

Abstract
Background:
Quality of life is a concept, which in recent years is considered as a measure for health in chronic diseases such as kidney diseases. Complications of chronic diseases can affect the quality of life in children and their families over time. Therefore, empowerment programs are necessary to improve their quality of life. This study aimed to investigate the impact of the family empowerment model on the quality of life in children with chronic kidney diseases.
Materials and Methods:
This quasi-experimental study was conducted on 64 children with chronic kidney diseases and their families. The research tools included the questionnaire of demographic characteristics and the quality of life questionnaire 4th edition. After data collection in the first phase, the family empowerment model was implemented in the intervention group and the test was repeated after 1 month. For comparison of data between the two groups and within each group, independent t-test and paired t-test were used, respectively.
Results:
Independent t-test showed that the mean score of quality of life was not significantly different in the two groups before intervention. However, after intervention, the differences were significant. Paired t-test showed a significant difference in the quality of life before and after intervention in the study group.
Conclusions:
The findings showed that family empowerment model was effective in increasing the quality of life of children with chronic kidney diseases. Thus, we suggest this model to be used in inpatient and outpatient children's health care.
Keywords: Chronic kidney disease, family empowerment, quality of life
INTRODUCTION
Chronic diseases refer to the diseases which exist for a long period, usually more than 6 months, and often to the end of patients’ life.[1] Therefore, these diseases are expected to affect patients’ interactions with the physical and social environment they live in.[2] Chronic diseases include a vast range of heart diseases, respiratory diseases, asthma, and renal diseases. Among them, renal diseases, which lead to gradual dysfunction of kidneys for more than 3 months, are one of the major causes for mortality and morbidity in the world.[3]
Existing statistics show that the number of patients with chronic renal diseases is growing, such that 1.5 million patients out of all patients with chronic diseases have renal diseases.[4] The total population of patients with chronic renal diseases has been reported to be 16,000, and is predicted to grow by twofold by the end of year 2012.[5] There is no available statistics about children with chronic renal diseases in Iran. Chronic renal diseases, as a threatening condition for patients’ health and socioeconomic status, as well as their families and society,[3] can also change the children's and families’ quality of life (QOL).[6] Based on the World Health Organization (WHO) statement, QOL includes individuals’ perceptions from their life situation with regard to their culture, value system, goals, expectations, standards, and concerns.[7] Therefore, the point important in treatment of a chronic disease like renal disease is promotion of patients’ QOL, in addition to control of disease signs. Health and treatment team members can affect patients’ QOL through investigation of individuals’ health and its provision. They can also determine the negative impact of the disease on individuals’ QOL through measurement of QOL.[8] One of the ways to improve QOL in children with chronic diseases is empowerment of the families. Family empowerment includes the interaction of health professionals with the families, so that it causes a sense of control of families’ life and leads to achievement to positive changes in the direction of power, ability, and enhancement of skillsin families.[9]
Family empowerment is so important. The nature of renal diseases disturbs the unit of the family and leaves serious complications since children with renal diseases receive a major part of their treatment at home and study in usual schools. Unfortunately, despite there being numerous researches conducted concerning family-centered cares and family empowerment, these cares are not basically administered based on parents–nurses reciprocal interactions.[10]
In Iran, family-centered care and family empowerment do not seem to be administered, since what is done is just one-side decision, made and conducted by nurses and physicians.
The goal of nursing interventions in family empowerment is to improve the ability of family members so that they can come over the existing obstacles in health context. Chronic renal diseases disturb the unit of family and leave serious complications.
So, family empowerment can diminish hospitalization costs and number, improve physical and mental function, and reduce disease signs and school absenteeism of children with renal diseases. Researcher observations and experiences in various pediatric wards confirm that what these children's parents receive is unstructured and disorganized information given to them by the physicians and nurses at the time of discharge, which is often forgotten due to lack of repetition and the use of medical terms in this education after discharge. These families should live their life in peace and physical and mental health from the time their children’ chronic disease is diagnosed, and have the ability of decision-making and determination of priorities for their own needs as well as their children's. The parents’ skills should be confirmed by nurses, although the families are deprived of this right. Therefore, the researcher decided to investigate the effect of family empowerment on QOL of the children with chronic renal diseases, in order to suggest appropriate strategies for the promotion of their QOL.
MATERIALS AND METHODS
This was a quasi-experimental two-group two-step study conducted on 64 children with chronic renal diseases and their families in two groups of study and control after obtaining their parents’ written consent. Inclusion criteria were age 8-12 years, no history of kidney transplantation and end-stage renal diseases, children's and their families’ interest to attend the study, ability of reading and writing in at least one of the parents, ability to understand Persian, children not affected withany other chronic diseases, parents not working as members of health and treatment team, lack of mental and psychological problems, and ability to fill the questionnaire. The exclusion criteria were patients’ interest to stop cooperating in the study, events such as parents’ divorce, parents’ or brother's or sister's death, and change of address during the study. The offices of children's renal diseases sub-specialists were selected as the research environment. Data collection tools were the demographic characteristics questionnaire and the questionnaire of Core Ped QoL, version 4. This questionnaire includes 23 questions of which 8 are on physical function and 15 are on psychosocial function (5 on emotional function, 5 on social function, and 5 on school function). Persian version of core Ped QoL was confirmed by Masaeli (2009) with Cronbach's alpha of 0.89.[11] The questionnaire was filled by the child and his/her parents, and if needed, by one of the researchers in two stages of before and 1 month after the last family empowerment session in the study and control groups in identical time points. Researcher, with agreement of the subjects, held needs assessment sessions of the study group in a building near one of the offices of children's renal diseases sub-specialists, and after detection of resources, limitations, needs, and weak points of the children and their parents, designed the content of empowerment program. Then, family empowerment model was held based on its steps and stages in six 45-min sessions, according to children's needs and tolerance. Three group discussion sessions were held for the parents too. Control group received no intervention. Family empowerment model contains four steps that are discussed below.
First step (knowledge increase)
The level of knowledge was improved in educational sessions through use of educational assistive materials such as Power Point, model, poster, group discussion methods, question and answer, lecture, and presentation. The subjects were assigned to 3-5 member groups based on their disease and received educational contents in a total of six 45-min sessions (four sessions of theory and two sessions of practical presentation) as follows.
In the first session physiology and anatomy of kidney, the children introduced themselves, and then, the general and behavioral goals, the evaluation method, and the duties of the subjects in educational sessions were explained by the researcher.
In the second session, the researcher explained the cause, signs, complications, and prognosis. In the third session, nutrition and laboratory tests and their normal values were explained. In the fourth session, medication was discussed with the children. For instance, the researcher explained the effect on nutrition on the disease. Then, the participants started discussing about it, based on their experiences, and the researcher conducted the session. Length of each session, based on children's desire, was decided to be 45 min. At the end of each session, the given materials were finalized and the questions were answered, and finally, the data and goal of the next session were determined. In each session, two questions were asked to the children in relation with the subjects of former sessions to evaluate the level of their learning.
Second step (improvement of self-efficacy)
To increase self-efficacy, two educational sessions were held by the practical presentation method. It was such that after explanation of each skill of weight and BP measurement, the skill was practically presented and taught to the children as follows:
Firstly, the researcher explained to the children about the related skill and its importance, the complications that arise due to lack of its control, and normal values of these measurements
The researcher presented the ultimate procedure of the skill in front of the children
Then, she divided the skill into more detailed components(for instance, concerning weight measurement, voiding before weight measurement, weight control after getting up in the morning, wearing identical clothes, tuning the scale's gage, standing on the scales with no vertical pressure, and holding nothing during measurement)
The children were asked to do the task
The children were given a chance to get skillful by practice and repetition of the skill to be able to do it
The children were asked to obtain self-efficacy in other components of the skill through practice and repetition to be able to do it without researcher's attendance
Finally, the children got completely self-efficient in the skill
Children's learning and the feeling of learning, as well as the ability of measurement and the feeling of capability resulted in their encouragement and increased self-esteem.
Third step (increase of self-esteem through educational participation)
At this stage, the children were asked to participate in their parents’ education concerning recognition of chronic disease-related issues and encourage their parents to help them. They transferred all they had learned in each group discussion session as well as all through observation in self-efficacy sessions to their parents. At this stage, the educational card of each session was given to the children and they were asked to pass the card to their parents to study. Parents wrote down their questions in this regard on a piece of paper after studying the card, concerning what they had learned from their children. If the parents were not interested in writing down the materials, they orally expressed their questions and their children wrote them down to be delivered to the researcher or to be discussed in the next session. In cases where the parents did not get self-efficient through their children's education and by studying the educational card, they were invited to discuss the disease trend, nutrition, physical activity, medication, and disease complications with the researcher during three 45-min educational sessions. Two weeks after holding the last session, phone calls were made to the subjects by the researcher to follow-up the skills and to be assured about application of the presented materials. In case of any further questions, researcher's phone number was given to the subjects for clarification.
Fourth step (process evaluation)
In empowerment-related sessions, an evaluation was made.
In order to evaluate the knowledge at the beginning of each session, two oral questions were asked to the children from the previous sessions. Self-efficacy evaluation was conducted by asking the children to represent two related skills correctly and their self-confidence and cooperation in education was evaluated in the form of returning the educational card related to their parents’ notes.
Final evaluation
One month after the last empowerment session held in the study group, core Ped QoL inventory was given to the study and control groups. Data were analyzed by descriptive and analytical statistics (Chi-square, paired t-test, independent t-test) through SPSS.
RESULTS
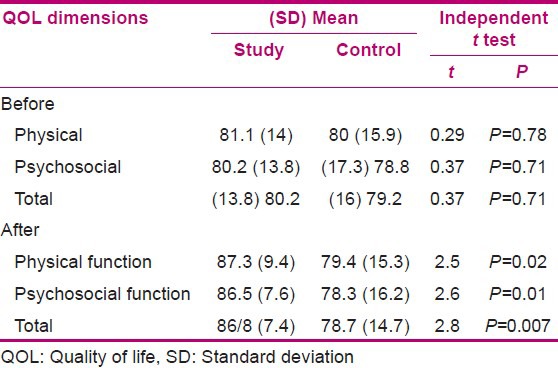
In the present study, frequency distribution of the children's education, location of residence, father's education, mother's education, father's occupation, and mother's occupation were identical [Table 1]. Subjects’ mean ages were 9.8 years and 10 years in the study and control groups, respectively. The mean lengths of disease were 5 years and 4.4 years and the mean ages of disease diagnosis were 5 years and 5.4 years in the study and control groups, respectively. Results showed no significant difference in the mean scores of QOL in the physical (P = 0.78) and psychosocial (P = 0.71) dimensions and the total score of QOL (P = 0.71) before intervention, but this difference was significant after intervention in physical (P = 0.02) and psychosocial (P = 0.01) dimensions and the total score of QOL (P = 0.007) in the study and control groups [Table 2]. There was also a significant difference in the mean scores of QOL in physical (P = 0.02) and psychosocial (P = 0.03) dimensions and the total QOL score (P = 0.02) after intervention, but this difference was not significant in the control group in physical (P = 0.81) and psychosocial (P = 0.81) dimensions and the total score of QOL (P = 0.79) [Table 2]. Results showed that the mean scores (standard deviation) of QOL in physical, psychosocial dimensions, and the total score of QOL were 81.1 (14), 80.2 (13.8), and 80.5 (12.3), respectively, before intervention and 87.3 (9.4), 86.5 (7.6) and 86.8 (7.4), respectively, after intervention. Paired t-test showed a significant difference before and after intervention. This difference was not significant in the control group.
Table 1.
Demographic characteristics of the subjects in the study and control groups
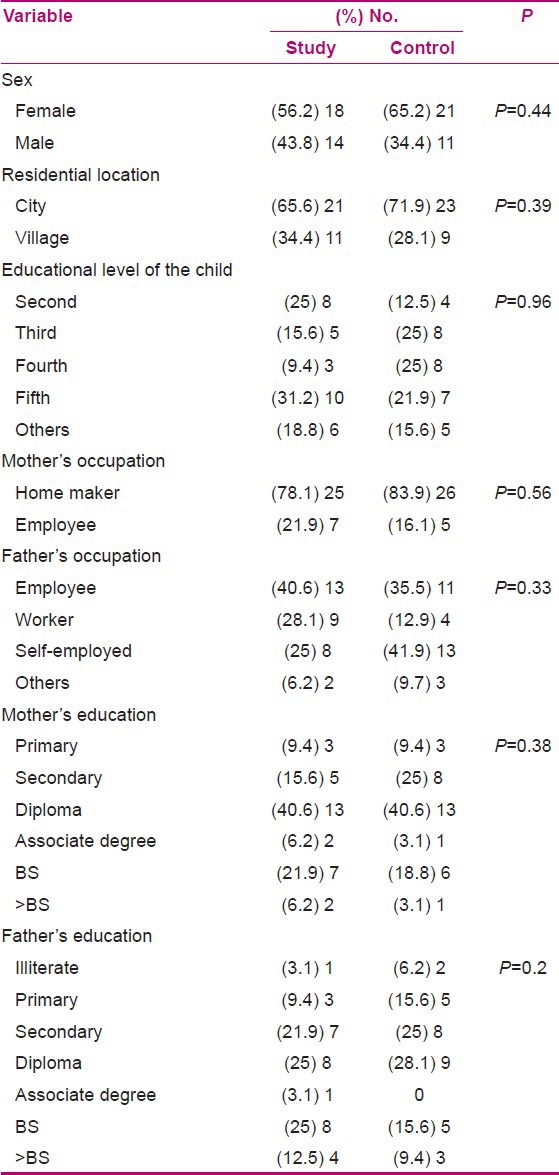
Table 2.
Mean and SD of children's QOL dimensions scores before and after intervention in the study and control groups
DISCUSSION
Independent t-test showed no significant difference in the mean total scores of QOL before intervention in the two groups, but the difference was significant after intervention. Teimori et al. (2011), in a study to define the effect of family-centered empowerment on QOL of the children with asthma, showed a significant difference in the children's total scores of QOL before and after intervention in the study and control groups.[12]
Allahyari et al., in a study on the effect of family empowerment model based on the of school-age children with thalassemia, showed a significant difference in the total scores of children's general QOL before and after intervention in the study and control groups,[13] which is consistent with our findings. Independent t-test showed no significant difference in QOL in the physical dimension means scores between the two groups before intervention, but the difference was significant after intervention. Yao et al. (2011) showed no significant difference in the QOL in children with vesicoureteral reflux in physical dimension compared to healthy children (P = 0.9999).[14] Buyan et al. (2009), in a study on QOL in children with a chronic kidney disease, showed no significant difference in QOL in the physical dimension between the study and control groups.[15] Marciano et al. showed that QOL score in the physical dimension was significantly lower in children with chronic renal diseases compared to healthy children.[16] Our obtained results are not in line with the results of previous studies. One of the reasons for the significant difference in the QOL score in physical dimension is that in our study, two identical groups of patients were compared, and on the other hand, it was an interventional study, whereas Yao et al. and Buyan et al. compared the QOL of healthy and diseased children in a descriptive study. In the present study, independent t-test showed no significant difference in the QOL mean scores in psychosocial dimension before intervention in the study and control groups, but the difference was significant after intervention. Mary Banacg et al. (2010), in a study on family empowerment in stress management and children's autism diagnosis acceptance, showed a significant difference in the empowerment of supportive systems after intervention[17] (P > 0.000). Marciano et al. (2011), in their study on behavioral disorders and low QOL in children and adolescents with chronic kidney diseases, showed that the QOL score in psychosocial dimension in these children was significantly lower, compared to that of healthy children[16] (P = 0.0001). Graves and Shelton, in a study on the effect of family empowerment on improvement of behavioral disorders in children, showed that these disorders were significantly different before and after intervention,[18] which is consistent with the above-mentioned studies. Paired t-test results presented in Table 2 show a significant difference in the QOL scores in physical and psychosocial dimensions and the total score of QOL in the study group before and after intervention, but the difference in the control group was not significant.
CONCLUSION
As the results showed, administration of family empowerment model can increase the QOL of children of age 8-12 years with chronic renal diseases. It is suggested to conduct further study in other age groups and for other chronic diseases.
ACKNOWLEDGMENTS
The researchers of this study want to thank the Research Center of the Faculty of Nursing and Midwifery of Isfahan University of Medical Sciences, collaborators, and diabetic participants for their cooperation.
Footnotes
Source of Support: Grant No. 391138
Conflict of Interest: Nil.
REFERENCES
- 1.Berman A, Snyder SL J, Kozier B, Genora Erb. 8th ed. USA: Pearson; 2007. Fundamentals of Nursing. [Google Scholar]
- 2.Aghvamy M, Mohammadzadeh SH, Gallalmanesh M2, Zare R. Assessment the education compariment to two ways: Group education and computer education on quality of life in the children 8-12 Years Suffering from Asthma in the Valiasr Hospital of Zanjan. ZUMS J. 2011;19:78–85. [Google Scholar]
- 3.Behrman RE, Kligman RM, Stanton BF, Schor MF, Geme JW. 19th ed. Philadelphia: Elsevier: Saunders; 2011. Nelson text book of pediatrics. [Google Scholar]
- 4.Cohen SD, Sharama T, Acquaviva K, Peterson RA, Patel SS, Kimmel PL. Washington: National Foundation Inc; 2007. Social support and Chronic Kidney Disease: An Update. [DOI] [PubMed] [Google Scholar]
- 5.Rambod M, Rafii F, Shirazi MK, Ghodsbin F, Heydari ST. Compasion of the quality of life in eldery with young and middle age chronic renal failure patiens. Salmand. 2011;6:52–8. [Google Scholar]
- 6.Woodgate RL. Life is never the same: Childhood cancer narratives. Eur J Cancer Care (Engl) 2006:158–18. doi: 10.1111/j.1365-2354.2005.00614.x. [DOI] [PubMed] [Google Scholar]
- 7.Pakpour HA A, Panahi CH D, Yekaninejad M, Ebadi Fard Azar F, Izy H. A comparative study on health related quality of life in hemodialysis patients and healthy people. Healt maagement. 2006;9:55–62. [Google Scholar]
- 8.Heydari M, Alhani F, Kazemnazhad A, Moazi F. The effect of empowerment model on quality of life in adolescents with diabetes. Iran J Pediatr. 2007;17:87–94. [Google Scholar]
- 9.Christensen BL, Kokckrow EO. 5th ed. Philadelphia: Mosbey; 2006. Foundations and adulth health nursing. [Google Scholar]
- 10.Jolly J, Shields L. The evolution of family- center care. J Pediatr Nurs. 2009;24:164–70. doi: 10.1016/j.pedn.2008.03.010. [DOI] [PubMed] [Google Scholar]
- 11.Ali M. Doctorin's Thesis. Iran: Isfahan University of Medical Sciences; Realated of health related quality of life on paracilinc results in patients under age 18 years old with Chronic Kidney Disease in Alzahra hospital. [Google Scholar]
- 12.Teimori F, Alhani F, Kazemnazhad A. The effect of family-centered empowerment model on the quality of life of school- age Asthma children. Nurs Re. 2010;6:52–63. [Google Scholar]
- 13.Allahyari I, Alhani F, Kazemnezhad A, Izadyar M. The effect of family empowerment model-based on the quality of life of school-age children with thalassemia. Iran J Pediatr. 2006;4:455–61. [Google Scholar]
- 14.Yao DF, Weinberg AC, Penna FJ, Huang L, Freilich DA, Minnillo BJ, et al. Quality of life in children with vesicoureteral reflux as perceived by children and parents. J Pediatr Urol. 2011;7:261–5. doi: 10.1016/j.jpurol.2011.02.026. [DOI] [PubMed] [Google Scholar]
- 15.Buyan N, Turkmen MA, Bilg H, Baskin E, Haberal M, Bilginer Y, et al. Quality of life in children with chronic kidney disease. Pediatr Nephrol. 2010;25:1487–96. doi: 10.1007/s00467-010-1486-1. [DOI] [PubMed] [Google Scholar]
- 16.Marciano RC, Soares CM, Diniz JS, Lima EM, Silva JM, Canhestro MR, et al. Behavioral disorders and low quality of life in children and adolescents with chronic kidney disease. Pediatr Nephrol. 2011;6:281–90. doi: 10.1007/s00467-010-1683-y. [DOI] [PubMed] [Google Scholar]
- 17.Banach M, Iudice J, Conway L, Couse LJ. Family Support and Empowerment: Post Autism Diagnosis Support Group for Parents. Routledge. 2010;33:69–83. [Google Scholar]
- 18.Graves KN, Shelton TL. Family empowerment as a mediator between family centered systems of care and changes in child functioning: Identifying an important mechanism of change. J Child Fam Stud. 2007;16:556–66. [Google Scholar]