

Abstract
Background:
End stage renal disease (ESRD) is a condition that inflammation and oxidative stress plays an important role in damaging to tissues, especially, in the vascular system. The effect of omega-3 fatty acids is well-documented in some inflammatory diseases via eicosapentanoic acid and docosahexanoic acid components of fish oil. The aim of this study was to investigate the effects of dietary omega-3 fatty acid supplementation on levels of lipid peroxidation and oxidative sttress in ESRD patients.
Materials and Methods:
This randomized controlled double-blind clinical trial consisted of 90 patients on chronic ambulatory peritoneal dialysis (CAPD). One group was treated orally with 3000 mg omega-3, per day for 8 weeks (n = 45) and the other matched group by placebo (n = 45). Serum levels of lipids, iron, ferritin, Protrombin Time, Partial thromboplastin time, superoxide dismutase (SOD), and reduced glutathione (GH) were measured at the beginning and at 8 weeks.
Results:
Our results showed that SOD and reduced GH were not significantly changed in omega-3 group where lipid profile showed no significant changes too. Erythropoietin requirements also had no significant differences.
Conclusion:
Incorporation of omega-3 fatty acids to CAPD patients had no beneficial effects on oxidative stress but should evaluate more.
Keywords: Chronic ambulatory peritoneal dialysis, omega-3 fatty acids, oxidative stress, reduced glutathione, superoxide dismutase
INTRODUCTION
Increased oxidative stress is postulated to be an important contributor to uremic cardiovascular risk factors in end stage renal disease (ESRD) patients.[1] Hemodialysis (HD)-induced inflammation can cause morbidity and mortality in long-term in these patients.[2] Oxidative stress corresponds to an imbalance between the production of reactive oxygen species (ROS), mainly the superoxide anion, hydroxyl radical, lipid proxyl radicals, and hydrogen peroxide, with protective mechanisms.[3] Primary antioxidant enzymes in mammalian cells that seen to be necessary for cell protection are superoxide dismutase (SOD) and glutathione (GH) peroxidase that is a substrate for specific peroxidase.[4]
Oxidative stress (or oxidant-derived tissue injury) takes place when the production of oxidants exceeds local antioxidant capacity.[5] several processes protect our body from these damages include enzymes SOD and GH peroxidase, which remove ROS.[6]
It is accepted that dietary intake of n-3 Polyunsaturated fatty acids (PUFA) or fish oil has a beneficial role on human such as atherosclerosis and vascular reactivity.[7,8,9,10] Increased lipid peroxidation in ESRD patients and its linkage to atherosclerosis may suggest that supplementation with omega-3 in this patients have salutary effects on oxidative stress.[11] In one study, omega-3 supplementation in HD patient for 2 months could increased antioxidant factors like SOD.[12]
The aim of this study was to observe the effects of fish oil supplementation on SOD and reduced GH as biomarkers of oxidative stress in the chronic ambulatory peritoneal dialysis (CAPD) patients.
MATERIALS AND METHODS
This randomized controlled double-blind clinical trial was carried out in two CAPD centers in two university hospitals in Isfahan, Iran. Clinically stable patients without serious illness on CAPD for at least 3 months were enrolled in the present study. Patients were eligible for enrollment if they were over 18 years of age.
The exclusion criteria included: History of steatorrhea, malignancy, thrombocytopenia Platelet (PLT < 100000/mm3), abnormal coagulation profile or need for anticoagulation therapy, and psychosomatic disorders. A total of 90 patients participated in the study after obtaining consent form from precipitants.
All candidates were randomized into either Omega-3 therapy (n = 45), with omega-3 capsules (Omega-3, Zahravi co. Tabriz. Iran) that each 1 g contains Eicosapentanoic (180 mg) and Dosahexanoic (120 mg) orally 3 times a day for 8 weeks or placebo therapy (n = 45), by same intervals and duration. Envelopes were closed and opaque. All patients and physicians were blinded to randomized groups until the end of the study and drugs were given to patients by PD nurses.
Serum levels of low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, total cholesterol, triglycerides were measured at the beginning and the end of the study using auto analyzer, by Greiner Diagnostic GmbH and Pars azmun respectively, Iran. Serum Iron level and ferritin were measured by gamma counter, Zimense, Germany as for PT and PTT by Fischer, Germany. Hemoglobin was measured by using the H1 coulter. SOD and reduced GH were measured using the Glory kits with Enzyme-linked immuno sorbent assay method. In this method, after adding SOD to monoclonal antibody Enzyme well which is pre-coated with SOD monoclonal antibody, they were incubated. After continuing the process, changing in color, technician measure level of SOD or reduced GH (like SOD measurement) in plasma.
Patients were notified of the possibility of adverse effects such as abdominal pain, bloating, diarrhea, nausea, and bleeding during the study. Incidence of these symptoms was evaluated by a specific questionnaire.
Statistical analysis
This study has approved by Isfahan Kidney Diseases Research Center (project No. 290370) and ethical committee of Isfahan University of Medical Sciences. This study was registered in Iranian registry of clinical trials with ID number: IRCT201212142417N10
All statistical analyses were performed with the SPSS software (version 18.0 SPSS Inc, Chicago, IL, USA). Statistical analysis was carried out with λ2 test, paired t-test and analysis of variance (ANOVA). A 2-sided probability value of < 0.05 was considered statistically significant and a 95% confidence interval was used.
RESULTS
A total of 90 patients participated in the study. All candidates were randomized into either Omega-3 therapy (n = 45) or placebo therapy (n = 45). During study, any patient describe significant side-effects leading to drug discontinuation in both groups.
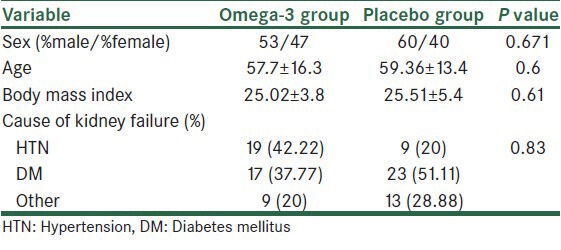
Baseline characteristics of patients included in the study are shown in Table 1. Our data showed no significant difference between groups regarding sex, age, body mass index, cause of renal failure, and medication usage.
Table 1.
Demographic characteristics of chronic ambulatory peritoneal dialysis patients at the start of study
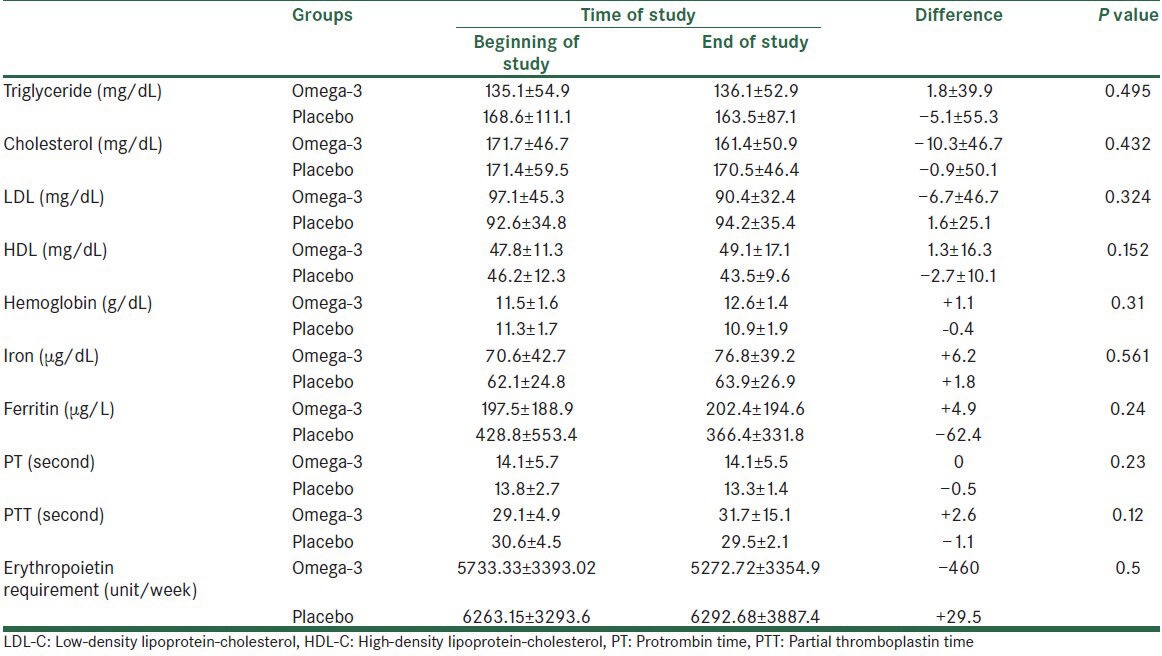
After 8 weeks, there were no significant differences in serum HDL-C, LDL-C, total cholesterol and triglycerides. PT and PTT measured at baseline and end of study for bleeding tendency and was showed significant differences in the course of study and two groups. Serum iron and ferritin level and hemoglobin had no significant differences as did for Erythropoietin need during study [Table 2].
Table 2.
Comparison of baseline and at 8 weeks triglyceride, cholesterol, LDL-C, HDL-C, and Iron, ferritin, PT and PTT and erythropoietin requirement in two groups
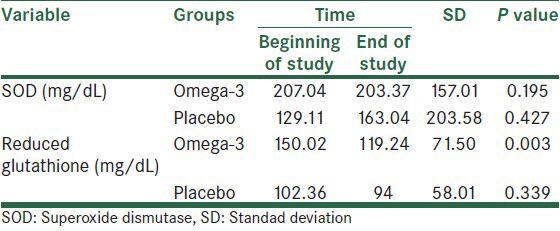
As shown in Table 3, SOD increased at the end of the study but it was no significantly in omega-3 group. In the other hand reduced GH decreased in the omega-3 group at the end of the study, but it was not significant statistically.
Table 3.
Comparison of superoxide dismutase and reduced glutathione in the baseline and at 8 weeks in two groups
DISCUSSION
Fish oil consumption as a supplement drug for inflammatory reduction is obvious in some disease like myocardial infarction,[13] rheumatoid arthritis,[14] Crohn disease[15] and some disease affect in kidney like IgA nephropathy.[16] A large prospective cohort study from Japan found a strong inverse relation between omega-3 intake and subsequent cardiovascular disease.[17]
In ESRD patients, application of fish oil was proposed in some abnormalities. In some studies, therapy with omega-3 could reduce hypertriglyceridemia in HD patients, too.[18] In our study, changes in triglyceride and other lipid components are not significant and were not support these effects. An explanation may be due to nearly acceptable baseline level of lipid profile in this study.
Inflammatory process increased in ESRD patients and some investigators proposed fish oil can reduce this process.[19] Snigger and Leitner have shown that the metabolism of arachidonic acid shifted from the cyclooxygenase pathway to the lipoxygenase pathway in the renal patients.[20] Kooshki et al. demonstrate that marine omega-3 supplementation did not change significantly oxidative stress parameters in HD patients.[21]
Our study revealed that SOD and GH were changed in omega-3 group without any significant value. These finding is in contrast with Tayyebi's study that demonstrate efficacy of omega-3 in reducing oxidative stress in HD patients.[11] One explanation may be the effect of high variable variance in laboratory data. On the other hand, duration of supplementation is short and may influence our results. However, it should be evaluate more by other studies.
Need to erythropoietin usage after fish oil treatment also evaluate in this study. In a pilot study, erythropoietin requirement decreased about 16% after omega-3 supplementation.[22] In our study, we did not revealed any significant changes in erythropoietin requirements. The reason for this finding is unclear for us, but this finding may be due to study limitations as mentioned below. On the other hand, other studies conducted in patients under HD but our study performed in patients on CAPD. Although, Filiopoulos et al. showed that inflammatory markers and oxidative stress parameters have not differences between HD and CAPD patients.[23] It may justify this paradoxical results, but more studies are needed.
Fish oil in CAPD patients contributing in our study did not induce any complications like nausea or vomiting and any patient did not discontinue the drug due to bad taste or malodor.
The present study had the following limitations: 1. The authors did not check all biochemical markers of inflammation and oxidative stress. 2. The duration of the study is short so. 3. Our informations about CAPD patients are little and more surveys should be carried out in this patients.
CONCLUSION
Omega-3 supplementation could not affect on oxidative stress in patients on CAPD. In addition, omega-3 incorporation did not affect on erythropoietin requirement in these patients
ACKNOWLEDGMENT
The finding of the research are the result of the corporation of CAPD centers in Alzahra and Aliasghar and Noor hospitals and special thanks to our CAPD nurses Mrs. Shirin Karimi, Elham Yazdani, and Akram Eslami and Miss Tahereh Gholamrezapoor for laboratory support.
This study was conducted as a fellowship thesis, funded by Vice chancellery of Research and Technology, Isfahan University of Medical Sciences, Isfahan, Iran.
Footnotes
Source of Support: Isfahan Kidney Disease Research Center, Isfahan University of Medical Science, Isfahan, Iran.
Conflict of Interest: None declared.
REFERENCES
- 1.Himmelfarb J. Linking oxidative stress and inflammation in kidney disease: Which is the chicken and which is the egg? Semin Dial. 2004;17:449–54. doi: 10.1111/j.0894-0959.2004.17605.x. [DOI] [PubMed] [Google Scholar]
- 2.Morena M, Delbosc S, Dupuy AM, Canaud B, Cristol JP. Overproduction of reactive oxygen species in end-stage renal disease patients: A potential component of hemodialysis-associated inflammation. Hemodial Int. 2005;9:37–46. doi: 10.1111/j.1492-7535.2005.01116.x. [DOI] [PubMed] [Google Scholar]
- 3.Himmelfarb J, Stenvinkel P, Ikizler TA, Hakim RM. The elephant in uremia: Oxidant stress as a unifying concept of cardiovascular disease in uremia. Kidney Int. 2002;62:1524–38. doi: 10.1046/j.1523-1755.2002.00600.x. [DOI] [PubMed] [Google Scholar]
- 4.Weydert CJ, Cullen JJ. Measurement of superoxide dismutase, catalase and glutathione peroxidase in cultured cells and tissue. Nat Protoc. 2010;5:51–66. doi: 10.1038/nprot.2009.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cristol JP, Bosc JY, Badiou S, Leblanc M, Lorrho R, Descomps B, et al. Erythropoietin and oxidative stress in haemodialysis: Beneficial effects of vitamin E supplementation. Nephrol Dial Transplant. 1997;12:2312–7. doi: 10.1093/ndt/12.11.2312. [DOI] [PubMed] [Google Scholar]
- 6.Attia AM, Nasr HM. Evaluation of protective effrct of omega-3 fatty acids and selenium on paraquat intoxicated rats. Slovak J Anim Sci. 2009;42:180–7. [Google Scholar]
- 7.Pekovic PG, Milutinovic RZ, Gluvic Z, Lackovic M, Medic DR, Glibetic M. Inflammation, nutritional status PUFA profile and outcome in hemodialysis patients. Arch Biol Sci. 2012;64:1173–80. [Google Scholar]
- 8.Friedman A, Moe S. Review of the effects of omega-3 supplementation in dialysis patients. Clin J Am Soc Nephrol. 2006;1:182–92. doi: 10.2215/CJN.00740805. [DOI] [PubMed] [Google Scholar]
- 9.Leaf A, Kang JX, Xiao YF, Billman GE. Clinical prevention of sudden cardiac death by n-3 polyunsaturated fatty acids and mechanism of prevention of arrhythmias by n-3 fish oils. Circulation. 2003;107:2646–52. doi: 10.1161/01.CIR.0000069566.78305.33. [DOI] [PubMed] [Google Scholar]
- 10.McGiff JC, Quilley J. 20-hydroxyeicosatetraenoic acid and epoxyeicosatrienoic acids and blood pressure. Curr Opin Nephrol Hypertens. 2001;10:231–7. doi: 10.1097/00041552-200103000-00012. [DOI] [PubMed] [Google Scholar]
- 11.Kalousová M, Sulková S, Fialová L, Soukupová J, Malbohan IM, Spacek P, et al. Glycoxidation and inflammation in chronic haemodialysis patients. Nephrol Dial Transplant. 2003;18:2577–81. doi: 10.1093/ndt/gfg404. [DOI] [PubMed] [Google Scholar]
- 12.Tayyebi-Khosroshahi H, Houshyar J, Tabrizi A, Vatankhah AM, Razzagi Zonouz N, Dehghan-Hesari R. Effect of omega-3 fatty acid on oxidative stress in patients on hemodialysis. Iran J Kidney Dis. 2010;4:322–6. [PubMed] [Google Scholar]
- 13.Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: Results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet. 1999;354:447–55. [PubMed] [Google Scholar]
- 14.Calder PC. Session 3: Joint Nutrition Society and Irish Nutrition and Dietetic Institute Symposium on ‘Nutrition and autoimmune disease’ PUFA, inflammatory processes and rheumatoid arthritis. Proc Nutr Soc. 2008;67:409–18. doi: 10.1017/S0029665108008690. [DOI] [PubMed] [Google Scholar]
- 15.Belluzzi A, Brignola C, Campieri M, Pera A, Boschi S, Miglioli M. Effect of an enteric-coated fish-oil preparation on relapses in Crohn's disease. N Engl J Med. 1996;334:1557–60. doi: 10.1056/NEJM199606133342401. [DOI] [PubMed] [Google Scholar]
- 16.Donadio JV, Jr, Bergstralh EJ, Offord KP, Spencer DC, Holley KE. A controlled trial of fish oil in IgA nephropathy. Mayo Nephrology Collaborative Group. N Engl J Med. 1994;331:1194–9. doi: 10.1056/NEJM199411033311804. [DOI] [PubMed] [Google Scholar]
- 17.Iso H, Kobayashi M, Ishihara J, Sasaki S, Okada K, Kita Y, et al. Intake of fish and n3 fatty acids and risk of coronary heart disease among Japanese: The Japan Public Health Center-Based (JPHC) Study Cohort I. Circulation. 2006;113:195–202. doi: 10.1161/CIRCULATIONAHA.105.581355. [DOI] [PubMed] [Google Scholar]
- 18.Khajehdehi P. Lipid-lowering effect of polyunsaturated fatty acids in hemodialysis patients. J Ren Nutr. 2000;10:191–5. doi: 10.1053/jren.2000.16326. [DOI] [PubMed] [Google Scholar]
- 19.Schmitz PG, McCloud LK, Reikes ST, Leonard CL, Gellens ME. Prophylaxis of hemodialysis graft thrombosis with fish oil: Double-blind, randomized, prospective trial. J Am Soc Nephrol. 2002;13:184–90. doi: 10.1681/ASN.V131184. [DOI] [PubMed] [Google Scholar]
- 20.Sinzinger H, Leithner C. Eicosanoids of platelets and vascular wall in chronic renal insufficiency. Am J Nephrol. 1987;7:212–20. doi: 10.1159/000167466. [DOI] [PubMed] [Google Scholar]
- 21.Kooshki A, Taleban FA, Tabibi H, Hedayati M. Effects of marine omega-3 fatty acids on serum systemic and vascular inflammation markers and oxidative stress in hemodialysis patients. Ann Nutr Metab. 2011;58:197–202. doi: 10.1159/000329727. [DOI] [PubMed] [Google Scholar]
- 22.Jones WL, Kaiser SP. Pilot study (An emulsified fish oil supplement significantly improved C-reactive protein, hemoglobin, albumin and urine output in chronic hemodialysis volunteers) J Assoc Nurses AIDS. 2002;5:45–50. [Google Scholar]
- 23.Filiopoulos V, Hadjiyannakos D, Takouli L, Metaxaki P, Sideris V, Vlassopoulos D. Inflammation and oxidative stress in end-stage renal disease patients treated with hemodialysis or peritoneal dialysis. Int J Artif Organs. 2009;32:872–82. doi: 10.1177/039139880903201206. [DOI] [PubMed] [Google Scholar]