

Abstract
BACKGROUND:
Acupuncture has been used as a treatment for cognitive impairment.
OBJECTIVE:
This review assesses clinical evidence for or against acupuncture as a treatment for cognitive impairment. This review also discusses the proposed mechanism(s) that could link acupuncture to improved cognitive function.
METHODS:
We searched the literature using PolyUone search from its inception to January 2013, with full text available and language limited to English. Levels of evidence were examined using Oxford Centre for Evidence-based Medicine–Levels of Evidence (March, 2009).
RESULTS:
Twelve studies met the inclusion criteria: 3 human studies and 9 animal studies. Levels of evidence ranged from level 1b to level 5.
CONCLUSION:
Most animal studies demonstrated a positive effect of acupuncture on cognitive impairment. However, the results of human studies were inconsistent. Further high-quality human studies with greater statistical power are needed to determine the effectiveness of acupuncture and an optimal protocol.
Keywords: neural regeneration, dementia, acupuncture, electroacupuncture, learning, cognitive, cognition, memory, neuroregeneration
Research Highlights
(1) This is a systematic review on 12 selected papers out of 227 to study acupuncture for cognitive impairment in human and animals.
(2) The results of acupuncture protocols are variable, although a number of individual studies reported positive effects on cognitive function.
(3) Further high-quality research is needed to determine the effectiveness of acupuncture and an optimal protocols.
INTRODUCTION
Cognitive impairments prevail among neurologic disorders. More than 60% of people experienced cognitive deficits after stroke[1]. 29% of patients with Parkinson's disease also met the criteria of dementia[2]. Cognitive impairment reduces the quality of life of patients, mainly because it affects mood and memory. Functional limitation due to cognitive impairment can also decrease quality of life. Study suggests that poor cognitive functioning is associated with reduced functional independence, social participation, depressive mood, and life satisfaction 1 year post stroke[3]. According to the World Health Organization, the number of people with dementia will continue to grow. The total population with dementia worldwide in 2010 was estimated to be 35.6 million and was projected to nearly double every 20 years[4]. The total estimated worldwide costs of dementia were US$604 billion in 2010[4]. It does create a serious financial burden on the society. Since treatment for cognitive impairment has not been well developed, some clinicians have suggested that acupuncture could be an alternative treatment of cognitive impairment.
Acupuncture is an alternative medicine methodology that originated in ancient China. It is an important part of Chinese medicine that involves the insertion of fine, solid needles into acupuncture points in the skin. According to traditional Chinese medicine, stimulating these points could correct imbalances of the flow of Qi through meridians[5].
There are many different ways to practice acupuncture. In this review, we will focus on traditional acupuncture where needles were inserted into the body according to traditional Chinese medicine framework[6] and electro acupuncture involved passing a pulsed current through the body tissues via acupuncture needles.
Acupuncture has become more popular not only in China but also in other foreign countries. Acupuncture has been claimed to be effective for a wide range of conditions, such as pain, musculoskeletal disorders and several neurologic diseases[7]. However, its use for cognitive diseases has been much less emphasized.
In order to justify the efficacy and make recommendations regarding acupuncture treatment for cognitive impairment, we conducted a review that summarizes the evidence from previous studies on this topic.
DATA AND METHODS
Search strategy
The following electronic databases were searched: PolyUone search included SciVerse ScienceDirect (Elsevier), MEDLINE (NLM), OneFile (GALE), Health Reference Center Academic (Gale), SpringerLink, American Psychological Association (APA), PMC (PubMed Central), Oxford Journals (Oxford University Press), Hindawi Journals, Sage Publications (CrossRef), Bentham Science (IngentaConnect), PLoS; and the following keywords were used: acupuncture, cognition, cognitive, dementia, Alzheimer's disease, memory.
Inclusion criteria
Two independent reviewers were responsible for data retrieval and quality evaluation.
Types of publication: All randomized controlled trials, randomized crossover trials and controlled trials that measured at least 1 cognitive domain. Only English articles were included. No publication date limits were set, and the search was completed in January 2013.
Participants: Human or animal studies on cognitive impairment were included.
Interventions: We included trials in which there was a comparison between a treatment group that received acupuncture with/without combined treatment, and a control or comparison group that received either an alternative form of intervention or no treatment.
Outcomes: The outcome measure of interest was cognitive function. This included any neuropsychological test designed to detect a change in cognitive function in any domain; for example, memory, learning or the Mini-Mental State Examination.
Published articles that did not meet the inclusion criteria were excluded using titles, abstracts and full text as appropriate.
RESULTS
Identification and selection of studies
A total of 227 articles were identified from searches performed in January 2013. Eighty-two articles were duplicated and 96 were excluded due to irrelevance to acupuncture and/or cognition, leaving 49 articles for further evaluation. Thirty-three of them were not experimental trials. Four remaining studies did not meet the inclusion criteria, because they did not have cognitive outcome measurements. In the end, 12 studies were included in this review. Three studies were human trials, while other nine studies used animals (Figure 1).
Figure 1.
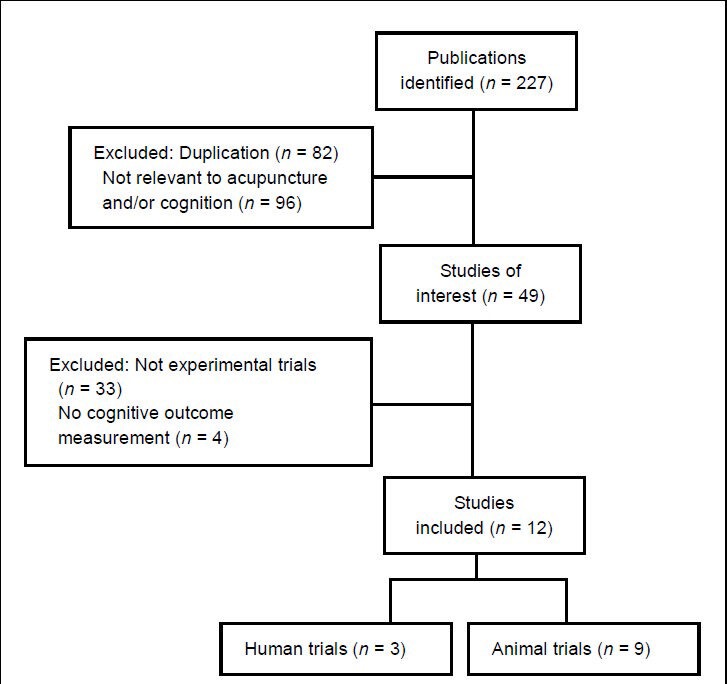
Flow chart of the literature selection process.
Description of studies
Level of evidence
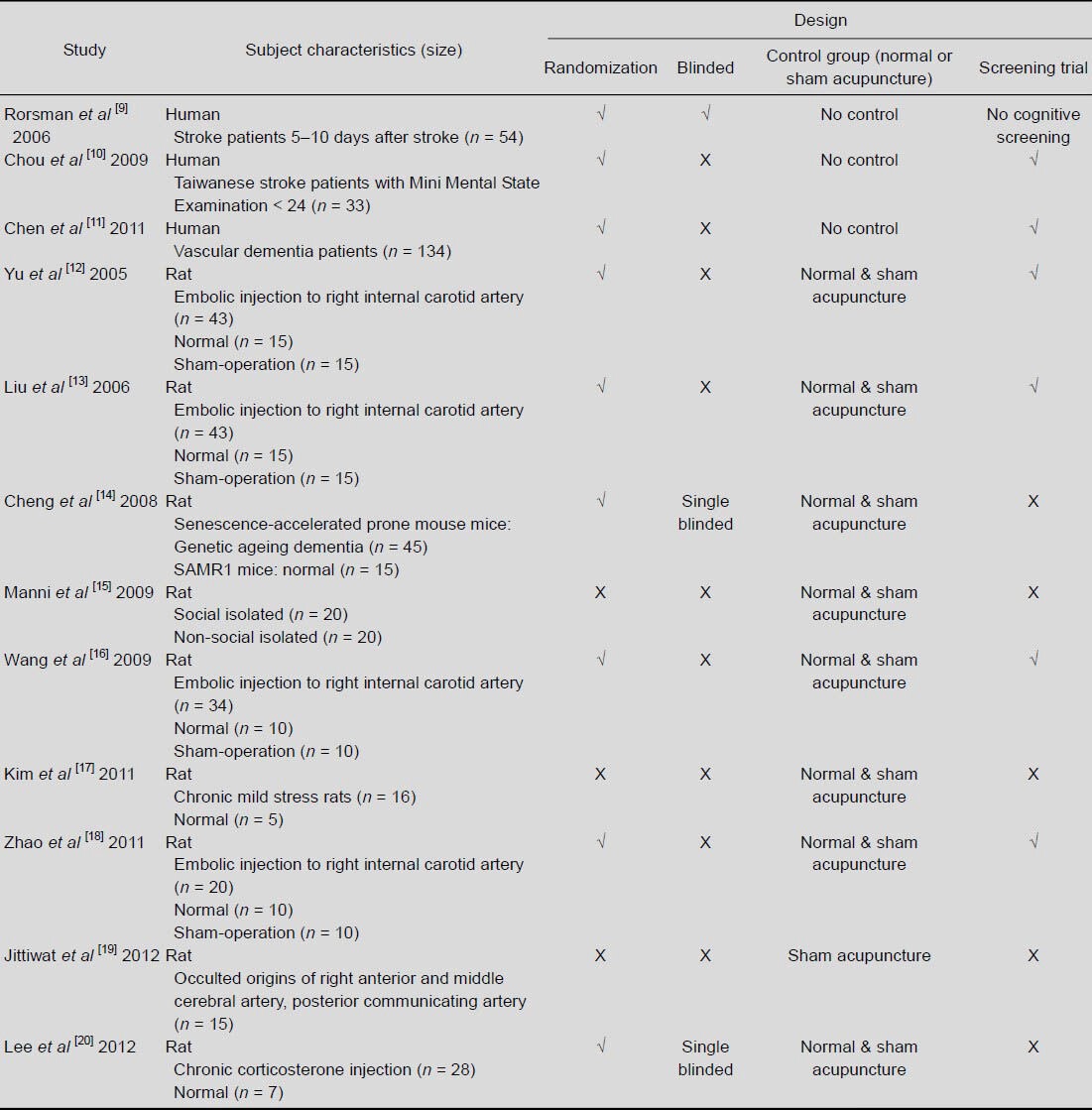
Studies were classified by Oxford Centre for Evidence-based Medicine–Levels of Evidence (March 2009)[8]. Among human trials, Rorsman and Johansson[9] was classified as level 1b evidence, Chou and colleagues[10] as level 2b evidence and Chen et al[11] as level 4 evidence. All the animal studies selected were classified as level 5[12,13,14,15,16,17,18,19,20] (Table 1).
Table 1.
Study design
Participants
A total of 105 subjects received acupuncture treatment across the 3 studies using human as subjects[9,10,11]. A further 116 subjects acted as control or received other treatment besides acupuncture. One hundred and sixty-seven subjects were between 59 and 90 years old and with Mini Mental State Examination scores less than 24[9,10]. There were 87 subjects with stroke, 33 subjects with stroke onset from 13 to 33 months[9] and 54 subjects were treated 5 to 10 days after stroke[11]. A total of 134 vascular dementia subjects with illness course ranging from 1 to 7 years were also included[10] (Table 2).
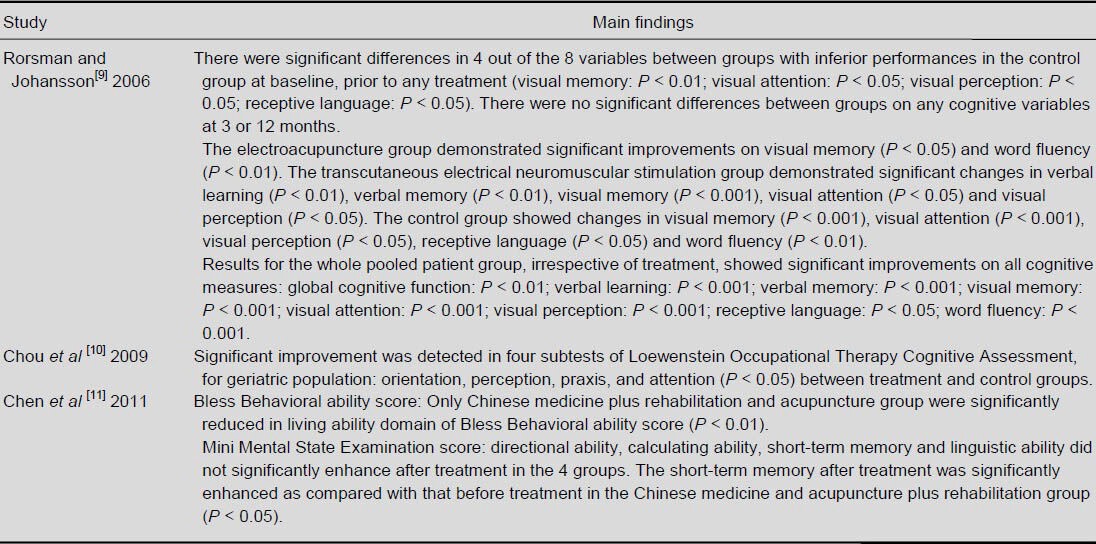
Table 2.
Major findings of human studies
A total of 421 rats (rats which died or screened out in any cognitive impairment check after surgeries were excluded) were used in studies[12,13,14,15,16,17,18,19,20]. In order to prepare cognitive impaired subjects, 150 rats had been injected a clot into the internal carotid artery[12,13,16,18]. Forty-five senescence-accelerated prone mouse rats were used[14]. Twenty rats were isolated[15]. Sixteen rats were under chronic mild stress[17]. The origin of the cerebral arteries of 15 rats were occulted[19] or 28 were induced with cognitive impairment by chronic injection of corticosterone[20]. A total of 117 rats had acupuncture treatment, whereas 304 rats acted as control or received other treatments.
Three clinical and nine animal studies examined the effect of acupuncture on human and rats, respectively. No adverse effects were reported after treatment.
Intervention
Acupuncture stimulation was applied using a variety of acupoints, needle stimulation and frequency setting. Selected acupoints included LI4, LI11, GV20, ST36, ST40, GB34, EX36:1, EX28:2, (1 study)[9], PC6, HT7 (1 study)[10], GV20, GV16, GB20, EX-HN5, LI4, LR3, EX-HN1, EX-HN3 (1 study)[11], “Yiqitiaoxue, fubenpeiyuan” acupuncture method CV17, CV12, CV6, ST36, SP10 (5 studies)[12,13,14,16,18], ST36 (1 study)[15], PC6 vs. TE5 (1 study)[17], GV20 (1 study)[19], HT7 vs. TE5 (1 study)[20]. Needle stimulation was either made by manual twisting or electrical stimulation. Control intervention consisted of needle insertion to a non-acupoint. Treatment duration ranged from 30 to 180 seconds for each acupoint (manual twisting)[12,17]; 20 to 30 minutes for each acupoint (electrical stimulation)[10,15], ranged from 2 sessions a week to 6 sessions a week[10,12]. The total session number ranged from 4 to 36[11,15].
Outcome measurements
In the human studies, cognitive function which was the primary outcome was measured by Loewenstein Occupational Therapy Cognitive Assessment, for geriatric population[10], Mini Mental State Examination[9,11] and Bless Behavioral ability[11] were used. Other cognitive functional aspects were measured, including verbal learning and memory by Rey Auditory Verbal Learning Test, visual memory by Facial Recognition Memory, visual attention by Star Cancellation Test, visual perception by Time Perception, receptive language by Token test and word fluency by Fast Application Switching[9]. Secondary outcome was quality of life, which was assessed by SF-36 questionnaire and Stroke-Specific Quality of Life Scale[11].
For the animal studies, the learning ability and memory aspects of cognitive function were assessed using Morris Water Maze test, which included hidden platform trial[12,13,14,16,18,19,20], probe trial[12,13,14,16,20] and reversal trial[12,13,14,16] and visible platform trial[12,13,14,16,20], and passive avoidance task[15,17] (Tables 3 and 4).
Table 3.
Major findings of rats studies (Morris Water Maze Test)
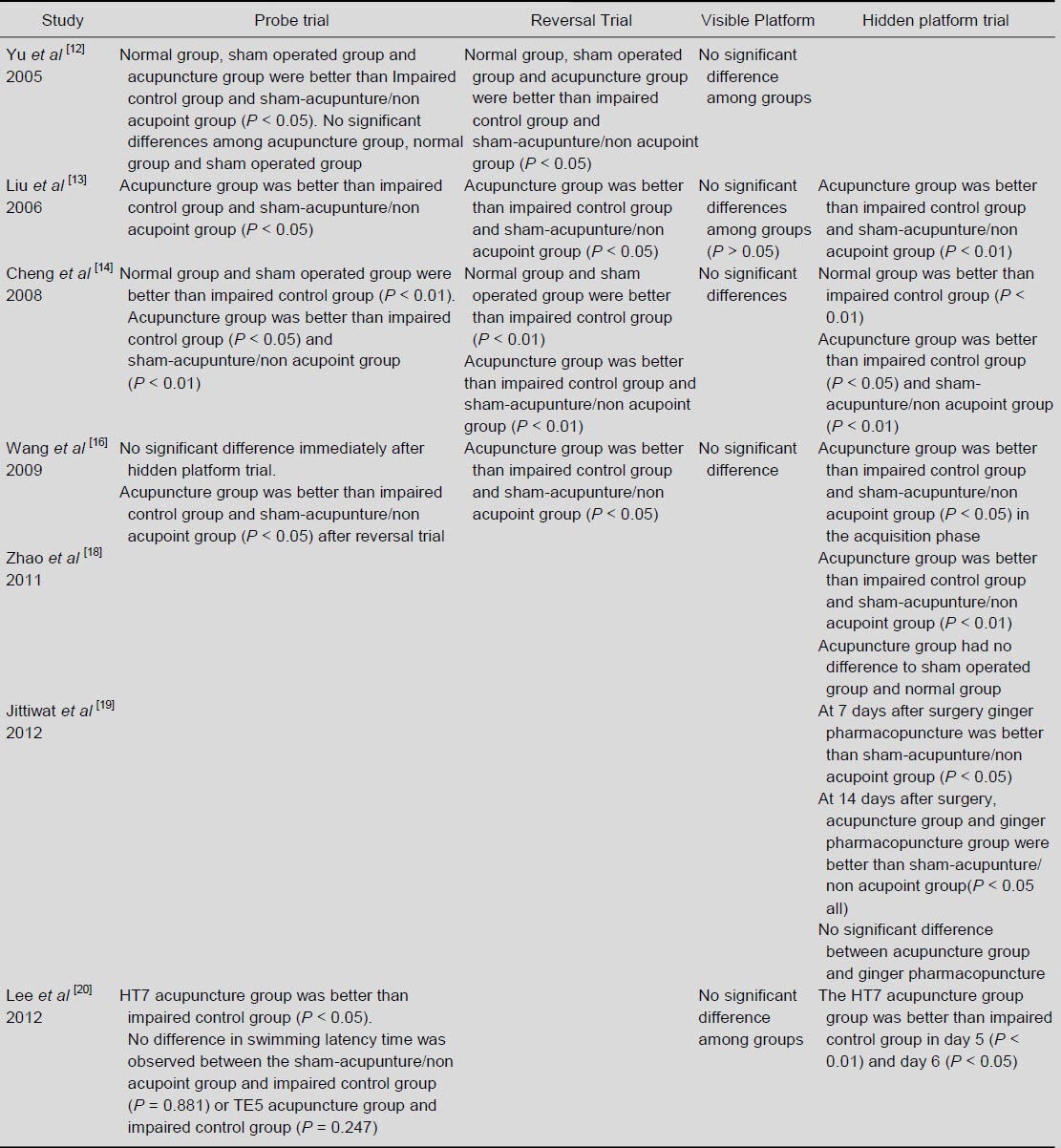
Table 4.
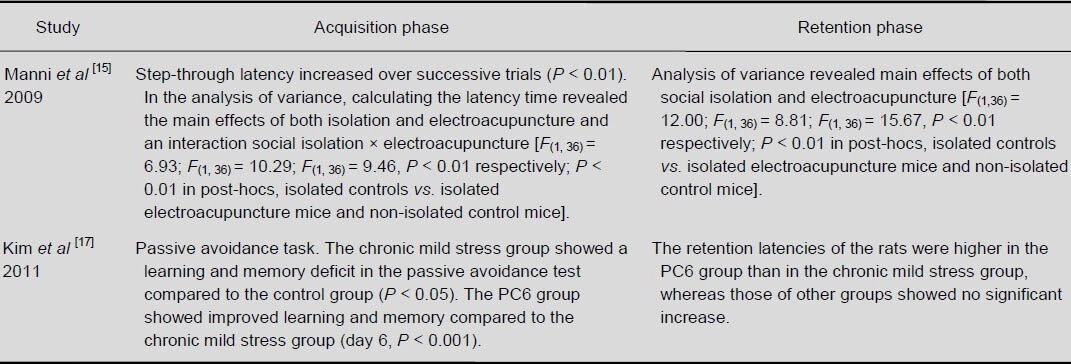
Major findings of rats studies (passive avoidance)
Enzyme activities of superoxide dismutase[13,19], catalase[13,19], glutathione peroxidase[13,19], nerve growth factor[15], brain-derived neurotrophic factor[15], acetylcholinesterase[17,20], hexokinase[18], pyruvate kinase[18], glucose-6-phosphate dehydrogenase[18], choline acetyltransferase[20] and expression of copper-zinc superoxide dismutase mRNA and its protein[13], Bcl-2 protein[16], Bax protein[16], lipid peroxidation product, malondialdehyde[19] in brain, brain cell proliferation[14] and nerve cell apoptosis[16] were measured for investigating the mechanisms by which acupuncture improved cognitive function.
DISCUSSION
Effect of acupuncture on cognition of human subjects
Electroacupuncture could improve Loewenstein Occupational Therapy Cognitive Assessment, for geriatric population: orientation, perception, praxis, and attention in patients with stroke.
Also, Chinese medicine plus rehabilitation and acupuncture could improve vascular dementia patients’ Bless Behavioral ability (Bless behavior score) and Mini Mental State Examination[9,10].
Effect of acupuncture on cognitive function for dementia rats
Nine studies[12,13,14,15,16,17,18,19,20] examined the effect of acupuncture on cognitive deficit induced by surgical emboli injection, social isolation, genetic pre-exposure, chronic mild stress and chronic injection of corticosterone of rats separately. Acupuncture was shown to have a significant beneficial effect on cognitive function, including learning or relearning ability and memory in all animal studies[12,13,14,15,16,17,18,19,20]. They were measured by Morris Water Maze test including all types of trial mentioned before[12,13,15,17,18,19,20] and passive avoidance task[14,16].
However, due to some limitations mentioned in these studies, this effect might be subjected to some biases.
General limitations of literature included
Human studies
There were only three human studies included in this review out of 12 published[9,10,11]. Among the three selected studies, two studies had a small sample size, less than 20 subjects per group[9,10]. None of them had justified the choice of sample size. Three studies were randomized, but methods of randomization were not stated. One study did not blind the tester[11]. The results might be subjected to bias of tester. Three studies only investigated the combined effect of acupuncture with conventional rehabilitation or Chinese medicine, no exact control group received no treatment and no treatment group received acupuncture alone[9,10,11]. Two studies did not have follow-up assessment[10,11]. The long lasting effect of acupuncture could not be justified.
Rat studies
There were nine rat studies selected for our review[12,13,14,15,16,17,18,19,20]. Even when the studies were well designed, animal studies were considered at level five of evidence which is the lowest. In fact, there were some limitations in these animal studies[12,13,14,15,16,17,18,19,20]. Six studies had 10–15 rats in each group[12,13,14,15,16,18]. Three studies had 5–10 rats in each group[17,19,20]. None of them had justified the choice of sample size.
Six studies stated they had allocated the rats randomly, but none of them stated the method of randomization[12,13,14,16,18,20]. Seven studies did not blind the tester[12,13,15,16,17,18,19]. The results might be subjected to bias of tester. All studies had an impaired treatment group receiving only acupuncture, and an impaired control group receiving no or sham treatment[12,13,14,15,16,17,18,19,20]. It was good to demonstrate the effect of acupuncture. Eight studies included a normal control group[12,13,14,15,16,17,18,20]. It was useful to exhibit the magnitude of recovery due to acupuncture treatment effect. Five studies did not conduct a screening trial to confirm that there were cognitive impairments in the rats[14,15,17,19,20].
The results might be affected by inclusion of some of the rats which did not suffer from cognitive impairment after surgery or other procedures. Four studies did not conduct a visible platform trial or open field test to exclude the effect of motor deficit or motivation problem as a result of Morris Water Maze or passive avoidance test[12,14,16,20].
There was no follow up in any of the rat studies[12,13,14,15,16,17,18,19,20]; hence it was not possible to evaluate the long lasting effect of acupuncture.
Since the treatment protocols and causes of cognitive impairment varied, it remains difficult to suggest an optimal protocol and indication.
Mechanism of acupuncture effect of cognitive impairment
Acetylcholinesterase and choline acetyltransferase
Previous studies had shown that the most profound change in patients with Alzheimer's disease was a progressive reduction in the activity of acetylcholinesterase in the neocortex and hippocampus compared with normal subjects[21,22]. Also, choline acetyltransferase activity was highly correlated with the severity of dementia across the neocortex of the Alzheimer's disease cases[21]. Therefore, it was generally accepted that the cellular loss and dysfunction of cholinergic neurons result in development of dementia in Alzheimer's disease[23].
In this review, two studies investigated the effect of acupuncture on acetylcholinesterase activity in the hippocampus. One study found that the acetylcholinesterase reactivity in the hippocampus of a chronic mild stress group of rats was significantly lower than that of the controls (P < 0.000 1), and acupuncture at PC6 could increase the acetylcholinesterase reactivity in both hippocampal CA1 (P < 0.05) and CA3 (P < 0.05) in chronic mild stress group. Learning and memory ability of the rats were tested by passive avoidance task, and the PC6 acupuncture group showed improvement in learning and memory compared to the chronic mild stress group (P < 0.001)[17]. Another study found that acetylcholinesterase reactivity in the hippocampal CA1 due to chronic exposure to exogenous corticosterone was significantly restored by acupuncture at HT7 (P < 0.05), but the restoration in the CA3 area was not statistically significant (P = 0.526). In the study that used Morris Water Maze test to measure the learning and memory functions, the HT7 acupuncture group had significantly reduced escape latency (P < 0.01 on day 5 and P < 0.05 on day 6) and spent more time around the platform area in probe trial compared with impaired group (P < 0.05)[20].
The above study also investigated the effect of acupuncture on choline acetyltransferase activity in brain. The number of choline acetyltransferase-immunoreactive neurons was significantly increased in the medial septum region and the hippocampal CA1 in the HT7 acupuncture group (P < 0.05), compared with the impaired group[20]. Nevertheless, the relationship between enzyme activities and learning and memory functions was not investigated in these two studies.
This might suggest that acupuncture attenuated the impairments of memory and cognition by restoring cholinergic neurochemical abnormalities. However, both studies had only a few rats in each group (Kim et al[17]: 5–6 rats in each group; Lee et al[20]: 4 rats in each group were used for acetylcholinesterase and choline acetyltransferase tests). In the study conducted by Lee et al[20], there was no screening for cognitive impairment after corticosterone injection. With all these limitations, future studies are needed to examine the thorough relationship between acupuncture and cholinergic neurochemical activities in different areas of the brain.
More well-designed studies are required to establish the mechanism of acupuncture effect on cognitive function with respect to activities of cholinergic neurons in the brain.
Effect on superoxide dismutase, catalase, glutathioneperoxidase
Free radicals and the oxidative stress were the prime candidates to be responsible for producing the neuronal damages and cognitive deficits[24]. Comparing patients with vascular dementia, with Alzheimer's disease and control group, antioxidant defense decreased and the susceptibility to oxidative stress increased[25].
There were two studies from this review which investigated the effects of antioxidants like superoxide dismutase, catalase, glutathioneperoxidase in relation to improvement in cognition[13,19].
Both acupuncture and ginger pharmacopuncture in which ginger extract was injected into acupoint induced significant elevation of catalase and glutathioneperoxidase activities in the cerebral cortex and hippocampus compared with the sham group (P < 0.05 for all). However, both acupuncture and ginger pharmacopuncture produced a significant elevation of superoxide dismutase activity only in the hippocampus compared with sham (P < 0.05)[19].
Another study also showed that there was a significant decrease in the superoxide dismutase activity in hippocampus of rats in impaired and placebo-acupuncture groups when compared with the normal rats (P < 0.05). However, acupunctural treatment caused a significant increase in hippocampal superoxide dismutase activity. A significant reduction in the glutathioneperoxidase activity was found in the hippocampus of rats in the impaired and placebo-acupuncture groups when compared with the normal rats (P < 0.01). After acupunctural treatment, a significant increase of glutathioneperoxidase activity was observed in the hippocampus. However, the catalase activity had no significant difference among all the five groups (P > 0.05)[13].
The insignificant changes in the catalase activity in the second study might be due to the fact that the catalase activity in the rat brain was very low[13,26]. Acupunctural treatment increased superoxide dismutase and glutathioneperoxidase activities in the hippocampus of the cerebral multi-infarction rats. The increase of superoxide dismutase induced by acupuncture could convert superoxide radicals into hydrogen peroxide. Subsequently, the increase of glutathioneperoxidase and catalase induced by acupuncture broke down hydrogen peroxide to water molecules, prevented hydrogen peroxide from converting into hydroxyl radicals, the most toxic form of free radicals which are involved in a number of brain lesions and in brain aging[13,26].
However, there were still some confounding factors. To illustrate this, only a small number of rats were sacrificed to examine their brains (24 rats[13] and 15 rats[19] respectively). In Jittiwat's study, there was no normal control group[19]. Therefore there was no comparison of catalase and glutathioneperoxidase activity between cognitive impaired subjects undergoing acupuncture and normal subjects, but only comparison with cognitive impaired subjects with sham acupuncture.
Effect of copper-zinc superoxide dismutase mRNA and its protein
In this review, one study[13] investigated the effect of acupuncture on copper-zinc superoxide dismutase mRNA and its protein. The decreased expression of copper-zinc superoxide dismutase mRNA in the hippocampus was observed in the impaired rats and the expression of copper-zinc superoxide dismutase mRNA in the hippocampus significantly increased in the acupuncture-treated group (P < 0.01). Copper-zinc superoxide dismutase positive cells in the hippocampus of the normal group was higher than in sham-operated groups, but was not statistically significant (P > 0.05). The copper-zinc superoxide dismutase positive cells in the acupuncture group were significantly higher than that in the impaired group (P < 0.01). The value of the placebo-acupuncture group did not differ from the impaired group. The expression pattern of copper-zinc superoxide dismutase protein was similar to that of its mRNA. There was no difference of the copper-zinc superoxide dismutase positive cells between normal and sham-operated groups (P > 0.05). The copper-zinc superoxide dismutase in the acupuncture group was significantly higher than that in the impaired group (P < 0.01). The value for the placebo-acupuncture group did not differ from the impaired group.
This study also showed that the lower copper-zinc superoxide dismutase expression of the cerebral multi-infarction rats increased in the acupuncture group. These results suggest that acupunctural treatment could maintain the oxidant-antioxidant balance to a greater extent[13].
To conclude, acupuncture could increase the copper-zinc superoxide dismutase expression, consequently exerting antioxidant effects and improve cognition. However, acupuncture might improve cognitive deficits by many possible ways, and the result might be affected by some confounding factors, including small sample size. Further studies are required to elucidate the mechanisms in detail.
Effect of neurotrophin regulation
Neurotrophins, a class of growth factors, are a family of proteins that induce the survival, development, and function of neurons.
In our review, two of the neurotrophins, i.e. brain-derived neurotrophic factor and nerve growth factor, were investigated in rats[15,20]. Brain-derived neurotrophic factor played an important role in hippocampal long-term[27]. Nerve growth factor was required for the survival of developing sympathetic and sensory neurons[28].
Brain-derived neurotrophic factor and nerve growth factor: Manni et al[15] studied the effect of electro-acupuncture in social isolated mice on brain-derived neurotrophic factor and nerve growth factor concentration in hypothalamus, hippocampus and striatum.
Only the isolated electroacupuncture group showed a significant decrease of brain-derived neurotrophic factor in the hippocampus compared to isolated control group (P < 0.05). While other groups showed no significant difference[15].
For nerve growth factor, no differences between all four groups were found in the hypothalamus. In the striatum and hippocampus, the isolated electroacupuncture group showed the lowest values when compared to isolated control and non-isolated electroacupuncture groups (P < 0.05)[15].
The learning abilities were measured by passive avoidance task. In acquisition phase, isolated control group had lower latency to step-through during 10 trials compared to isolated electroacupuncture and non-isolated controls (P < 0.01). Also isolated controls had high values of the number of trials to reach learning criteria compared to the other three groups (P < 0.05). This suggested a delay in learning performances of the isolated control groups[15].
This study suggested that electroacupuncture on ST36 could help socially isolated mice to improve the delay of learning performances and electroacupuncture had a down regulation effect on brain-derived neurotrophic factor and nerve growth factor. However, the treatment course for electroacupuncture lasted only 4 days, and it failed to show any differences in the retention phase of passive avoidance task[15].
Brain-derived neurotrophic factor: Lee et al[20] studied the effect of acupuncture on corticosterone-induced cognitive impairment rats on brain-derived neurotrophic factor mRNA expression in the hippocampus.
In the hippocampus, brain-derived neurotrophic factor mRNA expression in corticosterone (impaired) group significantly decreased compared to that in the normal group (P < 0.001). The brain-derived neurotrophic factor mRNA expression in corticosterone-HT group significantly increased compared to corticosterone group (P < 0.05), and the brain-derived neurotrophic factor mRNA level was similar to that of normal rats in the normal group (P < 0.001)[20].
The learning abilities were measured using Morris Water Maze; the corticosterone-HT group was significantly shorter in escape latency and longer retention time compared with the corticosterone group (both P < 0.05). It showed the recovery of spatial memory in the corticosterone-HT group[20].
This study suggested that acupuncture on HT7 could help to improve cognitive impairment due to chronic corticosterone injection and had an up-regulating effect on brain-derived neurotrophic factor expression. However, only 3 rats in each group were sacrificed for brain-derived neurotrophic factor analysis[20].
These two studies suggested that brain-derived neurotrophic factor was affected in different cases of cognitive impairment. Applying acupuncture to different acupoints could help to normalize the brain-derived neurotrophic factor level by either up- or down-regulation[15,20].
Bcl-2, Bax and apoptosis
The members of the bcl-2 family of genes play an important role in regulating apoptosis[29]. One member of the family, Bcl-2, functions as a repressor of apoptosis whereas another member of the family, Bax, acts as a promoter of cell death[30].
One study in our review studied the effect of acupuncture on memory performance, the expression of Bcl-2 family, and apoptosis in hippocampal CA1 region after cerebral multi-infarction in rats[16]. The acupuncture group showed improvements in acquisition (P < 0.05), relearning ability (P < 0.05) and retention of spatial memory (P < 0.05) when compared to the impaired and placebo-acupuncture groups. The mRNA expression (P < 0.01) and protein expression of Bcl-2 (P < 0.01) was up-regulated in the acupuncture group when compared with the impaired group; on the other hand, the mRNA expression (P < 0.01) and protein expression of Bax (P < 0.01) decreased in the acupuncture group when compared with the impaired group. For apoptosis, the number of apoptotic cells significantly decreased (P < 0.05) in the acupuncture group when compared with the impaired group.
According to these observations, acupuncture might protect the neurons in the hippocampus by regulating the apoptotic cell death, thus promoting cell survival and improve cognitive performances. In order to construct a complete mechanism, further well-designed studies should be conducted to investigate the effect of acupuncture on apoptosis in different areas of the brain after multi-infarction.
Acupuncture effects on brain cell proliferation and nerve cell apoptosis
Previous studies have shown that rat's brain cell proliferation could be influenced by exercise[31,32]. In our review, one group studied the effect of acupuncture on cognitive function and brain cell proliferation in senescence-accelerated prone mouse rats which were genetic pre-exposure to Alzheimer disease-like disease rats[14]. There was significant decrease of cell proliferation in the dentate gyrus, lateral ventricles, corpus callosum and dorsum of alveus hippocampi in the senescence-accelerated prone mouse control group when compared to normal control group (P < 0.05), while significant increase was noted in senescence-accelerated prone mouse acupuncture group when compared to control group and senescence-accelerated prone mouse non-acupoint control groups (P < 0.01). There was learning deficit (hidden platform trial), memory deficit (probe trial) and impaired relearning ability (reversal trial) of control group when compared to normal control group (P < 0.01). There was increase of learning and memory ability in acupuncture group compared to control group (P < 0.05) and non-acupoint control groups (P < 0.01), and also increase of relearning ability in acupuncture group compared to control group and non-acupoint control groups (P < 0.01)[14].
These results suggest that acupuncture could improve cognitive function in senescence-accelerated prone mouse rats. This improvement might be due to the increase of cell proliferation in multi-regions of the brain. Future studies should investigate the relationship between brain cell proliferation and cognitive function. Researchers could progress to test the effects on human subjects with Alzheimer's disease in order to provide higher level of evidence to support the use of acupuncture as an alternative treatment in dementia rehabilitation.
Effect of glycometabolic enzymes regulation
Some studies have indicated that there was abnormal energy metabolism in vascular dementia patient brain[33,34]. Recent studies showed that acupuncture could increase cerebral glucose metabolism in human with vascular dementia[35], and suggested that cognitive impairment caused by vascular dementia might be related to impaired glucose metabolism in the brain.
In our review, one study investigated the effects of acupuncture on the right cortex and hippocampus in rat brain glycometabolic enzymes, i.e., hexokinase, glucose 6-phosphate dehydrogenase and pyruvate kinase, in multi-infarct dementia rats. Impaired rats and impaired rats with non-acupuncture had significant lower enzyme activities than normal rats (normal group) (P < 0.01). Impaired rats with acupuncture had significant higher enzyme activities than impaired rats and impaired rats with non-acupuncture (P < 0.01), and the values were increased toward normal group. The learning abilities were measured by Morris Water Maze. Impaired rats and impaired rats with non-acupuncture had significant higher escape latency than normal group (P < 0.01) and impaired rats with acupuncture had significant lower escape latency than impaired rats and impaired rats with non-acupuncture (P < 0.01), and there were no differences when compared to normal group (no P value provided). But the relationship between enzyme activities and escape latency in Morris Water Maze was not investigated[18].
These results suggest that the improvement in learning abilities, one aspect of cognitive function, was associated with the up-regulation of glycometabolic enzyme activities. However, as only hidden-platform trial was used in Morris Water Maze, the decrease of escape latency in impaired rats with acupuncture compared to impaired rats might be due to the other confounding factors, including improvement of local motion ability and mood up-regulation. Future studies should investigate the relationship between those enzyme activities, ATP concentration or consumption in the brain and cognitive function, and study the thorough mechanism of acupuncture effects on cognitive function with respect to glycometabolic enzyme activities in the brain.
Implications for future research
While acupuncture has been advocated as a treatment to improve cognitive function impairment in patients with dementia, a lack of high-quality research in this area has so far prevented the development of sound recommendations for clinical practice. More high-quality research on human is essential. It might not be ethical to have a control group without any treatment. Future research should focus on the effect of acupuncture versus convention rehabilitation, medicines, and the effect of combined treatments, to find out the most cost-effective treatment that promotes the greatest magnitude of recovery. Also, a follow-up assessment should be included to investigate the long-lasting effect of acupuncture. Moreover, the acupoints and protocols that were used in published research varied a lot. Therefore, standardized treatment protocols are needed and should be developed.
Acupuncture has been used to treat cognitive impairment, but there is a lack of high-quality evidence in humans. Since there were only a limited number of published human studies and the results of the three human studies included in our review were not consistent, this may be due to many confounding factors. Therefore, we cannot draw any conclusion on the effectiveness of acupuncture for cognitive function improvement in humans. The results of acupuncture protocols are variable, although a number of individual studies reported positive effects on cognitive function. Further high-quality research is needed to determine the effectiveness of acupuncture and an optimal protocol.
Footnotes
Conflicts of interest: None declared.
(Reviewed by Xu XM)
(Edited by Liu WJ, Li CH, Song LP)
REFERENCES
- [1].Hoffmann M. Higher cortical function deficits after stroke: an analysis of 1,000 patients from a dedicated cognitive stroke registry. Neurorehabil Neural Repair. 2001;15(2):113–127. doi: 10.1177/154596830101500205. [DOI] [PubMed] [Google Scholar]
- [2].Riedel O, Klotsche J, Spottke A, et al. Cognitive impairment in 873 patients with idiopathic Parkinson's disease. Results from the German Study on Epidemiology of Parkinson's Disease with Dementia (GEPAD) J Neurol. 2008;255(2):255–264. doi: 10.1007/s00415-008-0720-2. [DOI] [PubMed] [Google Scholar]
- [3].Verhoeven CL, Post MW, Schiemanck SK, et al. Is cognitive functioning 1 year poststroke related to quality of life domain? J Stroke Cerebrovasc Dis. 2011;20(5):450–458. doi: 10.1016/j.jstrokecerebrovasdis.2010.02.018. [DOI] [PubMed] [Google Scholar]
- [4].Geneva: WHO; 2012. World Health Organization. Alzheimer's Disease International. Dementia: a public health priority. [Google Scholar]
- [5].Maciocia G. London: Churchill Livingstone; 1989. The foundation of Chinese medicine. [Google Scholar]
- [6].Filshie J, White A. Acupuncture in context. In: Cummings M, editor. Medical Acupuncture. London: Churchill Livingstone; 1998. [Google Scholar]
- [7].Helms JM. Berkeley: Medical Acupuncture Publishers; 1995. Acupuncture Energetics: A Clinical Approach for Physicians. [Google Scholar]
- [8].Centre for Evidence-based Medicine Oxford University; 2009. Mar, [Accessed March 25, 2013]. Levels of Evidence. Available at: http://www.cebm.net/index.aspx?o=1025 . [Google Scholar]
- [9].Rorsman Ia, Johansson B. Can electroacupuncture or transcutaneous nerve stimulation influence cognitive and emotional outcome after stroke? J Rehabil Med. 2006;38(1):13–19. doi: 10.1080/16501970510040362. [DOI] [PubMed] [Google Scholar]
- [10].Chou P, Chu H, Lin JG. Effects of electroacupuncture treatment on impaired cognition and quality of life in Taiwanese stroke patients. J Altern Complement Med. 2009;15(10):1067–1073. [PubMed] [Google Scholar]
- [11].Chen LP, Wang FW, Zuo F, et al. Clinical research on comprehensive treatment of senile vascular dementia. J Tradit Chin Med. 2011;31(3):178–181. doi: 10.1016/s0254-6272(11)60036-8. [DOI] [PubMed] [Google Scholar]
- [12].Yu J, Liu C, Zhang X, et al. Acupuncture improved cognitive impairment caused by multi-infarct dementia in rats. Physiol Behav. 2005;86(4):434–441. doi: 10.1016/j.physbeh.2005.07.015. [DOI] [PubMed] [Google Scholar]
- [13].Liu CZ, Yu JC, Zhang XZ, et al. Acupuncture prevents cognitive deficits and oxidative stress in cerebral multi-infarction rats. Neurosci Lett. 2006;393(1):45–50. doi: 10.1016/j.neulet.2005.09.049. [DOI] [PubMed] [Google Scholar]
- [14].Cheng H, Yu J, Jiang Z, et al. Acupuncture improves cognitive deficits and regulates the brain cell proliferation of senescence-accelerated prone mouse mice. Neurosci Lett. 2008;432(2):111–116. doi: 10.1016/j.neulet.2007.12.009. [DOI] [PubMed] [Google Scholar]
- [15].Manni L, Aloe L, Fiore M. Changes in cognition induced by social isolation in the mouse are restored by electro-acupuncture. Physiol Behav. 2009;98(5):537–542. doi: 10.1016/j.physbeh.2009.08.011. [DOI] [PubMed] [Google Scholar]
- [16].Wang T, Liu CZ, Yu JC, et al. Acupuncture protected cerebral multi-infarction rats from memory impairment by regulating the expression of apoptosis related genes Bcl-2 and Bax in hippocampus. Physiol Behav. 2009;96(1):155–161. doi: 10.1016/j.physbeh.2008.09.024. [DOI] [PubMed] [Google Scholar]
- [17].Kim H, Park H, Shim HS, et al. The effects of acupuncture (PC6) on chronic mild stress-induced memory loss. Neurosci Lett. 2011;488(3):225–228. doi: 10.1016/j.neulet.2010.09.080. [DOI] [PubMed] [Google Scholar]
- [18].Zhao L, Shen P, Han YY, et al. Effects of acupuncture on glycometabolic enzymes in multi-infarct dementia rats. Neurochem Res. 2011;36(5):693–700. doi: 10.1007/s11064-010-0378-x. [DOI] [PubMed] [Google Scholar]
- [19].Jittiwat J, Wattanathorn J. Ginger pharmacopuncture improves cognitive impairment and oxidative stress following cerebral ischemia. J Acupunct Meridian Stud. 2012;5(6):295–300. doi: 10.1016/j.jams.2012.09.003. [DOI] [PubMed] [Google Scholar]
- [20].Lee B, Sur B, Kwon S, et al. Acupuncture stimulation alleviates corticosterone-induced impairments of spatial memory and cholinergic neurons in rats. Evid Based Complement Alternat Med 2012. 2012 doi: 10.1155/2012/670536. 670536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Bierer LM, Haroutunian V, Gabriel S, et al. Neurochemical correlates of dementia severity in Alzheimer's disease: relative importance of cholinergic deficits. J Neurochem. 1995;64(2):749–760. doi: 10.1046/j.1471-4159.1995.64020749.x. [DOI] [PubMed] [Google Scholar]
- [22].Whitehouse PJ, Price DL, Clark AW, et al. Alzheimer's disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10(2):122–126. doi: 10.1002/ana.410100203. [DOI] [PubMed] [Google Scholar]
- [23].Oda Y. Choline acetyltransferase: the structure, distribution and pathologic changes in the central nervous system. Pathol Int. 1999;49(11):921–937. doi: 10.1046/j.1440-1827.1999.00977.x. [DOI] [PubMed] [Google Scholar]
- [24].Cantuti-Castelvetri I, Shukitt-Hale B, Joseph JA. Neurobehavioral aspects of antioxidants in aging. Int J Dev Neurosci. 2000;18(4-5):367–381. doi: 10.1016/s0736-5748(00)00008-3. [DOI] [PubMed] [Google Scholar]
- [25].Ryglewicz D, Rodo M, Kunicki PK, et al. Plasma antioxidant activity and vascular dementia. J Neurol Sci. 2002;203-204:195–197. doi: 10.1016/s0022-510x(02)00290-3. [DOI] [PubMed] [Google Scholar]
- [26].Moreno S, Mugnaini E, Cerù MP. Immunocytochemical localization of catalase in the central nervous system of the rat. J Histochem Cytochem. 1995;43(12):1253–1267. doi: 10.1177/43.12.8537642. [DOI] [PubMed] [Google Scholar]
- [27].Nacmias B, Piccini C, Bagnoli S, et al. Brain-derived neurotrophic factor, apoplipoprotein E genetic variants and cognitive performance in Alzheimer's disease. Neurosci Lett. 2004;367(3):379–383. doi: 10.1016/j.neulet.2004.06.039. [DOI] [PubMed] [Google Scholar]
- [28].Freeman RS, Burch RL, Crowder RJ, et al. NGF deprivation-induced gene expression: After ten years, where do we stand? Prog Brain Res. 2004;146:111–126. doi: 10.1016/S0079-6123(03)46008-1. [DOI] [PubMed] [Google Scholar]
- [29].Kroemer G. The proto-oncogene Bcl-2 and its role in regulating apoptosis. Nat Med. 1997;3(6):614–620. doi: 10.1038/nm0697-614. [DOI] [PubMed] [Google Scholar]
- [30].Brady HJ, Gil-Gómez G. Bax. The pro-apoptotic Bcl-2 family member, Bax. Int J Biochem Cell Biol. 1998;30(6):647–650. doi: 10.1016/s1357-2725(98)00006-5. [DOI] [PubMed] [Google Scholar]
- [31].Uda M, Ishido M, Kami K, et al. Effects of chronic treadmill running on neurogenesis in the dentate gyrus of the hippocampus of adult rat. Brain Res. 2006;1104(1):64–72. doi: 10.1016/j.brainres.2006.05.066. [DOI] [PubMed] [Google Scholar]
- [32].Wu CW, Chen YC, Yu L, et al. Treadmill exercise counteracts the suppressive effects of peripheral lipopolysaccharide on hippocampal neurogenesis and learning and memory. J Neurochem. 2007;103(6):2471–2481. doi: 10.1111/j.1471-4159.2007.04987.x. [DOI] [PubMed] [Google Scholar]
- [33].Zuo F, Shi X, Tian JH. Effects of electroacupuncture on the cerebral glucose metabolism of stroke patients: a PET study. Chi Arch Tradit Chin Med. 2008;26(4):742–743. [Google Scholar]
- [34].Kuczynski B, Reed B, Mungas D, et al. Cognitive and anatomic contributions of metabolic decline in Alzheimer's disease and cerebrovascular disease. Arch Neurol. 2008;65:650–655. doi: 10.1001/archneur.65.5.650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Huang Y, Chen J, Htut WM, et al. Acupuncture increases cerebral glucose metabolism in human vascular dementia. Intern. J. Neuroscience. 2007;117:1029–1037. doi: 10.1080/00207450600936825. [DOI] [PubMed] [Google Scholar]
- [36].Yu YF, Zhai F, Dai CF, et al. The relationship between age-related hearing loss and synaptic changes in the hippocampus of C57BL/6J mice. Exp Gerontol. 2011;46(9):716–722. doi: 10.1016/j.exger.2011.04.007. [DOI] [PubMed] [Google Scholar]