575–1581. doi: 10.1249/MSS.0b013e31821ece12. [DOI] [PubMed] [Google Scholar]
- 21.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lee SA, Xu WH, Zheng W, Li H, Yang G, Xiang YB, Shu XO. Physical activity patterns and their correlates among Chinese men in Shanghai. Med Sci Sports Exerc. 2007;39:1700–1707. doi: 10.1249/mss.0b013e3181238a52. [DOI] [PubMed] [Google Scholar]
- 23.Chu AH, Moy FM. Prev Med. 2012. Associations of occupational, transportation, household and leisure-time physical activity patterns with metabolic risk factors among middle-aged adults in a middle-income country. [DOI] [PubMed] [Google Scholar]
- 24.Khaing Nang EE, Khoo EY, Salim A, Tai ES, Lee J, Van Dam RM. Patterns of physical activity in different domains and implications for intervention in a multi-ethnic Asian population: a cross-sectional study. BMC Public Health. 2010;10:644. doi: 10.1186/1471-2458-10-644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Martinez-Gonzalez MA, Martinez JA, Hu FB, Gibney MJ, Kearney J. Physical inactivity, sedentary lifestyle and obesity in the European Union. Int J Obes (Lond) 1999;23:1192–1201. doi: 10.1038/sj.ijo.0801049. [DOI] [PubMed] [Google Scholar]
- 26.Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1081–1093. doi: 10.1161/CIRCULATIONAHA.107.185649. [DOI] [PubMed] [Google Scholar]
- 27.Collins R. What makes UK Biobank special? Lancet. 2012;379:1173–1174. doi: 10.1016/S0140-6736(12)60404-8. [DOI] [PubMed] [Google Scholar]
- 28.Manolio TA, Collins R. Enhancing the feasibility of large cohort studies. JAMA. 2010;304:2290–2291. doi: 10.1001/jama.2010.1686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Thuy AB, Blizzard L, Schmidt MD, Pham LH, Granger RH, Dwyer T. Physical activity and its association with cardiovascular risk factors in Vietnam. Asia Pac J Public Health. 2012;24:308–317. doi: 10.1177/1010539510379394. [DOI] [PubMed] [Google Scholar]
- 30.Slootmaker SM, Schuit AJ, Chinapaw MJ, Seidell JC, van Mechelen W. Disagreement in physical activity assessed by accelerometer and self-report in subgroups of age, gender, education and weight status. Int J Behav Nutr Phys Act. 2009;6:17. doi: 10.1186/1479-5868-6-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Banks E, Lim L, Seubsman SA, Bain C, Sleigh A. Relationship of obesity to physical activity, domestic activities, and sedentary behaviours: cross-sectional findings from a national cohort of over 70,000 Thai adults. BMC Public Health. 2011;11:762. doi: 10.1186/1471-2458-11-762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Jimenez-Pavon D, Konstabel K, Bergman P, Ahrens W, Pohlabeln H, Hadjigeorgiou C, Siani A, Iacoviello L, Molnar D, De Henauw S, Pitsiladis Y, Moreno LA. Physical activity and clustered cardiovascular disease risk factors in young children: a cross-sectional study (the IDEFICS study) BMC Med. 2013;11:172. doi: 10.1186/1741-7015-11-172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ng SW, Popkin BM. Time use and physical activity: a shift away from movement across the globe. Obes Rev. 2012;13:659–680. doi: 10.1111/j.1467-789X.2011.00982.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Haskell WL. Physical activity by self-report: a brief history and future issues. J Phys Act Health. 2012;9(Suppl 1):S5–S10. doi: 10.1123/jpah.9.s1.s5. [DOI] [PubMed] [Google Scholar]
Pre-publication history
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/826/prepub
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Figure S1: Levels of physical activity from different domains across 10 study areas. U: Urban areas; R: Rural areas. Levels of physical activity in each area was adjusted for age (in 5-year intervals). (PDF 20 KB)
Additional file 2: Figure S2: Commuting-related and household activity with BMI, waist circumference and percentage body fat in men. Associations were expressed as the regression coefficients (ß) for 3 MET-hr/day; Overall associations were estimated as inverse-variance-weighted averages. Analyses were adjusted for age, study area, education, income, sedentary leisure time, smoking, alcohol intake and other domain-specific activities. Only participants with some physical activity were included in analyses. (PDF 7 KB)
Additional file 3: Figure S3: Household activity with BMI, waist circumference and percentage body fat in 276 078 women. Conventions as in Additional file 2: Figure S2. (PDF 6 KB)