

Abstract
We report a case of a 72-year-old man who presented with a persistent pleural effusion and painful abscess in the right lower chest wall 6 months following a laparoscopic cholecystectomy. The patient subsequently developed a chronic cutaneous chest wall fistula requiring a large resection and complex closure. The complication was likely secondary to intraoperative spillage of gallstones. While previous reports describe gallstone spillage in the abdominal cavity as benign, this case illustrates that stones left in the abdominal cavity can potentially lead to significant morbidity. Therefore, stones should be diligently removed from the abdominal cavity when spillage occurs. In addition, it is important that operative notes reflect the occurrence of stone spillage so stones may be suspected when a patient presents with an abdominal or thoracic infection following a cholecystectomy.
Background
Laparoscopic cholecystectomy is currently the gold standard surgical procedure for symptomatic cholelithiasis. The most common complications arising from laparoscopic cholecystectomy include bile duct injury, bile leaks, bleeding, infection and bowel injury. While gallbladder perforation occurs in 10–40%1––4 of patients undergoing a laparoscopic cholecystectomy, spillage of stones occurs less frequently, in approximately 6–10%1 of cases. Most of the time, these spilled stones are benign and have no further clinical sequelae; however, in 2.3–8.5%1––3 5 of patients, significant complications arise from unretrieved gallstones. Given the lack of awareness of stone spillage during a previous cholecystectomy and the variability in patient presentation, the diagnosis of complications arising from stone spillage is often delayed. The aim of this work is to highlight the potentially serious risk of gallstone spillage during cholecystectomy in a patient's postoperative course.
Case presentation
A 72-year-old man presented with a chronic cutaneous chest wall fistula. In January 2011, the patient underwent a laparoscopic cholecystectomy at an outside institution. Postoperatively, he suffered from a chronic loculated pleural effusion that was diagnosed as pneumonia and not drained. In June of the same year, his effusion persisted and he developed increasing pain in the right lower chest wall posteriorly, overlying the area with previously documented loculated fluid. The fluid was subsequently drained surgically and gallstone fragments were found in a complex subcutaneous and submuscular abscess.
Postoperatively, his wound evolved to form a peritoneopleurocutaneous fistula with intermittent purulent drainage. The patient reported that his physician was able to probe the fistula and extract gallstones. A CT scan demonstrated a fistula tract extending between the ribs with soft tissue thickening. The fistula tract appeared to extend into the parietal pleura. In January 2012, the abscess was debrided and the wound closed. No gallstones or other foreign debris were identified at that time. Unfortunately, the chest wall fistula reopened (figure 1A), reconfirmed on a follow-up CT scan (figure 2). In order to achieve definitive closure, complex chest wall closure was required.
Figure 1.

(A) Chronic peritoneopleurocutaneous chest wall fistula. (B) Appearance of the surgical site at 6 months follow-up.
Figure 2.
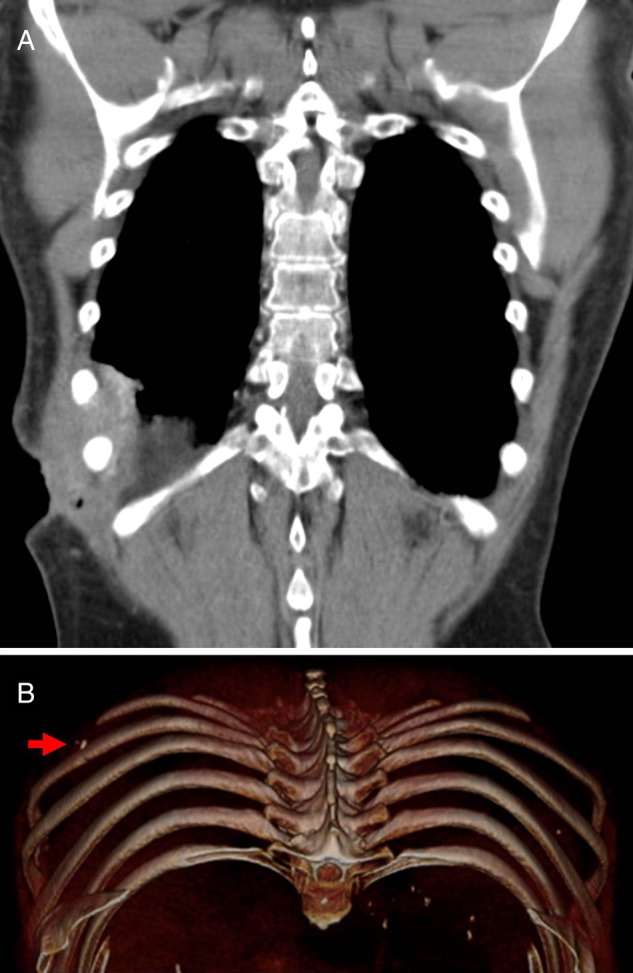
(A) Preoperative coronal CT image demonstrating the persistent fistula tract and (B) Three-dimensional reconstruction revealing a spilled stone along the fistula tract. Red arrow demarks location of a stone.
In September 2012, the patient was brought to the operating room for definitive treatment. To ensure adequate debridement, a surgical probe was used to determine the course and direction of the fistula tract. An 8 cm×7 cm ellipse of skin (surrounding the fistulous tract) was excised. Additionally, muscle, including the lower border of the latissimus, the serratus and the upper margin of the transversus abdominis muscle, as well as portions of ribs 9 and 10 were resected (figure 3A–C). A partial pulmonary decortication was also necessary. In the costophrenic sulcus, gallstones were identified and removed (figure 3D).
Figure 3.

Images of (A) preoperative markings, (B and C) anterior and posterior views of the en bloc resection of fistula including skin, muscle and portions of ribs 9 and 10 (D) Foreign body fragments resembling gallstones found in the costophrenic sulcus.
After resection was complete, a deep, full-thickness defect remained in the chest wall with exposure of liver, pleura and lung. To reconstruct the defect, a turnover flap was fashioned from the anterior muscle, keeping the thoracolumbar and intercostal perforators intact. Posteriorly, the latissimus dorsi muscle was raised while maintaining the thoracodorsal vessels. The muscle flaps were subsequently advanced to cover the defect and sutured into place with 2–0 Vicryl. Drains were placed in the wound and skin flaps advanced and closed primarily.
Outcome and follow-up
The patient tolerated the procedure without complication and his postoperative course was uncomplicated. By postoperative day 5, he was able to tolerate a regular diet, ambulate and was discharged home on levaquin due to Escherichia coli and streptococcal growth from the intraoperative wound culture. At 6 months follow-up, the patient remains well without complication (figure 1B). No wound healing complications were encountered.
Discussion
Laparoscopic cholecystectomy remains the gold standard treatment for symptomatic cholelithiasis because it is relatively safe, offers increased patient satisfaction and reduced hospital stay when compared to open procedures. However, the occurrence of gallbladder perforation (10–40%)1––4 and gallstone spillage (6–10%)1 during these procedures is not uncommon. This report provides an example of the potential complications arising from spilled stones after a laparoscopic cholecystectomy.
We present a case of a chronic peritoneopleurocutaneous fistula as a delayed complication of stone spillage. We believe that gallstone spillage occurred during the patient's laparoscopic cholecystectomy resulting in the trapping of stones between the liver and the diaphragm. Stones trapped in this unique location may be at increased risk of infection as this area is thought to escape the intra-abdominal clearing mechanism provided by the greater omentum and intestinal immune system.6 7 Therefore, it is likely that the spilled gallstones were a nidus of inflammation/infection resulting in a subdiaphragmatic abscess with ultimate fistulisation through the diaphragm and into the pleural cavity.
There have been very few reports describing similar complications arising from unretrieved stones following laparoscopic cholecystectomy. Although considered to be harmless by many,8 9 gallstones left in the abdominal cavity have been attributed to significant morbidity. Spilled stones have been associated with abscess formation, wound sinus or fistula formation, granuloma formation, empyema, small bowel obstruction, small bowel fistula, colonic fistula, septicaemia, diaphragmatic irritation and stone erosion through the flank.1 4 5 10––12 Other reports have described fistulas extending through the diaphragm, beyond the pleural space and into the bronchial tree, resulting in cholelithoptysis (expectoration of gallstones).13 14 Biliopleural fistula with thoracobilia and empyema has also been described.15 Boyd described in 1977 that subphrenic abscesses predictably perforate into the basal segments of the right lower lobe, as occurred in the presented case.
Several studies in rats have helped elucidate the principal factors that predispose for complications after stone spillage. While implantation of sterile stones into the peritoneal cavity of rats failed to increase morbidity after laparoscopic cholecystectomy, implantation of multiple stones with colonised bile has been demonstrated to increase the risk of adhesions and abscess formation.4 16 17 Furthermore, the chemical composition of the stone has been shown to correlate with the risk of intra-abdominal infection; bilirubinate stones are the most likely to harbour bacteria.4 18 In humans, reports have shown that up to 80–90% of pigmented stones have bacterial contamination,1 and the most common organism is E. coli.2
The need for intervention following a laparoscopic cholecystectomy with spilled stones has been documented to take place anywhere from 10 days to 20 years, with a peak incidence of 4–10 months.2 4 In our patient, the duration between laparoscopic cholecystectomy and initial complication of a loculated pleural effusion was 6 months. In addition, the broad range of complications and distance from or proximity to the liver make diagnosis of complications associated with spilled gallstones quite challenging. Therefore, only physicians with a high index of clinical suspicion are likely to identify the correct diagnosis. Perhaps a CT scan is warranted when a patient presents postoperatively with a right sided pleural effusion if there was a high index of suspicion of spilled stones.
The present report reveals the potential morbidity that can result from stone spillage at the time of laparoscopic cholecystectomy. The initial patient course may be indolent and the presenting symptoms may be benign, making initial diagnosis difficult. The best method for preventing such complications is avoidance of gallbladder perforation, routine use of endoscopic retrieval bags and diligent removal of stones from the abdominal cavity (in the event of gallbladder perforation). In addition, clear documentation regarding gallbladder perforation, regardless of whether it is pathological or iatrogenic, is essential in the operative note following cholecystectomy. Documentation of this detail provides valuable insights into the underlying disease process and aids in decision-making when physicians are presented with symptomatic patients following laparoscopic cholecystectomy.
Learning points.
Effort should be made to remove gallstones when gross stone spillage occurs.
Clear documentation should be included in the medical record when stone spillage occurs, regardless of whether all stones are suspected to have been retrieved.
Any patient with signs of infection or pain, in particular with right lower lobe pathology following cholecystectomy, should have complication from spilled gallstones on the differential.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Woodfield JC, Rodgers M, Windsor JA. Peritoneal gallstones following laparoscopic cholecystectomy: incidence, complications, and management. Surg Endosc 2004;18:1200–7 [DOI] [PubMed] [Google Scholar]
- 2.Irkorucu O, Tascilar O, Emre AU, et al. Missed gallstones in the bile duct and abdominal cavity: a case report. Clinics 2008;63:561–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rice DC, Memon MA, Jamison RL, et al. Long-term consequences of intraoperative spillage of bile and gallstones during laparoscopic cholecystectomy. J Gastrointest Surg 1997;1:85–90; discussion 90–1 [DOI] [PubMed] [Google Scholar]
- 4.Sathesh-Kumar T, Saklani AP, Vinayagam R, et al. Spilled gall stones during laparoscopic cholecystectomy: a review of the literature. Postgrad Med J 2004;80:77–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zehetner J, Shamiyeh A, Wayand W. Lost gallstones in laparoscopic cholecystectomy: all possible complications. Am J Surg 2007;193:73–8 [DOI] [PubMed] [Google Scholar]
- 6.Brockmann JG, Kocher T, Senninger NJ, et al. Complications due to gallstones lost during laparoscopic cholecystectomy. Surg Endosc 2002;16:1226–32 [DOI] [PubMed] [Google Scholar]
- 7.Cohen RV, Pereira PR, De Barros MV, et al. Is the retrieval of lost peritoneal gallstones worthwhile? Surg Endosc 1994;8:1360. [DOI] [PubMed] [Google Scholar]
- 8.Peters JH, Gibbons GD, Innes JT, et al. Complications of laparoscopic cholecystectomy. Surgery 1991;110:769–77; discussion 777–8 [PubMed] [Google Scholar]
- 9.Soper NJ, Dunnegan DL. Does intraoperative gallbladder perforation influence the early outcome of laparoscopic cholecystectomy? Surg Laparosc Endosc 1991;1:156–61 [PubMed] [Google Scholar]
- 10.Koç E, Suher M, Oztuğut SU, et al. Retroperitoneal abscess as a late complication following laparoscopic cholecystectomy. Med Sci Monit 2004;10:CS27–9 [PubMed] [Google Scholar]
- 11.Chin PT, Boland S, Percy JP. “Gallstone hip” and other sequelae of retained gallstones. HPB Surg 1997;10:165–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Memon MA, Deeik RK, Maffi TR, et al. The outcome of unretrieved gallstones in the peritoneal cavity during laparoscopic cholecystectomy. A prospective analysis. Surg Endosc 1999;13:848–57 [DOI] [PubMed] [Google Scholar]
- 13.Chopra P, Killorn P, Mehran RJ. Cholelithoptysis and pleural empyema. Ann Thorac Surg 1999;68:254–5 [DOI] [PubMed] [Google Scholar]
- 14.Downie GH, Robbins MK, Souza JJ, et al. Cholelithoptysis. A complication following laparoscopic cholecystectomy. Chest 1993;103:616–17 [DOI] [PubMed] [Google Scholar]
- 15.Boyd DP. Bronchobiliary and bronchopleural fistulas. Ann Thorac Surg 1977;24:481–7 [DOI] [PubMed] [Google Scholar]
- 16.Cline RW, Poulos E, Clifford EJ. An assessment of potential complications caused by intraperitoneal gallstones. Am Surg 1994;60:303–5 [PubMed] [Google Scholar]
- 17.Zorluoğlu A, Ozgüç H, Yilmazlar T, et al. Is it necessary to retrieve dropped gallstones during laparoscopic cholecystectomy? Surg Endosc 1997;11:64–6 [DOI] [PubMed] [Google Scholar]
- 18.Gürleyik E, Gürleyik G, Yücel O, et al. Does chemical composition have an influence on the fate of intraperitoneal gallstone in rat? Surg Laparosc Endosc 1998;8:113–16 [PubMed] [Google Scholar]