

Abstract
Patient: Male, 11
Final Diagnosis: Fibroepithelial polyp of epiglottis
Symptoms: Dysphagia • sore throat
Medication: —
Clinical Procedure: —
Specialty: —
Objective:
Rare disease
Background:
Fibroepithelial polyp, a common type of tumor in the skin and genitourinary tract, is very rare in the respiratory tract. We describe clinical, radiologic, and histological features of a fibroepithelial polyp as a rare cause of an epiglottic mass in a child.
Case Report:
An 11-year-old female presented with a 2-month history of sore throat and dysphagia. Flexible laryngoscopy and MRI (magnetic resonance imaging) revealed a mass on the lingual surface of the epiglottis. The mass was removed using a carbon dioxide laser and was confirmed histologically as a fibroepithelial polyp.
Conclusions:
Fibroepithelial polyp, although uncommon, should be considered in the differential diagnosis of epiglottic mass in children.
MeSH Keywords: Child; Epiglottis; Neoplasms, Fibroepithelial
Background
Fibroepithelial polyp is a benign lesion with mesodermal origin. The estimated prevalence of fibroepithelial polyp is 1.2%, with a male predilection [1]. Chronic inflammatory process has been suggested in the etiology of fibroepithelial polyp. Fibroepithelial polyps may have congenital, infectious, and traumatic origins [2]. The skin and genitourinary tract are common sites for fibroepithelial polyps. Fibroepithelial polyps in the head and neck region are documented in the external auditory canal, nasal cavity, oropharynx, hypopharynx, trachea, and bronchus [3–7]. To date, fibroepithelial polyp arising from the epiglottis has not been reported. Here, we describe clinical, radiologic, and histological features of a fibroepithelial polyp as a rare cause of an epiglottic mass in a child.
Case Report
An 11-year-old girl was referred to a tertiary care children’s hospital for assessment of an epiglottis mass. The child had a 2-month history of intermittent sore throat and discomfort with swallowing. The sore throat and discomfort with swallowing progressed without a history of fever, hoarseness, breathing difficulty, voice change, weight loss, night sweats, hemoptysis, or change in appetite. The birth history was un-remarkable; the patient had never been hospitalized and had never undergone surgery. Past medical history and family history also were unremarkable.
Physical examination revealed a well-appearing child in no respiratory distress, normal otologic exam results, and normal nasal exam results. A flexible laryngoscopic exam showed a mass with base attached to the lingual surface of the epiglottis. Attachment of the mass appeared to involve the majority of the right side of the epiglottis. No attachment to the tongue base was noted. The remainder of the glottis was within normal limits with good mobility of true vocal folds. No other abnormality was found in the head and neck region. MRI revealed a lobulated mass appearing hyperintense on T1- (Figure 1A) and T2-weighted images (Figure 1B). No intrinsic signal abnormality of the adjacent vallecula or tongue base was noted. After contrast administration, the mass showed no enhancement (Figure 1C).
Figure 1.

Axial T1-weighted (A) and T2-weighted (B) images show a lobulated mass along the free edge of the epiglottis to the right of midline. The mass was hyperintense. No intrinsic signal abnormality of the adjacent vallecula or tongue base was noted. Post contrast administration, the mass showed no enhancement (C).
The mass was removed with the aid of the CO2 laser and submitted for pathologic examination. Light microscopic examination showed features consistent with a fibroepithelial polyp (Figure 2).
Figure 2.
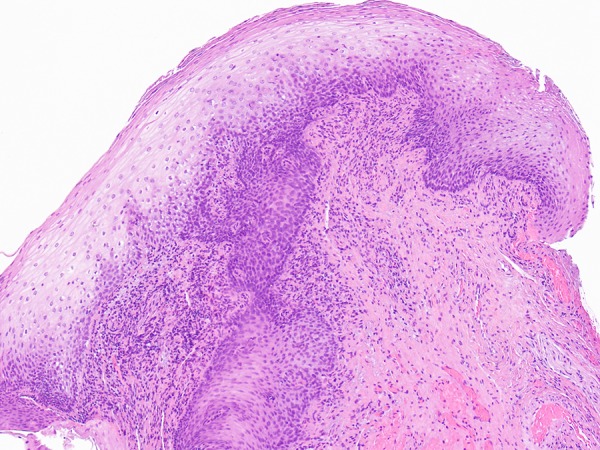
Photomicrograph of the epiglottic mass shows shows features consistent with a fibroepithelial polyp (hematoxylin and eosin, 100× total magnification).
Discussion
We documented the clinical presentation and management of a unique case of fibroepithelial polyp involving the epiglottis. The mass was identified when the patient became symptomatic and suffered from dysphagia and sore throat. Symptoms of fibroepithelial polyp are usually due to local mass effect. Depending on the size and location of the mass, the clinical presentations may include a wide variety of symptoms such as difficulty breathing, snoring, disturbed sleep, feeling something in the throat, or aural fullness. Fibroepithelial polyps of the pharynx or tracheobronchial tree may present as an acute medical emergency, causing upper airway obstruction. In the presence of airway obstruction, the airway must be secured.
Fibroepithelial polyps are rare benign tumors with low incidence of malignancy [8]. The etiology of fibroepithelial polyps has not been established. Fibroepithelial polyps may have congenital, infectious, inflammatory, and traumatic origins. The clinical differential diagnosis for epiglottic mass in children encompasses a wide spectrum of lesions, including, but not limited to, granulomatous lesions (tuberculosis, sarcoidosis, Wegener’s granulomatosis), infectious lesions (cat-scratch disease, fungal infections), neoplastic lesions, and systematic diseases (systemic lupus erythematosus, rheumatoid arthritis, relapsing polychondritis, and amyloidosis).
Radiologic assessment of an epiglottic mass in a child is useful to assess the origin and extent of the mass, to aid differential diagnosis, and to plan surgery. Computed tomography (CT) provides assessment of the mass and the surrounding bony changes; however, CT cannot discriminate between fibroepithelial polyp and other mass lesions of the epiglottis. MRI aids surgery planning by delineating the characteristics and extent of the mass. In the presence of a mass without rich vascular structures, the risk of bleeding during an endoscopic transoral excision is small.
Considering the potential to grow and possibility of complications, the treatment of choice for fibroepithelial polyp of the epiglottis is surgical excision and definitive diagnosis is made by histologic examination. Histological examination of fibroepithelial polyps demonstrates connective tissue covered by normal respiratory epithelium. Compared to papillomas, fibroepithelial polyps lack squamous epithelial overgrowth.
Conclusions
The present case emphasizes that fibroepithelial polyp should be included as one of the possible differential diagnoses in patients with epiglottic mass.
References:
- 1.Bouquot JE, Gunlach KKH. Oral exophytic lesions in 23616 white Americans over 35 years of age. Oral Surg Oral Med Pathol Oral Radiol Endod. 1986;62:284–91. doi: 10.1016/0030-4220(86)90010-1. [DOI] [PubMed] [Google Scholar]
- 2.Hasegawa Y, Mita K, Ueki T, et al. Retroperitoneoscopic treatment of ureteral invagination caused by a long fibroepithelial polyp protruding into the bladder: report of a case. Surg Today. 2011;41:1117–21. doi: 10.1007/s00595-010-4422-x. [DOI] [PubMed] [Google Scholar]
- 3.Li M, Zhang G, Peng A, Wang C. Bronchial fibroepithelial polyp: a case report and review of the literature. Intern Med. 2013;52(3):373–76. doi: 10.2169/internalmedicine.52.8864. [DOI] [PubMed] [Google Scholar]
- 4.Tanaka N, Matsunobu T, Shiotani A. Fibroepithelial polyp of the external auditory canal: a case report and a literature review. Case Rep Otolaryngol. 2013;2013:818197. doi: 10.1155/2013/818197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ushiki A, Yasuo M, Tanabe T, et al. A rare case of a tracheal fibroepithelial polyp treated by an endobronchial resection. Intern Med. 2008;47(19):1723–26. doi: 10.2169/internalmedicine.47.1241. [DOI] [PubMed] [Google Scholar]
- 6.Cho WK, Park JH, Paik JS, et al. A case of congenital orbital fibroepithelial polyp. Ophthal Plast Reconstr Surg. 2013;29(4):e107–8. doi: 10.1097/IOP.0b013e31827f59b9. [DOI] [PubMed] [Google Scholar]
- 7.Farboud A, Trinidade A, Harris M, Pfleiderer A. Fibroepithelial polyp of the tonsil: case report of a rare, benign tonsillar lesion. J Laryngol Otol. 2010;124(1):111–12. doi: 10.1017/S0022215109991198. [DOI] [PubMed] [Google Scholar]
- 8.Eads TJ, Chuang TY, Fabre’ VC, et al. The utility of submitting fibroepithelial polyps for histological examination. Arch Dermatol. 1996;132:1459–62. [PubMed] [Google Scholar]