

Abstract
Objective:
The aims of this study were to determine the prevalence of hypodontia in the permanent dentition in a sample of Sudanese patients who sought orthodontic treatment and to compare the results with the reported findings of other populations.
Materials and Methods:
Orthodontic files including orthopantomographs of 1069 patients (760 females and 309 males - more than 8 years old) were examined and inspected for evidence of hypodontia.
Results:
The prevalence of hypodontia of the present sample was 5.1%. Hypodontia was found considerably more frequently in the mandible than in the maxilla. The distribution of missing teeth was noticed in the left side more than in the right side. The most frequently missing teeth were the maxillary lateral incisors, followed by the mandibular second premolars, maxillary second premolars and mandibular left lateral incisor. The majority of patients had two or three teeth missing, but rarely more than 5 teeth missing.
Conclusions:
The prevalence of hypodontia of this study was within the range of that reported in the literature. The incidence of hypodontia in the anterior segment requires great need for orthodontic and prosthodontic treatment. With early detection of hypodontia, alternative treatment modalities can be planned and performed with a multidisciplinary team approach restoring the esthetic and function.
Keywords: Hypodontia, orthodontics, prevalence, tooth agenesis
INTRODUCTION AND REVIEW OF THE LITERATURE
Hypodontia is the developmental absence of one or more teeth, excluding the third molars. It is one of the most common craniofacial malformations, and it is more common in the permanent dentition than deciduous dentition.[1] It is classified according to the number of missing teeth. Mild hypodontia when there were two teeth missing, moderate hypodontia when there were 3-5 teeth missing and severe hypodontia when there were greater than six teeth missing. Oligodontia is the absence of multiple teeth, and it usually associated with systemic disorders.[2] Hypodontia is also classified as either isolated hypodontia or syndromic hypodontia. Isolated hypodontia refers to those cases without syndrome.[3,4]
The etiology of hypodontia is a consequence of physical obstruction or disruption of the dental lamina, space limitation, and functional abnormalities of the dental epithelium or failure of initiation of the underlying mesenchyme. However, what determines these events is still open to speculation.[5] Hypodontia is occasionally caused by environmental factors. In the majority of cases, hypodontia has genetic bases. It is more common among individuals related to hypodontia patients than in the general population.[1]
Some craniofacial problems like cleft lip and palate may be associated with congenitally missing teeth, the rates of anterior missing teeth on the cleft side varied between 70.8% and 97.1%, depending on cleft type. Different rates of agenesis can be related to the severity of the cleft phenotype, which has been shown to have a correlation with the number of affected teeth.[6]
Recent studies realized that hypodontia may be an indicator of susceptibility for developing cancer.[7] Hypodontia was reported more common (8.1 times) in women with epithelial ovarian cancer than women without epithelial ovarian cancer. This was documented by Chalothorn et al.[8]
The prevalence of hypodontia varies among different ethnic backgrounds. It is more common among females than males in many populations.[9] The most commonly affected site/tooth also appears to vary among different ethnic groups. The teeth that most affected (excluding the third molars) are the mandibular second premolars, the maxillary lateral incisors, and the maxillary second premolars. However, some studies have demonstrated the maxillary lateral incisors and the mandibular lateral incisors are the most common missing teeth.[1,10]
Many epidemiological studies concerning the prevalence of tooth anomalies have given a vast amount of information on the different types of hypodontia; it is prevalence and distribution in various part of the world. Different results have been reached by several authors showing the wide range of variety in the prevalence of hypodontia among orthodontic patients and populations between the different ethnic groups.
Chung et al.[9] studied the prevalence of hypodontia in the Korean population as well as its association with the congenital absence of the third molar. Casts, panoramic radiographs, and lateral cephalographs of 1622 Korean subjects (611 males, 1011 females) were used. The percentage of hypodontia was 11.2%. They noticed that hypodontia was higher in the mandible more than in the maxilla and the most commonly affected tooth was lateral incisors (40%) followed by second premolar (20.4%) in the mandible.
Endo et al.[11] investigated the association of hypodontia patterns and variations in craniofacial morphology in Japanese orthodontic patients, a total of 50 girls with hypodontia were selected and categorized into anterior, posterior, and anterior-posterior groups according to the location of the congenitally missing teeth. Every hypodontia group showed shorter anterior-mandibular incisors, and a larger interincisal angle than the control group.
Bhardwaj et al.[12] carried out study in Shimla, Himachal Pradesh, India among 16- and 17-year-old school-going children. A total of 622 students were examined. 8.7% of the students had at least one or more permanent teeth missing. Whereas in another study conducted in India; revealed that hypodontia was less common (4.2%).[13]
Ajami et al.[14] Investigated the prevalence of hypodontia in 600 Iranian children between 9 and 14 years old at Mashhad School of Dentistry. The result showed that, a total of 54 (9%) children were affected with hypodontia where 31 (9.2%) were girls and 23 (8.8%) were boys. Furthermore, the prevalence of hypodontia in girls was higher than in boys.
Polder et al.[15] did a study using the meta-analysis to gain more insight into the prevalence of dental agenesis and stated that agenesis differs by continent and gender, The prevalence for both sexes was higher in European population (males 4.6% and females 6.3%), and also the same was observed in an Australian sample (males 5.5%; females 7.6%) than for the North American Caucasians (males 3.2%; females 4.6%). Further, the prevalence of dental agenesis in females was almost 1.4 times higher than in males. The mandibular second premolar was the most affected tooth, followed by the maxillary lateral incisor and the maxillary second premolar.[15]
In Germany; a retrospective study was performed in 1353 patients by Behr et al.[16] at the Regensburg University Medical Center. Missing permanent teeth were found in 171 (12.6%); of these 64.3% had one or two missing teeth, three to five teeth were missing in 19.9%, and oligodontia was found in 15.8% of the patients. The percentage was equally distributed between the females and males. Further, the most frequently missing teeth were lower second premolar (5.9%), lower right second premolar (5.1%), upper left lateral incisor (4.0%), upper right lateral incisor (3.6%), upper right second premolar (3.1%), and upper left second premolar (3.0%).
Fekonja[2] evaluated the prevalence of hypodontia in orthodontically treated children from the records of 212 orthodontic patients. Of these, 24 patients; 9 males and 15 females had agenesis of one or more teeth (11.3%). Patients with more severe hypodontia showed a tendency to a Class III relationship and an increased overbite.
Furthermore, a retrospective study was done in Brazil by Gomes et al.[17] to determine the prevalence of hypodontia and associated dental anomalies in orthodontic patients. The records of 1049 orthodontic patients (507 males and 542 females) showed hypodontia in 6.3% of the patients. Maxillary hypodontia were found in 59.2% of patients and 40.8% in the mandible with an overall ratio of 1.45:1.[17]
Celikoglu et al.[10] evaluated the frequency of tooth agenesis among 3341 Turkish orthodontic patients (2040 females and 1301 males). The reported percentage of tooth agenesis was 4.6%.[10] In another Turkish study, a higher percentage (7.54%) was reported by Sisman et al.[18] Both studies show the prevalence was more common in females than males.[18] Furthermore, a much higher percentage was reported among Turkish patients with cleft lip and palate.[10]
Albashaireh and Khader[19] have reported 5.5% of hypodontia of the permanent teeth, crown size and shape deformity affecting upper lateral incisors in a Jourdan sample of 1045 dental patients aged 16-45 years. On the other hand, al-Emran et al.[20] found that hypodontia prevalence among the Saudi male school children was 4%. Whereas Afifiy and Zawawi[21] have reported a very high prevalence (25.7%) of congenitally missing teeth in the Western region of Saudi Arabia.
Ng’ang’a and Ng’ang’a[22] have reported the prevalence of hypodontia among 615 Kenyan children (331 males and 284 females) with male: female ratio of 2.4:1.5 was 6.3%. Further, Abuaffan[23] found the prevalence of congenitally missing teeth in 12 years Sudanese children was 6.6% in Khartoum state.
Hence, the aims of this study were to determine the prevalence of hypodontia in the permanent dentition among Sudanese population who sought orthodontic treatment in private clinics and to compare the results with the reported findings of other populations.
MATERIALS AND METHODS
The sample of this study consisted of orthodontic files including orthopantomographs of 1069 (760 females and 309 males, age more than 8 years old) who attended private orthodontic clinics. All selected files were examined and inspected for evidence of hypodontia. Patients with incomplete records, poor image quality and history of missing teeth due to trauma, extraction, syndromes or periodontal disease, patient with no previous history of orthodontic treatment were excluded. The study protocol was ethically approved by the research committees.
Data Collection Technique
Examinations and inspections of the orthopantomogrphs for the missing tooth on the radiographs were carried out using X-ray viewer in a dark room. The missing teeth were recorded in a data sheet.
Data Processing and Analysis
Data were analyzed using the SPSS software version 16.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were utilized to conduct the results.
RESULTS
Figure 1 exhibited that out of 1069 patients (760 females and 309 males); 55 patients had congenitally missing teeth. This value indicates that the prevalence in percentage of hypodontia among this sample was 5.1%.
Figure 1.
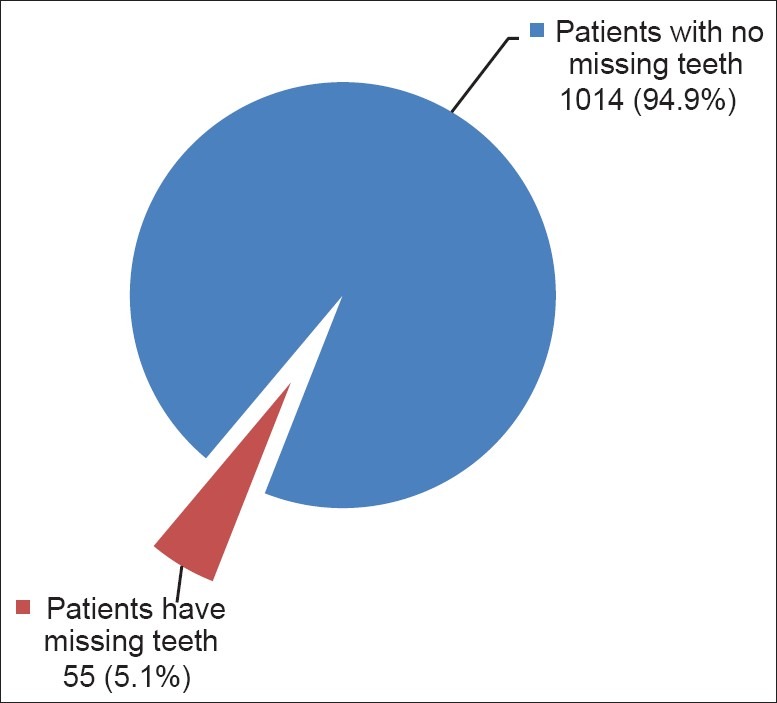
Prevalence of hypodontia in males and females combined among the Sudanese orthodontic patient sample (n: 1069)
Figure 2 showed that 87.3% (48) of the females and 12.7% (7) of the males had congenitally missing teeth indicating that hypodontia was found to be more common among females than males.
Figure 2.
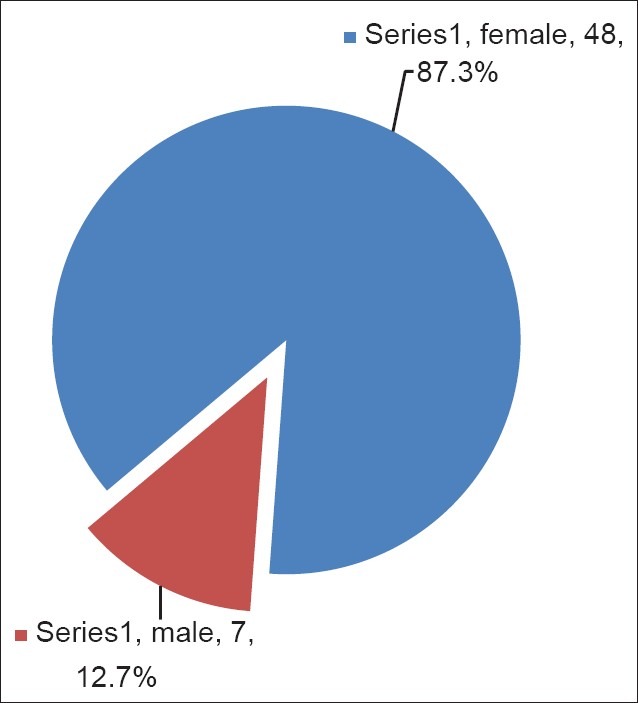
Gender distribution of hypodontia in orthodontic patient sample of this study
Table 1 revealed the prevalence of hypodontia in the upper jaw for females and males. The lateral incisors was found to be the most commonly missing tooth followed by second premolar, canine, but none of the central incisors or first premolars were missing.
Table 1.
Prevalence of hypodontia for females and males in the upper jaw

Table 2 demonstrated that in the lower jaw; hypodontia was noted to be more commonly in the left side and females were more affected than males. The most common missing tooth was the left second premolar followed by right second premolar, left lateral incisor, right lateral incisor then first premolars. None of the central incisor or canines was missing.
Table 2.
Prevalence of hypodontia for females and males in the lower jaw

The result of the histogram [Figure 3] demonstrated that hypodontia was found to be more common bilaterally (76.4%); whereas in unilateral cases; the left side was affected more than the right side.
Figure 3.
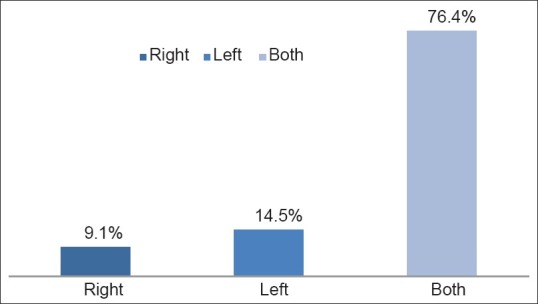
Most common affected side by the hypodontia in orthodontic patient sample
DISCUSSION
This is a descriptive cross-sectional study to determine the prevalence of hypodontia in a sample of Sudanese patients who sought orthodontic treatment in a private clinic in Khartoum state and to compare the results with the reported findings of other populations.
Hypodontia is generally defined as the developmental absence of one or more teeth excluding the third molars. It is more common in the permanent dentition. The prevalence of hypodontia in the primary dentition is found to be very low. The range has generally been between 0.1% and 0.9% of the population.[24] Researchers have used a variety of terminology to describe the condition, such as a reduction in teeth number, teeth aplasia, congenitally missing teeth, absence of teeth, agenesis of teeth, and lack of teeth.[24,25,26]
A distinct genetic influence on the development of teeth has been demonstrated, with a high proportion of individuals with hypodontia coming from families with previous hypodontia[27] and Environmental factors have also been implicated in the etiology of hypodontia.[28,29]
The result of this study showed prevalence of 5.1% of hypodontia in orthodontic patients in Khartoum state which was lower than that documented in other similar studies.[2,16,17] However, a very high prevalence was reported in two German studies (12.6%)[16] and (11.3%)[2] when compared to this study result. Further, in Japanese orthodontic patients, a lower percentage value of 8.5% was noted,[11] when compared to the German study and higher than the results of our study. Furthermore, the prevalence observed in this study was relatively higher than that in Turkish orthodontic patients (4.6%).[10]
Worldwide, many studies were conducted to evaluate the prevalence of hypodontia among the population,[9,12,13,14,15] The wide range of prevalence values (4.6-12.6%) observed in these studies has indicated that geographic, gender, races, and genetics differences as well as the large differences in the sample sizes and the criteria of selection were playing an important role in these various results of hypodontia.[2,9,10,11,16,17,18] This wide range make the comparison of this study result very limited with other previous studies in addition to other contributing factors.
In this study, the females show a higher prevalence of hypodontia than males (4.47% females - 0.65% males), which is in accordance with the majority of previous reports.[17,20,21,25] However, in the German study; the percentage was equally distributed between the females and males.[16] Nevertheless, the literature does not confirm this.
When comparing between the right and left sides, this study showed that hypodontia existed more on the left side (14.5% left, 9.1% right), whereas hypodontia was more common in the mandible than in the maxilla. This is in concert with the results that was reported by Chung et al.[9] in Korean population.
Some studies show that the most commonly missing teeth differed from one ethnic group to another. In this study, the most frequent congenitally missing teeth were the upper lateral incisors (2.1%) followed by lower left second premolar (1.7%), lower right second premolar (1.3%), upper second premolars (1.2%), subsequently followed by the lower lateral incisors (0.8%). On the other hand, the least tooth to be found missing were the bilateral upper canines (0.1%) which was observed in one patient. This result was partially in agreement with the result obtained by Abuaffan[23] in a previous study carried out among 12 years Sudanese school children. She reported that the permanent teeth most frequently congenitally missing were mandibular incisors 3% followed by maxillary lateral incisors 1.5%, maxillary second premolars 0.9% and mandibular second premolars 0.5%.[26] In this study, no central incisors, first upper premolars or lower canines were reported as missing. The differences might be due to age and ethnicity of the included subjects.[15] Other researcher suggested that evolutionary changes might as well contribute to these differences.[30]
The congenital absence of teeth can seriously disable a young person both physically and emotionally, especially during the turbulent years of adolescence. Thus, treatment of dental agenesis should be initiated during adolescence, independent of the number of missing permanent teeth and the cause of the condition. Ideally, interim treatment should take place even before these children realize that they are different from other children.[18]
Further, Lai and Seow[31] stated that in patients with missing permanent teeth, clinicians should be alert to the possibility of these associated anomalies and their accompanying clinical implications. Thus, with early detection of hypodontia, alternative treatment modalities can be planned and performed with a multidisciplinary team approach to restore the esthetic and function.
The result of this study warrants further multicenter investigations to include different parts of Sudan. This will increase the sample size and be more representative. The information obtained from such investigation will be of great value not only for the orthodontist, but also to the prosthodontist in diagnosis and treatment plan.
CONCLUSIONS
The prevalence of hypodontia in this study (5.1%) was within the range that reported in the literature
The incidence of hypodontia in the anterior segment requires great need for orthodontic and prosthodontic treatment
With early detection of hypodontia, alternative treatment modalities can be planned and performed with a multidisciplinary team approach to restore the esthetic and function.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kirzioğlu Z, Köseler Sentut T, Ozay Ertürk MS, Karayilmaz H. Clinical features of hypodontia and associated dental anomalies: A retrospective study. Oral Dise. 2005;11:399–404. doi: 10.1111/j.1601-0825.2005.01138.x. [DOI] [PubMed] [Google Scholar]
- 2.Fekonja A. Hypodontia in orthodontically treated children. Eur J Orthod. 2005;27:457–60. doi: 10.1093/ejo/cji027. [DOI] [PubMed] [Google Scholar]
- 3.Arte S, Nieminen P, Apajalahti S, Haavikko K, Thesleff I, Pirinen S. Characteristics of incisor-premolar hypodontia in families. J Dent Res. 2001;80:1445–50. doi: 10.1177/00220345010800051201. [DOI] [PubMed] [Google Scholar]
- 4.Tan SP, van Wijk AJ, Prahl-Andersen B. Severe hypodontia: Identifying patterns of human tooth agenesis. Eur J Orthod. 2011;33:150–54. doi: 10.1093/ejo/cjq046. [DOI] [PubMed] [Google Scholar]
- 5.Rushmah Meon. Hypodontia of the primary and permanent dentition. J Clin Pediatr Dent. 1992;16:121–23. [PubMed] [Google Scholar]
- 6.Akcam MO, Evirgen S, Uslu O, Memikoğlu UT. Dental anomalies in individuals with cleft lip and/or palate. Eur J Orthod. 2010;32:207–13. doi: 10.1093/ejo/cjp156. [DOI] [PubMed] [Google Scholar]
- 7.Ch. 7. 9th ed. 2011. Donald and Avery's Dentistry for the Child and Adolescent; pp. 108–9. [Google Scholar]
- 8.Chalothorn LA, Beeman CS, Ebersole JL, Kluemper GT, Hicks EP, Kryscio RJ, et al. Hypodontia as a risk marker for epithelial ovarian cancer: A case-controlled study. J Am Dent Assoc. 2008;139:163–69. doi: 10.14219/jada.archive.2008.0132. [DOI] [PubMed] [Google Scholar]
- 9.Chung CJ, Han JH, Kim KH. The pattern and prevalence of hypodontia in Koreans. Oral Dis. 2008;14:620–25. doi: 10.1111/j.1601-0825.2007.01434.x. [DOI] [PubMed] [Google Scholar]
- 10.Celikoglu M, Kazanci F, Miloglu O, Oztek O, Kamak H, Ceylan I. Frequency and characteristics of tooth agenesis among an orthodontic patient population. Med Oral Patol Oral Cir Bucal. 2010;15:e797–801. doi: 10.4317/medoral.15.e797. [DOI] [PubMed] [Google Scholar]
- 11.Endo T, Ozoe R, Yoshino S, Shimooka S. Hypodontia patterns and variations in craniofacial morphology in Japanese orthodontic patients. Angle Orthod. 2006;76:996–1003. doi: 10.2319/082905-303. [DOI] [PubMed] [Google Scholar]
- 12.Bhardwaj VK, Veeresha KL, Sharma KR. Prevalence of malocclusion and orthodontic treatment needs among 16 and 17 year-old school-going children in Shimla city, Himachal Pradesh. Indian J Dent Res. 2011;22:556–60. doi: 10.4103/0970-9290.90296. [DOI] [PubMed] [Google Scholar]
- 13.Gupta SK, Saxena P, Jain S, Jain D. Prevalence and distribution of selected developmental dental anomalies in an Indian population. J Oral Sci. 2011;53:231–38. doi: 10.2334/josnusd.53.231. [DOI] [PubMed] [Google Scholar]
- 14.Ajami BA, Shabzendedar M, Mehrjerdian M. Prevalence of hypodontia in nine-to fourteen-year-old children who attended the Mashhad School of Dentistry. Indian J Dent Res. 2010;21:549–51. doi: 10.4103/0970-9290.74215. [DOI] [PubMed] [Google Scholar]
- 15.Polder BJ, Van’t Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32:217–26. doi: 10.1111/j.1600-0528.2004.00158.x. [DOI] [PubMed] [Google Scholar]
- 16.Behr M, Proff P, Leitzmann M, Pretzel M, Handel G, Schmalz G, et al. Survey of congenitally missing teeth in orthodontic patients in Eastern Bavaria. Eur J Orthod. 2011;33:32–36. doi: 10.1093/ejo/cjq021. [DOI] [PubMed] [Google Scholar]
- 17.Gomes RR, da Fonseca JA, Paula LM, Faber J, Acevedo AC. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur J Orthod. 2010;32:302–06. doi: 10.1093/ejo/cjp107. [DOI] [PubMed] [Google Scholar]
- 18.Sisman Y, Uysal T, Gelgor IE. Hypodontia. Does the prevalence and distribution pattern differ in orthodontic patients? Eur J Dent. 2007;1:167–73. [PMC free article] [PubMed] [Google Scholar]
- 19.Albashaireh ZS, Khader YS. The prevalence and pattern of hypodontia of the permanent teeth and crown size and shape deformity affecting upper lateral incisors in a sample of Jordanian dental patients. Community Dent Health. 2006;23:239–43. [PubMed] [Google Scholar]
- 20.AL-Emran S, Wisth PJ, Böe OE. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18:253–55. doi: 10.1111/j.1600-0528.1990.tb00070.x. [DOI] [PubMed] [Google Scholar]
- 21.Afify AR, Zawawi KH. The prevalence of dental anomalies in the Western region of Saudi Arabia. ISRN Dent. 2012;2012:837270. doi: 10.5402/2012/837270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ng’ang’a RN, Ng’ang’a PM. Hypodontia of permanent teeth in a Kenyan population. East Afr Med J. 2001;78:200–03. doi: 10.4314/eamj.v78i4.9063. [DOI] [PubMed] [Google Scholar]
- 23.Abuaffan AH. Malocclusion and dental development in 12-years-old Sudanese children from the Khartoum area, Master of Science Thesis Faculty of Dentistry University of Bergen. 1987. ISBN 82-7249-078-1. [Google Scholar]
- 24.Brook AH. Dental anomalies of number, form and size: Their prevalence in British school children. J. Int. Assoc Dent Child. 1974;5:37–53. [PubMed] [Google Scholar]
- 25.Hunstadbraten K. Hypodontia in the permanent dentition. ASDC J Dent Child. 1973;40:115–17. [PubMed] [Google Scholar]
- 26.Jorgenson RJ. Clinician's view of hypodontia. J Am Dent Assoc. 1980;101:283–86. doi: 10.14219/jada.archive.1980.0186. [DOI] [PubMed] [Google Scholar]
- 27.Gahnen HJ. Hypodontia in the permanent dentition. Odontol Rev. 1965;7:77–78. [Google Scholar]
- 28.Brook AH. A unifying aetiological explanation for anomalies of human tooth number and size. Arch Oral Biol. 1984;29:373–78. doi: 10.1016/0003-9969(84)90163-8. [DOI] [PubMed] [Google Scholar]
- 29.Kjaer I, Kocsis G, Nodal M, Christensen LR. Aetiological aspects of mandibular tooth agenesis - Focusing on the role of nerve, oral mucosa, and supporting tissues. Eur J Orthod. 1994;16:371–75. doi: 10.1093/ejo/16.5.371. [DOI] [PubMed] [Google Scholar]
- 30.Amini F, Rakhshan V, Babaei P. Prevalence and pattern of hypodontia in the permanent dentition of 3374 Iranian orthodontic patients. Dent Res J (Isfahan) 2012;9:245–50. [PMC free article] [PubMed] [Google Scholar]
- 31.Lai PY, Seow WK. A controlled study of the association of various dental anomalies with hypodontia of permanent teeth. Pediatr Dent. 1989;11:291–96. [PubMed] [Google Scholar]