

Abstract
Background:
While critical care nurses are vulnerable to burnout because of the complex nature of patients’ health problems, working in critical care areas has become even more complicated by shift working schedules. This study aimed to determine the relationship between fixed and rotating shifts and burnout in a sample of critical care nurses working in critical care areas.
Materials and Methods:
In this retrospective cohort design, 170 critical care nurses from six selected hospitals were chosen using quota and random sampling and divided into two groups (exposed and non-exposed). Maslach Burnout Inventory was used for data collection and independent t-test and logistic regression was performed to analyze the data.
Results:
The mean scores of emotional exhaustion (EE) and depersonalization (DP) were significantly high in the non-exposed group, but the mean score of personal accomplishment (PA) had no significant difference in the two groups. Furthermore, the non-exposed group had 10.1 times the odds to expose to EE and 2.2 times the odds to expose to DP in comparison with the exposed group. High levels of burnout in the non-exposed group were 60%, 32.9%, and 27.1%, and in the exposed group were 12.9%, 18.8% and 43.5% in EE, DP and PA, respectively.
Conclusions:
The present study has revealed that critical care nurses with fixed shift schedules display more burnout compared to those working with rotating shift schedules.
Keywords: Burnout, critical care unit, nursing, shift work
INTRODUCTION
Nursing is cited as one of the most prone professions to burnout.[1] Critical care nurses work in an unpredictable and highly stressful environment. This physical and psychological distress can lead them to burnout.[2] Burnout consists of three dimensions: Emotional exhaustion (EE), depersonalization (DP), and reduced personal accomplishment (PA). EE refers to lack of energy and a feeling that emotional sources have been lost due to too much spiritual desire. DP is known as behaving others as objects pessimistically and with cruel views. Red uced PA is defined as self-evaluative feelings of incompetence and lack of achievement at work.[3,4]
Physical illness,[5] emotional problems,[1] increased turnover,[6] absenteeism,[2] poor job performance,[7] and negative attitudes in general[5] are some of the problems that have been associated with burnout. Moreover, burnout could affect the quality of patient care. Billions of dollars are lost annually due to low productivity, staff turnover, and work absence caused by burnout.[8]
High rates of severe burnout have been reported in critical care nurses. One study with a large number of Intensive Care Unit (ICU) nurses (N = 3000) across Europe found that burnout was contagious between colleagues. Nurses who reported the highest amount of burnout in their colleagues were also the most likely to experience high levels of burnout themselves.[9] Another study showed that psychologically stressful situations, a physically demanding workload, and a high requirement for technological skills can lead ICU caregivers to burnout. Other studies have reported that 28% of nurses had high level of burnout[10] and one-third of ICU nursing staff had severe burnout.[6] One study on more than 10,000 nurses from five different countries found an incidence of burnout that ranged from 54% to 32%.[11]
While critical care nurses are vulnerable to burnout because of the complex nature of wpatient's health problems, working in critical care areas has become even more complicated by shift working schedules. With regard to the influence of day, afternoon, night, and rotating shifts on nurses, it was found that job performances and satisfaction was less on a rotating roster than on a fixed roster. In addition, this can result in psychosocial effects such as feeling of fatigue and disorientation.[12] Many health impairments associated with shift work exposure have been reported.[12,13,14,15] Furthermore, studies have reported shift working as one of the inducing factors of burnout.[16]
Despite the overwhelming statistical evidence for adverse health and well-being in shift workers,[15] our knowledge about the relationship between shift work and burnout is far from complete. One of the reasons may stem from the fact that current schedules implemented in hospitals differ enormously.[17] Moreover, demands in each shift vary with the actual workload and time pressure, partly depending on the provision of co-workers and facilities, or a special setting such as critical care areas.
Most hospitals in Iran require nurses to work in rotating or fixed shifts. A typical work schedule for a nurse who works in rotating shift is a combination of morning shift (7 h), evening shift (7 h), and night shift (12 h) within a month. For a nurse working with a fixed shift, the work schedule is morning shifts (without a combination of evening and night shifts), evening shifts (without a combination of morning and night shifts), or night shifts alone without combination of other shifts within a month. Studies showed that burnout in different shift scheduling has a different prevalence.[18]
To our knowledge, there is no study to show particularly the relationship of fixed shifts and rotating shifts with burnout in critical care areas such as ICU, cardiac care unit (CCU) and emergency room (ER). Consequently, there is a recognized need for more research on specific shift working characteristics that have detrimental impacts on health,[17,19] burnout in particular.
Therefore, the purpose of this study was to determine the relationship between fixed and rotating shifts and burnout in a sample of critical care nurses working in critical care areas (including ICUs, CCUs, and ERs) in Isfahan, Iran.
MATERIALS AND METHODS
A retrospective cohort design was used to determine the relationship of fixed and rotating shifts with job burnout in nurses working in critical care areas in Isfahan in 2013. Rotating shift is considered as an exposed group, fixed shift as a non-exposed group, and burnout was considered as an outcome. A rotating shift consists of morning, evening, and night shifts altering during a month, and a fixed shift consists of fixed morning, fixed evening, or fixed night shifts alone during a month. Exposure time was considered to be at least 1 year in each shift working,[20] and critical care areas were defined as the ICU, CCU, and ER.
The total population of critical care nurses in six selected hospitals (15 ICUs, 6 CCUs, and 6 ERs) was 850 of whom 170 were chosen using quota and random sampling. With regard to the population of the study, the quota of each hospital was determined and divided into two equal groups (exposed and non-exposed). Then, through a random sampling, the subjects were selected within each group. Each group consisted of 85 subjects.
The inclusion criteria were being a critical care nurse and working in either rotating or fixed shift for at least 1 year in the studied units[21] (data were gathered from the records in nursing unit manager's office), having a BSc degree or above, not having more than one job, no history of special chronic diseases such as a mental disorder, severe headaches, or backaches, and not having taken sick leave for more than 1 month in the 6-month period before the study. Participation in the study was voluntary and based on the nurses’ ability to fill in and sign the informed consent. Participants were assured that all gathered data and information would be strictly confidential and would not be accessed by others without obtaining prior permission from them. Moreover, the participants had the right to withdraw at any time if they could not remember the past 1 year data to complete the questionnaire.
Two instruments were used for data collection. The first instrument was created by the authors, including demographic data such as sex, age group, marital status, education level, years of professional experience, hours of overtime working, shift schedules, and the related hospitals’ and wards’ names. The second instrument was the Maslach Burnout Inventory (MBI), version Human Services Survey (HSS), developed by Maslach and Jackson (1981) to assess the three dimensions of burnout.
The MBI-HSS consists of 22 items that measure burnout in terms of EE (nine items), DP (five items), and PA (eight items). It also has two scales: Frequency and intensity. Frequency is measured on a seven-point Likert's scale anchored by never (0) and every day (6). The scores thus can range from 0 to 54 on the EE subscale, from 0 to 30 on the DP subscale, and from 0 to 48 on the PA subscale. Intensity is measured on an eight-point Likert's scale anchored by barely noticeable (0) and very strong (7). The scores thus can range from 0 to 63 on the EE subscale, from 0 to 35 on the DP subscale, and from 0 to 56 on the PA subscale. Higher mean scores on the EE and DP subscales correspond to higher levels of burnout, whereas lower mean scores on the PA subscale correspond to higher levels of burnout.[22]
Total scores of each dimension were summed up and categorized as low, moderate, or high. In order to do so, high, moderate, and low scores were considered as ≥27, 17-26, and 0-16, respectively, in EE, ≥13, 7-12, and 0-6, respectively, in DP, and 0-31, 32-38, and ≥39, respectively, in personal performance.[23] The cutoff values indicating the presence of burnout were ≥27 for EE, ≥10 for DP, and ≤33 for PA, which was scored in the opposite direction.[24]
The MBI-HSS is a quantitative measure with established reliability and validity.[22] Internal consistency of the MBI-HSS was established and reported using Cronbach's alpha coefficient (N = 1316). The reported reliability for EE subscale was 0.90, DP subscale was 0.71, and for PA subscale was 0.79.[22] The employed questionnaire has been frequently assessed and confirmed to have a reliability of over 90% by Iranian researchers.[25]
All statistical analyses were performed with SPSS 21 software. Data are expressed as means (SD) or numbers and percentages. Independent t-test and logistic regression was performed to analyze the data and a P < 0.05 indicated significance.
RESULTS
The 85 subjects in the exposed group and 85 subjects in the non-exposed group who participated in the investigation did not differ significantly in demographic traits. The education level of 80 subjects (94.1%) was Bachelor's, and 41 (48.2%) were from ICU, 34 (40%) were from ER, and 10 were from (11.8%) CCU, which were the same in both groups. Chi-square test showed no significant difference in the distribution of sex and marital status in the two groups. With regard to sex, females formed the highest percentage in the both groups, with 52 (67.1%) and 51 (68.2%) in the exposed and non-exposed groups, respectively. With regard to marital status, married subjects formed the highest percentage, with 52 (61.2%) subjects in the exposed group and with 51 (60%) subjects in the non-exposed group.
Mann–Whitney test showed that the distribution of age group, work experiences, and working overtime remained insignificant in both groups. With regard to age group, the highest percentage of subjects were in 22-29 years age group with 38 (44.7%) in the exposed group and in 30-39 years age group with 44 (51.8%) in the non-exposed group. With regard to work experience, the highest percentage had 1-9 years of experience with 48 (56.5%) in the exposed group and 10-19 years of experience with 44 (51.8%) in the non-exposed group. With regard to overtime work, the highest percentage worked 1-49 h per month in both groups, with 54 (63.5%) in the exposed group and 61 (71.8%) in the non-exposed group. Analysis of the demographic data as mentioned above indicated that the two groups were matched which is ideal.
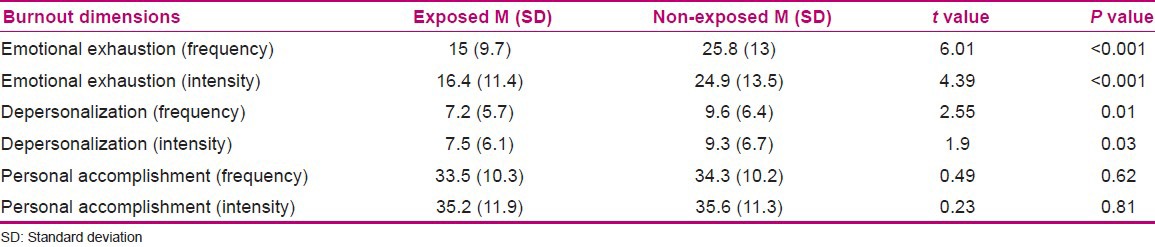
Independent t-test in the frequency scale of burnout dimensions indicated that the mean scores of EE (P < 0.001) and DP (P = 0.01) were significantly high in the non-exposed group, but the mean score of PA had no significant difference in the two groups [Table 1]. Independent t-test in the intensity scale of burnout dimensions revealed the same results as well [Table 1].
Table 1.
Mean scores of burnout dimensions in frequency and intensity scales in the two groups
With respect to the burnout cutoff values indicating the presence of burnout, it was observed that the burnout percentage in the exposed group was 12.9% in EE, 29.4% in DP, and 45.9% in PA, and in the non-exposed group was 60% in EE, 48.1% in DP, and 34.1% in PA.
Logistic regression analysis, using the cutoff values of burnout, showed that the non-exposed group (fixed shift schedule) was significantly associated with burnout in EE (odds ratio, 10.1; 95% confidence interval, 4.68-21.75) and DP dimensions (odds ratio, 2.2; 95% confidence interval, 1.19-4.21). In other words, the non-exposed group was 10.1 times more likely to be exposed to EE and 2.2 times more likely to be exposed to DP, in comparison with the exposed group [Table 2].
Table 2.
The results of logistic regression analysis for the relationship between two groups and three dimensions of burnout
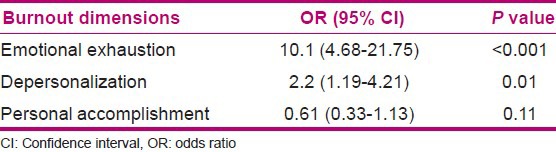
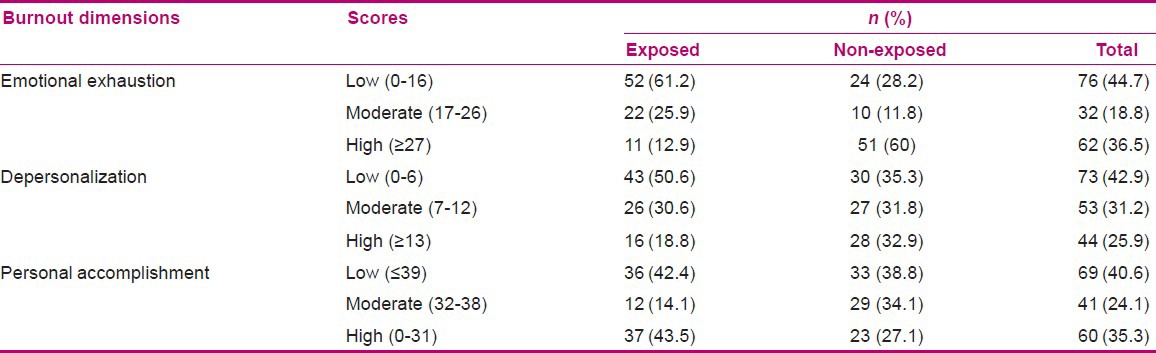
Table 3 indicates the frequency of low, moderate, and high levels of burnout in the two groups and the total number of participants in each level.
Table 3.
Frequency of burnout levels in the two groups
DISCUSSION
The present study reveals that nurses with a fixed shift schedule display more burnout compared to those with rotating shift schedule. Some studies have reported the same result,[16,26] while others reported the opposite.[27] No clear results were obtained with reference to shift work and burnout.[2] Since there is no consensus in the contemporary literature, further analyses are necessary.
The findings of this study show that the type of shift work had a significant relationship with burnout in critical care nurses. To be more precise, high level of burnout in EE and DP dimensions was significantly associated with fixed shift schedule. Although PA was high in fixed shift nurses compared with rotating shift nurses, independent t-test showed no significant differences between the two groups. On the contrary, other studies found rotating shift midwives had high scores of burnout in PA,[28] and the relationship between work pattern and EE and PA was found to be significant. Furthermore, PA level of nurses working in fixed day shifts was higher than the level of those working in fixed night shifts. Also EE level was higher in nurses who worked in fixed night shifts compared to those working in fixed day shifts and those working in rotating shifts.[16] Khazaei et al. found high level of EE and DP in fixed night shifts and high level of PA in fixed morning shifts,[26] which indicates high level of burnout in fixed shift schedules.
With regard to the mean scores in the two groups, the non-exposed group had moderate level of burnout in EE, DP, and PA and the exposed group had moderate level of burnout in DP and PA and low level in EE. Some studies found moderate level of EE and PA, which is consistent with our results, but low level of DP which is not in line with our results.[28,29]
High levels of burnout in the non-exposed group were 60%, 32.9%, and 27.1%, and in the exposed group were 12.9%, 18.8%, and 43.5% in EE, DP, and PA, respectively. Santos et al. observed high level of EE in 26.47%, DP in 26.47%, and PA in 29.41% of the responders,[30] while Pavlakis et al. observed high level of EE, DP, and PA in 21.5%, 33%, and 30.7% of participants, respectively.[31] In comparison with the studies mentioned above, EE and DP were much more frequently identified in the present study (in the non-exposed group), but PA was less frequent.
High level of burnout in fixed shift schedules in the present study, mainly fixed morning (42%) and fixed night shifts (39%), may be attributed to the fact that there are fewer nurses working at night and the ratio of nurses to patient is not appropriate.[12] Also, the time of 12 h allocated for night shift is too long. Furthermore, most of the attending visitations and interventions taking place in the morning shift result in a heavier workload than in other shifts. On the contrary, according to our observations, in rotational shifts, there are usually three shifts, namely morning, evening, and night shifts. Most rotational shifts are repetitive and do not require special skills to pass from one shift to another, and hence, they are interchangeable. There is tremendous convenience in this type of shift and provides the opportunity for additional inputs.
In order to maximize the relevance of these findings, we relied on the logistic regression to determine whether fixed and rotating shift nurses are at risk for burnout or not. Fixed shift nurses, who worked in mainly fixed morning (42%) and fixed night shifts (39%) in our study, had approximately 10.1 times the odds to expose to EE and 2.2 times the odds to expose to DP. On the contrary, rotating shift nurses had approximately 1.6 times the odds to expose to PA. Based upon the study findings, fixed shift nurses are generally a population at risk to burnout, and should be given special attention such as medical screening.
CONCLUSION
The results may offer useful information for nursing leaders. For example, with regard to the significant predictors obtained from the current analyses, rotating shift may be useful to reduce job burnout. However, literature reports have explained that there is no perfect schedule,[12] and recommendation should be pertinent to specific groups and work systems. It is to be noted that each setting has its own specific requirements. Literature reviews have also revealed the incongruousness in shift work research design and methodology, making comparison between studies intricate or even unachievable.[17] Experimental research would better reveal whether rotating shift schedule may help to reduce job burnout in critical care nurses. Further studies are required to find out more information, and the management will benefit with further research in this area.
ACKNOWLEDGEMENT
Our heartfelt thanks go out to critical care nurses for their participation and continued support in bringing this study into fruition.
Footnotes
Source of Support: Isfahan University of Medical Sciences. This article was derived from an MSc thesis in Isfahan University of Medical Sciences, No: 392011
Conflict of Interest: Nil.
REFERENCES
- 1.Garrosa E, Rainho C, Moreno-Jiménez B, Monteiro MJ. The relationship between job stressors, hardy personality, coping resources and burnout in a sample of nurses: A correlational study at two time points. Int J Nurs Stud. 2010;47:205–15. doi: 10.1016/j.ijnurstu.2009.05.014. [DOI] [PubMed] [Google Scholar]
- 2.Kedem Y, Bagan Y. Burnout and absenteeism among nurses in health care management. J Acad Bus Econ. 2005;5:93–112. [Google Scholar]
- 3.Jahanbakhsh GS, Omidi Arjenaki N, Nouri AA, Oreyzi H. The relationship of personality characteristics and burnout among nurses. Iran J Nurs Midwifery Res. 2009;14:190–4. [Google Scholar]
- 4.Maslach C, Leiter MP. Early predictors of job burnout and engagement. J Appl Psychol. 2008;93:498–512. doi: 10.1037/0021-9010.93.3.498. [DOI] [PubMed] [Google Scholar]
- 5.Hall E. Nurse burnout in a high stress health care environment: Prognosis better than expected? MSc. Univ Otago. 2005;5:36. [Google Scholar]
- 6.Poncet MC, Toullic P, Papazian L, Kentish-Barnes N, Timsit J-F, Pochard F, et al. Burnout syndrome in critical care nursing staff. Am J Respir Crit Care Med. 2007;175:698–704. doi: 10.1164/rccm.200606-806OC. [DOI] [PubMed] [Google Scholar]
- 7.Fall ML, Wolf KN, Schiller MR, Wilson SL. Dietetic technicians report low to moderate levels of burnout. J Am Diet Assoc. 2003;103:1520–2. doi: 10.1016/j.jada.2003.08.018. [DOI] [PubMed] [Google Scholar]
- 8.Embriaco N, Azoulay E, Barrau K, Kentish N, Pochard F, Loundou A, et al. High level of Burnout in intensivists prevalence and associated factors. Am J Respir Crit Care Med. 2007;175:686–92. doi: 10.1164/rccm.200608-1184OC. [DOI] [PubMed] [Google Scholar]
- 9.Bakker AB, Le Blanc PM, Schaufeli WB. Burnout contagion among intensive care nurses. J Adv Nurs. 2005;51:276–87. doi: 10.1111/j.1365-2648.2005.03494.x. [DOI] [PubMed] [Google Scholar]
- 10.Verdon M, Merlani P, Perneger T, Ricou B. Burnout in a surgical ICU team. Intensive Care Med. 2008;34:152–6. doi: 10.1007/s00134-007-0907-5. [DOI] [PubMed] [Google Scholar]
- 11.Kravits K, McAllister-Black R, Grant M, Kirk C. Self-care strategies for nurses: A psycho-educational intervention for stress reduction and the prevention of burnout. Appl Nurs Res. 2010;23:130–8. doi: 10.1016/j.apnr.2008.08.002. [DOI] [PubMed] [Google Scholar]
- 12.Abdalkader RH, Hayajneh FA. Effect of night shift on nurses working in intensive care units at Jordan University Hospital. Eur J Sci Res. 2008;23:70–86. [Google Scholar]
- 13.Natvik S, Bjorvatn B, Moen BE, Magerøy N, Sivertsen B, Pallesen S. Personality factors related to shift work tolerance in two-and three-shift workers. Appl Ergon. 2011;42:719–24. doi: 10.1016/j.apergo.2010.11.006. [DOI] [PubMed] [Google Scholar]
- 14.Wang X, Armstrong M, Cairns B, Key T, Travis R. Shift work and chronic disease: The epidemiological evidence. Occup Med (Lond) 2011;61:78–89. doi: 10.1093/occmed/kqr001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Knutsson A. Methodological aspects of shift-work research. Chronobiol Int. 2004;21:1037–47. doi: 10.1081/cbi-200038525. [DOI] [PubMed] [Google Scholar]
- 16.Demir A, Ulusoy M, Ulusoy M. Investigation of factors influencing burnout levels in the professional and private lives of nurses. Int J Nurs Stud. 2003;40:807. doi: 10.1016/s0020-7489(03)00077-4. [DOI] [PubMed] [Google Scholar]
- 17.Kantermann T, Juda M, Vetter C, Roenneberg T. Shift-work research: Where do we stand, where should we go? Sleep Biol Rhythms. 2010;8:95–105. [Google Scholar]
- 18.Al-Kandari F, Thomas D. Adverse nurse outcomes: Correlation to nurses’ workload, staffing, and shift rotation in Kuwaiti hospitals. Appl Nurs Res. 2008;21:139–46. doi: 10.1016/j.apnr.2006.10.008. [DOI] [PubMed] [Google Scholar]
- 19.Burch JB, Tom J, Zhai Y, Criswell L, Leo E, Ogoussan K. Shiftwork impacts and adaptation among health care workers. Occup Med (Lond) 2009;59:159–66. doi: 10.1093/occmed/kqp015. [DOI] [PubMed] [Google Scholar]
- 20.Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397–422. doi: 10.1146/annurev.psych.52.1.397. [DOI] [PubMed] [Google Scholar]
- 21.Hooper C, Craig J, Janvrin DR, Wetsel MA, Reimels E. Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J Emerg Nurs. 2010;36:420. doi: 10.1016/j.jen.2009.11.027. [DOI] [PubMed] [Google Scholar]
- 22.Maslach C, Jackson SE. 3rd ed. Palo Alto, Calif: Consulting Psychological Press; 1996. Maslach burnout inventory manual. [Google Scholar]
- 23.Peery AI. United States: North Carolina State University; 2006. Caring and Burnout in registered nurses: What's the connection? [Google Scholar]
- 24.Losa Iglesias ME, Becerro de Bengoa Vallejo R, Salvadores Fuentes P. The relationship between experiential avoidance and burnout syndrome in critical care nurses: A cross-sectional questionnaire survey. Int J Nurs Stud. 2010;47:30–7. doi: 10.1016/j.ijnurstu.2009.06.014. [DOI] [PubMed] [Google Scholar]
- 25.Savabi Esfahani M, Mirzaee M, Boroumandfar K, Abedi MR. Job burnout and its relation with personality traits among the midwives working in Isfahan, Iran. Iran J Nurs Midwifery Res. 2012;17:220–4. [PMC free article] [PubMed] [Google Scholar]
- 26.Khazaei T, Khazaei T, Sharif-Zadeh GR. Nurse burnout, and some related factors. Birjand Univ Med Sci. 2006;13:56–62. [Google Scholar]
- 27.Sotodeh AN, Bakhtiari A. Occupational exhaustion and its related factors in nurses and midwives of Semnan University of Medical Sciences Scientific. Sci J Kurdistan Univ Med Sci. 2006;11:77–83. [Google Scholar]
- 28.Mollart L, Skinner VM, Newing C, Foureur M. Factors that may influence midwives work-related stress and burnout. Women Birth. 2011;26:26–32. doi: 10.1016/j.wombi.2011.08.002. [DOI] [PubMed] [Google Scholar]
- 29.Kovács M, Kovács E, Hegedüs K. Emotion work and burnout: Cross-sectional study of nurses and physicians in Hungary. Croat Med J. 2010;51:432–42. doi: 10.3325/cmj.2010.51.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dos Santos FE, Alves JA, Rodrigues AB. Burnout syndrome in nurses in an Intensive Care Unit. Einstein. 2009;7:58–63. [Google Scholar]
- 31.Pavlakis A, Raftopoulos V, Theodorou M. Burnout syndrome in Cypriot physiotherapists: A national survey. BMC Health Serv Res. 2010;10:63. doi: 10.1186/1472-6963-10-63. [DOI] [PMC free article] [PubMed] [Google Scholar]