

Abstract
BACKGROUND
Importance of androgen receptor (AR) as an independent prognostic marker in Pakistani women with breast cancer (BCa) remains unexplored. Our aim was to identify the expression and potential prognostic value of AR, its upstream regulator (pAkt) and target gene (pPTEN) in invasive BCa.
METHODS
This study used a cohort of 200 Pakistani women with invasive BCa diagnosed during 2002-2011. Expression of AR, pAkt and pPTEN was determined on formalin fixed paraffin embedded tissue sections by immunohistochemistry. The association of AR, pAkt and pPTEN with clinicopathological parameters was determined. Survival analyses were undertaken on patients with ≥ 5 years of follow-up (n = 82).
RESULTS
Expression of AR, pAkt and pPTEN was observed in 47.5%, 81.3% and 50.6% of patients, respectively. AR-expressing tumors were low or intermediate in grade (P < .001) and expressed ER (P = .002) and PR (P = .001). Patients with AR+ tumors had significantly higher OS (Mean OS = 10.2 ± 0.465 years) compared to patients with AR− tumors (Mean OS = 5.8 ± 0.348 years) (P = .047). Furthermore, AR-positivity was associated with improved OS in patients receiving endocrine therapy (P = .020). Patients with AR+ /pAkt+ /pPTEN− tumors, had increased OS (Mean OS = 7.1 ± 0.535 years) compared to patients with AR−/pAkt+/pPTEN− tumors (Mean OS = 5.1 ± 0.738 years).
CONCLUSION
AR-expressing tumors are frequently characterized by low or intermediate grade tumors, expressing ER and PR. In addition, expression of AR, pAkt and pPTEN, could be considered in prognostication of patients with invasive BCa.
Introduction
Breast cancer (BCa) is the most common malignancy among women around the globe, and it is recognized to be the second most common cause of death in women [1]. Its rate is rising rapidly in Asian women and the developing world. According to the Surveillance, Epidemiology, and End Results database, Asian Indian/Pakistani women residing in the United States seem to have a higher frequency of BCa particularly at a younger age (< 40 years) compared to Caucasians [2]. The data from South Karachi, a pragmatic representative of the population of Pakistan, revealed that BCa accounted for approximately one third of cancers in women [3].
Hormone receptors such as estrogen (ERs) and progesterone receptors (PRs) play a seminal role in determining the treatment strategy and prognosis of patients with BCa. In addition, human epidermal growth factor receptor type 2 (HER2) has been found to be overexpressed in a subset of invasive BCa and is associated with poor prognosis [4], [5]. According to Surveillance, Epidemiology and End Results database, Asian Indian/Pakistani women residing in the United States had more ER/PR-negative BCa (30.6%) compared to Caucasians (21.8%) [2]. These data are similar to studies undertaken on samples of BCa from women residing in Pakistan that showed that 60% to 65% of the tumors expressed ER/PR [6], [7]. Furthermore, frequency of HER2 expression has also found to be higher in Pakistani women with BCa (30%-39%) [6], [8], [9] in contrast to Caucasians (25%-30%) [4], [5].
Only a limited number of studies have evaluated the role of the androgen receptor (AR), phosphorylated Akt (pAkt), and phosphorylated phosphatase and tensin homolog (pPTEN) as potential predictive or prognostic markers compared to the large number of studies on ER, PR, and HER2.
AR is a ligand-dependent transcription factor; its expression on BCa is known to be linked with improved survival [10], [11], [12]. Hu et al. assessed AR status in a large (n = 1467) cohort of patients with BCa; they found 91% and 86% 5-year survival in patients with AR-positive and AR-negative tumors, respectively [11], whereas other studies have not found a similar association with survival [13], [14]. AR expression has been observed in approximately 40% to 80% of BCas [11], [15], [16], [17], [18], [19]. Although a significant number of patients with BCa express AR, the underlying molecular mechanisms of AR signaling pathway in BCa biology have not been intensely studied, and the role of AR on survival in patients with BCa needs further delineation.
Protein kinase B (more commonly referred as Akt) is a serine/threonine kinase, which plays a role in BCa growth by promoting cell survival and inhibiting cell death [20], [21] and is being considered as a potential target for BCa therapy [22], [23], whereas PTEN, a well-recognized tumor suppressor gene, negatively regulates Akt and has been shown to inhibit BCa growth [24], [25]. Nagata and colleagues reported loss of PTEN in 50% of patients with BCa [26]. AR has been shown to increase PTEN expression by activating its promoter that in turn lowers Akt activity and decreases cellular proliferation in BCa [27]. Wang et al. also reported that AR increases PTEN expression and inhibits Akt phosphorylation in BCa cells [28]. PTEN is a positive modulator, whereas Akt is a negative modulator of AR transcriptional activity. The cross talk of AR signaling with Akt and PTEN that may have clinical significance in the development of BCa has not been well studied, though the expression of Akt and PTEN in BCa tissue has been reported [29], [30], [31].
To our knowledge, to date, no studies have been undertaken examining the expression of AR, active form of Akt (pAkt), and stable form of PTEN (pPTEN) on BCa in a cohort of Pakistani women. In this study, our aim was to determine the immunohistochemical expression of AR, pAkt, and pPTEN in Pakistani women with invasive BCa and their role as potential prognostic markers. We also examined the significance of AR expression on patient's survival after stratifying by ER, pAkt, and pPTEN status and endocrine treatment.
Materials and Methods
Patients and Setting
A total of 1103 patients were diagnosed with invasive BCa and treated at the section of breast diseases, Aga Khan University Hospital (Karachi, Pakistan), during 2002 to 2011. From a total of 1103 cases, 200 were selected for this study on the basis of the following criteria: 1) availability of formalin-fixed paraffin-embedded (FFPE) tissue blocks, 2) sufficient representative area of primary tumor in FFPE blocks, and 3) complete follow-up data. Demographical data, details of treatment regimen, clinicopathologic parameters including tumor size and type, ER/PR/HER2 status, grade, and lymph node status, and clinical follow-up were obtained by reviewing medical records. To minimize the selection bias, we compared the clinicopathologic characteristic between patients who were selected for this study (n = 200) with those who were not selected (n = 903), and no statistically significant difference was found between the two groups. All patients had previously consented for use of their tissues and clinicopathologic data for research.
Five-micron serial sections were cut from FFPE BCa tissue blocks. At least one section was stained with hematoxylin and eosin, assessed by a pathologist, and compared to original report. The study was approved by the Ethical Review Committee of the Aga Khan University (2390-RO-ERC-12).
Survival analysis was performed on a subgroup of patients with BCa who had follow-up of at least 5 years or more (n = 82). Patients diagnosed during 2002 to 2008 and followed up until December 2013 or death were included for survival analysis. Overall survival (OS) was calculated from the date of diagnosis to the date of last follow-up or death due to any cause.
Immunohistochemical Expression of AR, pAkt, and pPTEN
Immunohistochemistry was performed on FFPE sections to assess the expression of AR, pAkt, and pPTEN as described previously with some modifications [32], [33], [34]. Dako REAL EnVision Detection System, Peroxidase/DAB +, Rb/Mo (Dako, Glostrup, Denmark) was used for immunohistochemical staining. Briefly, 5-μm serial sections were cut from FFPE tissue onto Superfrost slides (Thermo Scientific, Braunschweig, Germany). Sections were deparaffinized in xylene (BDH, Poole, UK) and rehydrated in a graded series of ethanol (Merck, Darmstadt, Germany). Heat-induced antigen retrieval was performed in 10 mM citrate buffer (pH 6.0) for AR (1 hour), pAkt, and pPTEN (30 minutes) in a boiling water bath (Grant Instruments Ltd., Cambridge, UK). Endogenous peroxidase activity was blocked by immersing slides in 0.3% vol/vol H2O2 at room temperature (RT; 25°C) for 10 minutes. Next, anti-human AR antibody (mouse monoclonal IgG, clone AR441; Dako, diluted 1:50) was applied for 4 hours at RT, and anti-human Ser473 pAkt1/2/3 (rabbit polyclonal IgG; Santa Cruz Biotechnology, diluted 1:50) and Ser380/Thr382/383 pPTEN (rabbit polyclonal IgG; Santa Cruz Biotechnology (Santa Cruz, CA), diluted 1:50) were applied for overnight at 4°C onto serial tissue sections from each case. After three washes for 5 minutes each in phosphate-buffered saline (pH7.4) (Gibco, Carlsbad, CA), HRP-labeled secondary antibody was applied for 1 hour at RT. After washing, substrate was added, and DAB was used for visualization. Hematoxylin (BDH) was used for counterstaining, and images were obtained using microscope (Olympus BX41, Tokyo, Japan, DP70 camera). Negative (primary antibody replaced by phosphate buffer saline) and positive (a known BCa tissue section positive for AR, pAkt, pPTEN) controls were included with each run. Our experimental methodology including antigen retrieval, choice of the antibody, and detection system was in concordance with previously reported studies.
Scoring
Stained sections were scored by a pathologist who was masked for patient’s clinicopathologic parameters and outcomes. Slides were scored using Allred guidelines [35]. In brief, entire slide of each sample was evaluated using Olympus BX41 microscope at × 100 and × 200 magnifications. First, proportion of positively stained tumor cells (0, none; 1, < 1/100; 2, 1/100 to 1/10; 3, 1/10 to 1/3; 4, 1/3 to 2/3; and 5, > 2/3) was estimated. Next, an intensity score that represented the average intensity of positive tumor cells (1, weak; 2, intermediate; and 3, strong) was estimated. The proportion and intensity scores were then added to obtain a total score, which ranged from 0 to 8. Nuclear staining for AR and cytoplasmic staining for pAkt and pPTEN with a total score of ≥ 3 were considered positive.
Statistical Analysis
Frequencies of different markers including AR, pAkt, and pPTEN with 95% confidence intervals (CIs) were generated for the expression of these markers. Descriptive statistics was determined for continuous (mean ± SE) and categorical (percentages) variables. The associations of AR, pAkt, and pPTEN expression with demographical data, details of treatment regimen, and clinicopathologic parameters like tumor type, grade, size, status of lymph node, ER, PR, and HER2 were assessed by χ2 test if appropriate; otherwise, Fisher exact test was applied. OS were computed using Kaplan-Meier method. Means and SE of OS time were reported for clinicopathologic parameters. The association of different survival times by these markers was obtained using log-rank test. A P value < .05 (two sided) was considered statistically significant. SPSS (version 18.0, IBM Company, Chicago, IL) was used for all statistical analysis.
Results
Patients and Tumor Characteristics
Mean (± SE) age of patients at diagnosis was 54.8 (± 10.5) years, of which 39% were younger than 50 years. Most of the tumors (95.5%) were ductal, followed by lobular (3%) and mucinous carcinomas (1.5%). More than half of the tumors (56.5%) were of grade II, 54.5% of tumors were 2 to 5 cm in size, and 53.0% of the primary tumors had no lymph node involvement at diagnosis. Among 121 cases of ER-positive tumor, 115 (95%) patients received endocrine therapy. Majority of them (89.5%) received tamoxifen as first option, whereas the remainder (10.5%) received either Femara (Novartis, Basel, Switzerland) or Arimidex (ICI Pakistan Ltd., Karachi, Pakistan).
Expression of AR, pAkt, and pPTEN
Expression of AR, pAkt, and pPTEN was observed in 47.5% (95% CI = 40.6%-54.4%), 81.3% (95% CI = 75.4%-87.2%), and 50.6% (95% CI = 42.9%-58.3%) of patients, respectively.
The percentage of tumors that expressed AR, pAkt, pPTEN, ER, PR, and HER2 are shown in Table 1. AR expression was predominantly found to be localized in the nuclei, whereas pAkt and pPTEN were predominantly found to be localized in the cytoplasm. Representative photomicrographs of AR, pAkt, and pPTEN expression in tissue sections are shown in Figure 1.
Table 1.
Relative Percentage of Expression of AR, pAkt, pPTEN, ER, PR, and HER2 from Different Studies in Invasive BCa.
| Marker | Current Study (%) | Other Studies in Pakistani Population (%) | Caucasians (%) |
|---|---|---|---|
| AR | 47.5 | None | 70-80 [11], [36] |
| pAkt⁎ | 81.3 | None | 76-81 [30], [34] |
| pPTEN⁎⁎ | 50.6 | None | 49-52 [31], [37] |
| ER/PR | 56 | 60-65 [6], [7] | 55-70 [38], [39] |
| HER2⁎⁎⁎ | 24 | 30-39 [6], [8], [9] | 25-30 [4], [5] |
AR, androgen receptor; pAkt, phosphorylated Akt; pPTEN, phosphorylated phosphatase and tensin homolog; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor type 2.
n = 166.
n = 162.
n = 192.
Figure 1.

Immunohistochemical expression of AR, pAkt, and pPTEN in invasive breast carcinoma. (A) Heterogeneous nuclear AR, (B) cytoplasmic pAkt, and (C) pPTEN protein expression in a tumor. Images are at × 200, and insights are at × 400 magnification.
Association of AR with Clinicopathologic Parameters, pAkt, and pPTEN
Expression of AR was significantly associated with increasing age > 50 years (P = .040), low or intermediate grade (I and II) tumors (P = .001), expression of ER (P = .002), PR (P = .001), and therapeutic modalities including endocrine (P = .004) and chemotherapy (P = .015). There were no significant differences observed between AR expression and tumor size, lymph node involvement, HER2 status, tumor type, radiation therapy, and expression of pAkt and pPTEN (Table 2).
Table 2.
Association of AR Expression with Demographical, Clinicopathologic Parameters, pAkt, and pPTEN.
| Factor | AR-Positive n = 95 (47.5%) | AR-Negative n = 105 (52.5%) | P Value |
|---|---|---|---|
| Age at diagnosis (years) | .040⁎ | ||
| ≤ 50 | 30 (38.5) | 48 (61.5) | |
| > 50 | 65 (53.3) | 57 (46.7) | |
| Tumor size (n = 189)⁎⁎ | .400 | ||
| T1 | 20 (46.5) | 23 (53.5) | |
| T2 | 56 (51.4) | 53 (48.6) | |
| T3 | 10 (34.5) | 19 (65.5) | |
| T4 | 3 (37.5) | 5 (62.5) | |
| Node involvement (n = 192) | .287 | ||
| N0 | 45 (42.5) | 61 (57.5) | |
| N1 | 27 (55.1) | 22 (44.9) | |
| N2 | 8 (42.1) | 11 (57.9) | |
| N3 | 11 (61.1) | 7 (38.9) | |
| Grade (n = 197) | < .001⁎ | ||
| I and II | 71 (58.2) | 51 (41.8) | |
| III | 23 (30.7) | 52 (69.3) | |
| Tumor type ⁎⁎ | .097 | ||
| Invasive ductal | 88 (46.1) | 103 (53.9) | |
| Invasive lobular | 4 (66.7) | 2 (33.3) | |
| Invasive mucinous | 3 (100) | 0 (0) | |
| ER | .002⁎ | ||
| Positive | 68(56.2) | 53 (43.8) | |
| Negative | 27 (34.2) | 52 (65.8) | |
| PR | .001⁎ | ||
| Positive | 67 (57.3) | 50 (42.7) | |
| Negative | 28 33.7) | 55 (66.3) | |
| pAkt (n = 166) | .272 | ||
| Positive | 68 (50.4) | 67 (49.6) | |
| Negative | 19 (61.3) | 12 (38.7) | |
| pPTEN (n = 162) | .341 | ||
| Positive | 40 (48.8) | 42 (51.2) | |
| Negative | 45 (56.3) | 35(43.8) | |
| HER2 (n = 192) | .740 | ||
| Positive | 24 (51.1) | 23 (48.9) | |
| Negative | 70 (48.3) | 75 (51.7) | |
| Radiotherapy | .523 | ||
| Yes | 81 (48.5) | 86 (51.5) | |
| No | 14 (42.4) | 19 (57.6) | |
| Chemotherapy | .015⁎ | ||
| Yes | 64 (54.7) | 53 (45.3) | |
| No | 31 (37.3) | 52 (62.7) | |
| Endocrine therapy | .004⁎ | ||
| Yes | 67 (55.8) | 53 (44.2) | |
| No | 28 (35.0) | 52 (65.0) |
AR, androgen receptor; ER, estrogen receptor; PR, progesterone receptor; pAkt, phosphorylated Akt; pPTEN, phosphorylated phosphatase and tensin homolog; HER2, human epidermal growth factor receptor type 2.
Statistically significant.
Fisher exact test.
Overall Survival
Survival analysis was performed on 82 patients who had been followed for five or more years. A total of 16 deaths were reported during this period. The mean OS time was 9.2 ± 0.41 years, and lost to follow-up was 17% (n = 14) only.
AR expression and survival
Women with AR-expressing or positive tumors had significantly higher OS (mean OS = 10.2 ± 0.465 years) than women whose tumors did not express AR (mean OS = 5.8 ± 0.348 years) (P = .042; Figure 2A). Lymph node involvement showed a significant (P = .043) association with lower OS. Patients with large tumor size (P = .069) and positive pAkt status (P = .243) tended to also have decreased OS (Table 3).
Figure 2.
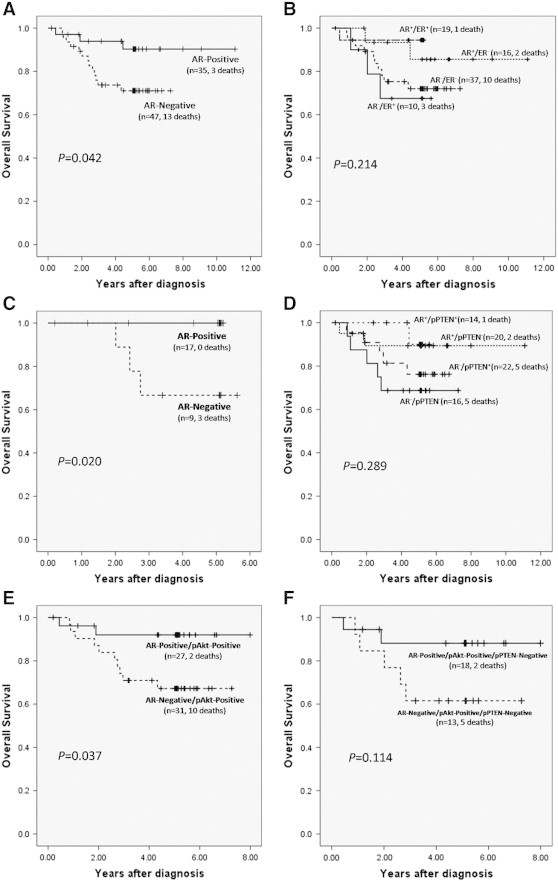
Kaplan-Meier curves compare OS stratified by (A) expression of AR in all patients with BCa, (B) expression of AR/ER, (C) expression of AR in patients receiving endocrine therapy, (D) expression of AR/pPTEN, (E) expression of AR in patients with pAkt-positive tumors, and (F) in patients with combinatorial status of pAkt-positive/pPTEN-negative tumor.
Table 3.
Survival Analysis (Kaplan-Meier and log-rank test) and Significance of AR, pAkt, Tumor Size, Grade, and Node Involvement.
| Factors | N | Mean OS in Years (± SE) | P Value |
|---|---|---|---|
| AR | .042⁎ | ||
| Negative | 47 | 5.8 (± 0.35) | |
| Positive | 35 | 10.2 (± 0.46) | |
| pAkt | .243 | ||
| Negative | 14 | 10.4 (± 0.57) | |
| Positive | 58 | 6.7 (± 0.33) | |
| Tumor size | .069 | ||
| T1 and T2 | 66 | 9.6 (± 0.42) | |
| T3 and T4 | 13 | 4.9 (± 0.54) | |
| Grade | .566 | ||
| I and II | 45 | 7.8 (± 0.42) | |
| III | 35 | 9.0 (± 0.625) | |
| Node involvement | .043⁎ | ||
| N0 | 44 | 9.5 (± 0.53) | |
| N1 | 20 | 8.6 (± 0.40) | |
| N2 | 8 | 4.7 (± 0.68) | |
| N3 | 8 | 3.9 (± 0.52) |
Statistically significant; N, number of patients; SE, standard error.
3.4.2. Relationship between AR/ER expression and survival
To compare the potential prognostic value of AR and ER coexpression on survival, patients were categorized into the following four groups: 1) AR+/ER+ (n = 19), 2) AR+/ER− (n = 16), 3) AR−/ER+ (n = 10), and 4) AR−/ER− (n = 37). Although survival analyses showed no significant OS difference among the four groups (P = .214), women with AR+/ER+ tumors showed a trend for a better OS (mean OS = 5.0 ± 0.257 years) compared to the AR−/ER+ (mean OS = 4.4 ± 0.573 years) subgroup. We also found a survival advantage of AR expression in the AR+/ER− group with only 12.5% deaths (2 of 16), compared to 27% (10 of 37) deaths in patients with AR−/ER− tumors (P = .214; Figure 2B).
AR expression, endocrine therapy, and survival
The association of AR expression with OS in the subgroup of patients receiving endocrine therapy was investigated (n = 26). In this subgroup, patients with AR-positive tumor showed significantly better OS compared to patients whose tumors did not express AR (P = .020; Figure 2C).
Relationship between AR/pPTEN expression and survival
To compare the potential prognostic impact of AR and pPTEN coexpression on survival, patients were categorized into the following four groups: 1) AR+/pPTEN+ (n = 14), 2) AR+/pPTEN− (n = 20), 3) AR−/pPTEN+ (n = 22), and 4) AR−/pPTEN− (n = 16). Although survival analyses showed that there was no significant OS difference among the four groups (P = .289), women with AR+/pPTEN+ tumors had better survival with only 7.1% deaths (1 of 14), compared to 32% deaths (5 of 16) in the AR−/pPTEN− group of patients with BCa. We also found a survival benefit of AR expression in the AR+/pPTEN− group with only 10% deaths (2 of 20), compared to 22.7% deaths in the group of patients with AR−/pPTEN + tumors (5 of 22) (P = .289; Figure 2D).
Relationship between AR/pAkt expression and survival
The association of AR with OS in pAkt-positive patients (n = 58) was determined, and we found that patients whose tumors expressed both pAkt and AR (AR+/pAkt+) had better OS compared to women with AR−/pAkt+ tumors (P = .037; Figure 2E).
Relationship of AR with pAkt+/pPTEN− combinatorial groups and survival
The implications of AR expression on disease outcome were assessed in pAkt+/pPTEN− (n = 31) tumors. Although survival analyses showed that there was no significant OS difference between patients with AR+/pAkt+/pPTEN− (n = 18) and AR−/pAkt+/pPTEN− (n = 13) tumors (P = .114), women with AR+/pAkt+/pPTEN− tumors had relatively higher OS (mean OS = 7.1 ± 0.535 years;) compared to women with AR−/pAkt+/pPTEN− tumors (mean OS = 5.1 ± 0.738 years) (Figure 2F).
Discussion
The expression of AR in this study, as determined by immunohistochemistry, demonstrated that 47.5% (95 of 200) of invasive BCa tumors, from a Pakistani cohort, expressed nuclear AR. This is similar to other reported studies, where the percentage of AR-positive tumors ranges from 40% to 80% [11], [17], [18], [19]. This wide range may reflect genuine biologic variations, arising due to environmental and genetic diversity across the globe.
In the current study, tumors that expressed AR were of low or intermediate grade (grades I and II) and expressed ER and PR, which is consistent with previous studies [11], [33]. We also found that AR expression in tumors was significantly associated with longer OS, with a survival advantage of 4.4 years, in comparison to women whose tumors did not express AR. Our data are consistent with previous studies that have assessed AR expression in BCa and its potential as an additional prognostic marker [10], [11], [12], [40], [41]. A recent meta-analysis showed that expression of AR in breast tumors emerges as an indicator of better survival [12]. We found a significant association between lymph node involvement and poor survival, whereas factors including age, HER2 status, ER, PR, and tumor size demonstrated no association with prognosis. To our knowledge, this is the first study that demonstrates a potential prognostic value of AR expression in Pakistani women who have been diagnosed with invasive BCa.
We further analyzed the prognostic significance of AR in patients who were stratified by ER status. Our analysis showed that patients with AR+/ER+ tumors had better OS compared to the group that was AR−/ER+. We also found that patients with ER-negative tumors expressing AR (AR+/ER−) had a better survival than patients with AR−/ER− tumors. However, despite displaying a positive trend of AR expression with survival, a significant association could not be ascribed in AR/ER subgroup analysis, and we would cautiously attribute this to the small sample size and low number of deaths. Previous studies suggest that AR expression is associated with improved survival among women with ER-positive tumors [42], [43]. Data supporting this assertion are based on an in vitro study that showed that AR interacted with estrogen-responsive elements on the ER gene and inhibited ER-mediated growth of BCa cells [44]. The role of AR in patients with ER-negative tumors has not been fully elucidated as only a few studies have examined AR’s role in these patients [36], [45]. There is inconsistency in studies examining AR expression in ER-negative BCa. Peters et al. found no association, whereas Agoff et al. found an association of AR expression with improved survival in patients with ER-negative tumors [45].
Expression of ER in tumors holds considerable value for the prediction of response to endocrine therapy [46], whereas only 50% of ER-positive tumors respond to endocrine therapies [47], [48]. To date, clinical benefits of AR expression in patients receiving endocrine therapy have not been exhaustively studied [49]. In our study, patients with AR+/ER+ tumors, receiving endocrine therapy, showed improved survival, compared to patients whose tumors were AR−/ER+. These results suggest that AR expression increased the sensitivity of tumors to endocrine therapy and AR negativity could possibly be associated with decreased response to endocrine therapy. Previously, Park et al. demonstrated AR as a marker for better response to endocrine treatment in ER-positive tumors [50]. Additionally, an in vitro study has found that aromatase inhibitors have a greater antiproliferative effect on AR+/ER+ BCa cell line. The inhibitory effect may have been due to inhibition of estrogen synthesis and activation of the intracellular AR signaling, caused by sustained androgen levels [51]. Taken together, these findings suggest that AR expression could be an additional significant marker for endocrine responsiveness in ER-positive cancers.
Role of PTEN as a negative regulator of Akt signaling pathway is well recognized, and these two variables are found to be inversely related with each other [52], [53]. To date, little is known about the AR-mediated regulation of Akt and PTEN expression. Therefore, we determined AR status along with pAkt and pPTEN in the same cohort of patients with BCa and analyzed the potential prognostic significance of AR in patients stratified by pAkt and pPTEN status. We found expression of pAkt and pPTEN in 81.3% and 50.6% of invasive BCa, respectively. We did not find independent association of pAkt or pPTEN expression with any clinicopathologic characteristics or survival, which is in contrast to previous studies showing association of activated Akt and loss of PTEN with poor survival [30], [37]. Absence of independent prognostic significance of pAkt and pPTEN in our study could be due to the ethnic background of the patient population and/or the number of patients studied.
To date, a very limited number of studies have examined the expression of AR/Akt/PTEN and their association or cross talk in BCas. Wang et al. reported positive correlation between AR and PTEN expression in BCa tissues [27]. Aleskandarany et al. also demonstrated a direct correlation of pAkt expression with AR status in invasive BCa [34]. Conversely, Lin et al. described an inverse relationship between Akt and AR signaling pathways, indicating that Akt inactivates AR [54] and promotes AR degradation [55] that resulted in suppression of AR-induced apoptosis. A few in vitro studies showing the related role of Akt, PTEN, and AR in BCa suggest that AR lowers Akt activity and increases PTEN expression that in turn decreases BCa cell proliferation [27], [28]. Collectively, these studies suggest that PTEN-Akt is a complex signaling pathway, operated under multiple levels of feedback; AR pathway is known to be involved in this feedback loop and has been shown to downregulate Akt and upregulate PTEN expression.
Unlike previous studies, we did not find any association between expression of pAkt and pPTEN with AR status. This suggests presence of mechanisms other than AR that might be responsible for regulating Akt/PTEN expression. However, we found that expression of AR was associated with significantly longer OS in patients with pAkt-positive tumors, suggesting protective role of AR in these patients. We also found a survival advantage with only 7.1% deaths in patients with AR+/pPTEN+ tumors, whereas loss of expression of both markers was found to be associated with lower OS with 32% deaths. These results suggest that AR-PTEN coexpression might be decreasing the cellular proliferation and increasing apoptosis (action mediated by pAkt), resulting in increased OS in the subset of patients with AR+/pPTEN+ tumors.
Reportedly, patients with Akt+ and PTEN− tumors have been shown to exhibit worst survival; however, these patients were not stratified into AR-positive and AR-negative groups [31]. We stratified tumors in context of combined expression of pAkt and pPTEN and determined the impact of AR expression on survival in patients with pAkt+/pPTEN− tumors. We found that, in a subset of women with pAkt+/pPTEN− tumors, expression of AR conferred a survival advantage, whereas loss of AR reduced the survival. Our results suggest that AR, independent of its coexpression with pPTEN, could be negatively regulating Akt-mediated proliferative effect as shown by survival advantage of 2 years in patients with AR+/pAkt+/pPTEN− tumors when compared with AR−/pAkt+/pPTEN− tumors. This did not reach to statistical significance possibly due to low number of patients (n = 31) in this subset (Figure 2D). The mechanism of these important observations where AR appears to negate the proliferative and antiapoptotic effect due to activation of Akt and loss of PTEN, respectively, warrants further study.
In the current study, survival analysis was limited to patients who went through a follow-up of 5 years or more (n = 82). A distinctly better survival was observed not only in patients with AR expression for whom we had 5-year follow-up but also in patients whose follow-up was between 2 to 11 years (n = 200, data not shown). However, relatively small number of deaths (n = 16) restricted us to perform multivariable analysis.
In conclusion, we found that, in a cohort of Pakistani women with BCa, expression of AR conferred a survival advantage independent of other markers. Furthermore, expression of AR in pAkt+/pPTEN− subgroup could be useful in distinguishing BCa with more favorable prognosis. Future studies on larger cohort of patients would be helpful in establishing the role of AR, pAkt, and pPTEN expression as significant independent prognostic and predictive factors in patients with BCa.
Acknowledgments
We are thankful to Aga Khan University for financial and technical support, the Department of Pathology and Microbiology (Zubair Ahmed) for assisting with retrieval of archival blocks, Amna Rehana Siddiqui from King Saud University for reviewing the manuscript and helpful suggestions, and all patients who contributed tissue specimen blocks that were used in the study.
Footnotes
Conflict of interest: None.
References
- 1.Bray F., McCarron P., Parkin D.M. The changing global patterns of female breast cancer incidence and mortality. Breast Cancer Res. 2004;6:229–239. doi: 10.1186/bcr932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kakarala M., Rozek L., Cote M., Liyanage S., Brenner D.E. Breast cancer histology and receptor status characterization in Asian Indian and Pakistani women in the U.S. - a SEER analysis. BMC Cancer. 2010;10:191. doi: 10.1186/1471-2407-10-191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bhurgri Y., Kayani N., Faridi N., Pervez S., Usman A., Bhurgri H., Malik J., Bashir I., Bhurgri A., Hasan S.H. Patho-epidemiology of breast cancer in Karachi '1995-1997'. Asian Pac J Cancer Prev. 2007;8:215–220. [PubMed] [Google Scholar]
- 4.Slamon D.J., Clark G.M., Wong S.G., Levin W.J., Ullrich A., McGuire W.L. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235:177–182. doi: 10.1126/science.3798106. [DOI] [PubMed] [Google Scholar]
- 5.Slamon D.J., Godolphin W., Jones L.A., Holt J.A., Wong S.G., Keith D.E., Levin W.J., Stuart S.G., Udove J., Ullrich A. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science. 1989;244:707–712. doi: 10.1126/science.2470152. [DOI] [PubMed] [Google Scholar]
- 6.Faheem M., Mahmood H., Khurram M., Qasim U., Irfan J. Estrogen receptor, progesterone receptor, and Her 2 Neu positivity and its association with tumour characteristics and menopausal status in a breast cancer cohort from northern Pakistan. Ecancermedicalscience. 2012;6:283. doi: 10.3332/ecancer.2012.283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sharif M.A., Mamoon N., Mushtaq S., Khadim M.T., Jamal S. Steroid hormone receptor association with prognostic markers in breast carcinoma in Northern Pakistan. J Coll Physicians Surg Pak. 2010;20:181–185. [PubMed] [Google Scholar]
- 8.Aziz S.A., Pervez S., Khan S., Kayani N., Azam S.I., Rahbar M.H. Significance of immunohistochemical c-ErbB-2 product localisation pattern for prognosis in human breast cancer. Pathol Oncol Res. 2001;7:190–196. doi: 10.1007/BF03032348. [DOI] [PubMed] [Google Scholar]
- 9.Moatter T., Aban M., Iqbal W., Azam I., Pervaiz A., Siddiqui F., Murad F., Pervez S. Status of HER2 amplification, polysomy 17 and histopathological features of 425 Pakistani breast cancer patients. Asian Pac J Cancer Prev. 2011;12:3069–3073. [PubMed] [Google Scholar]
- 10.Bryan R.M., Mercer R.J., Bennett R.C., Rennie G.C., Lie T.H., Morgan F.J. Androgen receptors in breast cancer. Cancer. 1984;54:2436–2440. doi: 10.1002/1097-0142(19841201)54:11<2436::aid-cncr2820541121>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 11.Hu R., Dawood S., Holmes M.D., Collins L.C., Schnitt S.J., Cole K., Marotti J.D., Hankinson S.E., Colditz G.A., Tamimi R.M. Androgen receptor expression and breast cancer survival in postmenopausal women. Clin Cancer Res. 2011;17:1867–1874. doi: 10.1158/1078-0432.CCR-10-2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Qu Q., Mao Y., Fei X.C., Shen K.W. The impact of androgen receptor expression on breast cancer survival: a retrospective study and meta-analysis. PLoS One. 2013;8:e82650. doi: 10.1371/journal.pone.0082650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Søreide J.A., Lea O.A., Varhaug J.E., Skarstein A., Kvinnsland S. Androgen receptors in operable breast cancer: relation to other steroid hormone receptors, correlations to prognostic factors and predictive value for effect of adjuvant tamoxifen treatment. Eur J Surg Oncol. 1992;18:112–118. [PubMed] [Google Scholar]
- 14.Schippinger W., Regitnig P., Dandachi N., Wernecke K.D., Bauernhofer T., Samonigg H., Moinfar F. Evaluation of the prognostic significance of androgen receptor expression in metastatic breast cancer. Virchows Arch. 2006;449:24–30. doi: 10.1007/s00428-006-0213-6. [DOI] [PubMed] [Google Scholar]
- 15.Narita D., Raica M., Suciu C., Cîmpean A., Anghel A. Immunohistochemical expression of androgen receptor and prostate-specific antigen in breast cancer. Folia Histochem Cytobiol. 2006;44:165–172. [PubMed] [Google Scholar]
- 16.Riva C., Dainese E., Caprara G., Rocca P.C., Massarelli G., Tot T., Capella C., Eusebi V. Immunohistochemical study of androgen receptors in breast carcinoma. Evidence of their frequent expression in lobular carcinoma. Virchows Arch. 2005;447:695–700. doi: 10.1007/s00428-005-0003-6. [DOI] [PubMed] [Google Scholar]
- 17.Mishra A.K., Agrawal U., Negi S., Bansal A., Mohil R., Chintamani C., Bhatnagar A., Bhatnagar D., Saxena S. Expression of androgen receptor in breast cancer & its correlation with other steroid receptors & growth factors. Indian J Med Res. 2012;135:843–852. [PMC free article] [PubMed] [Google Scholar]
- 18.Agrawal A.K., Jeleń M., Grzebieniak Z., Zukrowski P., Rudnicki J., Nienartowicz E. Androgen receptors as a prognostic and predictive factor in breast cancer. Folia Histochem Cytobiol. 2008;46:269–276. doi: 10.2478/v10042-008-0039-y. [DOI] [PubMed] [Google Scholar]
- 19.Yu Q., Niu Y., Liu N., Zhang J.Z., Liu T.J., Zhang R.J., Wang S.L., Ding X.M., Xiao X.Q. Expression of androgen receptor in breast cancer and its significance as a prognostic factor. Ann Oncol. 2010;22:1288–1294. doi: 10.1093/annonc/mdq586. [DOI] [PubMed] [Google Scholar]
- 20.Pérez-Tenorio G., Stål O., Southeast Sweden Breast Cancer Group Activation of AKT/PKB in breast cancer predicts a worse outcome among endocrine treated patients. Br J Cancer. 2002;86:540–545. doi: 10.1038/sj.bjc.6600126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Song G., Ouyang G., Bao S. The activation of Akt/PKB signaling pathway and cell survival. J Cell Mol Med. 2005;9:59–71. doi: 10.1111/j.1582-4934.2005.tb00337.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Crowder R.J., Ellis M.J. Treating breast cancer through novel inhibitors of the phosphatidylinositol 3'-kinase pathway. Breast Cancer Res. 2005;7:212–214. doi: 10.1186/bcr1307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liang K., Jin W., Knuefermann C., Schmidt M., Mills G.B., Ang K.K., Milas L., Fan Z. Targeting the phosphatidylinositol 3-kinase/Akt pathway for enhancing breast cancer cells to radiotherapy. Mol Cancer Ther. 2003;2:353–360. [PubMed] [Google Scholar]
- 24.Ghosh A.K., Grigorieva I., Steele R., Hoover R.G., Ray R.B. PTEN transcriptionally modulates c-myc gene expression in human breast carcinoma cells and is involved in cell growth regulation. Gene. 1999;235:85–91. doi: 10.1016/s0378-1119(99)00206-1. [DOI] [PubMed] [Google Scholar]
- 25.Paez J., Sellers W.R. PI3K/PTEN/AKT pathway. A critical mediator of oncogenic signaling. Cancer Treat Res. 2003;115:145–167. [PubMed] [Google Scholar]
- 26.Nagata Y., Lan K.H., Zhou X., Tan M., Esteva F.J., Sahin A.A., Klos K.S., Li P., Monia B.P., Nguyen N.T. PTEN activation contributes to tumor inhibition by trastuzumab, and loss of PTEN predicts trastuzumab resistance in patients. Cancer Cell. 2004;6:117–127. doi: 10.1016/j.ccr.2004.06.022. [DOI] [PubMed] [Google Scholar]
- 27.Wang Y., Romigh T., He X., Tan M.H., Orloff M.S., Silverman R.H., Heston W.D., Eng C. Differential regulation of PTEN expression by androgen receptor in prostate and breast cancers. Oncogene. 2011;30:4327–4338. doi: 10.1038/onc.2011.144. [DOI] [PubMed] [Google Scholar]
- 28.Wang Y., He X., Ngeow J., Eng C. GATA2 negatively regulates PTEN by preventing nuclear translocation of androgen receptor and by androgen-independent suppression of PTEN transcription in breast cancer. Hum Mol Genet. 2012;21:569–576. doi: 10.1093/hmg/ddr491. [DOI] [PubMed] [Google Scholar]
- 29.Schmitz K.J., Otterbach F., Callies R., Levkau B., Hölscher M., Hoffmann O., Grabellus F., Kimmig R., Schmid K.W., Baba H.A. Prognostic relevance of activated Akt kinase in node-negative breast cancer: a clinicopathological study of 99 cases. Mod Pathol. 2004;17:15–21. doi: 10.1038/modpathol.3800002. [DOI] [PubMed] [Google Scholar]
- 30.Vestey S.B., Sen C., Calder C.J., Perks C.M., Pignatelli M., Winters Z.E. Activated Akt expression in breast cancer: correlation with p53, Hdm2 and patient outcome. Eur J Cancer. 2005;41:1017–1025. doi: 10.1016/j.ejca.2005.02.011. [DOI] [PubMed] [Google Scholar]
- 31.Esteva F.J., Guo H., Zhang S., Santa-Maria C., Stone S., Lanchbury J.S., Sahin A.A., Hortobagyi G.N., Yu D. PTEN, PIK3CA, p-AKT, and p-p70S6K status: association with trastuzumab response and survival in patients with HER2-positive metastatic breast cancer. Am J Pathol. 2010;177:1647–1656. doi: 10.2353/ajpath.2010.090885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Polak J.M., Van Noorden S. Introduction to Immunocytochemistry. Second edition. BIOS Scientific Publishers; 1997. [Google Scholar]
- 33.Park S., Koo J., Park H.S., Kim J.H., Choi S.Y., Lee J.H., Park B.W., Lee K.S. Expression of androgen receptors in primary breast cancer. Ann Oncol. 2010;21:488–492. doi: 10.1093/annonc/mdp510. [DOI] [PubMed] [Google Scholar]
- 34.Aleskandarany M.A., Rakha E.A., Ahmed M.A., Powe D.G., Ellis I.O., Green A.R. Clinicopathologic and molecular significance of phospho-Akt expression in early invasive breast cancer. Breast Cancer Res Treat. 2011;127:407–416. doi: 10.1007/s10549-010-1012-y. [DOI] [PubMed] [Google Scholar]
- 35.Allred D.C., Harvey J.M., Berardo M., Clark G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol. 1998;11:155–168. [PubMed] [Google Scholar]
- 36.Niemeier L.A., Dabbs D.J., Beriwal S., Striebel J.M., Bhargava R. Androgen receptor in breast cancer: expression in estrogen receptor-positive tumors and in estrogen receptor-negative tumors with apocrine differentiation. Mod Pathol. 2010;23:205–212. doi: 10.1038/modpathol.2009.159. [DOI] [PubMed] [Google Scholar]
- 37.Depowski P.L., Rosenthal S.I., Ross J.S. Loss of expression of the PTEN gene protein product is associated with poor outcome in breast cancer. Mod Pathol. 2001;14:672–676. doi: 10.1038/modpathol.3880371. [DOI] [PubMed] [Google Scholar]
- 38.Dunnwald L.K., Rossing M.A., Li C.I. Hormone receptor status, tumor characteristics, and prognosis: a prospective cohort of breast cancer patients. Breast Cancer Res. 2007;9:R6. doi: 10.1186/bcr1639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Nadji M., Gomez-Fernandez C., Ganjei-Azar P., Morales A.R. Immunohistochemistry of estrogen and progesterone receptors reconsidered: experience with 5,993 breast cancers. Am J Clin Pathol. 2005;123:21–27. doi: 10.1309/4wv79n2ghj3x1841. [DOI] [PubMed] [Google Scholar]
- 40.Langer M., Kubista E., Schemper M., Spona J. Androgen receptors, serum androgen levels and survival of breast cancer patients. Arch Gynecol Obstet. 1990;247:203–209. doi: 10.1007/BF02389545. [DOI] [PubMed] [Google Scholar]
- 41.Søiland H., Kørner H., Skaland I., Janssen E.A., Gudlaugsson E., Varhaug J.E., Baak J.P., Søreide J.A. Prognostic relevance of androgen receptor detection in operable breast cancer. J Surg Oncol. 2008;98:551–558. doi: 10.1002/jso.21156. [DOI] [PubMed] [Google Scholar]
- 42.Castellano I., Allia E., Accortanzo V., Vandone A.M., Chiusa L., Arisio R., Durando A., Donadio M., Bussolati G., Coates A.S. Androgen receptor expression is a significant prognostic factor in estrogen receptor positive breast cancers. Breast Cancer Res Treat. 2010;124:607–617. doi: 10.1007/s10549-010-0761-y. [DOI] [PubMed] [Google Scholar]
- 43.Park S., Koo J.S., Kim M.S., Park H.S., Lee J.S., Lee J.S., Kim S.I., Park B.W., Lee K.S. Androgen receptor expression is significantly associated with better outcomes in estrogen receptor-positive breast cancers. Ann Oncol. 2011;22:1755–1762. doi: 10.1093/annonc/mdq678. [DOI] [PubMed] [Google Scholar]
- 44.Peters A.A., Buchanan G., Ricciardelli C., Bianco-Miotto T., Centenera M.M., Harris J.M., Jindal S., Segara D., Jia L., Moore N.L. Androgen receptor inhibits estrogen receptor-α activity and is prognostic in breast cancer. Cancer Res. 2009;69:6131–6140. doi: 10.1158/0008-5472.CAN-09-0452. [DOI] [PubMed] [Google Scholar]
- 45.Agoff S.N., Swanson P.E., Linden H., Hawes S.E., Lawton T.J. Androgen receptor expression in estrogen receptor–negative breast cancer. Immunohistochemical, clinical, and prognostic associations. Am J Clin Pathol. 2003;120:725–731. doi: 10.1309/42F0-0D0D-JD0J-5EDT. [DOI] [PubMed] [Google Scholar]
- 46.Cleator S.J., Ahamed E., Coombes R.C., Palmieri C. A 2009 update on the treatment of patients with hormone receptor-positive breast cancer. Clin Breast Cancer. 2009;9(Suppl 1):S6–S17. doi: 10.3816/CBC.2009.s.001. [DOI] [PubMed] [Google Scholar]
- 47.Bedard P.L., Freedman O.C., Howell A., Clemons M. Overcoming endocrine resistance in breast cancer: are signal transduction inhibitors the answer? Breast Cancer Res Treat. 2008;108:307–317. doi: 10.1007/s10549-007-9606-8. [DOI] [PubMed] [Google Scholar]
- 48.Ma C.X., Sanchez C.G., Ellis M.J. Predicting endocrine therapy responsiveness in breast cancer. Oncology. 2009;23:133–142. [PubMed] [Google Scholar]
- 49.Lundin K.B., Henningson M., Hietala M., Ingvar C., Rose C., Jernström H. Androgen receptor genotypes predict response to endocrine treatment in breast cancer patients. Br J Cancer. 2011;105:1676–1683. doi: 10.1038/bjc.2011.441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Park S., Park H.S., Koo J.S., Yang W.I., Kim S.I., Park B.W. Higher expression of androgen receptor is a significant predictor for better endocrine-responsiveness in estrogen receptor-positive breast cancers. Breast Cancer Res Treat. 2012;133:311–320. doi: 10.1007/s10549-011-1950-z. [DOI] [PubMed] [Google Scholar]
- 51.Macedo L.F., Guo Z., Tilghman S.L., Sabnis G.J., Qiu Y., Brodie A. Role of androgens on MCF-7 breast cancer cell growth and on the inhibitory effect of letrozole. Cancer Res. 2006;66:7775–7782. doi: 10.1158/0008-5472.CAN-05-3984. [DOI] [PubMed] [Google Scholar]
- 52.Shi W., Zhang X., Pintilie M., Ma N., Miller N., Banerjee D., Tsao M.S., Mak T., Fyles A., Liu F.F. Dysregulated PTEN-PKB and negative receptor status in human breast cancer. Int J Cancer. 2003;104:195–203. doi: 10.1002/ijc.10909. [DOI] [PubMed] [Google Scholar]
- 53.Stambolic V., Suzuki A., de la Pompa J.L., Brothers G.M., Mirtsos C., Sasaki T., Ruland J., Penninger J.M., Siderovski D.P., Mak T.W. Negative regulation of PKB/Akt-dependent cell survival by the tumor suppressor PTEN. Cell. 1998;95:29–39. doi: 10.1016/s0092-8674(00)81780-8. [DOI] [PubMed] [Google Scholar]
- 54.Lin H.K., Yeh S., Kang H.Y., Chang C. Akt suppresses androgen-induced apoptosis by phosphorylating and inhibiting androgen receptor. Proc Natl Acad Sci U S A. 2001;98:7200–7205. doi: 10.1073/pnas.121173298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lin H.K., Wang L., Hu Y.C., Altuwaijri S., Chang C. Phosphorylation-dependent ubiquitylation and degradation of androgen receptor by Akt require Mdm2 E3 ligase. EMBO J. 2002;21:4037–4048. doi: 10.1093/emboj/cdf406. [DOI] [PMC free article] [PubMed] [Google Scholar]