

Abstract
We present a case report where Tc-99m sulfur colloid single-photon emission computed tomography (SPECT)/computed tomography (CT) scan was useful in characterizing a soft tissue abdominal mass and helped with patient management. A 63-year-old male with no previous history of trauma had an incidental finding of a soft tissue nodule adjacent to the splenic hilum, unchanged in size over 4 months and with similar enhancing features as the spleen. A Tc-99m sulfur colloid SPECT/CT scan was performed to determine the nature of the nodule. It showed no uptake of tracer within this mass, therefore excluding splenic tissue. This prompted subsequent investigations and this tissue was found to represent a pancreatic neuroendocrine tumor, which was excised.
Keywords: Accessory spleen, neuroendocrine tumor, single-photon emission computed tomography/computed tomography, sulfur colloid
Introduction
Accessory splenic tissue can be difficult to differentiate from tumour on conventional cross-sectional imaging. We demonstrate in a case report how Tc-99m sulfur colloid single-photon emission computed tomography (SPECT)/computed tomography (CT) scan can be useful in characterizing a soft tissue abdominal mass and help with patient management.
Case Report
A 63-year-old male patient was referred to the hepatobiliary surgeons after an incidental finding of a well-defined nodule adjacent to the splenic hilum on an ultrasound scan investigating dysuria and urinary incontinence in January 2011. He had a previous Whipple's procedure in 1991 for distal cholangiocarcinoma and parathyroidectomy in 2007 for parathyroid adenoma. The lesion was subsequently investigated with a computed tomography (CT) in May 2011, which showed a 4.8 cm well-defined soft tissue mass in the region of the pancreatic tail remnant, close to the spleen with similar density and enhancing characteristics as the spleen [Figure 1a], with a further small 10 mm nodule posterior to this. This was thought to be a probable accessory spleen. A follow-up scan 4 months later showed no change in the size of the lesions [Figure 1b]. A Tc-99m sulfur colloid single-photon emission computed tomography (SPECT)/CT scan was arranged, which showed no uptake of tracer in these masses [Figure 2]. The patient underwent an endoscopic ultrasound and fine-needle aspiration. Fine-needle aspiration was performed and cytopathology was suggestive of an adenocarcinoma. The patient was admitted for elective completion distal pancreatectomy and splenectomy with an uneventful postoperative recovery. Histology of the resected specimen revealed a large, well-differentiated, intermediate grade neuroendocrine tumor (NET). Subsequently it was confirmed that the patient had multiple endocrine neoplasia-1.
Figure 1.
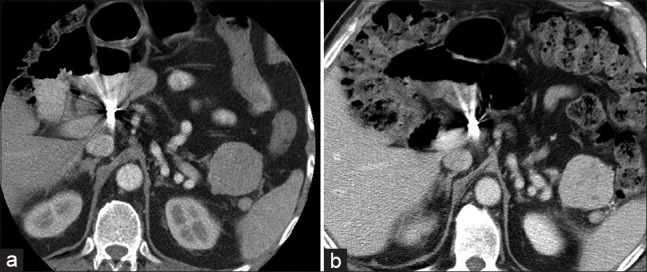
(a) Abdominal computed tomography (CT) showing a 4.8 cm well-defined soft tissue mass close to the spleen with similar density and enhancing characteristics as the spleen. A further 10 mm nodule is seen posterior to this. (b) Follow-up CT 4 months later showing unchanged that the soft tissue mass and nodule have not changed in size
Figure 2.
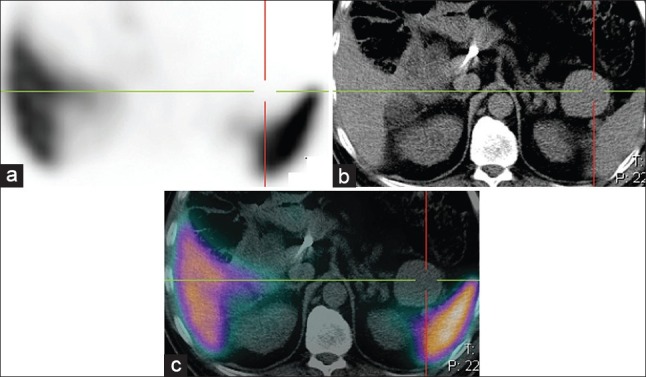
(a-c) Single-photon emission computed tomography (SPECT), computed tomography (CT) and SPECT-CT Tc-99m sulphur colloid study clearly demonstrates that there is no uptake of tracer within the soft tissue mass or adjacent nodule, excluding accessory spleen as a cause for the mass
Discussion
Ectopic splenic tissue can be the result of rupture of the spleen resulting in heterotopic autotransplanatation of splenic tissue (splenosis) or as a result of accessory splenic tissue, which has formed during embryonic development.[1] Whereas splenosis (which can be related to trauma or iatrogenic) can result in splenic tissue present almost anywhere in the body and may present in numbers >100,[2] accessory spleens are usually much less numerous (<6) and are usually <2 cm and are present close to the spleen, having its blood supply from a branch of the splenic artery.[3]
It is often difficult to differentiate splenic tissue from inflammatory or tumor cells on CT, particularly if they have similar enhancing pattern as the spleen. Thus, functional imaging can be useful in these situations.
The two nuclear medicine tests that have been used to identify splenic tissue are Tc-99m colloid scans[4] and Tc-99m heat damaged red blood cells.[5] Tc-99m labeled colloid is taken up by the reticuloendothelial system after intravenous injection and is thus taken up by the liver, spleen and bone marrow. In the past, detection of small nodules were limited by both the resolution of planar/SPECT images and the location of the lesion (nodules close to the spleen may not easily be visualized due to scatter from the spleen). With the development of high quality SPECT/CT cameras, it has become easier to accurately characterize small nodules, and thus reduce the number of indeterminate studies.
There have been a number of case reports where intra-abdominal splenosis or accessory spleens have mimicked metastatic cancer.[6,7,8,9,10] However, to the best of our knowledge, this to be the first report of a Tc-99m sulfur colloid SPECT/CT study used to exclude splenic tissue.
Neuroendocrine tumors may be slow growing and as was shown in this case, appearances may not change in 4 months interval. Functional imaging with somatostatin receptor imaging (e.g. In-111-pentetreotide or Ga-68-DOTATATE) would not have differentiated splenic tissue from NET as uptake within the spleen is part of the normal physiological distribution on somatostatin receptor imaging.[11]
Conclusion
This case demonstrates that Tc-99m sulfur colloid SPECT/CT scan can be useful to differentiate splenic tissue from nonsplenic tissue, and should be performed to characterize abdominal masses suspicious to represent splenosis or accessory spleen if clinically relevant.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Halpert B, Gyorkey F. Lesions observed in accessory spleens of 311 patients. Am J Clin Pathol. 1959;32:165–8. doi: 10.1093/ajcp/32.2.165. [DOI] [PubMed] [Google Scholar]
- 2.Brewster DC. Splenosis. Report of two cases and review of the literature. Am J Surg. 1973;126:14–9. doi: 10.1016/s0002-9610(73)80086-8. [DOI] [PubMed] [Google Scholar]
- 3.Mohan H, Amanjit B, Bhardwaj S, Handa U. Splenunculi-Report of three cases. J Anat Soc India. 2002;51:70–1. [Google Scholar]
- 4.Castellani M, Cappellini MD, Cappelletti M, Fedriga E, Reschini E, Cerino M, et al. Tc-99m sulphur colloid scintigraphy in the assessment of residual splenic tissue after splenectomy. Clin Radiol. 2001;56:596–8. doi: 10.1053/crad.2000.0674. [DOI] [PubMed] [Google Scholar]
- 5.Schiff RG, Leonidas J, Shende A, Lanzkowski P. The noninvasive diagnosis of intrathoracic splenosis using technetium-99m heat-damaged red blood cells. Clin Nucl Med. 1987;12:785–7. doi: 10.1097/00003072-198710000-00005. [DOI] [PubMed] [Google Scholar]
- 6.Liu Y, Ji B, Wang G, Wang Y. Abdominal multiple splenosis mimicking liver and colon tumors: A case report and review of the literature. Int J Med Sci. 2012;9:174–7. doi: 10.7150/ijms.3983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Short NJ, Hayes TG, Bhargava P. Intra-abdominal splenosis mimicking metastatic cancer. Am J Med Sci. 2011;341:246–9. doi: 10.1097/maj.0b013e318202893f. [DOI] [PubMed] [Google Scholar]
- 8.Gincu V, Kornprat P, Thimary F, Jahn S, Mischinger HJ. Intestinal obstruction caused by splenosis at the rectosigmoid junction, mimicking malignant pelvic tumor. Endoscopy. 2011;43 (Suppl 2 UCTN):E260. doi: 10.1055/s-0030-1256523. [DOI] [PubMed] [Google Scholar]
- 9.Kang KC, Cho GS, Chung GA, Kang GH, Kim YJ, Lee MS, et al. Intrahepatic splenosis mimicking liver metastasis in a patient with gastric cancer. J Gastric Cancer. 2011;11:64–8. doi: 10.5230/jgc.2011.11.1.64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rizzo S, Monfardini L, Belmonte M, Rocco B, Belloni M. Benign splenosis mimicking peritoneal seeding in a bladder cancer patient: A case report. Cases J. 2009;2:8982. doi: 10.4076/1757-1626-2-8982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Balon HR, Goldsmith SJ, Siegel BA, Silberstein EB, Krenning EP, Lang O, et al. Procedure guideline for somatostatin receptor scintigraphy with (111) In-pentetreotide. J Nucl Med. 2001;42:1134–8. [PubMed] [Google Scholar]