

Abstract
Purpose
To examine time-varying associations between predictors of recent multiple sexual partners from middle adolescence through young adulthood.
Methods
We examined whether the odds of multiple partners in the past year were differentially predicted by substance use and depression over time, using data from a nationally representative longitudinal study (N=11,963, 52.2% female, 18.3% African American, 11.9% Hispanic, 3.5% Asian, 2.6% other race, M age at Wave 1=16.1 years, SD=1.8). Data were analyzed using the time-varying effect model, which estimates associations between predictors and an outcome as a function of near-continuous time.
Results
The proportion of participants having multiple partners increased over time, leveling off at around 30% after age 20. Significant positive associations between substance use and multiple partners were strongest early in adolescence, and decreased sharply by around age 18. The significant positive association between depression and sexual behavior weakened with age, remaining significant in young adulthood for women, but not men.
Conclusions
These findings suggest that factors associated with having multiple recent sexual partners change from middle adolescence through young adulthood. The time-varying effect model can be used to identify risk factors that are especially salient at different ages, thus identifying which age periods may hold the greatest promise for intervention.
Keywords: Sexual behavior, adolescents, young adults, time-varying effect model
Introduction
Sexual behavior varies by age in prevalence, risks and correlates. By age 15, few individuals have engaged in sexual intercourse; by the mid-twenties it is a near-universal experience [1]. Predictors of, and, by extension, the most efficacious methods for prevention of, risky sexual behaviors likely vary over time. However, although longitudinal research on sexual behavior has expanded in recent years, there have been few studies that examine how the relevance of predictors of sexual behavior changes by age [2]. Such research determine age periods during which particular risk factors are most strongly linked to sexual behavior, and identify mediators to target in prevention programs at different ages. In this study, we demonstrate the utility of the time-varying effect model (TVEM) to uncover how correlates of sexual behaviors vary over time. Specifically, we examine how the associations between substance use and depression and multiple sexual partners differ from middle adolescence into young adulthood, using data from the National Longitudinal Study of Adolescent Health (Add Health).
Having a greater number of sexual partners is associated with risk of sexually transmitted infections (STIs). Of particular risk are concurrent (more than one partner during the same time period) or sequential (non-overlapping partners occurring close together in time) partners, as individuals may not show symptoms of an STI before passing it to another partner [3]. Concurrency of partners is a better predictor of STIs than number of partners alone [4]; furthermore, research from Add Health suggests that both concurrent and multiple sequential sexual partnerships in the last 18 months predicts STI risk over and above that of total lifetime partners [3]. Although research has demonstrated that rates of STI increase through the teens and peak in the mid-twenties [5], little is known about how the potential influence of various risk factors changes with age. Thus, we examine whether certain factors are most strongly linked to multiple recent partners at different ages.
Researchers have identified several predictors of multiple sexual partners. For example, use of substances, including alcohol, tobacco and marijuana, is associated with more partners or increased odds of multiple partners in adolescents and young adults [6–12]. Similarly, experiencing more depressive symptoms is associated with a greater number of sexual partners during adolescence and young adulthood [13–15]. Several studies have shown associations between substance use and depression and multiple partners for both male and female adolescents [7, 9, 14, 15], although some research has found that depressive symptoms only predict multiple partners for female adolescents [16], and that different substances may differentially predict number of partners by gender and race/ethnicity [12]. However, this research uses samples of adolescents and young adults at different ages, providing only snapshots of different periods. Reviewing the literature can give some sense of whether similar factors predict sexual behavior in individuals of different ages; for example, one review paper suggests that a history of problems (i.e., substance use, delinquency, depression) was a more consistent predictor of sexual behavior in early compared to middle or late adolescence [2]. However, variations between studies make it difficult to determine whether these are due to age differences or study design.
Relatively little research has examined, in a single study, rates and correlates of any aspect of sexual behavior in individuals of different ages. A recent national, cross-sectional study found that rates of sexual activity increase from adolescence to adulthood, whereas rates of condom use decrease [1, 17]. A few older studies examined having multiple partners at different ages. A national study of adults found that having multiple partners decreases over time, with 32% of 18–24 year-olds, 22.5% of 25–29 year-olds and 18.5% of 30–34 year olds having two or more partners in a given year [18]. However, these figures don’t account for marital status, which could greatly reduce odds of multiple partners, and do not include individuals under age 18. Another study found no significant difference in odds of recent multiple partners by age among 14–22 year-olds. However, this analysis examined only sexually active individuals; thus, because a larger number of younger adolescents have no sexual partners, the results may not represent the entire adolescent population [9]. In addition, a few studies have examined age as a moderator of the association between risk factors and sexual behaviors. For example, depression predicted odds of multiple partners similarly for 14–19 and 20–25 year old individuals, but only predicted condom use for the older group [19]. Research from Add Health has shown that associations between self-esteem and depression on sexual initiation vary by age, with higher self-esteem predicting sex in older adolescent boys, and higher depressive symptoms more strongly predicting sex in younger compared to older adolescent girls [20].
Such an understanding of the age-graded differences in predictors of sexual behavior is critical for both understanding sexual development and informing effective interventions to reduce sexual risk behaviors. However, changes in correlates of sexual behavior likely unfold in a more continuous fashion over time, rather than in discrete stages. Thus, grouping individuals by age, as has been done in most prior studies, may obscure important but nuanced shifts that occur as adolescents develop. Using an approach that examines associations between predictors and sexual behavior in continuous time enables researchers to systematically test periods in which particular factors are associated with sexual behavior and identify periods of particular risk upon which to intervene. Methods now exist to examine such changes as they unfold in continuous time.
One such approach is TVEM [21–22]. TVEM flexibly estimates how the association between a predictor and an outcome (e.g., heavy episodic drinking and multiple partners) differs over continuous time (e.g., from age 14 to age 32) without assuming the association follows a parametric function of time. Note that the term “effect” in this context refers to a regression coefficient, not a casual effect. In this study we use logistic TVEM, a variant of TVEM for binary outcomes [23–24], to test how substance use and depressive symptoms differ in their associations with multiple partners from age 14 to 32. In summary, we test the following:
How do rates of reporting multiple sexual partners in a given year change by age from middle adolescence to young adulthood, and how do these rates differ by gender?
How do substance use and depression differentially predict multiple sexual partners from middle adolescence through young adulthood, and how do these associations differ by gender?
Methods
Participants and Procedures
Data are from the contractual sample of Add Health [25]. Eighty high schools and associated middle schools were sampled, employing a clustered sampling design and survey weights to ensure that the sample was representative of schools in the United States with respect to region, urbanicity, school type and size, and ethnicity. Data collection was approved by the Public Institutional Review Board (IRB) at the University of North Carolina, and we received approval from the Penn State IRB to analyze Add Health data. Participants initially completed in-school and in-home interviews in 1994–1995 (Wave I), when they were in 7th through 12th grade. Follow-up in-home interviews occurred during 1995–1996 (Wave II; 12th graders not interviewed), 2001–2002 (Wave III) and 2007–2008 (Wave IV). We included only individuals from the core sample, which was designed to obtain a representative sample of the school-age population and is essentially self-weighting [25]. Our resulting sample contained 11,963 individuals (52.2% female, 18.3% African American, 11.9% Hispanic, 3.5% Asian, 2.6% other race, M age at Wave I=16.1 years, SD=1.8).
About 80% of participants from the Wave I sample participated in each of the later waves. We include person-waves of data from any measurement occasion in which an individual completed data on the relevant outcome and predictors, regardless of later attrition, as TVEM can handle different numbers and spacing of measurement occasions. However, we excluded all measurement occasions where an individual was married, as correlates of multiple partners may be different for married individuals. In addition, we restricted the data to occasions collected after age 14 and prior to age 32, due to the sparseness of data outside this range. Thus, we included 31,485 person-waves of data. Age in months was used as the time variable in analyses.
Measures
Outcome
Our primary outcome was Multiple Partners, a measure of whether an individual engaged in sexual behavior with more than one partner in the past year. At At Waves I and II, this measure was computed using two measures. First, participants were asked whether they engaged in series of behaviors with up to three relationship partners they have named previously, including “We had sexual intercourse.” This was followed by the item: “In addition to {____} and anyone whose initials you gave as a romantic relationship partner, have you had a sexual relationship with anyone else?” At Wave III, participants reported: “With how many different partners have you had vaginal intercourse in the past 12 months?” At Wave IV, participants were asked “Considering all types of sexual activity, with how many male/female partners have you had sex in the past 12 months?” about both their male and female partners; only opposite-sex partners were included to make the measures more comparable across waves. Scores were dichotomized (0=0–1 partner, 1=2+ partners). Across the study, multiple partners in the past year were reported on about 23% of occasions.
Predictors
We examined 4 time-varying risk factors for sexual behavior. Heavy Episodic Drinking (HED) at any time in the past year was dichotomized from an item asking about frequency of heavy drinking (4 or 5 drinks for females and males, respectively, except at W1 where 5 drinks was asked for all participants); HED was reported on 36% of occasions. Marijuana use in the 30 days was dichotomized from an item asking about frequency of marijuana use (reported on 17% of occasions). Any Smoking in the past month was dichotomized from an item asking how often they smoked cigarettes in the past month; any smoking was reported on 31% of occasions. Depressive Symptoms is a sum score of a subset of 9 items that parallel items in the Center for Epidemiological Studies Depression Scale (CES-D) [25]. A sample item was “You felt sad,” and items were rated in a 0–3 scale from Never/rarely to Most/all of the time (M=0.6, SD=0.5). The variable was standardized for ease of interpretation.
Statistical analyses
We used logistic TVEM to examine how four predictors were associated with odds of multiple partners over time (i.e., from ages 14–32). First, we ran intercept-only models to estimate rates of multiple partners by age separately for male and female participants. We then estimated how HED, marijuana, tobacco, and depressive symptoms were associated with multiple partners in four separate models. Models were run separately by gender to allow for time-varying gender differences. Because all predictors were assessed at all waves, we estimated time-varying coefficients of time-varying predictors. In each analysis, we also controlled for race/ethnicity with 4 dummy-coded variables (Hispanic/Latino (HL), non-HL Black, non-HL Asian, non-HL other, with non-HL White as the reference group) entered as time-invariant predictors. All TVEMs were fit using the logistic_TVEM SAS macro, which is available for download at methodology.psu.edu [21]. Note that results are presented as figures, as time-varying coefficients are estimated in continuous time leading to a number of coefficients too large to present in tables.
Results
Figure 1 shows results for intercept-only models, which examine how rates of reporting multiple partners changes with age for male and female participants. Each solid curve indicates the estimated percentage of participants who reported multiple partners in a given year at every age between 14 and 32 in continuous time. For example, for both male and female participants, about 5% reported multiple partners at age 14, whereas about 30% reported multiple partners at age 21. Dotted lines indicate 95% confidence intervals. Between ages 14 and 25 male and female adolescents were equally likely to have multiple partners. However, between ages 25 and 29, men had greater odds of multiple partners than women (as determined by the non-overlapping confidence intervals in Figure 1); at age 27 nearly 40% of men had multiple partners, compared to 30% of women. This difference disappeared by age 30.
Figure 1.
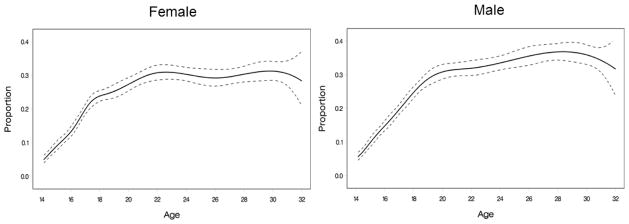
Proportion of individuals having multiple sexual partners in the past year from age 14 to age 32, estimated by an intercept-only TVEM. Dotted lines indicate 95% confidence intervals. The x-axis is labeled with age in years for clarity of presentation; age in months was used in analyses.
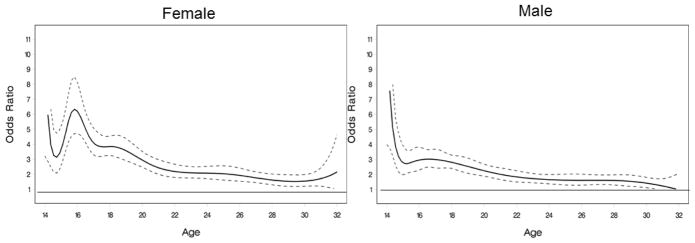
Figures 2–5 show the results of analyses examining associations between other risk factors and multiple partners. As associations are presented as odds ratios, confidence intervals not containing 1 indicate a significant association between the predictor and outcome at a particular age. HED is a significant predictor of multiple partners for female participants at all ages, and for male participants prior to age 31 (Figure 2). However, this association differs in strength by age: at age 14, individuals who had engaged in HED were 5.5 times (male) or 7 times (female) more likely to have multiple partners, whereas by age 24, individuals who had engaged in HED had only 2 times greater odds of having multiple partners. Patterns by age were similar for male and female participants, apart from a short period around age seventeen when the association between HED and multiple partners was slightly stronger for female participants.
Figure 2.
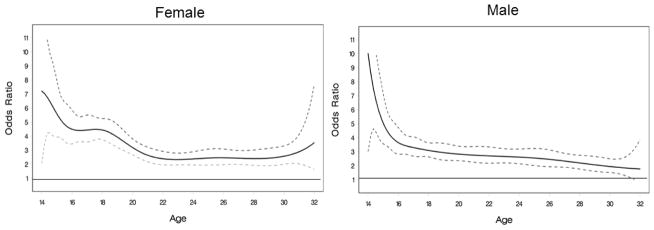
TVEM showing heavy episodic drinking predicting past year multiple sexual partners from age 14 to age 32. Dotted lines indicate 95% confidence intervals. The x-axis is labeled with age in years for clarity of presentation; age in months was used in analyses.
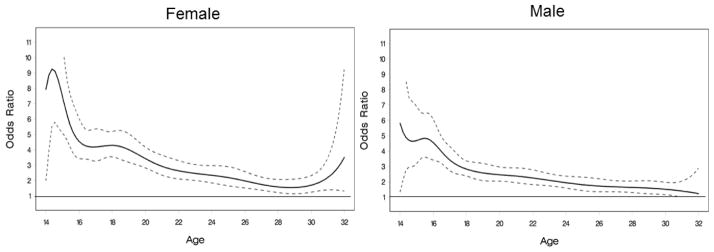
Figure 5.
TVEM showing past year depressive symptoms predicting past year multiple sexual partners from age 14 to 32. Dotted lines indicate 95% confidence intervals. The x-axis is labeled with age in years for clarity of presentation; age in months was used in analyses.
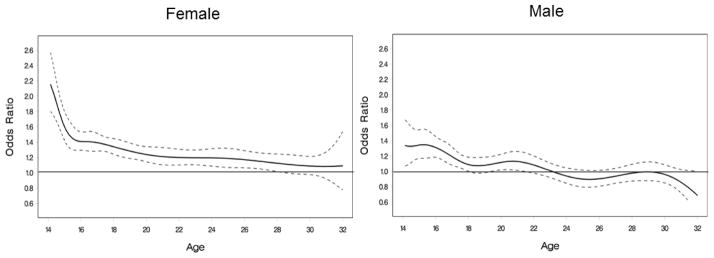
Results were similar for marijuana use and smoking (Figures 3–4). The association between use of these substances and multiple partners decreased over time, although it remained significant. There were also significant gender differences between ages 16 and 18 for smoking and 17 and 20 for marijuana, where associations were stronger for female compared to male participants.
Figure 3.
TVEM showing marijuana use predicting past year multiple sexual partners from age 14 to age 32. Dotted lines indicate 95% confidence intervals. The x-axis is labeled with age in years for clarity of presentation; age in months was used in analyses.
Figure 4.
TVEM showing cigarette smoking predicting past year multiple sexual partners from age 14 to age 32. Dotted lines indicate 95% confidence intervals. The x-axis is labeled with age in years for clarity of presentation; age in months was used in analyses.
Figure 5 presents the association between depression and multiple partners. This association declined over time, and was moderated by gender. At age 14, adolescent girls had a stronger association between multiple partners and depressive symptoms than boys (OR 2.2 v. 1.3). The association between multiple partners and depressive symptoms declined for both male and female participants. Associations were statistically significant for male participants through age 18, with a brief period of significance at age 20. For female participants this association remained significant through age 29.
Discussion
This study demonstrates the utility of examining time-varying predictors of sexual behavior by showing that the associations between risk factors and having multiple partners change—gradually at some ages and rapidly at others—over developmental time. In general, odds of multiple partners increase sharply throughout the teens, plateauing by the early twenties, when about 30% of individuals had more than one sexual partner in a given year. However, associations between substance use and depressive symptoms and odds of multiple partners became weaker by age. This suggests that in early and middle adolescence, having multiple partners may be part of a syndrome of problem behaviors [27]. However, as sexual behavior becomes more normative in late adolescence and early adulthood, risky sexual behaviors may frequently occur separately from other problem behaviors and negative mental health outcomes. This decoupling of multiple partners and other risk behaviors in young adulthood reflects that although having multiple partners may be associated with STI risk at any age, it may not be viewed as being problematic to the same extent in young adulthood compared to adolescence. Thus, prevention programs aimed at multiple problem behaviors may be effective in early and middle adolescence. However, in late adolescence and early adulthood, different types of risk behaviors may be more distinct, and require different strategies for intervention. For example, in adolescence, a general program to promote positive development may guard against a variety of problem behaviors, whereas in young adulthood, programs focusing specifically on aspects of sexual health, such as those relating to partner negotiation, condom use and STI risk may be more effective. In this study no predictors were more strongly associated with multiple partners at later ages. This may be due in part to the fact that some risk factors that may be more relevant for emerging adults were not measured at earlier waves. As this study only examined a small number of variables, future studies should examine the time-varying associations between sexual behavior and additional potential correlates, including factors related to healthy relationship functioning, which may be more important predictors in early adulthood.
We also examined gender differences in odds and predictors of multiple partners, and found that most predictors operated similarly for male and female participants. However, there are a few noteworthy differences. First, men were significantly more likely to have multiple partners in a given year between ages 25 and 29. This difference may suggest actual differences in behavior at this age, such as a greater acceptability of having sex outside a committed relationship in adulthood for men compared to women. However, research has documented biases that may be associated with over-reporting in men [28]. Thus, these differences may be due to reporting, rather than behavior. Second, although there was a drop in the strength of the association between substance use and multiple partners for both male and female participants over time, there was one period during which the association was stronger for young women: between about age 17 and 20. This stronger association may be because sex with multiple partners is more acceptable for men than women [29], and thus women engaging in sex with multiple partners are also likely to be involved with other deviant behavior. Sexual behaviors are likely seen as more problematic for both male and female early- to mid-adolescents; however, sex with multiple partners may become more socially acceptable for men at an earlier age than for women. However, this gender difference disappears by age 20, perhaps suggesting that sex is viewed as being less deviant for women after that age.
Finally, depressive symptoms were only associated with multiple partners for male participants in adolescence, whereas this association remained for female participants into the late twenties. Women with high levels of depressive symptoms may be more likely to use sex with multiple partners to seek comfort or avoid negative feelings, or may lack self-efficacy to refuse sexual behaviors [16]. However, because our predictor and outcome variables were assessed in the same measurement occasion, it is possible the directionality is reversed: women who have multiple partners are more depressed compared to men who have multiple partners. This is consistent with research suggesting that transitioning to sexual behavior is associated with depressive symptoms for female, but not male adolescents [30–31]. Findings are also consistent with sexual double standards, which suggest sexual behavior is more shameful for women, and thus more likely to cause distress [29]. However, because these time-varying associations do not assess causality, caution should be taken in interpretation. Methods for causal inference using observational data are now being adopted more broadly, [32–33], and incorporating such methods in TVEM is an important area for future research.
There are several other limitations to this study that provide areas for future research. First, the measurement of several variables changed slightly over the multiple waves of this study, including how number of partners was measured and the gender-specific definition of heavy episodic drinking. Although the variables were recoded in such a way as to make them as similar as possible, results must be interpreted with caution, as some observed differences may be due to changes in the measures rather than changes over time. Researchers should be sensitive to the possibility of this kind of analysis when designing their studies and endeavor to keep their measures consistent across measurement occasions. In addition, because participants of different ages were included in the first wave of the study, no single participant had data from the entire age range, meaning there may be cohort effects. The age range originally sampled was relatively small (approximately 6 years), limiting these cohort effects; however, this should be kept in mind when interpreting results. Our measure of multiple partners referred to a relatively long period of time (one year). Although research has found that having multiple partners during such a relatively long period to be associated with greater STI risk compared to those with a single partner [3] for some individuals, this may represent moving from one committed relationship to another, perhaps with adequate time and STI testing between partners, and thus may not carry substantial health risk. Future studies should examine whether results are similar with a shorter timeframe (e.g., 3 months), as has been used in other studies of multiple partners in adolescence [9]. As in most studies of sexual behavior, this study used self-report measures, and it is possible that some changes observed over time were due to age-related changes in reporting behaviors. Finally, we used a single, dichotomous measure of one aspect of sexual behavior, and other factors also play a role. For example, individuals who have multiple partners, but use a condom, may not be at increased risk compared to individuals who have unprotected sex. We also did include information about concurrency of sexual partners, the relationship context of sexual behaviors, or about sexual behavior with same-sex partners. Future research should examine other aspects of sexual behavior, such as condom use, concurrent partnerships and sex with non-relationship partners and how these change by age. Despite these limitations, this study provides a demonstration of a new method, TVEM, which has potential for enhancing our understanding of age-varying associations between sexual and other adolescent risk behaviors.
Implications and Contribution.
Although sexual behavior changes across adolescence and early adulthood, little is known about how predictors of sex change by age. Results show that the associations between substance use and depression and recent multiple sexual partners weakens over time. Programs targeting these factors hold greater promise for the prevention of sexual risk behavior earlier in adolescence.
Acknowledgments
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis. This research and the authors were supported by grants 2T32DA 017629 and P50-DA010075-15 from the National Institute on Drug Abuse (NIDA). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIDA, NICHD, or the National Institutes of Health. We thank Amanda Applegate for comments on a prior version of this manuscript.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Herbenick D, Reece M, Schick V, et al. Sexual behavior in the United States: Results from a national probability sample of men and women aged 14–94. J Sex Med. 2010;7(5 suppl):255–265. doi: 10.1111/j.1743-6109.2010.02012.x. [DOI] [PubMed] [Google Scholar]
- 2.Zimmer-Gembeck MJ, Helfand M. Ten years of longitudinal research on U.S. adolescent sexual behavior: Developmental correlates of sexual intercourse, and the importance of age, gender and ethnic background. Developmental Review. 2008;28(2):153–224. [Google Scholar]
- 3.Kelley S, Borawski E, Flocke S, et al. The role of sequential and concurrent sexual relationships in the risk of sexually transmitted diseases among adolescents. J Adolesc Health. 2003;32(4):296–305. doi: 10.1016/S1054-139X(02)00710-3. [DOI] [PubMed] [Google Scholar]
- 4.Rosenberg MD, Gurvey JE, Adler N, et al. Concurrent sex partners and risk for sexually transmitted diseases among adolescents. Sex Transm Dis. 1999;26:208–12. doi: 10.1097/00007435-199904000-00004. [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2011. Atlanta, GA: U.S. Department of Health and Human Services; 2012. [Google Scholar]
- 6.Baskin-Sommers A, Sommers I. The co-occurrence of substance use and high-risk behaviors. J Adolesc Health. 2006;38(5):609–11. doi: 10.1016/S1054-139X(02)00710-3. [DOI] [PubMed] [Google Scholar]
- 7.Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, et al. Number of sexual partners and associations with initiation and intensity of substance use. AIDS Behav. 2011;15(4):869–74. doi: 10.1007/s10461-010-9669-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Graves KL, Leigh BC. The relationship of substance use to sexual activity among young adults in the United States. Fam Plann Perspect. 1995;27(1):18–22. 33. doi: 10.1007/s10461-010-9669-0. [DOI] [PubMed] [Google Scholar]
- 9.Santelli JS, Brener ND, Lowry R, et al. Multiple sexual partners among U.S. adolescents and young adults. Fam Plann Perspect. 1998;30(6):271–5. [PubMed] [Google Scholar]
- 10.Shrier LA, Emans SJ, Woods ER, et al. The association of sexual risk behaviors and problem drug behaviors in high school students. J Adolesc Health. 1997;20(5):377–83. doi: 10.1016/S1054-139X(96)00180-2. [DOI] [PubMed] [Google Scholar]
- 11.Tubman JG, Windle M, Windle RC. Cumulative sexual intercourse patterns among middle adolescents: Problem behavior precursors and concurrent health risk behaviors. J Adolesc Health. 1996;18 (3):182–191. doi: 10.1016/1054-139X(95)00128-F. [DOI] [PubMed] [Google Scholar]
- 12.Valois RF, Oeltmann JE, Waller J, et al. Relationship between number of sexual intercourse partners and selected health risk behaviors among public high school adolescents. J Adolesc Health. 1999;25(5):328–35. doi: 10.1016/s1054-139x(99)00051-8. [DOI] [PubMed] [Google Scholar]
- 13.Ethier KA, Kershaw TS, Lewis JB, et al. Self-esteem, emotional distress and sexual behavior among adolescent females: Inter-relationships and temporal effects. J Adolesc Health. 2006;38 (3):268–274. doi: 10.1016/j.jadohealth.2004.12.010. [DOI] [PubMed] [Google Scholar]
- 14.Khan MR, Kaufman JS, Pence BW, et al. Depression, sexually transmitted infection, and sexual risk behavior among young adults in the United States. Arch of Pediatr Adolesc Med. 2009;163(7):644–52. doi: 10.1001/archpediatrics.2009.95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kosunen E, Kaltiala-Heino R, Rimpelä M, Laippala P. Risk-taking sexual behaviour and self-reported depression in middle adolescence--a school-based survey. Child Care Health Dev. 2003;29(5):337–44. doi: 10.1046/j.1365-2214.2003.00357.x. [DOI] [PubMed] [Google Scholar]
- 16.Lehrer JA, Shrier LA, Gortmaker S, et al. Depressive symptoms as a longitudinal predictor of sexual risk behaviors among US middle and high school students. [Accessed November 18, 2012];Pediatrics. 2006 118(1):189–200. doi: 10.1542/peds.2005-1320. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16818565. [DOI] [PubMed] [Google Scholar]
- 17.Reece M, Herbenick D, Schick V, et al. Condom use rates in a national probability sample of males and females ages 14 to 94. J Sex Med. 2010;7(5 suppl):266–276. doi: 10.1111/j.1743-6109.2010.02017.x. [DOI] [PubMed] [Google Scholar]
- 18.Laumann EO, Gagnon JH, Michael RT, et al. The social organization of sexuality: Sexual practices in the United States. Chicago, IL: University of Chicago Press; 2000. [Google Scholar]
- 19.Mazzaferro KE, Murray PJ, Ness RB, et al. Depression, stress, and social support as predictors of high-risk sexual behaviors and STIs in young women. J Adolesc Health. 2006;39(4):601–3. doi: 10.1016/j.jadohealth.2006.02.004. [DOI] [PubMed] [Google Scholar]
- 20.Longmore MA, Manning WD, Giordano PC, et al. Self-esteem, depressive symptoms, and adolescents’ sexual onset. Soc Psychol Quart. 2004;67(3):279–295. doi: 10.1177/019027250406700304. [DOI] [Google Scholar]
- 21.Shiyko MP, Lanza ST, Tan X, et al. Using the time-varying effect model (TVEM ) to examine dynamic associations between negative affect and self confidence on smoking urges: Differences between successful quitters and relapsers. Prev Sci. 2012;13(3):288–299. doi: 10.1007/s11121-011-0264-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tan X, Shiyko MP, Li R, et al. A time-varying effect model for intensive longitudinal data. Psychol Methods. 2012;17(1):61–77. doi: 10.1037/a0025814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Vasilenko SA, Lanza ST, Liu X, et al. Time-varying processes involved in smoking lapse in a randomized trial of smoking cessation therapies. Nicotine Tob Res. 2013 doi: 10.1093/ntr/ntt185. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yang J, Tan X, Li R, et al. TVEM (time-varying effect model) SAS macro suite users’ guide (Version 2.0.0) University Park: The Methodology Center, Penn State; 2012. Retrieved from http://methodology.psu.edu. [Google Scholar]
- 25.Harris KM. Design features of Add Health. Chapel Hill, NC: University of North Carolina at Chapel Hill; 2011. [Google Scholar]
- 26.Radloff LS. The use of the Center for Epidemiological Studies Depression Scale in adolescents and young adults. J Youth Adolesc. 1991;20(2):149–66. doi: 10.1007/BF01537606. [DOI] [PubMed] [Google Scholar]
- 27.Jessor R, Jessor S. Problem behavior and psychosocial development: A longitudinal study of youth. New York, NY: Academic Press; 1977. [Google Scholar]
- 28.Brown NR, Sinclair RC. Estimating number of lifetime sexual partners: Men and women do it differently. J Sex Res. 1999;36 (3):292–297. doi: 10.1080/00224499909551999. [DOI] [Google Scholar]
- 29.Crawford M, Popp D. Sexual double standards: A review and methodological critique of two decades of research. Journal of Sex Research. 2003;40:13–26. doi: 10.1080/00224490309552163. [DOI] [PubMed] [Google Scholar]
- 30.Meier AM. Adolescent first sex and subsequent mental health. Am J Sociol. 2007;112(6):1811–1847. doi: 10.1086/512708. [DOI] [Google Scholar]
- 31.Spriggs AL, Halpern CT. Sexual debut timing and depressive symptoms in emerging adulthood. J Youth Adolesc. 2008;37(9):1085–1096. doi: 10.1007/s10964-008-9303-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lanza ST, Moore JE, Butera NM. Drawing causal inference using propensity scores: A practical guide for community psychologists. American Journal of Community Psychology. 2013;52(3–4):380–392. doi: 10.1007/s10464-013-9604-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Stuart EA, Green KM. Using full matching to estimate causal effects in nonexperimental studies: Examining the relationship between adolescent marijuana use and adult outcomes. Developmental Psychology. 2008;44(2):395–406. doi: 10.1037/0012-1649.44.2.395. [DOI] [PMC free article] [PubMed] [Google Scholar]