

Abstract
Background:
The transition from the International Classification of Disease-9th clinical modification to the new ICD-10 was all set to occur on 1 October 2015. The American Medical Association has previously been successful in delaying the transition by over 10 years and has been able to further postpone its introduction to 2015. The new system will overcome many of the limitations present in the older version, thus paving the way to more accurate capture of clinical information.
Methods:
The benefits of the new ICD-10 system include improved quality of care, potential cost savings, reduction of unpaid claims, and improved tracking of healthcare data. The areas where challenges will be evident include planning and implementation, the cost to transition, a shortage of qualified coders, training and education of the healthcare workforce, and a loss of productivity when this occurs. The impacts include substantial costs to the healthcare system, but the projected long-term savings and benefits will be significant. Improved fraud detection, accurate data entry, ability to analyze cost benefits with procedures, and enhanced quality outcome measures are the most significant beneficial factors with this change.
Results:
The present Current Procedural Terminology and Healthcare Common Procedure Coding System code sets will be used for reporting ambulatory procedures in the same manner as they have been. ICD-10-PCS will replace ICD-9 procedure codes for inpatient hospital services. The ICD-10-CM will replace the clinical code sets. Our article will focus on the challenges to execution of an ICD change and strategies to minimize risk while transitioning to the new system.
Conclusion:
With the implementation deadline gradually approaching, spine surgery practices that include multidisciplinary health specialists have to anticipate and prepare for the ICD change in order to mitigate risk. Education and communication is the key to this process in spine practices.
Keywords: Diagnostic coding systems, implementation, International Classification of Disease version 10, practice management, spine surgery
INTRODUCTION
The transition to the new International classification of disease version 10 clinical modification/procedure code system (ICD-10-CM/PCS) system has been mandated to now occur on 1 October, 2015. This is the first major change that will impact the healthcare industry that has occurred since the conversion to diagnosis-related groups (DRGs). The new system enables better documentation of disease states and complications, categorization of disease by community, and more specific tracking of healthcare outcomes. Resources can be allocated based on health patterns identified in the community, availability and the ability to provide continuity of care.
The advances that have occurred in medical technology along with the expansion of procedures have resulted in the need for a more specific diagnostic and procedural coding system. This transition to ICD-10-CM/PCS is a chance for the US healthcare system to more accurately collect treatment and outcomes data, ultimately improving the quality, cost, and type of healthcare required by a community.
Anticipating and preparing for the changes that will occur is an important step toward risk reduction.[4,5,12,13] A few of the steps include reviewing existing practice management billing software to ensure its ability to successfully transition to ICD-10, staff training, technology updates, avoiding fraud, waste, and abuse, appropriate self-regulations and reporting, ensuring compliance with third party vendors and payers, determining accurate clinical documentation to reflect the increased detail required by ICD-10-CM/PCS, and using third party entities to audit records for about 1 year into the transition. This enables the early identification of activity that might be considered fraudulent and ability to take action immediately.[3,6,14] A number of resources are available online with the American Medical Association (AMA), the American Association of Neurological Surgeons (AANS), and the North American Spine Society (NASS). Detailed courses during the annual meetings, as well as dedicated coding courses for spine surgeons take place throughout the year to provide appropriate education about surgical coding and reimbursements.
We discuss the challenges to successful execution, suggest some strategies to help mitigate risk in spine surgery practices.
METHODS
Challenges to the ICD-10 transition
There have been gradual and progressing efforts by both federal agencies, the public and private sector to help prepare for an easy transition to ICD-10-CM/PCS. This process began almost two decades ago, and is set to go into action beginning 1 October 2015. However, there are a few obstacles that have to be overcome prior to its final implementation and we will discuss each one below.[1]
Planning
Making the transition from ICD-9 to the ICD-10-CM/PCS system required developing a modification of the World Health Organization (WHO)-based version 10 for clinical application as the ICD-10-CM and, developing a modification for procedures, the ICD-10-PCS for use in the US. This by no means is a small undertaking This involves the need to hire contractors to test out the new system, conduct pilot studies, and perform cost benefit analyses on the effects of this transition. Additionally, ICD-10-CM/PCS has to be adopted as the new standard for Health Insurance Portability and Accountability Act (HIPAA), along with appropriate mapping of the old ICD-9 to the new ICD-10-CM/PCS and vice versa. It requires getting personnel trained to educate the workforce, an overhaul of the current coding courses, conversion of the MS-DRGs to ICD-10-CM/PCS, and getting this information out to hospitals, practices, and physicians using the AMA and various other specialty and sub-specialty organizations.
The transition to ICD-10-CM/PCS requires the release of new software taking these changes into account, thereby converting hundreds of payment systems to adapt to these code changes. Additionally frequent updates and efforts to reach a diverse group of caregivers are some of the factors that have to be considered in the transition to this new coding system.
Shortage of qualified coders
There is a lack of skilled coders that are available to educate and bring the personnel up-to-date with the change to ICD-10. Adequate training of the present workforce is essential. The organization has to understand the competencies of different coders and their ability to multi-task during the change, taking care to appropriately utilize these competencies. The organizations have to provide coders with adequate support during the transition and provide the opportunities to be recognized and excel in the changing environment. This would minimize attrition of the workforce and over a period of time, thus filling a gap in an area much in need over the next few years.
Workforce training and education
Organizations have to decide on the best way to train their personnel. Identifying a physician leader in the group is extremely helpful as physicians tend to respond better to their colleagues who have an understanding of this topic and can share their knowledge and communicate the necessity of better documentation and data collection. The result would mean enhanced coding accuracy, thereby providing information to improve healthcare practice. There is no need for physicians to be trained as coders; however, a physician leader may help others with the transition and its effective use.
The primary focus of physicians will always be the evaluation of their patients and a detailed documentation of their findings.[16] It is essential to make assessments and diagnoses, as well as carry out treatments based on their diagnoses. To effectively assist physicians in the transition, they would require training in tools designed to assist them at the point of care, enabling the capture of essential clinical information with adequate details for coders to select suitable and specific ICD-10-CM/PCS codes.[7] One method is to enable physicians to search for familiar, colloquial terms and phrases using the procedure-friendly terminology (PFT) resources in the electronic medical record software to help them code those terms in ICD-9 or ICD-10.
For example, a surgeon performing a procedure may describe removal of the L3 lamina., However, the PCS would define resection as “cutting off or out without replacement of a body part” whereas the definition of removal is “taking out or off a device from a body part” and the term excision is defined as “cutting out or off without replacement of a portion of a body part.” The spine surgeon may use these terms interchangeably and incorrectly, thus, education plays a key role in this transition. In addition, examples of revenue lost as a result of inadequate or incomplete documentation could be used for training physicians and other clinical staff.
Physician leaders can demonstrate the effectiveness of additional pieces of documentation that can boost the bottom line for the organization. This will help reduce the impact of lost productivity and will be a great benefit to help administrative staff carry out their responsibilities. The absence of appropriate entries will delay claims processing and, result in devoting a significant amount of time going through the entire process again [Figure 1]. Spine surgery groups will have to identify their leaders to communicate and train other colleagues during the ICD-10 transition.
Figure 1.

Incorrect procedural documentation beginning with the physicians/surgeon can lead to incorrect recognition and entry of code sets, resulting in errors in the APC or ICD codes for ambulatory and outpatient setting and DRGs for hospital inpatient setting. The result would be delayed, incorrect, or no reimbursement to the hospital. This, in turn, will get the surgeon queried, thus starting back at the top
Productivity and training
The anticipated time to train the staff members is about 16 h of training and 10 h of practice prior to clinical use of the new codes.[14,15] The potential for double billing exists during the transition from an ICD-9 to ICD-10 system, which may unintentionally create False Claims Act (FCA) violations. The shortage of well-trained coding professionals poses a risk, as General equivalence mapping (GEMs) do not provide a definitive equivalent mapping at the moment. The initial change will require a significant amount of manual review and will impact productivity during the initial transition.
RESULTS
The consequence of this transition is that ICD-10 conversions will need constant scrutiny and a manual check due to the significant differences in language and structure between ICD-9 and ICD-10. Hence, this is not an easy software vendor fix, but the conversion will be effective and require professionally trained clinical coders and physicians who are cognizant and available to work as a team and complete the task at hand. With the hospital focusing on making process changes in almost every other area [Figure 2], educating and training personnel and updating software, detailed documentation, and an accurate understanding of the relationship of documentation ICD-10-CM/PCS would go a long way in helping hospitals maintain productivity and reimbursement during the transition.
Figure 2.

Non-directional cycle representing the inter-relationships resulting from changes in documentation and billing, education and training required among all the key players in the hospitals/ambulatory service centers and practices
Centers for Medicare and Medicaid Services (CMS) has estimated an initial loss of revenue and increased denial of claims for 2 years following the implementation of ICD-10. Additionally, the rate of claims errors is estimated to increase to about 6-10% from the present 3% with ICD-9. In order to prepare and minimize these losses on initiation of the change to ICD-10, it is critical that hospitals and practices plan ahead for this change. It will be necessary for organizations to budget for diminished cash flow and prepare for delayed claims and adjudication. It is necessary that software and Electronic medical record (EMR) vendors are on board with updates in software and the ability to convert and test their systems well in advance. There will be delays due to educating the workforce and getting them up to speed with these changes, and budgets for educational expenses have to be kept aside and appropriately allocated. There will be a need to vigilantly track denials and reporting critical issues. It will be essential to staff the services appropriately in order to handle the increased workload through the transition.
The impact can be minimized by making sure that physicians, spine surgeons focus on good documentation and are up-to-date with the requirements and details. The guidelines indicate that providers have to be thorough and complete in their documentation, as this will directly affect coding, billing, and in turn re-imbursements. There has to be collaboration between the spine surgeon, payer and, CMS in order to perfect payments and mapping of these codes. This is important in hospital based spine surgical practices, private spine surgeon led group or solitary practices and ambulatory surgical centers. Inventories and resources are to be managed with care in order to avoid unnecessary costs and expenses. It is essential that immediate work is performed on all denials and learning from these errors to increase first time payoffs and assertively manage denials and write-offs.
Manchikanti et al. in their publications on the topic provide some illustrative examples of the effect of the code changes on conditions like spondylosis, used to describe facet arthropathy in their pain practice.[8,9,10,11] In addition, they provide descriptions for the changes in codes for cervical, thoracic, and lumbosacral spondylosis with and without myelopathy. One ICD-9 code associated with these conditions will, in the future, have about nine or more associated codes in the ICD-10 system. The specific details of these new codes have to be studied, as they now include laterality, exact location in the spinal column, along with associated symptoms. A case example of the specificity of ICD-10-PCS in spine surgery is provided [Appendix 1], and the details of coder queries and the methodology in coding are described [Figure 3].
Figure 3.
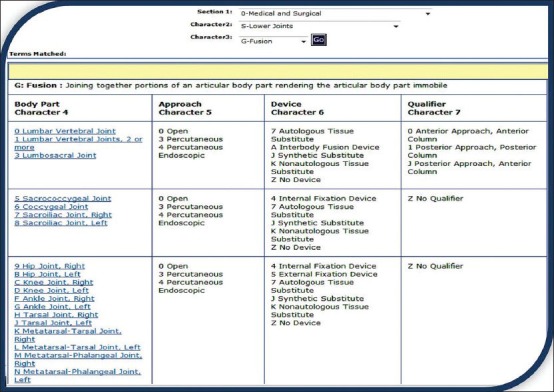
This image illustrates the coding screen for entering the ICD-10-PCS codes. All seven characters must be specified to be a valid code. If the documentation is incomplete for coding purposes, the surgeon should be queried for the necessary information. Within a PCS table, valid codes include all combinations of choices in characters 4 through 7 contained in the same row of the table. In the example shown, 0SG13A1 is a valid code and 0SG5AZ is not a valid code. The surgeon does not need to use the terms in the PCS description and does not need to be queried if the documentation is clear
DISCUSSION
There are undoubted benefits to the transition from ICD-9 to ICD-10-CM/PCS. The ability to more accurately pay for newer procedures with fewer fraudulent and rejected claims will save the system a significant amount in the long term. There would be minimal error with this new system with decreased errors, rejections, and improper paperwork. The potential advantages and disadvantages have been detailed in separate tables in part I of this paper.
Success for organizations during the transition is initially highly dependent on correct coding. Inaccurate coding would mean denial of reimbursements, prolonged periods of scrutiny into the healthcare records and downstream processes. This can be avoided initially by having well-trained coders; however, this will not be enough if physician documentation is inadequate or inaccurate. It is essential to get all spine physicians and surgeons on board and engage them in the process of this transition. Important strategies include making a case about the relevance of good documentation, finding a physician leader or champion to help support and guide other physician colleagues and, avoid trying to convert physicians into coders.[2]
The ICD-9 was initially published by the WHO in 1978 and the ICD-10 in 1992, resulting in the use of an outdated framework whose main role is to bill patients. There is no means of comparing data on an international platform for morbidity or mortality. There would be increased parity between the health record and the ICD-10 coding data, enabling appropriate classification of data. In turn, this would result in better disease identification within communities and appropriate allocation of funding to the communities in need. The potential to use this data to develop to discover previously unknown relationships could be enormous. The US healthcare is a trillion dollar industry, with even small potential changes giving rise to savings of millions of dollars. Every industry undergoes a process of quality improvement, continuously measured in terms of input and output. Until now, the healthcare sector has been unable to measure this metric, but with this change, these metrics can now be used to plan for positive long-term change. The transition to ICD-10-CM/PCS will, without a doubt, enhance our understanding of the health of the population across the US and the impact of the medical and surgical care they receive. The question remains as to how smoothly and cost effectively this transition is made and the most effective ways to utilize this enormous resource of data.
CONCLUSION
A team-based approach with physician leaders plays a key role in the path to change from the old ICD-9 to new ICD-10-CM/PCS coding system. Spine surgeons and coders need to work together to identify the most appropriate codes. The accurate detailing of spine procedures, devices inserted, implant types, clear delineation of approach, laterality, and body part will go a long way in making this transition easier. Preparation is the key to a smooth transition.
APPENDIX I
An illustrative example is presented discussing the role of the surgeon and documentation required to enable coders to appropriately enter ICD-10 codes.
ILLUSTRATIVE EXAMPLE SPINE FUSION
The surgeon can clarify queries of the coder based on the complexity of the case and documentation
Procedure: Posterior Lumbar Decompression via Laminectomy facetectomy L5-S1 w Interbody Cage Placement, Autologous Iliac Crest Autograft, Posterolateral Arthrodesis, Interbody Arthrodesis, Nonsegmental Pedicle Screw-Rod Fixation via Frameless Spinal Stereotactics.
Learning
Root, Device, Qualifier, Coding Guidance.
Questions
Does a decompression laminectomy release the spinal cord or the nerve root?
Should the excision of the vertebral bone (laminectomy) be coded in addition to the release code?
Was an interbody fusion device used or other device? Can you explain the cage placement and later interbody arthrodesis?
7-Autologous Tissue Substitute
A-Interbody Fusion Device
J-Synthetic Substitute
K-Nonautologous Tissue Substitute
Z-No Device.
After a fusion of the spine, the surgeon adds internal fixation/spinal stabilization devices for further stability. Listed below are the choices:
-
0SG (insertion-joint)
- B-Spinal Stabilization Device, Interspinous Process
- C-Spinal Stabilization Device, Pedicle-Based
- D-Spinal Stabilization Device, Facet Replacement
- 4-Internal Fixation Device
- 8-Spacer.
-
Fusion codes require identification of posterior or anterior approach along with the posterior column or the anterior column information:
- 0-Anterior Approach, Anterior Column
- 1-Posterior Approach, Posterior Column
- J-Posterior Approach, Anterior Column.
Codes
0SG30A1: Fusion of Lumbosacral Joint with Interbody Fusion Device, Posterior Approach, Posterior Column, Open Approach interbody cage placement
00NY0ZZ: Release Lumbar Spinal Cord, Open Approach
(laminectomy/facetectomy) (part of release – do not code)
0SH30CZ: Insertion Lumbosacral Joint, Spinal Stabilization Device, Pedicle-Based, Open Approach
0QB20ZZ: Excision of Right Pelvic Bone, Open Approach (excision iliac for bone graft).
Coding Guidance
Fusion procedures of the spine
B3.10a
The body part coded for a spinal vertebral joint(s) rendered immobile by a spinal fusion procedure is classified by the level of the spine (e.g. thoracic). There are distinct body part values for a single vertebral joint and for multiple vertebral joints at each spinal level.
Example: Body part values specify Lumbar Vertebral Joint, Lumbar Vertebral Joints, 2 or more and Lumbosacral Vertebral Joint.
B3.10b
If multiple vertebral joints are fused, a separate procedure is coded for each vertebral joint that uses a different device and/or qualifier.
Example: Fusion of lumbar vertebral joint, posterior approach, anterior column and fusion of lumbar vertebral joint, posterior approach, posterior column are coded separately.
B3.10c
Combinations of devices and materials are often used on a vertebral joint to render the joint immobile. When combinations of devices are used on the same vertebral joint, the device value coded for the procedure is as follows:
If an interbody fusion device is used to render the joint immobile (alone or containing other material like bone graft), the procedure is coded with the device value Interbody Fusion Device.
If bone graft is the only device used to render the joint immobile, the procedure is coded with the device value Nonautologous Tissue Substitute or Autologous Tissue Substitute.
If a mixture of autologous and nonautologous bone graft (with or without biological or synthetic extenders or binders) is used to render the joint immobile, code the procedure with the device value Autologous Tissue Substitute.
Examples: Fusion of a vertebral joint using a cage style interbody fusion device containing morselized bone graft is coded to the device Interbody Fusion Device.
Fusion of a vertebral joint using a bone dowel interbody fusion device made of cadaver bone and packed with a mixture of local morselized bone and demineralized bone matrix is coded to the device Interbody Fusion Device.
Fusion of a vertebral joint using both autologous bone graft and bone bank bone graft is coded to the device Autologous Tissue Substitute.
Excision for graft
B3.9
If an autograft is obtained from a different body part in order to complete the objective of the procedure, a separate procedure is coded.
Example: Coronary bypass with excision of saphenous vein graft, excision of saphenous vein is coded separately.
Release procedures
B3.13
In the root operation Release, the body part value coded is the body part being freed and not the tissue being manipulated or cut to free the body part.
Example: Lysis of intestinal adhesions is coded to the specific intestine body part value.
Per ICD-10-PCS - Applied Approach, the root operation of release is used when a vertebra is excised or cut (such as a Laminectomy, Hemi-laminectomy or a Laminotomy) to free a compressed nerve rather than the root operation Excision.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2014/5/4/192/137182
Contributor Information
Gazanfar Rahmathulla, Email: Rahmathulla.Gazanfar@mayo.edu.
H. Gordon Deen, Email: Hdeen@mayo.edu.
Judith A. Dokken, Email: Dokken.Judith@mayo.edu.
Stephen M. Pirris, Email: Pirris.Stephen@mayo.edu.
Mark A. Pichelmann, Email: Pichelmann.Mark@mayo.edu.
Eric W. Nottmeier, Email: enottmeier@icloud.com.
Ronald Reimer, Email: Reimer.Ronald@mayo.edu.
Robert E. Wharen, Jr, Email: Wharen.Robert@mayo.edu.
References
REFERENCES
- 1.5 steps for a smooth transition to ICD-10. Med Econ. 2012;89:22. [PubMed] [Google Scholar]
- 2.Bielby JA. Coding with integrity. J AHIMA. 2013;84:28–32. [PubMed] [Google Scholar]
- 3.D’Amato C, D’Andrea R, Bronnert J, Cook J, Foley M, Garret G, et al. Planning organizational transition to ICD-10-CM/PCS. J AHIMA. 2009;80:72–7. [PubMed] [Google Scholar]
- 4.D’Amato C, D’Andrea R, Bronnert J, Cook J, Foley M, Garret G, et al. Transitioning ICD-10-CM/PCS data management processes. J AHIMA. 2009;80:66–70. [PubMed] [Google Scholar]
- 5.Diamond F. Anti-fraud efforts turn to prevention. Manag Care. 2013;22:29–32. [PubMed] [Google Scholar]
- 6.Hartman K, Phillips SC, Sornberger L. Computer-assisted coding at the Cleveland Clinic: A strategic solution. Addressing clinical documentation improvement, ICD-10-CM/PCS implementation, and more. J AHIMA. 2012;83:24–8. [PubMed] [Google Scholar]
- 7.Hirsch JA, Falco FJ, Manchikanti L. Necessity and implications of ICD-10: Facts and fallacies. Pain Physician. 2012;15:E153. [PubMed] [Google Scholar]
- 8.Hirsch JA, Manchikanti L. Response to ready or not! Here comes ICD-10. J Neurointerv Surg. 2013;5:621. doi: 10.1136/neurintsurg-2012-010325. [DOI] [PubMed] [Google Scholar]
- 9.ICD-10 means better documentation is a must. Hosp Case Manag. 2013;21:113–4. [PubMed] [Google Scholar]
- 10.Manchikanti L, Falco FJ, Hirsch JA. Necessity and implications of ICD-10: Facts and fallacies. Pain Physician. 2011;14:E405–25. [PubMed] [Google Scholar]
- 11.Manchikanti L, Falco FJ, Hirsch JA. Ready or not! Here comes ICD-10. J Neurointerv Surg. 2013;5:86–91. doi: 10.1136/neurintsurg-2011-010155. [DOI] [PubMed] [Google Scholar]
- 12.Piselli C. What's your ICD-10 plan? Findings and recommendations from research on ICD-10 implementation. J AHIMA. 2005;76:34–7. [PubMed] [Google Scholar]
- 13.Rose AD. Transitioning a physician practice to ICD-10. J AHIMA. 2012;83:70–2. [PubMed] [Google Scholar]
- 14.Sanders TB, Bowens FM, Pierce W, Stasher-Booker B, Thompson EQ, Jones WA. The road to ICD-10-CM/PCS implementation: Forecasting the transition for providers, payers, and other healthcare organizations. Perspect Health Inf Manag. 2012;9:1f. [PMC free article] [PubMed] [Google Scholar]
- 15.Sullivan T. Budgeting for ICD-10. J AHIMA. 2010;81:30–3. [PubMed] [Google Scholar]
- 16.Wiedemann LA. Strategizing clinical documentation improvement. J AHIMA. 2013;84:52–3. [PubMed] [Google Scholar]