

Abstract
Objective. To examine the rational (systematic and rule-based) and experiential (fast and intuitive) decision-making preferences of student pharmacists, and to compare these preferences to the preferences of other health professionals and student populations.
Methods. The Rational-Experiential Inventory (REI-40), a validated psychometric tool, was administered electronically to 114 third-year (P3) student pharmacists. Student demographics and preadmission data were collected. The REI-40 results were compared with student demographics and admissions data to identify possible correlations between these factors.
Results. Mean REI-40 rational scores were higher than experiential scores. Rational scores for younger students were significantly higher than students aged 30 years and older (p<0.05). No significant differences were found based on gender, race, or the presence of a prior degree. All correlations between REI-40 scores and incoming grade point average (GPA) and Pharmacy College Admission Test (PCAT) scores were weak.
Conclusion. Student pharmacists favored rational decision making over experiential decision making, which was similar to results of studies done of other health professions.
Keywords: decision making, student pharmacists, rational, experiential
INTRODUCTION
Pharmacists are challenged with processing information and making decisions amid growing amounts of accessible medical information, increasingly complex healthcare systems, mounting legal pressures, and ongoing demands for patient autonomy. In addition, pharmacists’ decision making responsibilities have increased as their roles in team-based models of care and collaborative drug therapy management have expanded. Heuristics (“rules of thumb”) and biases can significantly influence clinical decision making, but the resulting systematic errors have prompted a shift towards objective, rational, and informed decision making through the use of evidence-based medicine (EBM).1-3 Understanding the underlying preferences for decision making in pharmacy is critical for informing pharmacy education and developing educational approaches that promote good decisions.3,4
Decision making is a complex process that can be explained, in part, by dual-process theories of cognitive psychology.5-7 Models of decision making derived from Cognitive-Experiential Self-Theory (CEST) propose that there are 2 primary modes of information processing operating simultaneously and sequentially. Rational processing incorporates the use of conscious, deliberate, analytical, rule-based criteria.8 It involves critical evaluation of evidence and a structured decision-making process. In contrast, experiential processing is considered automatic, fast, recognition-primed, and intuitive; it can be influenced by context, personal dispositions, and emotional arousal.8,9
Individuals tend to prefer one mode over another10 and are relatively consistent in using that mode; however, decision-making styles can be influenced by the way information is presented.3,11 Further, preferences in decision-making and thinking styles may differ by a specific population (ie, undergraduate students) or profession (ie, doctors).6,12,13 As such, careful consideration should be given to the design and implementation of strategies that inform and influence decision making, particularly as they relate to context-specific populations.14
For healthcare professionals making clinical decisions, there is a need to balance rational and experiential thought processes to make correct decisions in a time-efficient manner. While cognitive psychology has extensively explored issues underlying the decision-making process, the extent to which pharmacists rely on rational and experiential modes of information processing is not known. Decision making by pharmacists and student pharmacists may differ distinctly from other populations and professions because of context, resources, responsibilities, and general personality characteristics. The purpose of this study was to examine student pharmacists’ preferences towards experiential and rational thinking, and to compare these preferences to the preferences of other health professionals and student populations. Understanding the underlying constructs that drive decision making in future pharmacists can provide insight into teaching and learning strategies that promote safe decision making, especially as it relates to the efficacy of direct patient care and mitigation of medication errors.
METHODS
In spring 2013, all P3 students (n=150) enrolled in the doctor of pharmacy (PharmD) program at the University of North Carolina (UNC) at Chapel Hill Eshelman School of Pharmacy were invited to participate in the study. Participation was voluntary and no incentives (eg, course credit, compensation) were provided. Consent to participate was implied by completion of the survey instrument described below. This study was approved by the UNC Institutional Review Board.
To collect data about student pharmacist decision-making styles, all participants were asked to complete an electronic survey instrument consisting of demographic questions (gender, race/ethnicity, age, and prior degree completion) followed by the Rational Experiential Inventory (REI-40). The REI-40 is a 40-question survey designed to examine an individual’s preference for 2 decision-making styles: the need for cognition (rationality) and faith in intuition (experientiality).5 The survey instrument had 4 subscales, each measured by 10 items using a 5-point Likert scale ranging from definitely false (1) to definitely true (5). Each item required users to reflect on perceived ability or enjoyment associated with the following rational or experiential decision-making activities:
(1) Rational ability refers to perceived ability to use logical and analytic thinking (eg, “I have a logical mind.”)
(2) Rational engagement refers to perceived reliance on and enjoyment of using logical and analytic thinking (ie, “I enjoy intellectual challenges.”)
(3) Experiential ability refers to perceived ability with respect to one’s intuitive impressions and feelings (eg, “I believe in trusting my hunches.”)
(4) Experiential engagement refers to perceived reliance on and enjoyment of using feelings and intuitions (eg, “I tend to use my heart as a guide for my actions.”)
A composite rational score was obtained by summing responses from the rational ability (r-ability) and rational engagement (r-engagement) items, while a composite experiential score was obtained by summing the experiential ability (e-ability) and experiential engagement (e-engagement) items.5
The REI-40 has been validated among various populations, including college students,5 paramedics,15 potential jurors,16 cardiologists,14 and emergency physicians.12 This psychometric instrument is internally consistent and highly reliable, with the Cronbach alpha ranging from 0.74 to 0.91.
All quantitative data analysis was conducted in SPSS, version 20 (IBM Corp, Armonk, NY). Continuous data were presented as mean ± standard deviation (SD). Independent t tests and ANOVA were used to examine differences between groups. Post hoc analysis was performed using the Tukey test to compare pairs of means. The Pearson coefficient was used to investigate correlations between continuous variables. Statistical significance was established at α=0.05.
RESULTS
The study sample consisted of 114 P3 student pharmacists (76% response rate) aged 27.5±5.2 years; 70 were female, 79 were white, and 85 students completed a degree prior to entering pharmacy school. All REI-40 responses were aggregated and averaged by scale and subscale to provide scores ranging from 1 to 5, with higher scores reflecting a greater preference towards the construct measured. The total scale reliabilities (the Cronbach alpha) for this sample ranged from 0.78 to 0.85 (Table 1), suggesting that survey items used to compute scores for each of the scales demonstrate acceptable internal consistency. The correlation between the rationality and experientiality scales was weak and nonsignificant (r=-0.03), supporting the CEST assumption of 2 independent information processing modes for student pharmacists.
Table 1.
Intercorrelations and Reliabilities of Rational-Experiential Inventory Scales
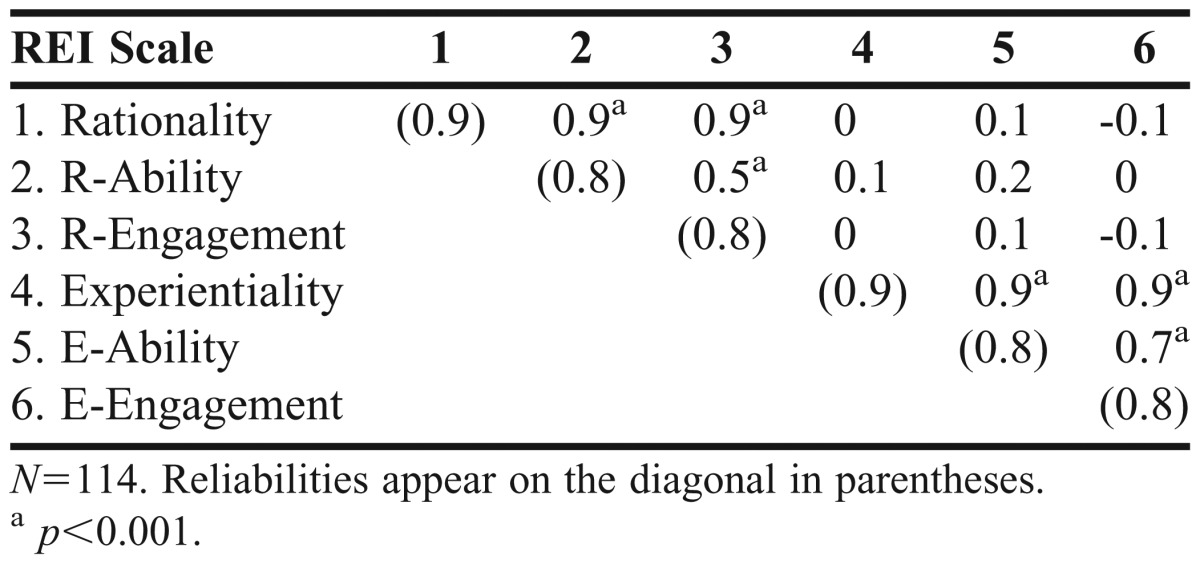
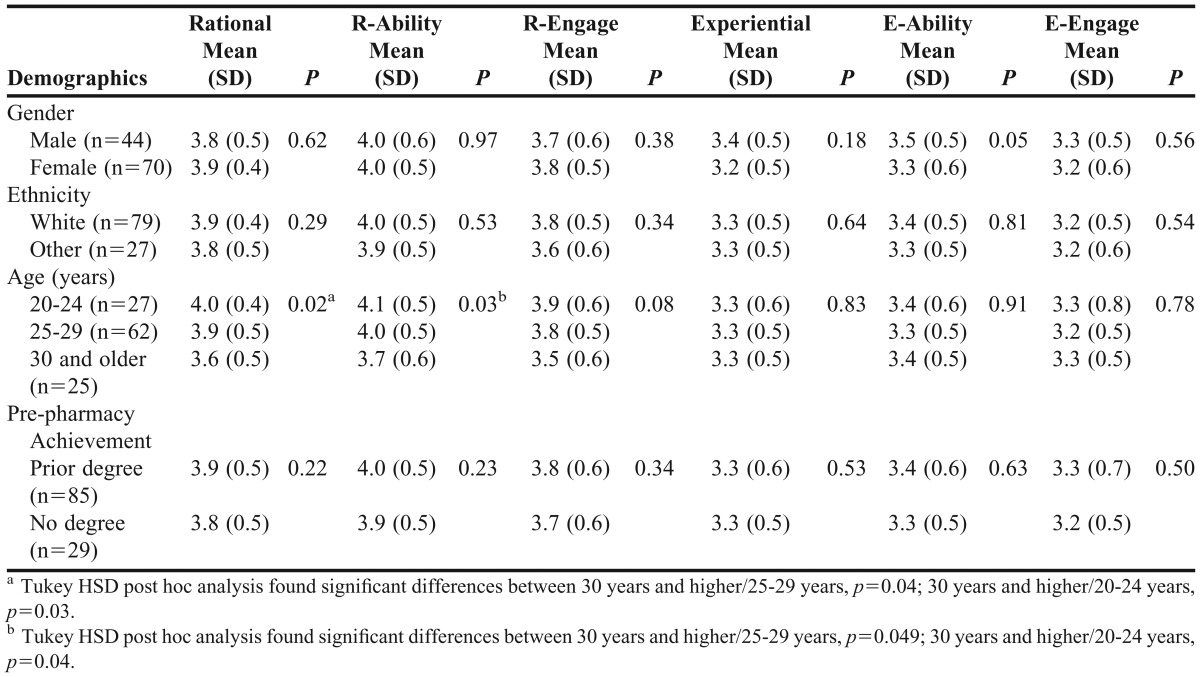
Student pharmacists’ mean rational scores were 3.9±0.33 for rationality; 4.0±0.50 for R-Ability; and 3.8±0.55 for r-engagement. Mean experiential scores were 3.3±0.50 overall; 3.4±0.54 for e-ability; and 3.2±0.55 for e-engagement. No significant differences in decision-making styles were found among students based on gender, race, or prior degree (Table 2). However, post hoc analysis showed that older students presented significantly lower rational (30 and older/25-29, p=0.04; 30 years and older/20-24 years, p=0.03); and r-ability scores (30 years and higher/25-29 years, p=0.049; 30 years and older/20-24 years, p=0.04). All correlations between academic performance indicators (PCAT and GPA) and REI-40 scores and subscores were weak (r<0.03).
Table 2.
Comparison of Rational-Experiential Inventory Means of Participants
We also compared the mean rational and experiential REI scores between the student pharmacists in our study and those of health professions populations from 4 other studies (Table 3).5,12,14,15 Like the other health professions populations presented, namely practicing emergency physicians, cardiologists, and paramedics, the student pharmacists in our study favored rational decision making over experiential decision making. The student pharmacists in our study had significantly higher rational scores (p<0.01) and significantly lower experiential scores (p<0.01) than undergraduate students. Mean experiential scores for student pharmacists were also significantly lower than paramedics’ scores (p=0.02) and significantly higher than cardiologists’ scores (p<0.01).
Table 3.
Comparison of Rational-Experiential Inventory Means of Student Pharmacists Versus Study Samples of Other Health Professions Groups

DISCUSSION
Understanding the underlying preferences for student pharmacists’ decision making is critical for informing pharmacy education and developing educational approaches that promote good decisions. This study supported an extensive body of literature on dual-processing theory and CEST, which suggest that there are 2 independent modes of processing that operate simultaneously and sequentially during decision making.5,8,11 In our sample, the total scale reliabilities were high, suggesting 2 distinct information-processing systems. While student pharmacists used both rational and experiential decision-making styles, this population more strongly endorsed analytical and structured processes. Although this is the first study to measure REI in student pharmacists, these findings are consistent with studies using the Myers-Briggs Type Indicator, which show that pharmacists and student pharmacists prefer sensing (also described as fact-oriented, sequential, or logical) over intuition.17-19
Decision making is a complex process that can vary based on individual, social, and context-specific influences. To some extent, professions attract individuals with personality preferences that are compatible with the tasks required.17,20 This study revealed that student pharmacists are unique with regards to their decision-making processes. While REI research examining gender differences has consistently shown that female subjects prefer and rely more on experiential processes, the average rational, r-ability, and r-engagement scores for the female students in our study were higher than the corresponding experiential scores. Also, prior to this study, no relationship between age and the rational scale had been documented.12,21 Differences by age have been examined in various populations, including adults 20 to 74 years old21 and practicing health professionals 20 to 60 years old and over 60 years old.12 Preferences for experiential decision making can decline with age;21 however, this is the first study to demonstrate lower scores in rational decision making among older students. Although 1 of the original assumptions of CEST was an increasing dominance of rational processing from childhood to maturity,9 our study showed that the reverse could happen in older students. Understanding this finding warrants further investigation.
Given the systematic processes and analytic tasks frequently associated with pharmacy practice, students enrolled in a PharmD program not surprisingly favor rational processes. The process of evaluating the appropriateness of a patient’s medication regimen, for example, involves a systematic analysis of numerous factors (ie, patient age, indication, dosing considerations, drug allergies, concomitant disease states, laboratory values, vital signs, potential drug interactions, access to care issues, health literacy, cultural issues, patient values, tolerability, overall health status, and evidence-based practices). This study, coupled with research showing that clinical decisions based on intuition or experience alone can overestimate drug efficacy and underestimate drug risks,3 supports ongoing efforts to teach EBM strategies.22 With rational tendencies and preferences, student pharmacists should favor the use of EBM because it draws from a systematic and analytic process to support decision making.4
Although the student pharmacists in this study demonstrated tendencies toward rational decision making, the importance of experiential decision making in pharmacy should not be overlooked. Experiential decision making is faster and can increase efficiency of routine tasks. It also can help with unconscious recognition of errors. For example, when checking an intravenous solution prepared by a new technician, even though the correct amounts of drug and fluid were used, the pharmacist may feel that something “does not look right.” This spurs a closer review of the product and materials used, which may help the pharmacist determine that a regular needle was used when a filtered one should have been used. However, the effectiveness of intuition in decision making is positively related to level of domain expertise,23 ie, the decision-making process benefits from intuition when an individual’s implicit knowledge extends or adds value to explicit or rule-based knowledge.24 Early in the curriculum, most student pharmacists lack the clinical experience and professional confidence needed to bolster experiential decision making in clinical situations. As such, instructors should consider how to foster the development of experiential decision making in student pharmacists as well as the understanding that the effective use of this type of processing requires a certain amount of expertise.
While this study provided significant insight into student pharmacist decision making, additional areas of research warrant future consideration. First, the decision-making preferences of student pharmacists could have significant implications for experiential education in which the knowledge and skills obtained during the classroom portion of the curriculum are applied to clinical problems. Instructional methods in residency training, which have been endorsed by the American Society of Health-System Pharmacists, also focus on teaching clinical problem-solving skills to students in clinical practice. This model describes preceptor roles that facilitate the advancement to higher-order learning using methods tailored to the learner that begin with direct instruction, progress to modeling and coaching, and finally advance to facilitating.24 Understanding the relationship between decision-making style and student performance in advanced pharmacy practice experiences (APPEs), and the effect of pharmacy experiential learning on decision-making preference could inform pharmacy curriculum development and preceptors’ approaches to teaching clinical problem solving.25 Second, conducting a study of the decision-making tendencies of practicing pharmacists could have important implications in fostering effective decision-making skills, especially as they relate to complex drug-therapy management and therapeutic dilemmas.
This study provides insight into the decision-making preferences of student pharmacists; however, it has several limitations. This study examined a sample from a single school of pharmacy. To fully understand rational and experiential decision making for student pharmacists and pharmacists in general, the research should be extended to other institutions and to workplace settings. In addition, the study sample was limited to P3 student pharmacists. Although professions can attract individuals with preferences that are compatible with the tasks required,17,20 having completed 2 years of pharmacy school may have impacted students’ decision-making preferences. Examining the decision-making preferences of first-year student pharmacists could provide insight into the preferences of students upon entry to a pharmacy program. Furthermore, the REI-40 measures perceived ability and enjoyment of cognitive and intuitive tasks and not actual decision-making behavior. Future research should consider data collection methods that use direct evidence, such as measuring actual decision making.
CONCLUSION
Pharmacists face a wide range of situations that require effective and appropriate decision making. Most of the student pharmacists in this study favored rational over experiential decision-making styles, which was similar to the findings in studies done of other health professions. Future research should examine decision making in APPEs, other student pharmacist sample populations, and practicing pharmacists.
ACKNOWLEDGEMENTS
The authors thank Andrew Clapper for his assistance with survey instrument administration.
REFERENCES
- 1.Eddy D.Probablistic reasoning in clinical medicine: problems and opportunities Kahneman D, Slovic P, Tversky A.Judgment Under Uncertainty: Heuristics and Biases New York, NY: Cambridge University Press; 1982249-267 [Google Scholar]
- 2.Bryant PJ, Pace HA, editors. The Pharmacist's Guide to Evidence-based Medicine for Clinical Decision Making. ASHP: 2008. [Google Scholar]
- 3.Phansalkar S, Hoffman JM, Hurdle JF, Patel VL. Understanding pharmacist decision making for adverse drug event (ADE) detection. J Eval Clin Pract. 2009;15(2):266–275. doi: 10.1111/j.1365-2753.2008.00992.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bartels CE. Minneapolis, MN: University of Minnesota; 2013. Analysis of experienced pharmacist clinical decision-making for drug therapy management in the ambulatory care setting [dissertation] [Google Scholar]
- 5.Epstein S, Pacini R, Denes-Raj V, Heier H. Individual differences in intuitive-experiential and analytical-rational thinking styles. J Pers Soc Psychol. 1996;71(2):390–405. doi: 10.1037//0022-3514.71.2.390. [DOI] [PubMed] [Google Scholar]
- 6.Pacini R, Epstein S. The relation of rational and experiential information processing styles to personality, basic beliefs, and the ratio-bias phenomenon. J Pers Soc Psychol. 1999;76(6):972–987. doi: 10.1037//0022-3514.76.6.972. [DOI] [PubMed] [Google Scholar]
- 7.Sladek RM, Phillips PA, Bond MJ. Implementation science: a role for parallel dual processing models of reasoning? Implement Sci. 2006;1:12. doi: 10.1186/1748-5908-1-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Epstein S. The implications of cognitive-experiential self-theory for research in social psychology and personality. J Theory Soc Behav. 1985;15(3):283–310. [Google Scholar]
- 9.Epstein S. Integration of the cognitive and the psychodynamic unconscious. Am Psychol. 1994;49(8):709–724. doi: 10.1037//0003-066x.49.8.709. [DOI] [PubMed] [Google Scholar]
- 10.Witteman C, van den Bercken J, Claes L, Godoy A. Assessing rational and intuitive thinking styles. Eur J Psychol Assess. 2009;25(1):39–47. [Google Scholar]
- 11.Epstein S. Cognitive-experiential self-theory of personality. In: Millon T, Lerner MJ, editors. Personality and Social Psychology. New York: Wiley; 2003. [Google Scholar]
- 12.Calder LA, Forster AJ, Stiell IG, et al. Experiential and rational decision making: A survey to determine how emergency physicians make clinical decisions. Emerg Med J. 2012;29(10):811–816. doi: 10.1136/emermed-2011-200468. [DOI] [PubMed] [Google Scholar]
- 13.West M, O’Donnell M. Personality type and curriculum preference in primary care. Med Educ. 1982;16(2):94–96. doi: 10.1111/j.1365-2923.1982.tb01231.x. [DOI] [PubMed] [Google Scholar]
- 14.Sladek RM, Bond MJ, Huynh LT, Chew DPB, Phillips PA. Thinking styles and doctors’ knowledge and behaviours relating to acute coronary syndromes guidelines. Implement Sci. 2008;3:23. doi: 10.1186/1748-5908-3-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jensen J, Calder L, Walker M, et al. Experiential and rational clinical decision making: A survey to determine decision-making styles of paramedics. Can J Emerg Med. 2013;15(S1) [Google Scholar]
- 16.Gunnell JJ, Ceci SJ. When emotionality trumps reason: a study of individual processing style and juror bias. Behav Sci Law. 2010;28(6):850–877. doi: 10.1002/bsl.939. [DOI] [PubMed] [Google Scholar]
- 17.Hardigan PC, Cohen SR. A comparison of osteopathic, pharmacy, physical therapy, physician assistant, and occupational therapy students' personality styles: implications for education and practice. J Pharm Teach. 1999;7(2):67–79. [Google Scholar]
- 18.Lowenthal W. Myers-Briggs Type Inventory preferences of pharmacy students and practitioners. Eval Health Prof. 1994;17(1):22–42. [Google Scholar]
- 19.Shuck AA, Phillips CR. Assessing pharmacy students' learning styles and personality types: a ten-year analysis. Am J Pharm Educ. 1999;63(Spring):27–33. [Google Scholar]
- 20.Silberman SL, Cain MJ, Mahan JM. Dental students’ personality: a Jungian perspective. J Dent Educ. 1982;46(11):646–651. [PubMed] [Google Scholar]
- 21.Sladek RM, Bond MJ, Phillips PA. Age and gender differences in preferences for rational and experiential thinking. Pers Individ Dif. 2010;49(8):907–911. [Google Scholar]
- 22.Brown TE, Carter BL, Butler CK. Using decision analysis to modify clinical decisions made by pharmacists and students. Am J Pharm Educ. 1995;59(1):14–19. [Google Scholar]
- 23.Dane E, Rockmann KW, Pratt MG. When should I trust my gut? Linking domain expertise to intuitive decision-making effectiveness. Organ Behav Hum Decis Process. 2012;119(2):187–194. [Google Scholar]
- 24.Plessner H, Czenna S.The benefits of intuition Plessner H, Betsch C, Betsch T.Intuition in Judgment and Decision Making Mahwah, NJ: Lawrence Erlbaum; 2008251–265 [Google Scholar]
- 25.Weitzel KW, Walters EA, Taylor J. Teaching clinical problem solving: a preceptor’s guide. Am J Health-Syst Pharm. 2012;69(18):1588–1599. doi: 10.2146/ajhp110521. [DOI] [PubMed] [Google Scholar]