

Abstract
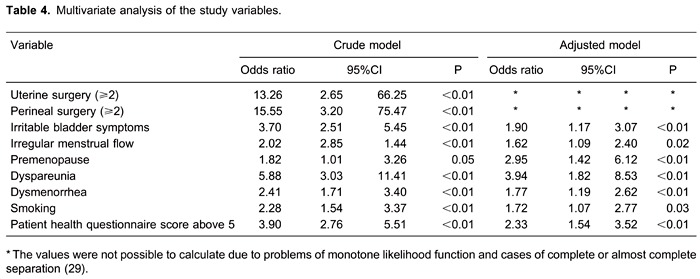
The objective of the present study was to estimate the prevalence of chronic pelvic pain in the community of São Luís, capital of the State of Maranhão, Northeastern Brazil, and to identify independent conditions associated with it. A cross-sectional study was conducted, including a sample of 1470 women older than 14 years predominantly served by the public health system. The interviews were held in the subject's home by trained interviewers not affiliated with the public health services of the municipality. The homes were visited at random according to the city map and the prevalence of the condition was estimated. To identify the associated conditions, the significant variables (P=0.10) were selected and entered in a multivariate analysis model. Data are reported as odds ratio and 95% confidence interval, with the level of significance set at 0.05. The prevalence of chronic pelvic pain was 19.0%. The independent conditions associated with this diagnosis were: dyspareunia (OR=3.94), premenopausal status (OR=2.95), depressive symptoms (OR=2.33), dysmenorrhea (OR=1.77), smoking (OR=1.72), irregular menstrual flow (OR=1.62), and irritative bladder symptoms (OR=1.90). The prevalence of chronic pelvic pain in Sao Luís is high and is associated with the conditions cited above. Guidelines based on prevention and/or early identification of risk factors may reduce the prevalence of chronic pelvic pain in São Luís, Brazil.
Keywords: Chronic pelvic pain, Prevalence, Dyspareunia, Dysmenorrhea
Introduction
Chronic pelvic pain (CPP) is a highly prevalent and debilitating clinical condition with a significant impact on the social, working and family activities of women, negatively affecting their quality of life. Some factors contribute to the variability of prevalence, among them the characteristics and quality of the studies, the definition used, the prevalence of sexually transmissible diseases, and the cultural characteristics of the population studied (1). The prevalence rates have ranged from 2.1 (2,3) to 43.4% (4). The studies reporting them are heterogeneous, nevertheless, a high quality study found a prevalence rate of 24% (5). It is a clinical condition whose cause in most cases is not identified and usually results from a complex interaction between the gastrointestinal, urinary, gynecological, musculoskeletal, neurologic, psychological and endocrine systems, and is additionally influenced by sociocultural factors. Any abdominal and/or pelvic region may be involved in the etiology of CPP, with no consensus existing about the diseases that may cause it, although endometriosis, interstitial cystitis, pelvic inflammatory disease, irritable bowel syndrome, constipation and pelvic adhesions are those most often associated with it (6).
In a recent systematic review, Latthe et al. (7) observed that drug or alcohol abuse, miscarriage, heavy menstrual flow, pelvic inflammatory disease, previous cesarean section, pelvic pathology, abuse, and psychological comorbidity were associated with an increased risk of noncyclical pelvic pain. However, few survey studies worldwide have evaluated the condition. Our group observed a prevalence of approximately 11% in the Southeast of Brazil, and identified as associated independent conditions: dyspareunia, previous abdominal surgery, depression, dysmenorrhea, anxiety, current sexual activity, low back pain, constipation, irritative urinary symptoms, and low educational level (8). We believe that this information is important because our country shares many characteristics with other developing countries around the world. However, Brazil is a vast and culturally heterogeneous territory, so that the conclusion of that study alone cannot be generalized to the country as a whole. Furthermore, some conditions, such as educational level, are not similar in all States or Regions of Brazil. Because of this, healthcare policies may be different in order to set targets to prevent or minimize the occurrence or impact of CPP. Recently, the University Hospital at São Luís created a service specialized in the care of women with CPP in response to a request from health professionals in the region. On this basis, we carried out the present study with the aim of investigating the community prevalence of CPP in São Luís, Brazil, as well as eventual clinical conditions associated with it.
Material and Methods
Study design
This was a cross-sectional survey study conducted during the period from June 2009 to May 2010. It followed the Declaration of Helsinki set of principles and was approved by the Local Research Review Board. All subjects or those responsible for them gave written informed consent to participate.
Setting
The subjects were recruited in the urban area of the municipality of São Luís, capital of the State of Maranhão, Northeastern Brazil, with an estimated population of 1,014,837 inhabitants, 539,842 of them women (53.2%). According to the latest demographic census (2010) (http://cidades.ibge.gov.br/xtras/perfil.php?lang=&codmun=211130&search=||infogr%E1ficos:-informa%E7%F5es-completas), 511,515 of these women (94.8%) are estimated to live in the urban zone. A total of 876,826 inhabitants residing in the municipality (86.4%) are literate and the mean household per capita income is R$645.00 (approximately US$360.00), while the median is R$430.00 (approximately US$240.00).
Participants
The study included 1470 women who were interviewed at home. The target population consisted of women who use exclusively the Unified Health System. Only women aged at least 14 years and having had menarche were included in the study. The maximum age was 60 years.
Variables
We adopted the definition of CPP proposed by the American Congress of Obstetricians and Gynecologists (ACOG): “A noncyclic pain of 6 or more months' duration that localizes to the anatomic pelvis, anterior abdominal wall at or below the umbilicus, and is of sufficient severity to cause functional disability or lead to medical care”. All women with a diagnosis of the condition were referred to the city hospital specializing in women's health and the diagnosis was confirmed before inclusion in the data bank.
The visual analogue scale (VAS) was used to assess the intensity of pain, an instrument extensively employed in clinical practice because of its rapid use and clinical applicability. We considered patients to have significant pain when their VAS score was 30 mm or higher and when they had at least one pain episode per week.
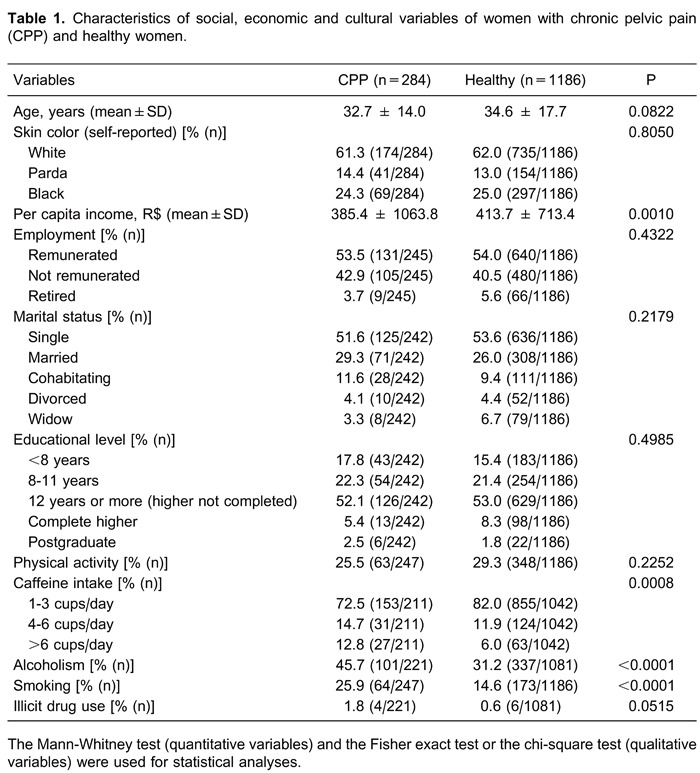
The variables evaluated were grouped as social, economic, and cultural: age, skin color (self-reported), per capita income, employment, marital status, educational level, physical activity (women who engaged in activities such as running, walking, pedaling, dancing, or other sport activity for at least 150 min a week; according to the World Health Organization <http://www.who.int/topics/physical_activity/en/>), caffeine intake, alcoholism (excessive intake during the weekend with frequent drunkenness and/or daily consumption with or without drunkenness), smoking (current or former daily smoker), and illicit drug use.
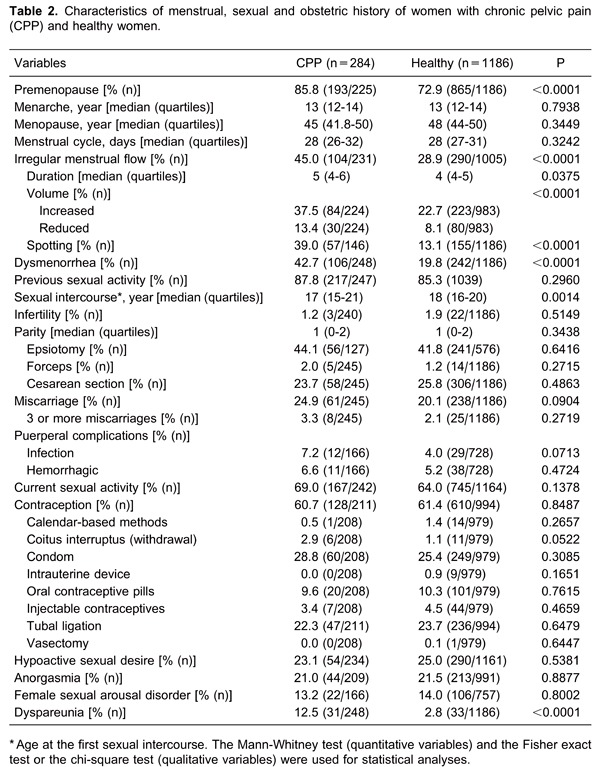
Sexual, menstrual and obstetric history: menstrual status, age at menarche, age at menopause, menstrual cycle (number of days), regularity of menstrual flow (volume: divided into increased or reduced subjectively; duration: normal when it lasted from 2 to 8 days), spotting (intermenstrual bleeding considered when presented in most cycles in the last 6 months), dysmenorrhea, previous sexual activity, age at first sexual intercourse, infertility (defined as proposed by the WHO when the woman has not become pregnant after 2 years of regular sexual intercourse, without contraception), parity, episiotomy, forceps, cesarean section, miscarriage, puerperal complications, current sexual activity, contraception, sexual disorders (hypoactive sexual desire, anorgasmia, female sexual arousal disorder, and dyspareunia), sexual and physical violence.
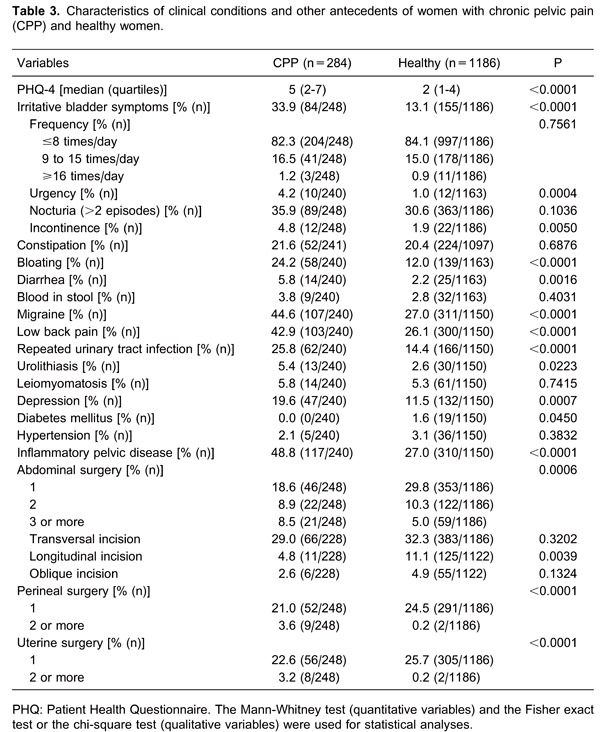
Clinical conditions and other antecedents: PHQ-4 (Patient Health Questionnaire: a 4-item measure of symptoms of depression) (9,10), urinary symptoms (frequency, urgency, nocturia, incontinence), intestinal symptoms (functional bowel disorders by Rome III criteria) (11): constipation, bloating, diarrhea, and blood in stool; comorbidities previously diagnosed such as inflammatory pelvic disease, migraine, low back pain, repetition urinary tract infection (three or more episodes in the last year), urinary calculi, leiomyomatosis, depression, diabetes mellitus, chronic hypertension, abdominal surgeries (number and incision type), perineal surgeries (such as colpoplasty, hemorrhoidectomy), uterine surgeries (such as curettage, hysteroscopy).
Data sources
A questionnaire was chosen as the collection instrument because it is applicable to all segments of the population studied, which is quite heterogeneous, containing both illiterate and literate people. The interviews were held in a private environment. The interviewers, who were not affiliated with the city health care programs, were trained and selected by the researcher responsible for the study. The data collected by the interviewers were entered during the interview and sent to an electronic database (software Filemaker¯ Pro Advanced 8, USA). Five percent of the subjects were selected at random and re-interviewed to check data consistency. Independent investigators who did not participate directly in data collection carried out the analyses. All women with symptoms suggestive of chronic pelvic pain during the interview were sent to specialized service in order to confirm the diagnosis by a physician. Two women did not attend, but a physician visited them and he did not confirm the diagnosis due to absence of symptoms.
Bias
Sample selection was random by cluster sampling (stratification by area and estimated population density) in a stepwise manner. The sampling process consisted of areas chosen at random by drawing lots after analysis of maps of the city neighborhoods, followed by systematic sampling with a withdrawal interval proportional to the number of residences and local population density. All women in the household were invited to participate in the study.
Study size
The sample size was defined considering a population estimated of 539,842 women, confidence interval of 95% (95%CI), maximum error of 1%, and estimated prevalence rate of 4%.
Statistical analysis
Statistical analysis was performed using the SAS¯ 9.0 software (USA). Analysis of the quantitative variables was performed by the Mann-Whitney test after some variables were found not to have normal distribution according to the Kolmogorov-Smirnov test, while qualitative variables were analyzed by the Fisher exact test or the chi-square test.
Logistic regression was used to identify the significant and independent variables and to estimate the simultaneous association of these factors in CPP. All variables with a P<0.10 in bivariate analysis and those we considered to be plausible to justify the pain and that were significant in other studies (7,8) were included in a logistic regression model. Simple and multiple logistic regressions were used to estimate the odds ratio. The analysis was carried out using the PROC LOGISTIC procedure of the SAS¯ 9.0 software and the best model observed was presented. We also report the 95% confidence interval, considering P<0.05.
Results
Participants
The characteristics of the subjects and the univariate analysis are presented in Tables 1, 2, and 3. Because of wide variability, it was not possible to divide the professional activities into groups. The activities most frequently reported were: student (23.6%), housewife (16.6%), maid (11.3%), retired (5.7%), teacher (5.4%), self-employed professional (3.5%), nurse technician (2.8%), storekeeper (2.6%), saleswoman (2.6%), and public servant (2.4%), among others.
Main results
The 1-year prevalence of CPP in São Luís, Brazil, was 19.0% (279/1470). The women with CPP had been symptomatic for 47.8±66.3 months (median: 20, range: 6-360 months) and presented an intensity of 63.2±20.0 mm (median: 60, range: 30-100 mm), with 8.6% (n=24) of them having symptoms compatible with allodynia.
A total of 58.4% (n=163) of the women stated that they took analgesics on a weekly or daily basis (paracetamol/acetaminophen/dipyrone) and/or non-steroidal anti-inflammatory drugs (NSAIDs) without a medical prescription.
In logistic analysis, the independent variables associated with CPP were: dyspareunia, premenopausal status, patient health questionnaire above 5, dysmenorrhea, smoking, irregular menstrual flow, and irritative bladder symptoms. The results of multivariate analysis are reported in detail in Table 4.
Discussion
The prevalence of CPP was 19.0% in the subjects of this study. Our two studies showed that Brazil is one of the countries with a higher prevalence of the condition, particularly in contrast to developed countries (7,8). In addition, a large part of the sample routinely used painkillers without a medical prescription, which predispose to several undesirable events, including financial expenditures without guarantee of clinical improvement.
We observed a significant association with dyspareunia, premenopausal status, patient health questionnaire score, dysmenorrhea, smoking, irregular menstrual flow, and irritative bladder symptoms. Most of them are associated symptoms and, probably are not sufficient to cause CPP. Our results also suggest that a history of previous perineal and uterine surgery are important elements associated with the development of CPP. However, some OR values did not converge due to sample size and the frequency of some characteristics.
Interpretation
Most of the associated conditions are symptoms without potential of causality. Although it is important to know them, it is necessary to reflect on the complexity of the determinants of the condition. The presence of dyspareunia, a high prevalent condition (7 to 75%) (12,13), was significantly higher in women with CPP. In a recent study, we had also observed that dyspareunia was associated with pelvic muscle tenderness (14). Although pelvic muscle tenderness may be a primary cause of CPP, we hypothesize that it is more often secondary to cross-talk communication between the viscera and muscles (15). The high prevalence of a history of a diagnosis of pelvic inflammatory disease in the last year, which in turn may explain the infertility rates, may also explain the occurrence of dyspareunia. That condition, in detriment of this last, was not confirmed in the adjusted model as an independent variable, probably due to overlap between them.
Depression disorders are frequently concomitant with chronic pain, particularly in women (16). The idea that pain, particularly chronic pain, can lead to feelings of frustration, worry, anxiety, and depression seems obvious. There is some evidence that it is the stress of living with chronic pain, and not personal or family predisposition, that causes depression in these patients (17). It, therefore, remains uncertain whether depression precedes or is a consequence of chronic pain (18).
Dysmenorrhea is a condition that is frequently concomitant with CPP. Its association with endometriosis or adenomyosis may explain the relationship to CPP (19). Several other hypotheses may be raised and we emphasize two that we believe to be more plausible: 1) low pain thresholds in women with CPP and dysmenorrhea (20) or even central sensitization induced by the primary disease (21) may favor the higher prevalence of dysmenorrhea in this group; 2) uterine inflammation secondary to neurogenic inflammation that is evident in animal models may result in viscero-visceral hyperalgesia between organs (22), a fact that may also explain uterine sensitivity in humans.
More recently, it has been discovered that smoking is a risk factor for chronic pain. Another epidemiological study conducted in Brazil also observed that smoking is an independent factor associated with chronic pain conditions (23). Robust epidemiological evidence is showing that smokers not only have higher rates of chronic pain but also rate their pain as more intense than nonsmokers (24). It has been observed that the act of smoking may be a way of dealing with stress and the already present long-lasting pain (coping strategy) (25). In the present study, smoking was a more important factor than alcohol drinking, though the latter is also an element significantly associated with chronic pain conditions and with smoking itself. Abnormal menstrual bleeding is a prevalent clinical problem among women of reproductive age.
In contrast to what we observed in Ribeirão Preto (8), we did not observe previous abdominal surgery and low educational level as independent factors. Regarding the former, although an association is plausible, we do not know if other confounding variables or even cultural aspects may have interfered with the results. Curiously, the presence of a previous abdominal surgery was not a variable associated with the condition, at least in this sample, even though a history of three or more previous abdominal surgeries was two times more frequent among women with CPP. Almost 40% of the women interviewed had already been submitted to at least one previous abdominal surgery. We consider this prevalence to be a potential source of concern. A quarter of the women had given birth by cesarean section. Thus, we emphasize the importance of recognizing abdominal myofascial syndrome and the neuralgias, particularly ilioinguinal and iliohypogastric ones, as a differential diagnosis (26). Regarding the second factor (educational level), the high frequency of subjects who had not concluded elementary school in both groups (almost 20%) may have influenced the findings.
Sexual, emotional, or physical abuse, particularly childhood sexual abuse, has been linked to CPP and to sexual dysfunction (27). Although many authors and clinicians have mentioned this association, it has also been suggested that both physical and sexual abuse may be associated with psychological distress in women with CPP but not with other domains of pain experience (28). Further studies in this field are essential to clarify the relationship between history of both abuse and violence and the development and promotion of chronicity of CPP.
Limitations
None of the women contacted refused to respond to the questionnaire, a fact that makes the results reliable, at least from the viewpoint of sample representation. All women had diagnosis confirmed by a physician before inclusion in the study. On the other hand, the questionnaire covers responses that are always subjective and that require memories and truthfulness. We believe that the accuracy of the information has been maintained because interviews were conducted in private and in a home environment of the participant.
Our study has identified that prevalence of CPP in São Luís is high and several independent conditions were associated with it. However, most of them are associated symptoms and, investigation of a possible causal relationship is essential. We believe that CPP is a condition determined by a complex interaction of numerous factors. Although abdominal surgeries and functional disorders of the intestine were not identified in the present study, we believe that special attention should be paid to this question. Further studies are necessary to corroborate our results.
Acknowledgments
We thank Ms. Elettra Greene for editing the English and the statistician Mayra Piani by statistical analysis. Research supported by the Program for the Implementation of Scientific Initiation Fellowships (Pibic) and by the Program of Academic Cooperation (PROCAD/CAPES).
Footnotes
First published online July 25, 2014.
References
- 1.Latthe P, Latthe M, Say L, Gulmezoglu M, Khan KS. WHO systematic review of prevalence of chronic pelvic pain: a neglected reproductive health morbidity. BMC Public Health. 2006;6:177. doi: 10.1186/1471-2458-6-177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rulin MC, Davidson AR, Philliber SG, Graves WL, Cushman LF. Long-term effect of tubal sterilization on menstrual indices and pelvic pain. Obstet Gynecol. 1993;82:118–121. [PubMed] [Google Scholar]
- 3.Zondervan KT, Yudkin PL, Vessey MP, Dawes MG, Barlow DH, Kennedy SH. Prevalence and incidence of chronic pelvic pain in primary care: evidence from a national general practice database. Br J Obstet Gynaecol. 1999;106:1149–1155. doi: 10.1111/j.1471-0528.1999.tb08140.x. [DOI] [PubMed] [Google Scholar]
- 4.Thongkrajai P, Pengsaa P, Lulitanond V. An epidemiological survey of female reproductive health status: gynecological complaints and sexually-transmitted diseases. Southeast Asian J Trop Med Public Health. 1999;30:287–295. [PubMed] [Google Scholar]
- 5.Zondervan KT, Yudkin PL, Vessey MP, Jenkinson CP, Dawes MG, Barlow DH, et al. The community prevalence of chronic pelvic pain in women and associated illness behaviour. Br J Gen Pract. 2001;51:541–547. [PMC free article] [PubMed] [Google Scholar]
- 6.ACOG Practice Bulletin No. 51. Chronic pelvic pain. Obstet Gynecol. 2004;103:589–605. [PubMed] [Google Scholar]
- 7.Latthe P, Mignini L, Gray R, Hills R, Khan K. Factors predisposing women to chronic pelvic pain: systematic review. BMJ. 2006;332:749–755. doi: 10.1136/bmj.38748.697465.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Silva GP, Nascimento AL, Michelazzo D, Alves Junior FF, Rocha MG, Silva JC, et al. High prevalence of chronic pelvic pain in women in Ribeirao Preto, Brazil and direct association with abdominal surgery. Clinics. 2011;66:1307–1312. doi: 10.1590/S1807-59322011000800001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kroenke K, Spitzer RL, Williams JB. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41:1284–1292. doi: 10.1097/01.MLR.0000093487.78664.3C. [DOI] [PubMed] [Google Scholar]
- 10.de Lima Osorio F, Vilela Mendes A, Crippa JA, Loureiro SR. Study of the discriminative validity of the PHQ-9 and PHQ-2 in a sample of Brazilian women in the context of primary health care. Perspect Psychiatr Care. 2009;45:216–227. doi: 10.1111/j.1744-6163.2009.00224.x. [DOI] [PubMed] [Google Scholar]
- 11.Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130:1480–1491. doi: 10.1053/j.gastro.2005.11.061. [DOI] [PubMed] [Google Scholar]
- 12.Heim LJ. Evaluation and differential diagnosis of dyspareunia. Am Fam Physician. 2001;63:1535–1544. [PubMed] [Google Scholar]
- 13.Danielsson I, Sjoberg I, Stenlund H, Wikman M. Prevalence and incidence of prolonged and severe dyspareunia in women: results from a population study. Scand J Public Health. 2003;31:113–118. doi: 10.1080/14034940210134040. [DOI] [PubMed] [Google Scholar]
- 14.Montenegro ML, Mateus-Vasconcelos EC, Rosa e Silva JC, Nogueira AA, Dos Reis FJ, Poli Neto OB. Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Med. 2010;11:224–228. doi: 10.1111/j.1526-4637.2009.00758.x. [DOI] [PubMed] [Google Scholar]
- 15.Pezzone MA, Liang R, Fraser MO. A model of neural cross-talk and irritation in the pelvis: implications for the overlap of chronic pelvic pain disorders. Gastroenterology. 2005;128:1953–1964. doi: 10.1053/j.gastro.2005.03.008. [DOI] [PubMed] [Google Scholar]
- 16.Castro M, Kraychete D, Daltro C, Lopes J, Menezes R, Oliveira I. Comorbid anxiety and depression disorders in patients with chronic pain. Arq Neuropsiquiatr. 2009;67:982–985. doi: 10.1590/S0004-282X2009000600004. [DOI] [PubMed] [Google Scholar]
- 17.Gallagher RM, Verma S. Managing pain and comorbid depression: A public health challenge. Semin Clin Neuropsychiatry. 1999;4:203–220. doi: 10.153/SCNP00400203. [DOI] [PubMed] [Google Scholar]
- 18.Fishbain DA, Cutler R, Rosomoff HL, Rosomoff RS. Chronic pain-associated depression: antecedent or consequence of chronic pain? A review. Clin J Pain. 1997;13:116–137. doi: 10.1097/00002508-199706000-00006. [DOI] [PubMed] [Google Scholar]
- 19.Fauconnier A, Chapron C. Endometriosis and pelvic pain: epidemiological evidence of the relationship and implications. Hum Reprod Update. 2005;11:595–606. doi: 10.1093/humupd/dmi029. [DOI] [PubMed] [Google Scholar]
- 20.Giamberardino MA, Berkley KJ, Iezzi S, de Bigontina P, Vecchiet L. Pain threshold variations in somatic wall tissues as a function of menstrual cycle, segmental site and tissue depth in non-dysmenorrheic women, dysmenorrheic women and men. Pain. 1997;71:187–197. doi: 10.1016/S0304-3959(97)03362-9. [DOI] [PubMed] [Google Scholar]
- 21.Bajaj P, Bajaj P, Madsen H, Arendt-Nielsen L. Endometriosis is associated with central sensitization: a psychophysical controlled study. J Pain. 2003;4:372–380. doi: 10.1016/S1526-5900(03)00720-X. [DOI] [PubMed] [Google Scholar]
- 22.Giamberardino MA, Costantini R, Affaitati G, Fabrizio A, Lapenna D, Tafuri E, et al. Viscero-visceral hyperalgesia: characterization in different clinical models. Pain. 2010;151:307–322. doi: 10.1016/j.pain.2010.06.023. [DOI] [PubMed] [Google Scholar]
- 23.Sa KN, Baptista AF, Matos MA, Lessa I. Chronic pain and gender in Salvador population, Brazil. Pain. 2008;139:498–506. doi: 10.1016/j.pain.2008.06.008. [DOI] [PubMed] [Google Scholar]
- 24.Weingarten TN, Shi Y, Mantilla CB, Hooten WM, Warner DO. Smoking and chronic pain: a real-but-puzzling relationship. Minn Med. 2011;94:35–37. [PubMed] [Google Scholar]
- 25.Patterson AL, Gritzner S, Resnick MP, Dobscha SK, Turk DC, Morasco BJ. Smoking cigarettes as a coping strategy for chronic pain is associated with greater pain intensity and poorer pain-related function. J Pain. 2012;13:285–292. doi: 10.1016/j.jpain.2011.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Loos MJ, Scheltinga MR, Roumen RM. Surgical management of inguinal neuralgia after a low transverse Pfannenstiel incision. Ann Surg. 2008;248:880–885. doi: 10.1097/SLA.0b013e318185da2e. [DOI] [PubMed] [Google Scholar]
- 27.Randolph ME, Reddy DM. Sexual abuse and sexual functioning in a chronic pelvic pain sample. J Child Sex Abus. 2006;15:61–78. doi: 10.1300/J070v15n03_04. [DOI] [PubMed] [Google Scholar]
- 28.Poleshuck EL, Dworkin RH, Howard FM, Foster DC, Shields CG, Giles DE, et al. Contributions of physical and sexual abuse to women's experiences with chronic pelvic pain. J Reprod Med. 2005;50:91–100. [PMC free article] [PubMed] [Google Scholar]
- 29.Albert A, Anderson JA. On the existence of maximum likelihood estimates in logistic regression models. Biometrika. 1984;71:1–10. doi: 10.1093/biomet/71.1.1. [DOI] [Google Scholar]