

Abstract
Introduction
There has been an increase in the prevalence of erectile dysfunction (ED) in the general population especially among Diabetic patients. This seems to be neglected problem in low-income countries. This study aims at establishing the prevalence of ED and associated risk factors in diabetic patients attended at Diabetic Clinic at Muhimbili National Hospital.
Methods
A cross-sectional hospital based study was conducted among 312 diabetic patients attending diabetic clinic at Muhimbili National Hospital between May and December 2011.
Results
More than half (55.1%) of the patients were found to have some form of ED (12.8% had mild dysfunction, 11.5% moderate and 27.9% severe dysfunction). The severity of ED was correlated with increased age. Multivariate logistic regression revealed that ED was significantly predicted by old age (odds ratio (OR) = 7.1, 95% CI 1.2-40.7), evidence of peripheral neuropathy (OR) =5.9, 95% CI 1.6-21.3), and evidence of peripheral vascular disease (OR =2.5, 95% CI 1.2-5.3). Also longer duration of DM was marginally associated with ED (p=0.056). Patients with ED were also more likely to suffer other sexual domains (p<0.001). No lifestyle factor was associated with ED.
Conclusion
The prevalence of ED is high among DM patients. Interventions aimed at prevention, early diagnosis and detection of DM and its complications, and adherence to treatment to prevent complications should be implemented. Further studies should emphasize on temporal variation to show true causality of DM on erectile dysfunction.
Keywords: Diabetes mellitus, erectile dysfunction, sexual domains, peripheral vascular disease, monofilament score, peripheral neuropathy
Introduction
Erectile dysfunction (ED) defined as inability to achieve and maintain an erection sufficient to permit satisfactory sexual intercourse is documented to be a major problem especially among diabetic patients [1].
There are numerous causes of ED generally falling into two categories, organic or psychogenic. The organic causes can be subdivided into five categories: vascular, traumatic/post surgical, neurological, endocrine-induced, and drug-induced. Reported psychogenic causes include depression, performance anxiety, and relationship problems [2].
A variety of chronic illnesses such as diabetes mellitus DM), cardiovascular disease and depression are associated with higher rates of ED [3] where DM appears to be a major determinant [4]. In study that was done in Massachusetts, United States of America showed that diabetic men are 3 times as likely to develop ED as non-diabetic men [5]. Also increased duration of diabetes was shown to increases both the prevalence rate and severity of ED [6]. ED can occur early in the course of the disease and it can occasionally be the presenting symptom [7]. Some documented reports gave out the main risk factors of ED in people with diabetes as neuropathy, vascular insufficiency, poor glycemic control, hypertension, low testosterone levels, and lifestyle factors such as smoking, alcohol and inactivity. In addition the prevalence of ED greatly increases with age [8–11].
A wide range of prevalence rates of ED among diabetic men has been reported in various studies. These studies [6, 12–15] suggest that its prevalence in men with diabetes ranges from 35–90% versus 26% in general population. Variation in prevalence is mainly due to differences on definitions used, differences in the populations studied, study design, classification, and the diagnostic tools- especially for studies conducted in the past. Introduction of validated questionnaire (the IIEF) minimized this variation [2].
Many male sexual function profiles and ED questionnaires have been developed. The International Index of Erectile Function Questionnaire (IIEF) is the most reliable measure of ED [3, 16]. It has 15 questions and the total score is obtained by the sum of the individual scores of each question. It addresses and quantifies five domains, namely: erection function, orgasmic (ejaculation) function, sexual desire (libido), intercourse satisfaction (ability to sustain intercourse), and overall satisfaction/premature ejaculation.
The current study aimed at determining the prevalence of erectile dysfunction and associated factors among diabetic men attending the diabetic clinic at Muhimbili National Hospital (MNH), Dar-es-Salaam.
Specifically the study wanted to answer the following questions: to determine the prevalence of erectile dysfunction among male diabetic patients attending diabetic clinic at MNH, Dar-es-Salaam, to determine the severity of erectile dysfunction among male diabetic patients attending diabetic clinic at MNH, Dar-es-Salaam, to determine factors influencing erectile dysfunction among male diabetic patients attending diabetic clinic at MNH, Dar-es-Salaam, and to describe the association between erectile dysfunction and other sexual function domains among male diabetic patients attending diabetic clinic at MNH, Dar es Salaam.
Methods
This was a cross section hospital based prospective study, which was conducted at MNH for the period of 8 month from May to December 2011. The study population included all adult (≥ 18 years) diabetic men attending diabetic clinic at MNH with duration of diabetic ≥ 1 year. We excluded very sick patients who were defined as: Patients with unstable vital signs/mental status e.g. in diabetic ketoacidosis or hyperosmolar hyperglycemic state, confused, or in septicemia as in infected diabetic foot.
During recruitment, the principal investigator (PI) filled in a standardized structured questionnaire for each patient included in the study. The questionnaire included socio-demographic and clinical aspects data, to assess the different sexual domains the International Index of Erectile Function (IIEF) Questionnaire was used. The IIEF was translated into Kiswahili language and the author asked all the 15 questions.
Measures included Socio-demographic data and Medical history regarding duration of diabetes, type of diabetes, medications taken for diabetes; presence of co morbid conditions was obtained. Moreover, anthropometric measurements were recorded and blood for laboratory tests was taken.
Height (in meters) was taken using a commercially available stadiometer (AXIOM, AX - 120) and weight (in kilograms) was measured using a standard weighing. The body mass index (BMI) was derived by dividing the weight (kg) by the square of the height (m) and classification of obesity was done according to World Health Organization [17] criteria.
Blood pressure measurement using standard well-calibrated mercury sphygmomanometer based was taken. Hypertension was defined as SBP ≥ 140mmHg and/or DBP ≥ 90mmHg [18] or known hypertensive on treatment.
The 10g Semmes Weinstein monofilament (NovoMi× 30) was used to screen diabetic patients for peripheral neuropathy. Patients was asked to close their eyes while the monofilament is pressed perpendicular 9 areas of the plantar surface and one on dorsal surface of the feet until it buckles. The patients were asked to say ‘Yes’ each time they feels the filament. Failure to feel the filament at 4 of 10 sites is 97% sensitive and 83% specific for identifying loss of protective sensation [19].
Ankle Brachial Index (ABI), the ratio of SBP of the brachial artery to that of pedal artery was measured to assess lower limb blood flow to rule out peripheral vascular disease. A bedside, Hand-held Doppler ultrasound machine (MEDA SONICS), 8 MHz probe was used, Ultrasound transducer gel, phygmomanometer and cuff, and a Calculator. Scores were: < 0.9 abnormal, 0.9 to 1.0 normal, and > 1.3 non-compressible.
Fasting blood samples for total serum cholesterol, high-density lipoproteins (good cholesterol), low-density lipoprotein (bad cholesterol), serum triglycerides and blood glucose, estimation was taken. Five milliliters of venous blood was taken from the antecubital fossa and placed in empty sterile tubes. The samples were taken to the laboratory for analysis within a day. Quality assurance prior to carrying out sample processing and analysis was adhered to. Blood samples for Glycosylated hemoglobin was collected and analyzed at the diabetic clinic, using DCA 2000+ (Bayer).
The IIEF questionnaire has 15 questions and the total score is obtained by the sum of the individual scores of each question. It addresses and quantifies five domains: erection function, orgasmic (ejaculation) function, sexual desire (libido), intercourse satisfaction (ability to sustain intercourse), and overall satisfaction/premature ejaculation domains. It classifies individual sexual function domains into mild, moderate or severe form depending on scores.
Questionnaires were checked every day after interviews for consistence filling. Then data were entered into Statistical Package for Social Studies (SPSS) version 15.0 software (SPSS, Chicago, IL, USA) which was used in the analysis of the data. Some smaller categories were aggregated into larger categories to make a statistical meaning. First descriptive statistics were calculated. Then bivariate analysis was done using Chi-square (X2) for categorical variables and t-test for dichotomous and continuous variables. Multivariate Logistic regression was run to identify ad quantify the adjusted odds predictors of ED. These predictors were adjusted for age, education, gender, and some other demographic variables. A 2-tailed p-value of 0.05 was taken as statistically significant.
This study was ethically approved by the Muhimbili University College of Health and Allied sciences (MUHAS) Research Ethics Committee after meeting the required ethical standards.
The principal investigator fully explained to every prospective participant the purpose of the research and was requested to participate freely. A consent form containing details of the study regarding main purpose, role of participants, and benefits associated with participating in the study (if any) was given to each prospective participant. Those who agreed to participate in the study gave a verbal consent as well as signing a written consent form written both in English and Swahili language. Swahili language is a lingua franca in Eastern Africa. Patients who did not agree to participate in the study were not denied any services and were treated accordingly.
Patients who were found to have erectile dysfunction were counseled (those who came as a couple were counseled as thus after obtaining consent), about the available treatment options and their advantages/side effects. Prescriptions were written for those who agreed to be put on treatments while maintaining confidentiality. Patients with evidence of peripheral vascular disease were planned to regularly attend the clinic every 2months for check-up. Those with hyperlipidemia were prescribed lipid-lowering drugs and the patients newly diagnosed with hypertension were managed accordingly.
Results
Over a period of 8 months, May to December 2011, a total of 503 male diabetic patients were attended at MNH diabetic clinic where by 312 (62%) were eligible for the current study. The mean age was 51.33 (SD=15.03). Most of them were aged 45-60 years and had attained primary level of education. The details of socio-demographic are as shown on Table 1.
Table 1.
Socio-demographic characteristics of male diabetic patients attending Diabetic clinic at MNH (N=312)
| Characteristics | Frequency (N) | % |
|---|---|---|
| Age group (years) | ||
| < 30 | 35 | 11.2 |
| 30 – 44 | 55 | 17.6 |
| 45 - 59 | 113 | 36.2 |
| 60+ | 109 | 34.9 |
| Marital status | ||
| Married | 256 | 82.1 |
| Single | 36 | 11.5 |
| Divorced | 4 | 1.3 |
| Cohabiting | 7 | 2.2 |
| Widowed | 9 | 2.9 |
| Employment | ||
| Peasant | 71 | 22.8 |
| Government | 38 | 12.2 |
| Private sector | 57 | 18.3 |
| Self-employee | 114 | 36.5 |
| Others | 32 | 10.2 |
| Level of education | ||
| Informal | 40 | 12.8 |
| Primary | 152 | 48.7 |
| Secondary | 82 | 26.3 |
| Post-secondary | 38 | 12.2 |
About four-fifth of the patients (n=251) had type 2 Diabetes Mellitus (T2DM) and one fifth (n=61) had Type 1 Diabetes Mellitus (T1DM). The mean diabetic duration of this study population was 8.99 (SD = 7.62) years with a minimum of 1year and maximum of 37years.
The prevalence of erectile dysfunction was found to be 55.1% (n=171) with the highest proportion having severe dysfunction as shown in Figure 1. As the age increases the prevalence of and severity of ED increases significantly as shown in Figure 2 below (p<0.001).
Figure 1.
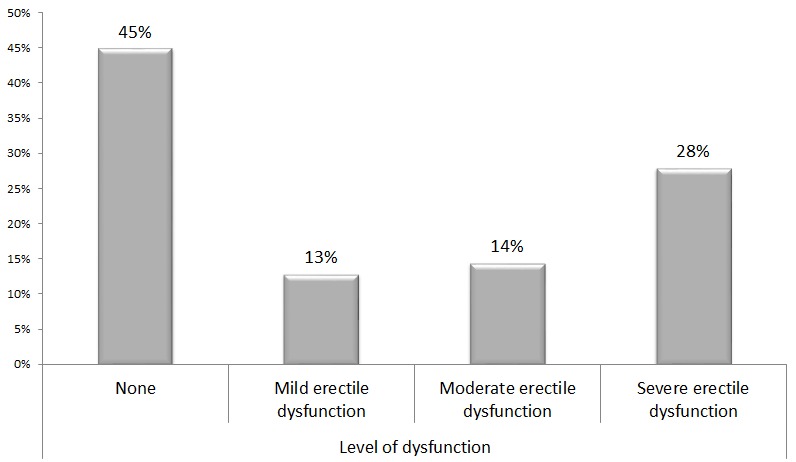
Prevalence and Severity of erectile dysfunction among male patients attending Diabetic Clinic at MNH (N=312)
Figure 2.
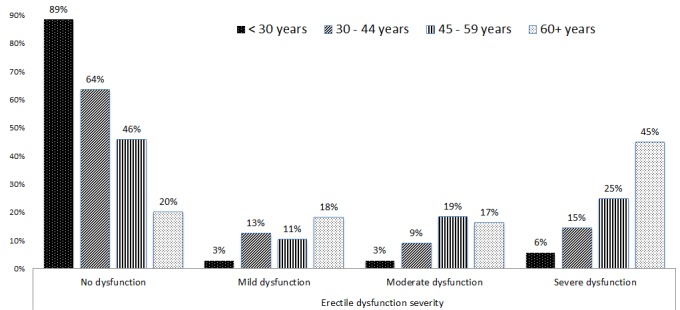
Severity of erectile dysfunction by age groups among male Diabetic patients attending Diabetic clinic at MNH in 2012 (N=312)
When the ED was dichotomized into “yes” and “no” options and analyzed at bivariate level there was a significant association with an increased in age, longer duration of DM (both types), and T2DM. Also ED was associated with histories of hypertension, alcohol intake and stroke as shown in Table 2. Also bivariate analysis was done to relate the prevalence of ED and clinical parameters where by only men who could not feel on monofilament test and those with abnormal ankle brachial index score were more likely to have the disorder as shown on Table 3.
Table 2.
Bivariate analysis of socio-demographic and clinical variables associated with erectile dysfunction among male diabetic patients attending diabetic clinic at MNH
| Variable | Number | Prevalence (%) of ED | p-value a |
|---|---|---|---|
| Age group (yrs) | |||
| < 30 | 35 | 6 (17.1) | <0.001* |
| 30– 44 | 55 | 23 (41.8) | |
| 45 – 59 | 113 | 58 (51.3) | |
| 60+ | 109 | 85 (78.0) | |
| Education level | |||
| None | 40 | 28 (70) | 0.16 |
| Primary | 152 | 82 (53.9) | |
| Secondary | 82 | 40 (48.8) | |
| Post-secondary | 38 | 22 (57.9) | |
| Current employment | |||
| Peasant | 71 | 51 (71.8) | 0.03* |
| Government | 38 | 19 (50.0) | |
| Private | 57 | 28 (49.1) | |
| Self-employment | 114 | 58 (50.9) | |
| Others | 32 | 16 (50.0) | |
| Duration DM(years) | |||
| < 10 | 180 | 83 (46.1) | 0.001* |
| 10 – 19 | 106 | 70 (66.0) | |
| > 20 | 26 | 19 (73.1) | |
| Type of diabetes | |||
| T1DM | 61 | 14 (23.0) | <0.001* |
| T2DM | 251 | 158 (62.9) | |
| H/o smoking | |||
| Never smoked | 252 | 131 (52) | 0.02* |
| Ever smoked | 60 | 41 (68.3) | |
| H/o alcohol | |||
| Never drunk | 182 | 92 (50.5) | 0.05* |
| Ever drunk | 130 | 80 (61.5) | |
| Hypertensive** | |||
| No | 154 | 68 (44.2) | <0.001* |
| Yes | 158 | 104 (65.8) | |
| H/o stroke | |||
| No | 291 | 155 (53.3) | 0.01* |
| Yes | 21 | 17 (81.0) | |
| H/o p/neuropathy | |||
| No | 146 | 59 (40.4) | <0.001* |
| Yes | 166 | 113 (68.1) | |
| TOTAL | 312 | 117 (55.1) |
X2 test
p<0.05
20 patients were diagnosed with ↑BP during the study
Table 3.
Bivariate analysis of clinical parameters associated with erectile dysfunction among male diabetic patients attending diabetic clinic at MNH (N=312)
| Variable | Number | Prevalence (%) of ED | p-value a |
|---|---|---|---|
| Monofilament test | |||
| Could feel | 217 | 95 (43.8) | <0.001* |
| Could not feel | 95 | 77 (81.1) | |
| LDL-c (mmol/l) | |||
| Normal (≥3.34) | 210 | 118 (56.2) | 0.59 |
| Abnormal (<3.34) | 102 | 54 (52.9) | |
| Triglyc (mmol/l) | |||
| Normal (≤ 2.3) | 266 | 149 (56.0) | 0.45 |
| Abnormal (>2.3) | 46 | 23 (50.0) | |
| Total chol (mmol/l) | |||
| Normal (≤ 5.2) | 209 | 113 (54.1) | 0.59 |
| Abnormal | 103 | 59 (57.3) | |
| Fasting b/sugar | |||
| Normal (≤ 7) | 103 | 55 (53.4) | 0.66 |
| Abnormal (>7) | 209 | 117 (56.0) | |
| HbA1c (%) b | |||
| Normal (≤ 7%) | 32 | 20 (62.5) | 0.49 |
| Abnormal (7%) | 113 | 63 (55.8) | |
| Ankle Brachial Index score | |||
| Normal | 264 | 127 (48.1) | <0.001* |
| Abnormal | 48 | 45 (93.8) | |
| Body mass index c | |||
| <18.5 | 20 | 9 (45) | 0.27 |
| 18.5 – 24.9 | 152 | 77 (50.3) | |
| 25 – 29.9 | 90 | 56 (62.2) | |
| >30 | 38 | 20 (52.6) |
Chi square test
p<0.05
HbA1c was done among 145 patients
BMI of 12 individuals could not be determined because these patients each have one limb amputated and were not stable to stand for weight and height determination.
Variables that were significant at bivariate analysis were adjusted for potential confounders such as socio-demographics (age groups, education background), duration of diabetes, history of stroke and alcohol using multivariate logistic regression. Also identification and quantification potential predictors of ED were conducted. Table 4 shows that as the age increase the odds of having ED increased significantly e.g. age group 60+ years had almost 15 times higher odds compared to those Table 4.
Table 4.
Multivariate logistic regression analysis of factors associated with erectile dysfunction among male diabetic patients attending diabetic clinic at MNH (N=312)
| Variable * | aOR | 95% CI | p-value |
|---|---|---|---|
| Age group (years) | |||
| < 30 | 1 | ||
| 30– 44 | 3.992 | 1.382 – 11.530 | 0.011 |
| 45 – 59 | 7.023 | 2.589 – 19.051 | 0.001 |
| 60+ | 15.730 | 5.567 – 44.447 | 0.001 |
| Duration of diabetes (years) | 1.038 | 0.999 – 1.078 | 0.056 |
| Type of diabetes | |||
| T1DM | 1 | ||
| T2DM | 2.695 | 0.947 – 7.666 | 0.063 |
| H/o smoking | |||
| Never smoked | 1 | ||
| Ever smoked | 1.421 | 0.722 – 2.799 | 0.309 |
| H/o p/neuropathy | |||
| No | 1 | ||
| Yes | 2.583 | 1.525 – 4.375 | 0.001 |
| Monofilament test | |||
| Could feel | 1 | ||
| Couldn't feel | 4.989 | 2.600 – 9.575 | 0.001 |
| ABI score | |||
| Normal | 1 | ||
| Abnormal | 11.316 | 3.247 – 39.443 | 0.001 |
The reference category is first group in each variable
Discussion
This hospital-based study confirms that the prevalence of ED is high among DM patients. It further confirms that duration of DM and age were independently correlated with the ED and its severity. As expected the history of peripheral neuropathy and abnormal ABI score were highly associated with ED. Erectile dysfunction was related to other sexual domains. Surprisingly type of diabetes, lifestyle histories and history of other conditions such as hypertension and stroke were related to ED at bivariate analyses but not on multivariate suggesting that they could have been confounded by other demographic variables.
The high prevalence of ED among DM patients is in line with several studies, which have been conducted in Italy, South America and other parts of the world. The prevalence of ED globally was found to be as low as 35% in UK, McCulloch et al [14] and in Italy, Fedele et al [15] to as high as 90% in Japan, Sasaki et al [20]. This indicates that this study incidence of 55% is with the global range as well. The prevalence is relatively lower than that of Kenyatta National Hospital which was found to be 74% [21]. The reason for the higher prevalence could be due to different in composition of study population and the methodology used.
However, the prevalence observed from current study is similar from that of the study done by Balde, NM et al [22] in Conakry (Guinea), whereby erectile dysfunction was (48%). The explanation for these large differences in the reported prevalence of ED among diabetic men could be due to differences in methodology (definitions used and scales) and population characteristics. Also inadequate linguistic validation and cultural adaptation of the IIEF may have had an influence on the prevalence reported in studies conducted in different ethnic communities.
Some studies conducted in high income countries [14, 15] reported low prevalence as compared to those done in developing world due to the fact that in developed world DM may be early detected and blood sugar may be well controlled and therefore the chronic complications are prevented i.e. differences in diabetic care or educated are more likely to deny ED.
With respect to age and peripheral neuropathy, this study confirms discoveries done by McCulloch [14] these parameters were highly associated with ED despite different analytical methods.
In contrast to the findings by Fedele et al [15] which showed that ED was more in T2DM than T1DM and in those with poor glycemic control, in this study these variables were not significant. The reason may be due to different geographical patterns and/or different statistical methods used. This entails that more studies with large sample may be needed to ascertain these factors in this setting. Also the findings in this study were in odds with those revealed by Khatib et al [23] which showed that apart from age other independent risk factors of ED were hypertension and poor glycemic control.
Conclusion
This study showed that the prevalence of erectile dysfunction is high among DM patients. The study further showed that old age, peripheral neuropathy and evidence of peripheral arterial disease are main factors strongly associated with ED. These findings reinforce the need to screen for ED in diabetic patients as it is done for other chronic complications of diabetes in routine clinical practices for early detection, treatment and possibly prevention. The screening for presence or absence of ED can be best done by the use of IIEF questionnaire. Interventions aimed at prevention of DM especially type 2; early diagnosis of DM and detection of its complications e.g ED, and adherence to treatment to prevent these complication should be implemented. ED is a neglected medical problem that necessitates screening of all DM patients at each visit to aid the delivery appropriate treatment.
Acknowledgments
We acknowledge the Department of Internal Medicine, MUHAS for their enormous support. I'm also grateful to my employer, Muhimbili Orthopaedic Institute for granting me a study leave and financial support to conduct this study. Above all, I highly acknowledge all my patients who participated in this study.
Competing interests
The authors declare that they have no any competing interests.
Authors’ contributions
RKM: first author of this work, involved in all steps including; proposal development, data collection, data analysis, manuscript writing and submitting to the publishing journal. JL: contributed to the study design, global and direct supervision of data collection, report and manuscript writing. AM: contributed to the study design, direct supervision of data collection, manuscript discussion writing. BAK: was involved in data manipulation, statistical analysis and results writing manuscript preparation.
References
- 1.NIH Consensus Conference. Impotence: NIH Consensus Development Panel on Impotence. JAMA. 1993;270(1):83–90. [PubMed] [Google Scholar]
- 2.Neelima V Chu, Edelman SV. Diabetes and Erectile Dysfunction. Clinical diabetes. 2001;19(1):45–47. [Google Scholar]
- 3.Kubin M, Wagner G, Fugl-Meyer AR. Epidemiology of erectile dysfunction. Int J Impot Res. 2003;15(1):63–71. doi: 10.1038/sj.ijir.3900949. [DOI] [PubMed] [Google Scholar]
- 4.Shiri R, Hakama M, Häkkinen J, Tammela TLJ, et al. Relationship between smoking and erectile dysfunction. Int J Impot Res. 2005;17(2):164–9. doi: 10.1038/sj.ijir.3901280. [DOI] [PubMed] [Google Scholar]
- 5.Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychological correlates: results of the Massachusetts Male Ageing Study. J urol. 1994;151(1):54–61. doi: 10.1016/s0022-5347(17)34871-1. [DOI] [PubMed] [Google Scholar]
- 6.Siu SC, Lo SK, Wong KW, Ip KM, Wong YS. Prevalence of and risk factors for erectile dysfunction in Hong Kong diabetic patients. Diabet Med. 2001;18(9):732–738. doi: 10.1046/j.0742-3071.2001.00557.x. [DOI] [PubMed] [Google Scholar]
- 7.Deutsch S, Sherman L. Previously unrecognized diabetes mellitus in sexually impotent men. JAMA. 1980;244(21):2430–32. [PubMed] [Google Scholar]
- 8.Braun M, Wassmer G, Klotz T, Reifennah B, Mathers M, Engelman U. Epidemiol of ED: results of the Cologne male survey. Int J of Impot Res. 2000;12(6):305–11. doi: 10.1038/sj.ijir.3900622. [DOI] [PubMed] [Google Scholar]
- 9.Marumo K, Nakashima J, Murai M. Age-related prevalence of erectile dysfunction in Japan: assessment by the International Index of Erectile Function. Int J Urol. 2001;8(2):53–5. doi: 10.1046/j.1442-2042.2001.00258.x. [DOI] [PubMed] [Google Scholar]
- 10.Nicolosi A, Moreira ED, Jr, Shirai M, Bin Mohd Tambi MI, Glasser DB. Epidemiology of erectile dysfunction in four countries: Cross-national study of the prevalence and correlates of erectile dysfunction. Urology. 2003;61(1):201–6. doi: 10.1016/s0090-4295(02)02102-7. [DOI] [PubMed] [Google Scholar]
- 11.Mueleman EJ. Prevalence of erectile dysfunction: need for treatment? Int J Impot Res. 2002;14(Suppl 1):S22–28. doi: 10.1038/sj.ijir.3900793. [DOI] [PubMed] [Google Scholar]
- 12.Cho NH, Ahn CW, Park JY, Ahn TY, et al. Prevalence of erectile dysfunction in Korean men with Type 2 diabetes mellitus. Diabet Med. 2006;23(2):198–203. doi: 10.1111/j.1464-5491.2005.01789.x. [DOI] [PubMed] [Google Scholar]
- 13.Malavige LS, Jayaratne SD, Kathriarachchi ST, Sivayogan S, et al. Erectile dysfunction among men with diabetes is strongly associated with premature ejaculation and reduced libido. J Sex Med. 2008;5(9):2125–34. doi: 10.1111/j.1743-6109.2008.00907.x. [DOI] [PubMed] [Google Scholar]
- 14.McCulloch DK, Campbell IW, Wu FC, Prescott RJ, Clarke BF. The prevalence of diabetic impotence. Diabetologia. 1980;18(4):279–83. doi: 10.1007/BF00251005. [DOI] [PubMed] [Google Scholar]
- 15.Fedele D, Coscelli C, Santeusanio F, Bortolotti A, et al. Erectile dysfunction in diabetic subjects in Italy: Gruppo Italiano Studio Deficit Erettile nei Diabetici. Diabetes Care. 1998;21(11):1973–7. doi: 10.2337/diacare.21.11.1973. [DOI] [PubMed] [Google Scholar]
- 16.Ryder AB, Robert EJ. New Treatment Options for Erectile Dysfunction in patients with Diabetes Mellitus. Drugs. 2004;64(23):2667–2688. doi: 10.2165/00003495-200464230-00004. [DOI] [PubMed] [Google Scholar]
- 17.WHO. Geneva: WHO; 1995. Physical status: the use and interpretation of anthropometry: Report of a WHO Expert Committee: WHO Technical Report. [PubMed] [Google Scholar]
- 18.WHO. J Hypertens. Geneva: WHO; 1999. International Society of Hypertension guidelines for the management of hypertension. [PubMed] [Google Scholar]
- 19.Amstrong DG, Lavery LA. Diabetic Foot Ulcers: Prevention, Diagnosis, and Classification. Am Fam Physician. 1998;57(6):1325–1332. [PubMed] [Google Scholar]
- 20.Sasaki H, Yamasaki H, Ogawa K, Nanjo K, Iwamoto Y, et al. Prevalence and risk factors for erectile dysfunction in Japanese diabetics. Diabetes Res Clin. 2005;70(1):81–9. doi: 10.1016/j.diabres.2005.02.018. [DOI] [PubMed] [Google Scholar]
- 21.Ngalyuka PK, Amayo EO, Otieno CF, Kayima JK. University of Nairobi; 2008. The prevalence of erectile dysfunction and the associated risk factors in Kenyan men with type II diabetes at the Kenyatta national outpatient clinic: Master of Medicine dissertation. http://erepository.uonbi.ac.ke/handle/11295/25512. Accessed 19 March 2014. [Google Scholar]
- 22.Balde NM, Diallo AB, Balde MC, Kake A, Diallo M, Maugendre D. Erectile dysfunction and diabetes in Conakry (Guinea): frequency and clinical characteristics from 187 diabetic patients. Ann Endocrinol (Paris) 2006;67(4):338–42. doi: 10.1016/s0003-4266(06)72608-7. [DOI] [PubMed] [Google Scholar]
- 23.Khatib FA, Jarrah NS, Shegem NS, Bateiha AM, et al. Sexual dysfunction among Jordanian men with diabetes. Saudi Med J. 2006;27(3):351–6. [PubMed] [Google Scholar]