

Abstract
A 62-year-old, male patient radiologically diagnosed as a case of avascular necrosis of femur head with grade 4, presented the following chief complaints. Pain in the left hip joint radiating to thigh (anterior part), of grade ‘9’ on “visual analog scale (VAS)” associated with swelling in bilateral feet and decreased range of movements in the hip joint. This presentation was correlated with Asthi-majjagata vāta (musculo-skeletal disorder) and treated accordingly. Initially, patient had been administered dīpana and pācana followed by nityavirecana (therapeutic purgation). Further Saghrita kṣīrabasti (medicated enema prepared with milk and ghee) was administered in kalābasti schedule (16 in number). This resulted with relief of pain to grade “3” on “VAS” and complete resolution of pedal edema and improvement in range of movement of hip joint.
KEY WORDS: Asthi-majjagata vata, avascular necrosis of head of femur, Saghrita ksheerabasti
INTRODUCTION
Avascular necrosis (AVN) is a progressive disorder with surgical intervention as the prime choice. A patient presented to us had grade 4 presentation and advised for surgery. In this acute stage, the case was well managed and relieved significantly by Saghṛta kṣīrabasti. Going by the results presented here, it can be safely con cludedthat, AVN can be treated effectively with ayurveda approach which is non-invasive in nature.
AVN is a condition affecting different bones as a result of transient/permanent loss of blood supply to the bones. Eventual collapse of the bone tissue and its death is the resultant of the ischemia along with its overlying joint surface.[1] Necrosis is caused due to the arterial occlusion[2] and femoral head is the most commonly affected area. Most of the patients presenting this diagnosis are in their third or fourth decade of life with increased ratio in females.[3] Symptoms of AVN of femoral head are presented by groin or hip pain radiating to buttocks, anteromedial thigh or knee that is aggravated by weight-bearing and sometimes by coughing. Progressive increase of the pain worsens with time and use, patient experiences pain on rest which may be worse during night and may have association with morning stiffness.[2]
Asthi-majjagata vāta, vātavyādhi, occurs due to the vitiated vāta doṣa residing in asthi (bones) and majjā (marrow).[4] It presents with the clinical features as bhedo-asthiparvaṇāṃ (breaking type of pain in bones), sandhishūla (joint pain), satata ruk (continuous in nature), māṃsabalakṣaya (loss of strength and muscles weakness) and asvapna (disturbed sleep), which correlates with symptoms of AVN. Administration of snehana (oleation therapy) both external and internal form is the best treatment modality. External administration is performed by abhyaṅga (massage) with medicated oils, internally it is administered in the form of pāna (internal oleation through oral route) and basti (oleation through rectal route).[5] Therapeutic enemas in painful diseased conditions of basti-vaṅkṣaṇa-pārshwa-uru-parwa-asthi (anatomical land marks indicating lower part of the body) is the precise approach, which are administered in the form of Saghṛta kṣīrabasti (milk infusions processed with ghee).[6]
CASE REPORT
This is the case report of a 62-year-old, non-diabetic and non-hypertensive who presented with pain since one year in the left hip radiating to left anterior thigh. The pain was continuous in nature and used to aggravate during walking and night hours, with rest as relieving factor. Transient relief was found in conventional treatments with recurrence with intensified pain, weakness in left lower limb and swelling in the feet after few days. His condition gradually worsened and he developed inability to walk without support. Surgical intervention was advised, which the patient refused and approached Ayurvedic treatment for the condition.
Personal history revealed mixed diet, reduced appetite, irregular and constipated bowel and disturbed sleep (due to pain). He has habit of chewing tobacco and drinking since 40 years.
Systemic examination
Locomotor system findings were unable to be elicited because of complete arrest of range of movements and severe pain in the hip joints. Inspection revealed non-pitting type of pedal edema associated with blackish discoloration and local rise of temperature. Patient had normal muscle bulk and tone. Cardiovascular and respiratory systems were in normal limits.
Investigations
Magnetic resonance imaging revealed - AVN of both hip joints, grade 4 of the left hip joint.
Treatment schedule
Dīpana ~carminative and pācana ~digestive treatment was adapted by administration of hingvaṣṭka cūrṇa[7] (half teaspoon thrice a day) and śuṇṭhi kaṣāya[8] (40 ml twice a day) for 2 days in order to relieve āma (a state where metabolism is hampered) symptoms such as jihvāliptatā (coated tongue), aruci (lack of appetite and lack of interest in food), aṅgagauravatā (heaviness in the body) and malabaddhatā (irregular and constipated bowel habits). The treatment was aimed at āmapacana (digestion of āma) and vātānuolamana (downward movement of vāta doṣa) effect.
Pādaśotha (pedal edema) confirmed the increased kledaguṇa (increased fluidity) and kapha in the body causing srotorodha (obstruction of channels). Hence nityavirecana (regular therapeutic purgation) was planned with harītakī cūrṇa (powder of Terminalia chebula 5 g) + gomūtra (cow's urine) (50 ml) for clearing srotorodha which resulted in relief of pedal edema.
Jihvā aliptatā (tongue not being coated) dehalāghavatā (lightness in the body), agnidīpti (increased appetite), vātānulomana and relief in pedal edema suggests nirāmāvasthā (corrected state of metabolism).
Later Saghṛta kṣīrabasti (therapeutic enema) was planned from 5th day in the following (Tables 1 and 2) pattern:
Table 1.
Basti
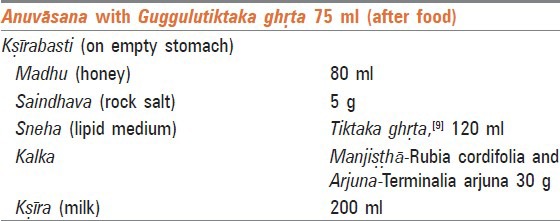
Table 2.
Basti pattern (therapeutic schedule pattern)
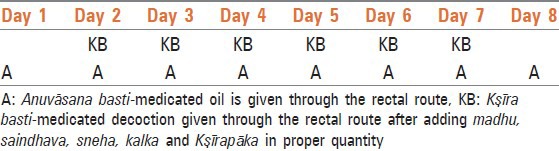
After Basti pain intensity reduced, improvement in strength and range of movements was observed.
Outcome and follow-up
Pain, pedal edema and range of movements were assessed. Pain is assessed by using visual analog scale (VAS), where “0” is no pain and “10” is severe pain. Circumference of the feet in inches was measured before and after the treatment to assess the swelling. Range of movements assessed subjectively.
Pain
On the day of admission, pain graded as “9” on VAS. After administration of carminatives and regular therapeutic purgative, pain reduced to grade 8. During the course of basti treatment assessment of pain grading is depicted in the graph every day [Graph 1].
Graph 1.
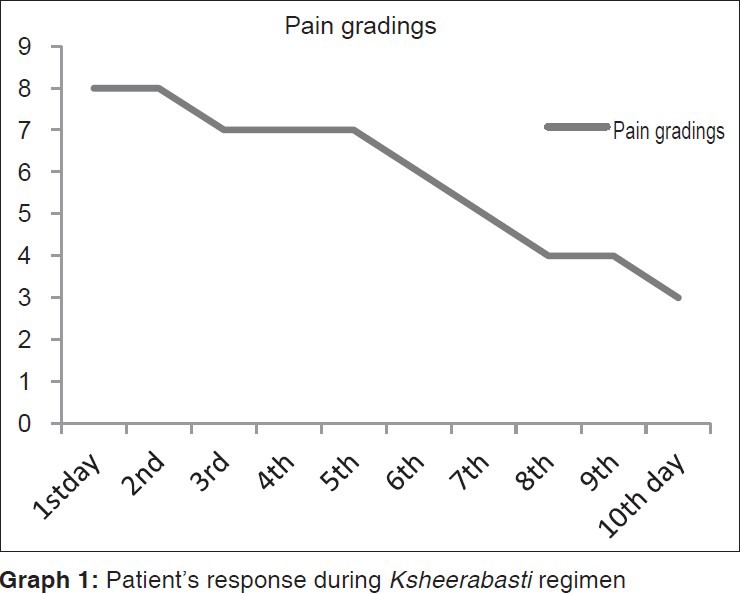
Patient's response during Ksheerabasti regimen
Swelling
On the 1st day, circumference feet, was around 27 in. After nityavirechana swelling was reduced and circumference measured about 23.5 in.
Range of movements
Initially, the patient was moving on wheel chair. At the time of discharge, he started walking with support which signifies improvement in strength and range of movements.
Advice on discharge
Amṛtottara kaṣāaya,[10] 15 ml 3 times a day with equal amount of warm water, does āmapacana (digests the āma) and vātānulomana. Kaiśor guggulu[11] one tablet thrice daily, possesses śothahara property (capacity to reduce edema) and rasāyana (rejuvenator) effect and advised with anupāna of Mahāmañjiṣṭhādi kaṣāya.[12] Mahāmañjiṣṭhādi kaṣāya is recommended for rakta prasādana (improveing circulation and favoring regeneration of tissue) and relieves prasupti (tingling sensation). Sahacaarādi kaṣāyam[13] is the medicine that is prescribed in conditions like siragata vāta (vāta doṣa taking shelter in vessels) and administered one tablet thrice daily. Guggulutiktaka ghṛta[14] mainly indicated in asthi (bony tissue), sandhi (joints), majjāgata vikāras (diseases of bone marrow). It also contains tiktarasapradhānadravya (drugs predominant in bitter taste), possesses Pṛthvī mahābhuta (earth element) which helps in bone formation and nourishment hence administered 20 ml twice daily with milk before food as śamana sneha (palliative oleation).
Follow-up after 15 days
During the follow-up, patient presented with a significant improvement by subjective assessment and second course of Saghṛta kṣīrabasti (therapeutic enema) with above same medicines was administered.
DISCUSSION
AVN is a pathologic condition that results from temporary or permanent loss of blood supply to the particular part, frequently affecting the femoral head. Though pathophysiology of AVN of the femoral head has been poorly understood, following mechanisms can theorized as the causes: [15]
Vascular occlusion: Due to direct trauma (e.g. fracture and dislocation), non-traumatic stress and stress fracture, there will be an interruption of the extra osseous blood supply
Altered lipid metabolism: Lipid-level-lowering drugs in animals showed reversal of lipid deposition in the femoral head
Intravascular coagulation: Coagulative disorders have been implicated in the pathogenesis of AVN
Healing process: Repair process triggered by necrotic bone which includes osteoclasts, osteoblasts, histiocytes and vascular elements. There will be new bone formation over the dead bone and forms a thick layer on the dead bone which prevents revascularization of the dead/necrotic bone
Mechanical stress: Animal studies have shown an association between increased weight bearing and an increased incidence of AVN of the femoral head.[15]
Whatever may be the reason, prime pathology involves the reduction in blood supply to the femoral head. Which can be inferred in Ayurvedic pathogenesis as follows: Rakta dhātu (blood tissue) supply to the femoral head is decreased. It leads to decreased nutrition supply to that part and reduction in its density (asthidhātukṣāya). As majjā (bone marrow) resides in asthidhātu, it may further result in majjādhātukṣaya.
Hiṅgvaṣṭaka cūrṇa and śuṇṭhi kaśāya were administered to increase the appetite as they contain ingredients such as hiṅgu (Ferula northax), trikaṭu (pippali - Piper longum, marīca - Piper nigrum, śuṇṭhi-Zingiber officinale), ajamoda (Apium graveolens), saindhava, jīraka (Cumium cymium), kṛṣṇa jīraka (Carum carvi) - which predominate in kaṭu rasa (pungent taste), ushṇa vīrya (hot in potency). These qualities increase jaṭharāgni (digestive power) and help to regulate apāna vāyu (a type of vāta doṣa) in downward direction. Involvement of rasadhātu duṣṭ (1st body tissue) and kleda (increased fluidity) was evident by pādaśotha (pedal edema). Hence nityavirecana was planned with harītakī cūrṇ (powder of Terminalia chebula) and gomūtra (cow's urine). Harītakī is kaṣāya pradhāna (predominant in astringent taste) pañcarasa, uṣṇa vīrya, rūkṣa gṇa pradhāna (predominant in drying property) and anulomaka (facilitates downward movement). Gomūtra is kaṭu, tikta (bitter taste), kaṣāya rasa (astringent taste), uṣṇa vīrya (hot in potency) and lekhana (scraping action). After nityavirecana, pādśotha and constipation were relieved.
Tiktaka kṣīrabasti was planned for strengthening of asthi dhātu. Tikta rasa is predominance of Vāyu and Ākāśa Mahābhūta. Hence, it has got affinity toward the body elements like Asthi which has same mahābhautika tattva (subtle constituents of matter). Most ingredients of Guggulutiktaka ghṛta that is administered for anuvāsana basti (retention enema) have tikta rasa, uṣṇa vīrya and madhura (sweet) and kaṭu vipāka favors normal functioning of dhātvagni (metabolic stage), facilitating increased nutrition of the asthi dhātu (bony tissue). As a result, degeneration of asthi and majjā dhātu reduced helping its regeneration. Ghṛta (ghee) is vāta-pittashāmaka (reduces vāta and pitta doṣa), balya (increases body strength), agnivardhaka (increases appetite as well as metabolism), madhura, śīta vīrya (cold in potency). Thus, it pacifies vāta; improves the dhātu upacaya (metabolism of the tissues) and acts as a rejuvenator of the body. Ghṛta has the properties of saṃskarāsya anuvartana (that which inherits the properties of other drugs without altering itself) precipitating bio-availability of other drugs. Ghṛta also contains vitamin D which plays an important role to utilize calcium and phosphorous from blood and helps in bone formation.[16] Thus, helps in the samprāpti vighaṭana (breaking down of pathology) of the ashti-majjāgata vāta. Niruha basti (a type of enema evacuation enema) containing kṣīra (milk) as the main ingredient is called as kṣīrrabasti. Kṣīra has madhura and snigdha (having oleation property) properties which help to control vāta doṣa and acts as bṛhmaṇa (nourishing). Research studies on kṣīrabasti proved to be efficacious in asthi-kshaya (osteoporosis) conditions.[17] The kalka dravya manjista possess madhura (sweet), tikta (bitter) and kaṣāya (astringent). The uṣṇa quality allows the herb to penetrate into the cellular level of the tissues and helps in blood purification and cleansing of the lymphatic system. Mañjiṣṭhā maintains normal blood pressure and favors smooth blood flow.[18] The other kalka dravya arjuna is kaṣāya rasa (astringent), śīta vīrya (cooling). It pacifies kapha and pitta. The kaṣāya rasa is sandhānakara (improves the compactness) in nature. Its usage with milk has been mentioned by the Ācāryas as asthi-sandhānakara. The bark of the Arjuna tree contains nutrients such as calcium helps bone regeneration. It enhances the elimination of cholesterol by accelerating the turnover of low density lipoprotein-cholesterol in the liver and lowers beta-lipoprotein lipids and the recovery of high density lipoprotein components in hyperlipidemia.[19] Thus, it prevents the deposition of lipids in the femoral head which increase the patency of vessels for increased circulation. It helps in reversing the hardening of the blood vessels. Thus the whole formation acts at different levels.
At the end of treatment, patient had complete relief of pedal edema, increased strength and range of movements, walking witnessed with support. Pain intensity reduced and graded as “3” on VAS.
TAKE HOME MESSAGE
It can be concluded that AVN can be well managed by Saghṛta kṣīrabasti as results show in the present study.
Footnotes
Source of Support: Nill
Conflict of Interest: None declared.
REFERENCES
- 1.Schoenstadt A. Avascular necrosis. [Last updated/reviewed on 2008 Nov 05]. Available from: http://www.bones.emedtv.com/avascularnecrosis/avascular-necrosis.html .
- 2.Aiello MR. Avascular necrosis of the femoral head. [Last accessed on 2008 Aug 01]. Available from: http://www.emedicine.medscape.com/article/386808 .
- 3.Aldridge JM, 3rd, Urbaniak JR. Avascular necrosis of the femoral head: Etiology, pathophysiology, classification, and current treatment guidelines. Am J Orthop (Belle Mead NJ) 2004;33:327–32. [PubMed] [Google Scholar]
- 4.Trikramji AJ, editor. 5th ed. Varanasi: Chaukhambha Sanskri Sansthan; 2006. Charaka Samhita. 28th Adhyaya 33rd shloka Chikitsasthana; p. 617. [Google Scholar]
- 5.Trikramji AJ, editor. 5th ed. Varanasi: Chaukhambha Sanskri Sansthan; 2006. Charaka Samhita. 28th Adhyaya 93rd shloka Chikitsasthana; p. 621. [Google Scholar]
- 6.Trikramji AJ, editor. 5th ed. Varanasi: Chaukhambha Sanskri Sansthan; 2006. Charaka Samhita. 29th Adhyaya 88 and 89th shloka Chikitsasthana; p. 631. [Google Scholar]
- 7.Shastri SA. Varanasi: Chaukhambha Sanskrit Samsthana; commentator. “10th Adhyaya 59th shloka”. Bhaishajya Ratnavali. Hindi translation; p. 242. [Google Scholar]
- 8.Gopinath GB. In: Bharat Bhaishajya Ratnakara. 1st ed. Part 5. Yoga No.7232. Rasavaidya Nageendas Chaganlal Shah., editor. New Delhi: Motilal Banarasidas; 1928-37. p. 13. [Google Scholar]
- 9.2nd to 7th shloka. Chikitsasthana. 2nd ed. 19th Ch. II. Varanasi: Krishnadas Academy; 1995. Vagbhata's Astanga Hradayam, Text with English Translation, Translated by Prof. KR Srikantha Murthy; p. 472. [Google Scholar]
- 10.Nishteshwar K, Vidyanath R, editors. Varanasi: Chaukhambha Krishnadas Academy; “Kashaya Prakarana”. Sahasrayoga English translation; p. 4. [Google Scholar]
- 11.Chandra Murthy HP., editor. Varanasi: Chaukhambha Sanskrit Series Office; 7th Adhyaya Madhyama Khanda 70–81 shloka. Sharangadhara Samhita. English commentary; pp. 187–8. [Google Scholar]
- 12.Chandra Murthy HP., editor. Varanasi: Chaukhambha Sanskrit Series Office; 2nd Adhyaya Madhyama Khanda 137-42 shloka. Sharangadhara Samhita. English commentary; pp. 135–6. [Google Scholar]
- 13.Kunte AM, Navre Shastri KR, Vaidya HP. Varanasi: Krishnadas Academy; 21st Adhyaya Chikitsasthana 56th shloka. Astanga Hradaya. Sanskrit commentary; p. 726. [Google Scholar]
- 14.Kunte AM, Navre Shastri KR, Vaidya HP, editors. Varanasi: Krishnadas Academy; 21st Adhyaya Chikitsasthana 58-61 shloka. Astanga Hradaya. Sanskrit commentary; pp. 726–7. [Google Scholar]
- 15.Tofferi JK. Avascular necrosis. [Last accessed on 2012 Jan 19]. Available from: http://www.emedicine.medscape.com/article/333364-overview#a0104 .
- 16.Akhtar B, Mahto RR, Dave AR, Shukla VD. Clinical study on Sandhigata Vata w.s.r. to Osteoarthritis and its management by Panchatikta Ghrita Guggulu. Ayu. 2010;31:53–7. doi: 10.4103/0974-8520.68210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sanjaya K, Subbanagouda PG. Clinical evaluation of the role of Tikta ksheera basti and Ajasthi Bhasma in the management of Astgi-Kshaya vis-à-vis osteoporosis. Ayu. 2009;30:131–41. [Google Scholar]
- 18.Himalya Manjistha/Manjistha. [Last accessed on 2013 Apr 25]. Available from: http://www.favorfinesse.com/manjishtha.shtml .
- 19.Arjuna Herb-Benefits and side effects. [Last posted on 2010 Sep 09, 06:30 am by admin, 2013 Apr 25]. Available from: http://www.sweetadditions.net/health/arjuna-herb-benefits-side-effects .