

Abstract
This article addresses how individuals can adjust to the experience of unattainable goals and protect their subjective well-being and physical health. We discuss theoretical aspects involved in the self-regulation of unattainable goals and point to the importance of general individual differences in goal disengagement and goal reengagement capacities. In addition, we review the extant literature, suggesting that goal disengagement capacities can reduce psychological distress and ameliorate patterns of biological dysregulation and physical health problems if individuals experience unattainable goals. Goal reengagement capacities, by contrast, are shown to be associated with positive indicators of subjective well-being (e.g., positive affect or purpose in life), but rarely predict psychological distress or physical health outcomes. We finally address several remaining issues that have become apparent in the extant literature and may deserve more attention in future research.
Self-regulation approaches to personality functioning often emphasize that the successful attainment of desired goals facilitates subjective well-being and physical health (Bandura, 1997; Carver & Scheier, 1981, 1998; Emmons, 1986, Heckhausen, Wrosch, & Schulz, 2010). This is not surprising as goals are the building blocks for the accomplishment of a variety of developmental tasks and their attainment is likely to foster long-term patterns of successful development (Heckhausen, 1999; Ryff, 1989). At times, however, it is impossible for a person to make further progress towards an important goal because the goal itself is not attainable. Such circumstances associated with the experience of unattainable goals are a relatively common phenomenon (Bauer, 2004) and can result from a lack of individual skills necessary for realizing a desired goal. In addition, goals may become unattainable if individuals encounter stressful life circumstances or age-related changes that deplete their resources and opportunities necessary for attaining them (e.g., an accident, unemployment, or a health problem, Wrosch, Scheier, Carver, & Schulz, 2003a). Regardless of its reasons, facing an unattainable goal creates a problem for a person’s quality of life because goal failure has the potential to trigger psychological distress and physical health problems (Carver & Scheier, 1990; Higgins, 1987).
Approximately ten years ago, we began to examine how individuals can minimize the adverse consequences associated with encountering unattainable goals (Wrosch, Scheier, Miller, Schulz, & Carver, 2003b). In brief, our theoretical model postulates that adaptation to unattainable goals requires individuals to disengage from the unattainable goal and to reengage in more feasible goals. In addition, it assumes that individuals differ widely and reliably in their general tendencies to disengage from unattainable goals and to reengage in other goals across different domains (i.e., in goal adjustment capacities, Wrosch et al., 2003b, 2007a; for conceptually related approaches, see Brandtstädter & Renner, 1990; Heckhausen & Schulz, 1995). These individual difference variables, in turn, are expected to play an important role in fostering quality of life if individuals experience unattainable goals.
Self-Regulation of Unattainable Goals
Different theories of self-regulation share the assumption that personal goals are important determinants of quality of life. Goals provide purpose for living, direct individual behavior, and contribute to long-term patterns of successful development (Carver & Scheier, 1998; Emmons, 1986; Heckhausen et al., 2010; Ryff, 1989). Self-regulation theories further note that personal goals can influence quality of life by forming feedback loops, in which a person’s perception is compared to a reference value (i.e., a goal, cf. Miller, Galanter, & Pribram, 1960). If such a comparison process yields a negative discrepancy (e.g., a person perceives insufficient goal progress), it typically motivates a person to engage in specific behaviors aimed at reducing this discrepancy. The perceived consequences of the ensuing behavioral response are subsequently re-compared to the reference value, resulting in a continuous process of goal regulation (Carver & Scheier, 1981, 1998).
Goals thus play an important role in the self-regulation of behavior. In particular when individuals confront difficulty, their goals can motivate persistent or new behaviors that secure the attainment of desired outcomes and improve associated quality of life (Carver & Scheier, 1998). A problem occurs, however, if it is not possible for a person to overcome goal-related problems because there is no behavior that can promote the attainment of a threatened goal. In such circumstances, when a person is confronting an unattainable goal, a likely outcome is that the person experiences emotional distress (Wrosch et al., 2003a, 2007a).
An implication of the previous discussion is that effort and persistence are not always the most adaptive responses to the experience of goal-related problems. Instead, we and others have argued that there are two fundamentally different categories of individual responses to goal-related challenges and that these responses are most effective if they are adjusted to a person’s opportunities for overcoming a goal-related problem (Carver & Scheier, 1998; Heckhausen et al., 2010; Kukla, 1972; Wright & Brehm, 1989; Wrosch, 2011). One category of responses relates to a person’s persistent and continued engagement with a threatened goal. This type of response incorporates the renewal of goal commitment and effort and should be adaptive if a person has sufficient opportunities to overcome a problem and make further progress towards a threatened goal. However, if such opportunities are absent or sharply reduced, and a person confronts an unattainable goal, the person may need to react with a different type of response. In particular, the latter circumstances may require the person to disengage from the threatened goal and to engage in other new goals. Note that the scientific literature has frequently associated goal disengagement with maladaptive psychological states, such as helplessness and depression (e.g., Seligman, 1975; Wortman & Brehm, 1975). Different from these frameworks, our approach assumes that goal disengagement and goal reengagement are natural responses that become adaptive when individuals confront unattainable goals (Wrosch et al., 2003a). In such circumstances, goal adjustment processes are likely to facilitate the abandonment of futile endeavors and promote the pursuit of new meaningful activities.
From a personality perspective, it is important to acknowledge that individuals vary widely in their responses to the experience of specific unattainable goals (Wrosch, 2011). Said differently, while some individuals easily abandon unattainable goals and readily find new goals to pursue when an important goal proves to be unattainable, other individuals have a more difficult time with disengaging from unattainable goals and reengaging in new ones (Wrosch et al., 2003b). We think that these individual differences reflect an underlying personality dimension, which shapes people’s responses to goal threats across multiple domains. We refer to these tendencies as goal adjustment capacities (Wrosch et al., 2007a).
To capture the different components involved in successful goal adjustment, we have further conceptualized the motivational processes associated with individual differences in goal disengagement and goal reengagement capacities. More specifically, goal disengagement capacities are thought to incorporate a person’s tendency to withdraw both behavioral efforts and psychological commitment from the pursuit of an unattainable goal. Goal reengagement capacities, by contrast, involve the tendency to identify new goals, commit to new goals, and start pursuing new goals when unattainable goals are being encountered (Wrosch et al., 2003b).
Our theoretical framework emphasizes the role of individual differences in goal adjustment capacities (see Figure 1). This perspective postulates that goal disengagement can reduce the psychological impact of an unattainable goal by preventing the experience of repeated failure. Goal disengagement capacities should therefore be related to the avoidance of negative aspects of subjective well-being (e.g., depression or negative affect, see solid arrows in Figure 1). The primary function of goal reengagement, by contrast, is to keep individuals who confront unattainable goals engaged in the pursuit of meaningful and attainable goals. Goal reengagement capacities should therefore promote positive aspects of subjective well-being (e.g., purpose or positive affect, Wrosch et al., 2003b, 2007a; see solid arrows in Figure 1). Further, given that effective emotional functioning can promote health-relevant biological processes (e.g., in the endocrine or immune systems, Cohen et al., 2007; Segerstrom & Miller, 2004), the psychological benefits deriving from individuals’ goal adjustment capacities should likely forecast adaptive physiological processes (e.g., normative cortisol secretion or low levels of inflammation) and reduce vulnerability to developing physical disease (see solid arrows in Figure 1).
Figure 1.
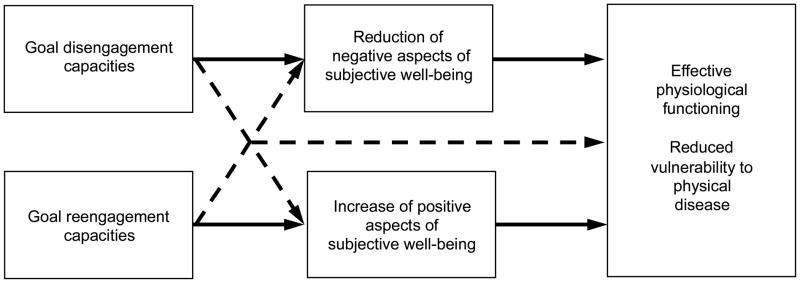
Theoretical model predicting psychological and health-related benefits of goal adjustment capacities.
Note that there may also be secondary functions of goal adjustment capacities (see dotted arrows in Figure 1). In particular, successful goal disengagement could provide resources necessary for pursuing new goals and thus also improve positive aspects of subjective well-being. In a similar vein, the engagement in new goals could make it easier for a person to accept that an important goal can no longer be pursued, which could reduce emotional distress (for functions of new goals and associated attentional shifts, see Atkinson & Birch, 1970; Gross, 1999). Finally, it is possible that goal adjustment capacities could also influence individuals’ physiological and physical health directly (see dotted arrow in Figure 1) if, for example, the abandonment of a goal has an immediate effect on the reduction of physiological stress (e.g., by lessening the likelihood that the person would be trying to accomplish too much) or if the pursuit of a new goal would result in salubrious behaviors (e.g., exercising regularly; Wrosch & Sabiston, 2013).
Goal Adjustment Capacities and Quality of Life: Empirical Evidence
To start examining our theoretical propositions, we asked participants to report how they usually react if they can no longer pursue an important goal. This approach resulted in the development of the Goal Adjustment Scale, which is a 10-item self-report instrument designed to assess general goal disengagement and goal reengagement capacities (GAS, Wrosch et al., 2003b). The items of the GAS are reported in Table 1 and were written to reflect the specific motivational components identified above (e.g., in the case of disengagement, withdrawal of effort and commitment; and in the case of reengagement, goal identification, goal commitment, and goal pursuit).
Table 1.
The Goal Adjustment Scale (adapted from Wrosch et al., 2003b).
| If I have to stop pursuing an important goal in my life, … |
|---|
Goal disengagement capacities
|
Goal reengagement capacities
|
Note. Items 2 and 4 need to be reversed coded before scale computation. The items are typically administered in a mixed order, measured on 5-point Likert-type scales (endpoints: 1 = strongly disagree; 5 = strongly agree), and averaged to obtain separate scale scores for goal disengagement and goal reengagement capacities. For further instructions, please contact the authors before use.
Research using the GAS has documented that goal disengagement and goal reengagement capacities show appropriate psychometric characteristics (Wrosch et al., 2003b, 2007a), increase from adolescence to old age (Wrosch & Miller, 2009; Wrosch et al., 2003b), and have a moderate amount of stability over time (1-year: rs = .45 to .47; 2-years: rs = .30 to .46; Dunne et al., 2011; Wrosch, 2013). In addition, associations between goal disengagement and goal reengagement capacities have generally been absent or of small to moderate size, indicating that they are largely independent constructs (Wrosch et al. 2003b, 2007a). Moreover, research has shown that goal adjustment capacities can predict adaptive outcomes, above and beyond sociodemographic characteristics and other personality constructs, such as the Big Five personality factors, dispositional optimism, or goal assimilation and accommodation (Dunne et al., 2011; Wrosch et al., 2003b). Finally, it appears that goal adjustment capacities are trans-situational in their influence, given the wide variety of circumstances in which associations with goal adjustment capacities have been found (Wrosch, 2011).
Subjective Well-Being
Several cross-sectional studies have provided evidence that goal adjustment capacities can be associated with high levels of subjective well-being. For example, studies examining samples of college students and community-dwelling adults have shown that goal disengagement capacities can relate to lower levels of perceived stress, depressive symptoms, or intrusive thoughts (Wrosch et al., 2003b, 2007a). In addition, research suggests that goal disengagement capacities are associated with beneficial outcomes among individuals who confront stressful life situations. For example, a study on female breast cancer survivors showed that goal disengagement capacities were associated with lower levels of daily negative affect (Wrosch & Sabiston, 2013). In addition, research comparing parents whose children had been diagnosed with cancer and parents of physically healthy children documented that goal disengagement capacities were particularly strongly associated with fewer depressive symptoms among parents of children with cancer (Wrosch, et al., 2003b). Such emotional benefits may occur in the context of demanding life stressors if individuals are able to disengage from goals that have become constrained by the stressor (e.g., career or leisure goals) and reprioritize time and energy for the most pressing activities (e.g., caring about their child).
There are also longitudinal studies demonstrating that goal disengagement capacities can reduce negative affect over time, thereby providing evidence for directional effects. For example, Wrosch and colleagues (2007a) showed in a sample of college students that baseline levels of goal disengagement capacities predicted fewer increases in emotional distress over the course of one semester. In addition, a longitudinal study of adolescent girls documented that improvements in goal disengagement capacities predicted subsequent declines in depressive symptoms (Wrosch & Miller, 2009).
Longitudinal research further supports that goal disengagement capacities become paramount among individuals confronting stressors that are likely to constrain their goals. For example, a study of caregivers of mentally ill family members showed that baseline levels of caregiving burden predicted 17-months increases in depressive symptoms. However, this effect was observed only among caregivers who had a difficult time disengaging from unattainable goals, but not among their counterparts who were better able to disengage (Wrosch, Amir, & Miller, 2011). Converging evidence has been reported in a 6-year longitudinal study of community-dwelling older adults, demonstrating that those older adults who experienced enhanced functional disability were particularly likely to report increases in depressive symptoms over time. However, this association was again observed only among participants who had poor goal disengagement capacities and not among participants who had high goal disengagement capacities (Dunne, Wrosch & Miller, 2011). Finally, data from the same aging study examined the role of goal disengagement capacities in the context of age-related declines in social support networks. The results showed that both long-term longitudinal and transient declines in participants’ social support networks predicted higher levels of dissatisfaction with social support. Consistent with the previous studies, these associations were obtained only among older adults who either had low levels or experienced declines in goal disengagement capacities, but not among their counterparts who reported high levels or increases in goal disengagement capacities (Wrosch, Rueggeberg, & Hoppmann, 2013).
The reported cross-sectional and longitudinal evidence provides strong support for the assumption that goal disengagement capacities can buffer the experience of psychological distress, particularly so if stressful events render important goals unattainable. Note that these studies also used participants’ goal reengagement capacities as a predictor of outcomes and the reported findings thus suggest that goal disengagement capacities are independently associated with reduced levels of psychological distress. However, the results from these studies also suggest that the effects of goal reengagement capacities frequently differ from the effects of goal disengagement capacities. In fact, the above-reported studies showed that associations between goal reengagement capacities and negative aspects of subjective well-being are often weak or absent. For example, goal reengagement capacities were not significantly associated with negative affect among breast cancer survivors (Wrosch & Sabiston, 2013), did not predict changes in emotional distress among college students or adolescent girls (Wrosch et al., 2007a; Wrosch & Miller, 2009), and were unrelated to changes in depressive symptoms among older adults who experienced functional disability (Dunne et al., 2011).
These findings do not imply that goal reengagement capacities are unrelated to all indicators of subjective well-being. By contrast, there are several studies suggesting that goal reengagement capacities can have reliable effects on positive aspects of subjective well-being. For example, goal reengagement (but not goal disengagement) capacities predicted high levels of, or longitudinal improvements in, positive affect in samples of community-dwelling adults and breast cancer survivors (Bauer, 2004; Wrosch & Sabiston, 2013). Moreover, associations between goal reengagement (but not goal disengagement) capacities and purpose in life have been documented in samples of Scottish and Canadian students and family caregivers (O’Connor & Forgan, 2007a; Wrosch et al., 2003b, 2011).
Together, these findings suggest that while goal reengagement capacities can facilitate positive aspects of subjective well-being, goal disengagement capacities are particularly likely to ameliorate negative aspects of subjective well-being. Although there are exceptions to this pattern of findings across studies (Wrosch et al., 2007a), we think that these differential effects may be based on the main functions of goal disengagement and goal reengagement capacities. As stated earlier, goal disengagement is thought to primarily relieve psychological distress by preventing repeated goal failure. The primary function of goal reengagement, by contrast, is to keep a person engaged in feasible activities that are meaningful and valuable, which could cause the stronger effects of goal reengagement capacities on positive aspects of subjective well-being (Wrosch et al., 2007a).
Nonetheless, there is another possibility that could explain the generally weak effects of goal reengagement capacities on relieving psychological distress. In this regard, it should be considered that individuals sometimes adopt goals that are maladaptive or too many in number, which may expend their coping resources and prevent them from effectively addressing pressing life demands (cf. Wrosch, Bauer, & Scheier, 2005). Evidence for such detrimental effects has been reported in two studies. First, the previously addressed study of family caregivers demonstrated that although goal reengagement capacities were positively associated with caregivers’ purpose in life, at the same time goal reengagement capacities predicted higher levels of caregiving burden (Wrosch et al., 2011). Second, the above-reported research on older adults’ social support showed that if older adults experienced a longitudinal increase in social support (which often occurs in the context of emerging illness, Helgeson, 1993), they were able to prevent social dissatisfaction only if they did not tend to engage in new goals (Wrosch et al., 2013). These findings imply that it is, at times, more beneficial for a person’s well-being not to pursue new goals. We think that such effects may occur if the pursuit of maladaptive or too many goals depletes an individual’s resources needed for appropriately managing stressful life circumstances (e.g., an illness or caregiving). In such situations, it may be more useful to maintain a balanced set of goals to prevent conflicts between different goals and protect resources needed for effectively addressing the stressor. Consistent with this conclusion, a mismatch between personal resources and situational demands has been shown to elicit adverse psychological states in other research (Nakamura & Csikszentmihalyi, 2002).
Physical Health
Research has also examined the associations between goal adjustment capacities and processes involved with indicators of physical health. These studies are based on the assumption that failure to adjust to unattainable goals can have adverse effects on a person’s biological functioning and physical health. In addition, some of these studies have investigated whether effects of goal adjustment capacities on physical health may occur because the successful adjustment to unattainable goals protects individuals’ emotional well-being (for associations between emotions, biological functioning, and disease, see Cohen et al., 2007; Kiecolt-Glaser et al., 2002; Miller, Chen, & Zhou, 2007).
Empirical evidence for an association between goal disengagement capacities and physical health outcomes has been reported in a cross-sectional study of community-dwelling adults. The results of this study documented that goal disengagement capacities were significantly associated with reports of fewer illness symptoms (e.g., eczema, headaches, constipation). Moreover, this association was statistically mediated by low levels of depressive symptoms (Wrosch et al., 2007a). This pattern of findings has been replicated in a longitudinal study of colleague students. The study’s results demonstrated that to the extent students had higher levels of goal disengagement capacities at the beginning of the semester, they reported fewer illness symptoms and better sleep towards the end of the semester. Similar to the previous study, the associations between poor goal disengagement capacities with more symptom complaints and sleeping problems were mediated by increases in emotional distress across the semester (Wrosch et al., 2007a). These findings indicate that goal disengagement capacities may contribute to better self-perceived health because they ameliorate emotional distress.
Research has also begun to identify some of the underlying biological mechanisms that could link goal adjustment capacities and physical health. Such biological pathways may be associated with processes in specific health-relevant bodily systems that can become dysregulated by the experience of failure and distress, such as individuals’ endocrine and immune functioning (as indicated in levels of cortisol or C-reactive protein, Cohen et al., 2007; Miller & Blackwell, 2006). Consistent with this possibility, a cross-sectional study of adults showed that goal disengagement capacities predicted a steeper, more normative, slope of diurnal cortisol secretion across a typical day in participants’ lives. In particular, those participants who had difficulty disengaging from unattainable goals secreted higher levels of cortisol during the day and evening hours, as compared to their counterparts who were more capable of disengaging from unattainable goals (Wrosch et al., 2007a). These findings imply that goal disengagement capacities have the potential to affect secretion patterns of a hormone that has wide-ranging regulatory influences in the body and through this mechanism could influence physical health outcomes (Sephton et al., 2000; Smyth, Ockenfels, Gorin, et al., 1997).
There is also longitudinal evidence associating goal disengagement capacities with changes in a biological indicator of immune function. This study examined a group of adolescent girls over approximately one year and predicted changes in C-reactive protein (CRP), which is a biomarker of mild, chronic inflammation. The results showed that among participants with poor goal disengagement capacities, levels of CRP increased reliably over the study period. By contrast, levels of CRP remained low and fairly stable among participants who had an easier time disengaging from unattainable goals (Miller & Wrosch, 2007). Given that chronic inflammation represents a risk factor for a variety of diseases (e.g., diabetes or heart disease, Dandona, Aljada, Chaudhuri, et al., 2005; Willerson & Ridker, 2004), these findings provide evidence for another mechanism potentially linking goal disengagement capacities and physical health outcomes.
The reported results examining associations between goal disengagement capacities and indicators of physical health were also controlled for participants’ goal reengagement capacities and thus suggest that goal disengagement capacities are a unique predictor of health-relevant processes. However, similar to the findings for predicting subjective well-being, goal reengagement capacities did not exert the same health effects as goal disengagement capacities. In particular, goal reengagement capacities were not significantly associated with levels of physical illness symptoms or cortisol secretion in the reported samples of adults (Wrosch et al., 2007a), and they did not predict CRP among adolescent girls or breast cancer survivors (Miller & Wrosch, 2007). In addition, goal reengagement capacities did not forecast fewer illness symptoms and better sleep quality in the addressed longitudinal study of college students.
We think that the frequent absence of an association between goal reengagement capacities and indicators of physical health could be related to the different emotional consequences of goal disengagement and goal reengagement capacities. In this regard, the presence of emotional distress may exert more reliable effects on health-relevant outcomes than the absence of positive emotions. Such a pattern may occur because negative emotions seem to be more consistently associated with biological processes and physical health outcomes than positive emotions (Pressman & Cohen, 2005). In fact, positive emotions may not only facilitate adaptive behavioral and physiological processes, but at times also exert opposing effects (e.g., not recognizing symptoms of disease, increased cardiovascular response, poor pulmonary function, or increased cortisol; Pressman & Cohen, 2005). Thus, the mixed health-related consequences of positive emotions and the relatively weak associations between goal reengagement capacities and emotional distress may explain why goal reengagement capacities are often unrelated to indicators of physical health.
Note that the latter conclusion does not imply that that there are no circumstances in which goal reengagement capacities could contribute to physical health benefits. While extant research has largely focused on emotion-related mechanisms linking goal adjustment capacities and physical health, it is important to consider that there are also behavioral mechanisms that could be directly influenced by goal reengagement capacities and contribute independently to physical health outcomes. Evidence for such a possibility has been documented in the previously addressed study of breast cancer survivors. In this study, participants’ goal reengagement capacities were associated with the perception of fewer daily physical symptoms (e.g., pain or difficulty breathing), and this effect was mediated by higher levels of physical activity (Wrosch & Sabiston, 2013). Thus, goal reengagement capacities may provide physical health benefits if these capacities trigger behavioral responses that are likely to provide health-related benefits.
Remaining Issues
The reviewed literature demonstrates that the capacity to disengage from unattainable goals can ameliorate psychological distress and through this mechanism may protect individuals against health-compromising biological and physical changes. Goal reengagement capacities, by contrast, were shown to predict positive aspects of subjective well-being, but are frequently unrelated to psychological distress and physical health processes (unless they directly motivate salubrious behaviors). In addition, goal reengagement capacities may at times deplete important resources in the context of demanding life stressors, which could create goal conflicts and declines in subjective well-being. Although these findings clearly suggest that goal adjustment capacities play an important role in minimizing some of the adverse consequences of encountering unattainable goals, there are remaining issues that may deserve more attention in future research.
Interactions Between Goal Adjustment Capacities
As mentioned earlier, goal disengagement and goal reengagement capacities are typically not strongly correlated with each other, which makes it possible to conceptualize interaction effects involving both dimensions (Wrosch et al., 2003b, 2007a). To this end, it seems reasonable to assume that the combination of high goal disengagement in conjunction with high goal reengagement capacities is most beneficial because it could increase the likelihood that a person abandons an unattainable goal and engages in new meaningful activities. Such a pattern has been reported among breast cancer survivors, showing that women who had high levels of both goal disengagement and goal reengagement capacities reported the most adaptive lifestyle behaviors and the largest increases in positive affect over time (Wrosch & Sabiston, 2013). This finding could imply that goal disengagement and goal reengagement capacities are both needed for the effective management of particularly difficult life circumstances.
Other research, however, has documented different patterns of interaction effects. For example, two studies of young adults showed that among participants who reported difficulty disengaging from unattainable goals, a higher capacity to reengage was associated with better emotional well-being and fewer health symptoms (Wrosch et al., 2003b, 2007a). Thus, goal reengagement capacities may also buffer the adverse emotional consequences of poor goal disengagement capacities. We think that such buffering effects may be observed if reengaging in new goals does not deplete a person’s resources, which could occur particularly among younger adults who often have relatively few responsibilities and greater psychological and physical reserves than older adults, or populations that are experiencing extreme circumstances.
Finally, interaction effects have been considered in research among vulnerable individuals whose life circumstances often involve relatively few available alternative goals (i.e., patients who had a suicidal episode or older adults, O’Connor et al., 2009; Wrosch et al., 2003b, 2007a). This research suggests that if individuals are not able to identify and pursue new goals, it may at times be more adaptive for them to continue the pursuit of important goals, even if they are unfeasible, than to have nothing else to pursue in life. Interestingly, this research also suggests that, among individuals who tend to disengage from unattainable goals, reengagement capacities become particularly important, supposedly because high reengagement capacity promotes the pursuit of some new meaningful activities in situations that involve only few available goals. Overall, we think that the obtained patterns of interaction effects are meaningful and indicate that different profiles of goal disengagement and goal reengagement capacities can become more or less adaptive in different life circumstances. Future research should examine this possibility more systematically to shed light on the adaptive value of the interplay between different goal adjustment capacities.
The Role of Coping
Our previous discussion suggests that beneficial effects of goal reengagement capacities on physical health can be triggered by specific behavioral strategies (e.g., physical activity, Wrosch & Sabiston, 2013). Such a behavioral response to the occurrence of a stressor could be conceptualized as coping (Lazarus & Folkman, 1984) and may represent an adaptive mechanism that links goal adjustment capacities with psychological and physical health benefits. Effective coping responses, however, could also be facilitated by goal disengagement capacities. If individuals are capable of disengaging from goals that have become constrained by the occurrence of a stressor, this process may free resources that can be used to manage the challenging situation more effectively. Evidence for such behavioral consequences of goal disengagement capacities has been shown in a study examining the inter-generational succession process in family business. In this study, goal disengagement capacities were related to more concrete steps towards retirement over time among business owners nearing normative retirement age (Gagne, Wrosch, & Brun de Pontet, 2011). In addition, research from the reported study of family caregivers showed that the beneficial effect of goal disengagement capacities on fewer depressive symptoms was mediated by effective coping responses, in particular by the avoidance of self-blame for caregiving problems and a reduced use of substances for regulating caregiving-related emotions (Wrosch et al., 2011). Individual differences in such emotion-focused coping strategies may be particularly influential in circumstances when a stressor is likely to persist in a person’s future because they may protect the person’s emotional and behavioral resources needed for effective future action (Heckhausen et al., 2010). Nonetheless, we think that more research is needed to identify the specific coping patterns of individuals who are able to protect their psychological and physical health by adjusting to unattainable goals.
What Facilitates Goal Adjustment?
Considering the observed benefits of goal adjustment capacities, it will be important to identify the processes that make it generally easier for people to adjust to unattainable goals. Such knowledge could be used to improve quality of life among individuals who have difficulty adjusting to unattainable goals. However, there is a paucity of research examining this question. One of the few existing studies revealed that baseline levels of depressive mood predicted a steeper increase in goal disengagement capacities over time in a sample of adolescents (Wrosch & Miller, 2009). Although this finding is consistent with theories linking depressive states with goal disengagement (Seligman, 1975; Wortman & Brehm, 1975), it also confirms evolutionary approaches, suggesting that when individuals are unable to overcome obstacles in the pursuit of personal goals, ensuing depressive mood can serve adaptive functions by facilitating goal disengagement (Klinger, 1975; Nesse, 2000). Supporting the latter assumption, further analyses showed that the observed increase in adolescents’ goal disengagement capacities predicted a subsequent reduction of depressive symptoms (Wrosch & Miller, 2009). However, more research is needed to examine whether such effects can also be observed in other segments of the life course, and whether they are restricted to the influence of ordinary low mood or extend to clinical states of depression. In addition, theory and research has suggested that other personality factors (e.g., optimism, self-mastery, social comparisons, or reappraisals; Aspinwall & Richter, 1999; Heckhausen et al., 2010) can facilitate disengagement from specific unattainable goals. In this regard, future research may reveal whether these factors also improve individuals’ general goal disengagement capacities. Finally, research may identify variables that could enhance individuals’ goal reengagement capacities. In this regard, a recent study building on the motivational benefits of positive emotions (Fredrickson, 2001) suggests that improvements in goal reengagement capacities could derive from positive psychological states (Haase, Aviram, Wrosch, et al., 2013).
When is it Time to Disengage?
Although our research showed that being able to adjust to unattainable goals is an adaptive personality characteristic, it did not address when exactly it is an appropriate time to disengage? We think that there is no easy answer to this question since it can be costly to persist in the pursuit of goals that are already out of reach, just as disengaging too early may result in failing to accomplish important life tasks. To shed light on the process that could make disengagement adaptive, some theories have suggested that individuals step out of their goal attainment efforts if they encounter problems with goal progress to reevaluate the goal-related circumstances by weighing the pros and cons of continued goal pursuit (Brandstätter & Schüler, 2012; Carver & Scheier, 1998; Heckhausen et al., 2010). From this perspective, a realistic perception and evaluation of opportunities for goal attainment would be key for making adaptive decisions about persisting versus disengaging. Other theories, however, have suggested that disengagement may not necessarily occur as a consequence of conscious evaluations, but could be an automatic response during which a person non-consciously adjusts the value of a goal (Brandtstädter, 2000). To this end, more research is needed to examine whether goal disengagement is a deliberative or non-conscious process, and whether accurate perceptions of goal-related opportunities are necessary for producing adaptive consequences of persistence and disengagement. Such research may also use experimental paradigms to manipulate participants’ opportunity perceptions of, or disengagement processes from, specific goals and assess the extent to which individuals’ resources become depleted (Baumeister et al., 1998). Some research has already begun to apply such an approach by engaging individuals who experienced life regrets that were hard to undo in disengagement-supportive processes (e.g., self-protective social comparison and attributions) through a writing intervention (e.g., writing about other people’s regrets and factors outside a person’s control). This research demonstrated that facilitating disengagement-supportive processes through intervention resulted in improvements of individuals’ sleep quality (Wrosch et al., 2007b). We feel that more research along these lines is warranted and may further contribute to revealing the psychological processes that enable individuals to adjust successfully to the experience of unattainable goals.
Acknowledgments
The completion of this manuscript was supported by a grant from Social Sciences and Humanities Research Council of Canada to Carsten Wrosch, grants from Canadian Institutes of Health Research to Carsten Wrosch or Gregory Miller, and support from the National Center for Complementary and Alternative Medicine (AT007262) to Michael Scheier.
Biographies
Carsten Wrosch is Professor of Psychology at Concordia University in Montreal, Canada. His research addresses the importance of personality processes for maintaining psychological and physical health in the context of age-normative and non-normative life challenges. Dr. Wrosch’s theoretical and empirical work has been published in the leading journals of psychology. He received a New Investigator Award and the Recognition Prize in Research in Aging from Canadian Institutes of Health Research (CIHR). His research has been funded by CIHR and Social Sciences and Humanities Research Council of Canada.
Michael F. Scheier is Professor and Head of Psychology at Carnegie Mellon University. He is a personality and social psychologist interested in understanding individual differences in well-being and health. Dr. Scheier’s lifetime contributions on the effects of different personality dimensions (e.g., self-awareness, optimism, or coping) have resulted in a comprehensive body of theory and research on the self-regulation of behavior. He received awards from the American Psychological Association for Outstanding Contributions to Health Psychology and the Donald T. Campbell Award for Distinguished Lifetime Contributions to Social Psychology.
Gregory E. Miller is Professor of Psychology at Northwestern University. He previously held appointments in the psychology departments at Washington University and University of British Columbia. His research addresses the psychobiological pathways linking stressful life circumstances with physical health outcomes. Dr. Miller has published numerous influential articles in both leading psychological and medical journals. For his work, he received the Herbert Weiner Early Career Award from the American Psychosomatic Society and the Distinguished Scientific Award for Early Career Contributions to Health Psychology from the American Psychological Association. His research has been funded by CIHR and National Institutes of Health.
References
- Aspinwall LG, Richter L. Optimism and self-mastery predict more rapid disengagement from unsolvable tasks in the presence of alternatives. Motivation and Emotion. 1999;23:221–45. doi: 10.1023/A:1021367331817. [DOI] [Google Scholar]
- Atkinson JW, Birch D. The dynamics of action. New York: John Wiley; 1970. [PubMed] [Google Scholar]
- Bandura A. Self-efficacy: The exercise of control. New York: Freeman; 1997. [DOI] [Google Scholar]
- Bauer I. Unpublished master’s thesis. Concordia University; Montreal, Quebec, Canada: 2004. Unattainable goals across adulthood and old age: Benefits of goal adjustment capacities on well-being. [Google Scholar]
- Brandtstädter J. Emotion, cognition, and control: Limits of intentionality. In: Perrig WJ, Grob A, editors. Control of human behavior, mental processes, and consciousness: Essays in honor of the 60th birthday of August Flammer. Mahwah, NJ: Erlbaum; 2000. pp. 3–16. [Google Scholar]
- Brandtstädter J, Renner G. Tenacious goal pursuit and flexible goal adjustment: Explication and age-related analysis of assimilative and accommodative strategies of coping. Psychology and Aging. 1990;5:58–67. doi: 10.1037/0882-7974.5.1.58. [DOI] [PubMed] [Google Scholar]
- Brandstätter V, Schüler J. Action crisis and cost-benefit thinking: A cognitive analysis of a goal-disengagement phase. Journal of Experimental Social Psychology. 2012;49:543–553. doi: 10.1016/j.jesp.2012.10.004. [DOI] [Google Scholar]
- Baumeister RF, Bratslavsky E, Muraven M, Tice DM. Ego depletion: Is the active self a limited resource? Journal of Personality and Social Psychology. 1998;74:1252–1265. doi: 10.1037//0022-3514.74.5.1252. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF. Attention and self-regulation: A control-theory approach to human behavior. New York, NY: Springer-Verlag; 1981. [DOI] [Google Scholar]
- Carver CS, Scheier MF. Origins and functions of positive and negative affect: A control-process view. Psychological Review. 1990;97:19–35. doi: 10.1037/0033-295X.97.1.19. [DOI] [Google Scholar]
- Carver CS, Scheier MF. On the self-regulation of behavior. New York, NY: Cambridge University Press; 1998. [DOI] [Google Scholar]
- Cohen S, Janicki-Deverts D, Miller GE. Psychological stress and disease. Journal of the American Medical Association. 2007;298:1685–1687. doi: 10.1001/jama.298.14.1685. [DOI] [PubMed] [Google Scholar]
- Dandona P, Aljada A, Chaudhuri A, Mohanty P, Garg R. Metabolic syndrome: A comprehensive perspective based on interactions between obesity, diabetes, and inflammation. Circulation. 2005;111:1448–54. doi: 10.1161/01.CIR.0000158483.13093.9D. [DOI] [PubMed] [Google Scholar]
- Dunne E, Wrosch C, Miller GE. Goal disengagement, functional disability, and depressive symptoms in old age. Health Psychology. 2011;30:763–770. doi: 10.1037/a0024019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emmons RA. Personal strivings: An approach to personality and subjective well-being. Journal of Personality and Social Psychology. 1986;51:1058–1068. doi: 10.1037/0022-3514.51.5.1058. [DOI] [Google Scholar]
- Fredrickson BL. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. American Psychologist. 2001;56:218–226. doi: 10.1037/0003-066X.56.3.218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gagne M, Wrosch C, Brun de Pontet S. Retiring from the family business: The role of goal adjustment capacities. Family Business Review. 2011;24:292–304. doi: 10.1177/0894486511410688. [DOI] [Google Scholar]
- Gross JJ. Emotion regulation: Past, present, future. Cognition and Emotion. 1999;13:551–573. doi: 10.1080/026999399379186. [DOI] [Google Scholar]
- Haase CM, Aviram T, Wrosch C, Silbereisen RK, Heckhausen J. Well-being as a resource for goal reengagement: Evidence from two longitudinal studies. 2013 Manuscript under review. [Google Scholar]
- Heckhausen J. Developmental regulation in adulthood. New York: Cambridge University Press; 1999. [Google Scholar]
- Heckhausen J, Wrosch C, Schulz R. A motivational theory of life-span development. Psychological Review. 2010;117:32–60. doi: 10.1037/a0017668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heckhausen J, Schulz R. A life-span theory of control. Psychological Review. 1995;102:284–304. doi: 10.1037/0033-295X.102.2.284. [DOI] [PubMed] [Google Scholar]
- Helgeson VS. The onset of chronic illness: Its effect on the patient-spouse relationship. Journal of Social and Clinical Psychology. 1993;12:406–428. doi: 10.1521/jscp.1993.12.4.406. [DOI] [Google Scholar]
- Higgins ET. Self-discrepancy: A theory relating self and affect. Psychological Review. 1987;94:319–340. doi: 10.1037/0033-295X.94.3.319. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, McGuire L, Robles T, Glaser R. Emotions, morbidity, and mortality: New perspectives from psychoneuroimmunology. Annual Review of Psychology. 2002;53:83–107. doi: 10.1146/annurev.psych.53.100901.135217. [DOI] [PubMed] [Google Scholar]
- Klinger E. Consequences of commitment to and disengagement from incentives. Psychological Review. 1975;82:1–25. doi: 10.1037/h0076171. [DOI] [Google Scholar]
- Kukla A. Foundations of an attributional theory of performance. Psychological Review. 1972;79:454–70. doi: 10.1037/h0033494. [DOI] [Google Scholar]
- Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984. [Google Scholar]
- Miller GA, Galanter E, Pribram KH. Plans and the structure of behavior. New York: Henry Holt & Co; 1960. [DOI] [Google Scholar]
- Miller GE, Blackwell E. Turn up the heat: Inflammation as a mechanism linking chronic stress, depression, and heart disease. Current Directions in Psychological Science. 2006;15:269–72. doi: 10.1111/j.1467-8721.2006.00450.x. [DOI] [Google Scholar]
- Miller GE, Chen E, Zhou ES. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychological Bulletin. 2007;133:25–45. doi: 10.1037/0033-2909.133.1.25. [DOI] [PubMed] [Google Scholar]
- Miller GE, Wrosch C. You’ve gotta know when to fold’em: Goal disengagement and systemic inflammation in adolescence. Psychological Science. 2007;18:773–777. doi: 10.1111/j.1467-9280.2007.01977.x. [DOI] [PubMed] [Google Scholar]
- Nakamura J, Csikszentmihalyi M. The concept of flow. In: Snyder CR, Lopez SJ, editors. Handbook of positive psychology. Oxford University Press; New York: 2002. pp. 89–105. [Google Scholar]
- Nesse RM. Is depression an adaptation? Archives of General Psychiatry. 2000;57:14–20. doi: 10.1001/archpsyc.57.1.14. [DOI] [PubMed] [Google Scholar]
- O’Connor RC, Forgan G. Suicidal thinking and perfectionism: The role of goal adjustment and behavioral inhibition/activation systems. Journal of Rational-Emotive & Cognitive-Behavior Therapy. 2007;25:321–341. doi: 10.1007/s10942-007-0057-2. [DOI] [Google Scholar]
- O’Connor RC, Fraser L, Whyte MC, MacHale S, Masterton G. Self-regulation of unattainable goals in suicide attempters: The relationship between goal disengagement, goal reengagement and suicidal ideation. Behaviour Research and Therapy. 2009;47:164–9. doi: 10.1016/j.brat.2008.11.001. [DOI] [PubMed] [Google Scholar]
- Pressman SD, Cohen S. Does positive affect influence health? Psychological Bulletin. 2005;131:925–971. doi: 10.1037/0033-2909.131.6.925. [DOI] [PubMed] [Google Scholar]
- Ryff CD. Happiness is everything, or is it? Exploration of the meaning of psychological well-being. Journal of Personality and Social Psychology. 1989;57:1069–1081. doi: 10.1037/0022-3514.57.6.1069. [DOI] [Google Scholar]
- Segerstrom SC, Miller GE. Stress and the human immune system: A meta-analytic review of 30 years of inquiry. Psychological Bulletin. 2004;130:601–30. doi: 10.1037/0033-2909.130.4.601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seligman MEP. Helplessness. San Francisco: Freeman; 1975. [Google Scholar]
- Sephton SE, Sapolsky RM, Kraemer HC, Spiegel D. Diurnal cortisol rhythm as a predictor of breast cancer survival. Journal of the National Cancer Institute. 2000;92:994–1000. doi: 10.1093/jnci/92.12.994. [DOI] [PubMed] [Google Scholar]
- Smyth JM, Ockenfels MC, Gorin AA, Catley D, et al. Individual differences in the diurnal cycle of cortisol. Psychoneuroendocrinology. 1997;22:89–105. doi: 10.1016/S0306-4530(96)00039-X. [DOI] [PubMed] [Google Scholar]
- Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor. Circulation. 2004;109:2–10. doi: 10.1161/01.CIR.0000129535.04194.38. [DOI] [PubMed] [Google Scholar]
- Wortman CB, Brehm JW. Responses to uncontrollable outcomes: An integration of reactance theory and the learned helplessness model. In: Berkowitz L, editor. Advances in experimental social psychology. Vol. 8. New York: Academic Press; 1975. pp. 277–336. [Google Scholar]
- Wright RA, Brehm JW. Energization and goal attractiveness. In: Pervin LA, editor. Goal concepts in personality and social psychology. Hillsdale, NJ: Erlbaum; 1989. pp. 169–210. [Google Scholar]
- Wrosch C. Self-regulation of unattainable goals and pathways to quality of life. In: Folkman S, editor. The Oxford Handbook of Stress, Health, and Coping. New York: Oxford University Press; 2011. pp. 319–333. [DOI] [Google Scholar]
- Wrosch C. Unpublished data. Concordia University; 2013. Analysis of longitudinal data among romantic couples. [Google Scholar]
- Wrosch C, Amir E, Miller GE. Goal adjustment capacities, coping, and subjective well-being: The sample case of caregiving for a family member with mental illness. Journal of Personality and Social Psychology. 2011;100:934–946. doi: 10.1037/a0022873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wrosch C, Bauer I, Miller GE, Lupien S. Regret intensity, diurnal cortisol secretion, and physical health in older individuals: Evidence for directional effects and protective factors. Psychology and Aging. 2007b;22:319–330. doi: 10.1037/0882-7974.22.2.319. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Bauer I, Scheier MF. Regret and quality of life across the adult life span: The influence of disengagement and available future goals. Psychology and Aging. 2005;20:657–670. doi: 10.1037/0882-7974.20.4.657. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Miller GE. Depressive symptoms can be useful: Self-regulatory and emotional benefits of dysphoric mood in adolescence. Journal of Personality and Social Psychology. 2009;96:1181–1190. doi: 10.1037/a0015172. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Miller GE, Scheier MF, Brun de Pontet S. Giving up on unattainable goals: Benefits for health? Personality and Social Psychology Bulletin. 2007a;33:251–65. doi: 10.1177/0146167206294905. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Rueggeberg R, Hoppmann CA. Satisfaction with social support in older adulthood: The influence of social support declines and goal adjustment capacities. Psychology & Aging. 2013 doi: 10.1037/a0032730. Online first. [DOI] [PubMed]
- Wrosch C, Sabiston CM. Goal adjustment, physical and sedentary activity, and well-being and health among breast cancer survivors. Psychooncology. 2013;22:581–589. doi: 10.1002/pon.3037. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Scheier MF, Carver CS, Schulz R. The importance of goal disengagement in adaptive self-regulation: When giving up is beneficial. Self and Identity. 2003a;2:1–20. doi: 10.1080/15298860309021. [DOI] [Google Scholar]
- Wrosch C, Scheier MF, Miller GE, Carver CS. When meaning is threatened: The importance of goal adjustment for psychological and physical health. In: Wong PT, editor. The Human Quest for Meaning. Routledge: 2012. pp. 535–553. [DOI] [Google Scholar]
- Wrosch C, Scheier MF, Miller GE, Schulz R, Carver CS. Adaptive self-regulation of unattainable goals: Goal disengagement, goal reengagement, and subjective well-being. Personality and Social Psychology Bulletin. 2003b;29:1494–1508. doi: 10.1177/0146167203256921. [DOI] [PubMed] [Google Scholar]