

Ambulatory blood pressure monitoring (ABPM) has established roles in the evaluation and management of hypertension in adults but has only been applied to children and adolescents more recently.1 In 2008, the American Heart Association (AHA) issued the first set of consensus recommendations for performance and interpretation of ABPM in pediatrics. Since then, ABPM has found increasing use in children and adolescents, as recently summarized.2 The present document updates the 2008 AHA statement on the use of ABPM in the pediatric population3 with additional data published since the release of that report and also presents a revised interpretation schema. Because no outcome studies are yet available relating ABPM levels in children to outcomes such as myocardial infarction or stroke, these guidelines are largely driven by expert opinion, although they are also informed by available pediatric data on ABPM and surrogate markers of cardiovascular disease.
Cardiovascular Risk in the Pediatric Population
Epidemiology of Hypertension
High blood pressure (BP) is the leading risk factor–related cause of death throughout the world, accounting for 12.8% of all deaths, including 51% of stroke deaths and 45% of coronary heart disease deaths.4 In the United States, 33.0% of adults >20 years of age have hypertension.5 As our population continues to age, this will only increase, because 90% of people with normal BP at age 55 years will go on to develop hypertension in their lifetimes.6
The prevalence of hypertension in youths is also on the rise. US National Health and Nutrition Examination Survey (NHANES) data from 1963 to 2002 showed a 2.3% increase in prehypertension and a 1% increase in hypertension from 1988 to 1999, with higher rates in non-Hispanic blacks and Mexican Americans.7 In fact, the entire distribution of childhood BP has shifted upward in the United States by 1.4 mm Hg for systolic BP (SBP) and 3.3 mm Hg for diastolic BP (DBP).8 However, adjustment of the NHANES data for body mass index (BMI) attenuated the increase in SBP by 29% and DBP by 12%, which suggests that some of the increase may be related to the obesity epidemic.8 This is supported by studies of the effect of the westernization of primitive societies, in which BMI has the most substantial effect on the age-related increase in BP compared with all other risk factors.9 A cross-sectional pediatric study conducted in Canada found that obese adolescents had 7.6 mm Hg higher SBP than normal-weight youths, with BMI exerting the strongest effect on BP.10 The increased prevalence of prehypertension and sustained hypertension with increasing BMI was confirmed in a school-based study in Texas.11 Furthermore, longitudinal evaluation of the National High Blood Pressure Education Program childhood BP database confirmed that a higher BMI increases the rate of progression from prehypertension to hypertension.12
However, an obesity-related increase in BP has not been documented in all studies. In the Bogalusa Heart Study, which used the mean of 6 resting BP measurements instead of 2 or 3 measurements, there was a significant increase in the prevalence of obesity from 1974 to 1993, yet there were only small changes in BP levels.13 Therefore, despite methodological differences that make cross-population estimates of hypertension difficult to interpret,14 most investigators believe obesity-related hypertension is on the rise.
The rise in prevalence of hypertension in the young is especially worrisome, because autopsy studies such as the Bogalusa Heart Study and the Pathobiological Determinates of Atherosclerosis in Youth study have demonstrated increased atherosclerosis at higher BP levels in youths.15,16 Therefore, accurate assessment of BP and treatment of hypertension in children and adolescents are essential for the prevention of future heart disease.17 Emerging data suggest that ABPM may be superior to clinic BP in predicting cardiovascular morbidity and mortality in adults.18 For this reason, ABPM is being increasingly used in the evaluation for hypertension and risk of end-organ damage in youths.
BP and Risk for Target-Organ Damage
Substantial data exist that link elevated BP levels measured in childhood and future target-organ damage. Pooled data from longitudinal epidemiological studies of cardiovascular risk factors in youths from the International Childhood Cardiovascular Cohort (i3C) Consortium demonstrated that higher BP measured at as young as 12 years of age predicted increased adult carotid intima-media thickness (cIMT).19 Similarly, childhood hypertension was related to higher adult pulse-wave velocity in the Cardiovascular Risk in Young Finns Study,20 which indicates increased arterial stiffness, and the Bogalusa Heart Study found that the cumulative burden of SBP from childhood to adulthood was a significant predictor of adult left ventricular mass (LVM).21
BP levels have also been related to target-organ damage measured in childhood. SBP has been demonstrated to independently determine cIMT in both children22 and adolescents.23 Alterations of vascular function also occur at higher levels of childhood BP, including reduced brachial artery distensibility,24,25 higher pulse-wave velocity,26,27 and increased augmentation index,28 all of which indicate increasing arterial stiffness. This is relevant to future cardiovascular disease, because increased vascular thickness29 and stiffness30 are associated with higher LVM in adolescents, a risk factor for future adult cardiovascular disease.31 Therefore, it is not surprising that hypertensive youths may demonstrate left ventricular hypertrophy (LVH),32,33 but what is even more worrisome is the observation that adolescents with prehypertension already have higher LVM values than normotensive control subjects.28,34 Furthermore, hypertension may also have neurovascular consequences, because untreated hypertensive children had lower cerebral artery reactivity than normotensive control subjects,35 which may explain the lower scores on cognitive tests found in children with elevated BP.36
ABPM may be superior to casual (office) BP measurement in its ability to distinguish patients at the highest risk for target-organ damage. In adults, ABPM correlates more strongly with LVM than casual BP.37 In children in a hypertension clinic, no correlation was found between LVM and casual BP, yet a strong relationship existed with ABPM parameters.38 In fact, when hypertension was confirmed by 24-hour ABPM, the odds for LVH were 7.23 compared with only 4.13 when hypertension was diagnosed with casual BP levels.39 Another study found APBM parameters were superior to both casual and home BP in predicting LVM.40 Most other pediatric studies, with 1 notable exception,41 have confirmed the strong relationship between hypertension diagnosed with ABPM and elevated LVM.34,42–44 The 1 study that found no association between ABPM and LVM was missing echocardiograms on 24% of subjects (possible selection bias) and used oscillometric devices to measure casual BP (possible measurement bias).41
Increased cIMT, a risk factor for stroke in adults,45 is similarly correlated with high BP on ABPM,46,47 with the relationship independent of casual BP.48 In hypertensive children, thicker cIMT is found with higher ABPM levels,49–51 even when the children are matched by BMI.52 The only study that found no relationship between ABPM levels and cIMT was a small study of children who had received a renal transplant, in whom other serious disease processes or medication use may have confounded the relationship.53 New data are now available relating BP measured with ABPM and arterial stiffness. The ambulatory arterial stiffness index (AASI), which correlates with pulse-wave velocity, is calculated as 1 minus the regression slope of DBP plotted against SBP from ABPM. Using this technique, Simonetti et al54 found that hypertensive children had higher AASI values than normotensive control subjects. This has been replicated in youths with type 1 diabetes mellitus and hypertension.55 Using direct measurements, when BP was evaluated with ABPM, youths categorized as either prehypertensive or truly hypertensive had increased pulse-wave velocity compared with normotensive subjects.56 In obese youths, higher ABPM (but not casual BP) was found to be associated with higher carotid stiffness and reduced endothelial function.57 Similarly, decreased carotid distensibility was associated with higher daytime ambulatory SBP load in pediatric renal transplant recipients.58
Usefulness of ABPM to Classify BP
White Coat Hypertension
White coat hypertension (WCH) is defined as casual/office BP levels that are ≥95th percentile but normal outside of a clinical setting. It has been suggested that high BP variability, perhaps caused by transient, stress-induced elevation of BP, may contribute to clinical misclassification of hypertension.59 However, WCH may not be entirely benign. In adults with normal ABPM, BP variability increases with increasing BP and is associated with target-organ damage and cardiovascular events.60 In fact, WCH may represent an intermediate pathophysiological stage between normotension and hypertension.61 Target-organ damage, such as increased LVM,32,51,62,63 increased cIMT,51,63 abnormalities in BP and heart rate rhythmicity,64 and impaired cerebral vascular reactivity,65 may develop in youths with WCH.
A wide range of WCH prevalence has been reported in the literature. A study of 18 male adolescent athletes reported 88% had WCH,66 whereas a study of 1071 Icelandic children 9 to 10 years of age found sustained hypertension in 2.5% and WCH in just 0.6%.67 Other pediatric studies have reported the prevalence of WCH to be in the range of 22% to 32%.68 Of note, Sorof et al69 have suggested that the use of ABPM to rule out WCH should be limited to patients with borderline or mild clinical hypertension, because patients with higher office BP levels are more likely to be truly hypertensive.
Masked Hypertension
ABPM may also detect masked hypertension (MH), defined as a normal clinic BP but elevated ambulatory levels. MH is difficult to detect but may be suspected with previous reports of elevated clinical BP from other providers, or if the clinical presentation (ie, LVH) appears inconsistent with the clinic BP. Estimates of the prevalence of MH range from 7.6% in 592 unselected children70 to 9.4% in 85 youths referred for hypertension evaluation71 to 15% in Brazilian youths.72 In 1 study, rates of MH did not appear to differ by age (older or younger than 15 years),73 but MH may be more common in obese youths (19%), especially if they display a nondipper pattern (32.3%; P≤0.001).74 A meta-analysis reported a 7% prevalence of MH in children and 19% in adults, with an overall average of 16.8%.75 This report also found that LVM in patients with MH was higher than in normotensive people and similar to that in people with sustained hypertension, which suggests that MH imparts a similar cardiovascular risk as sustained hypertension.75 In pediatric patients, data also suggest that MH predicts target-organ damage.70,71 Unfortunately, determining the true prevalence of MH would require the use of ABPM in large unselected populations.
Other situations in which ABPM may be especially helpful in “unmasking” hypertension include pediatric dialysis patients, whose BP may be normal after dialysis but hypertensive at other times.76 Similarly, after aortic coarctation repair, MH was associated with abnormal left ventricular structure and function.77 The prevalence of MH was reported at 9.5% in youths with type 1 diabetes mellitus.68
Prehypertension and Progression to Sustained (Ambulatory) Hypertension
Prehypertension is now recognized as a condition that requires careful evaluation and follow-up. Pediatric patients with casual prehypertension may demonstrate abnormalities on ABPM intermediate between normotensive and truly hypertensive people,78 and some studies have demonstrated subtle signs of target-organ damage in patients with prehypertension, including LVM values similar to youths with sustained hypertension,34 lower glomerular filtration rate, and increased urine protein excretion,79 as well as higher cIMT than normotensive patients.80 Patients with prehypertension may also be at higher risk of progressing to sustained hypertension.12 Although no longitudinal ABPM studies have been performed to evaluate the risk of progression of prehypertension, such studies could clarify the importance of prehypertension by providing more careful phenotyping of the BP patterns that produce the highest risk of progression to sustained hypertension.
Determinants of Ambulatory BP
Several determinants that influence ambulatory BP must be adjusted for in the establishment of normalized values in pediatric patients. In the pediatric population, age is independently correlated with 24-hour SBP81 and BP variability.82,83 Birth weight has been shown to be associated with ambulatory BP. Most but not all studies84 find an inverse association between birth weight and daytime SBP after controlling for covariates.85–89 Ethnicity is known to influence ambulatory BP in children and youths, an effect that may be attributable to racial differences in the relationship of body size to BP90,91 or racial differences in the effect of psychosocial stress on BP.92 Ambulatory BP is also affected by sex, with male youths having higher ambulatory BP than their female counterparts, irrespective of ethnicity.93,94 Obesity, possibly through the restriction of sodium excretion,95 is associated with increased ambulatory BP.95,96
Other proposed determinants of ambulatory BP include autonomic tone,97–99 adiponectin,100,101 and serum uric acid.102 Lower plasma renin activity was independently associated with lower 24-hour SBP in obese adolescents.103 However, blood aldosterone-to-renin ratio was not found to be associated with ambulatory BP in healthy children, although it did correlate with LVM.104 Finally, elevation of several ambulatory BP parameters has been associated with stimulant use in pediatric patients, including stimulants used for attention deficit/hyperactivity disorder105,106 and caffeine.107
Normative Data for ABPM
Data on normal ambulatory BP ranges in pediatric patients are required for the effective application of this assessment tool to this population. Once normal reference values are established, clinically relevant ABPM abnormalities can be differentiated and quantified as important deviations from the population-based distributions. Reference data must be derived from studies of healthy populations with sufficiently large samples that are proportionally representative of the larger pediatric population. Ideally, samples should be free of confounders that may alter BP measurement, including concurrent medication use and comorbidities such as obesity. Normative data should allow calculation of standardized values, particularly z scores and percentiles. Particularly in pediatric patients, assessment should be adjusted for various determinants of BP, such as age, sex, body size, race, and ethnicity. Established normative ambulatory BP ranges should also be validated by determination of associations with clinically relevant outcomes in the reference population, for example, end-organ damage and cardiovascular mortality/ morbidity.108 Although these associations have been determined in adults on the basis of a growing body of evidence, outcomes are largely preclinical in the pediatric population, and necessary longitudinal data are lacking; hence, the definitions are based on population-based distributions.
ABPM values differ substantially from casual measurements; therefore, comparisons to normative casual BP values such as those in the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents101a or the more recent integrated pediatric cardiovascular risk reduction guidelines17 may result in mis-classification of BP category.109,110 Reference values provided by the German Working Group on Pediatric Hypertension are currently considered the best available data for pediatric ABPM.81,111 Of several ABPM studies in healthy control subjects, this study alone has established percentiles normalized for the nongaussian distribution of 24-hour BP in children according to age and sex, using the LMS analysis method.81 However, as highlighted by Flynn,112 this data set has several limitations. First, it includes only central European white children, which limits its generalizability given that normal ABPM ranges appear to vary with ethnicity.113 Furthermore, relatively few shorter children (<140 cm in height) were included, which may limit the applicability of the results to children with certain health conditions, specifically chronic kidney disease (CKD).112 Finally, the data set demonstrated a striking lack of variability in ambulatory DBP values (Figure); resting DBP is known to vary by age and height, whereas at least 1 study has shown that ambulatory DBP varies with age.112,114 Thus, the normative values provided by the German Working Group on Pediatric Hypertension may not be representative of the normal ambulatory DBP in all pediatric patients.
Figure.
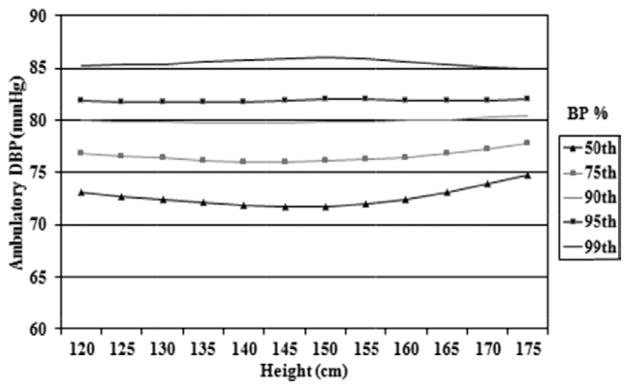
Graph of mean daytime diastolic ambulatory blood pressure (BP) for girls according to height in the Central European pediatric ambulatory blood pressure monitoring database. DBP indicates diastolic blood pressure. Modified from Wühl et al81 with permission of the publisher. Copyright © 2002, Lippincott Williams & Wilkins, Inc.
Beyond these data, other groups have measured ABPM in healthy populations, although none have provided useful normative values. O’Sullivan et al115 studied ambulatory BP in 1121 healthy school-aged children, reporting mean SBP and DBP during time at school, at home, and asleep. Ambulatory SBP was found to have a wide range in normal children, and no important differences were noted between school and home hours. Another study by Lurbe et al116 assessed ABPM values in 241 healthy children aged 6 to 16 years and reported BP as systolic and diastolic means and percentiles, circadian variability, and pressure load. Some ABPM data have also been collected from very young healthy children; Varda et al117 studied the applicability of ABPM in 97 healthy infants and toddlers, reporting mean daytime, nighttime, and 24-hour SBP and DBP. Similarly, Gellermann et al118 reported mean daytime and nighttime SBP and DBP for healthy children aged 3 to 6 years. Still, despite this research, there is a critical need for expanded normative data for pediatric ABPM; specifically, normal values for ambulatory DBP are needed, because they may not be appropriately represented by the currently available data.
Methods for Performance of ABPM
Nursing Implications
Nurses and other healthcare personnel involved in ABPM should follow a standardized approach to ABPM to maintain the functionality of the equipment, minimize measurement errors, and obtain valid, reliable, and reproducible BP data.3 Care of the equipment may include yearly calibration (by either the institution’s biomedical engineering department or the manufacturer), depending on the manufacturer’s recommendation; cleaning the hardware with disinfecting wipes; and laundering the reusable cloth covers for the BP cuffs between patients. The nurse or other appropriately trained staff should review the patient’s history for any contraindications to ABPM (severe clotting disorders or rhythm disturbances, and for some brands of equipment, latex allergy). Serious adverse events such as arm vein thrombosis have not been reported in children, although mild sleep disturbances have been documented.119,120 Although some investigators do not believe these alterations in sleep substantially alter ABPM results,121 1 study did find higher 48-hour ABPM in white but not black adolescents who had shortened actigraphy-assessed sleep time.122
Care should be taken in selection of the appropriate size cuff according to published guidelines.101a Although casual BP is usually taken in the dominant arm, ABPM should be applied to the child’s nondominant arm to avoid interference with school work, unless the child has arterial surgery on that side, such as repair of coarctation of the aorta or creation of an arteriovenous fistula.101a After application, the ambulatory BP should be measured and compared with resting, clinic BP by use of the same technique as the ABPM (auscultatory or oscillometric). If the average of 3 values is >5 mm Hg higher or lower, cuff placement should be adjusted or the device checked for calibration.
Successful ABPM is possible in most patients even during sleep,124 and comprehensive, standardized patient/parent education will reduce the failure rate in obtaining accurate ABPM.125 Patients and their parents need to be instructed how to stop a reading if there is excessive discomfort. This may signal kinked tubing. They should also be told to keep the arm still during readings. This is essential. Continuing with normal activities of daily living is encouraged, but monitors should not be allowed to get wet during swimming or damaged during contact sports. Removal of the monitor is not recommended, but if absolutely necessary, the device should be removed immediately after a reading to reduce the number of missed readings and reapplied as soon as possible. Finally, children should maintain a diary that indicates sleep and wake times, as well as activities that may influence BP measurements, including stressful situations or exercise, and timing of anti-hypertensive medications. Symptoms such as dizziness should also be recorded, because up to 91% of children with a history of syncope demonstrate postural hypotension on ABPM.126
After the ABPM data have been downloaded, the readings should be scanned briefly to assess the quality of the study. If BP dipping is seen at times other than the sleep time noted in the patient log, clarification with the patient of actual sleep/ wake times may be needed. Common reasons for missing data include the patient disconnecting the device at night, suspension of a reading by use of the cancellation button, turning the monitor off, dead batteries, movement artifact, or kinks in the tubing. Obtaining additional information from the patient will help determine whether missing data are patient or device related. Because ABPM studies as short as 6 hours’ duration have been found to correlate with 24-hour results in 1 recent pediatric study,127 many physicians will still interpret and accept the results of shortened monitoring periods for routine clinical care.
Equipment
For more detail on equipment used in ABPM, refer to the 2008 AHA scientific statement.3 Briefly, both oscillometric and auscultatory monitors are available for use in pediatric ABPM.111,115 Many monitors are available and have been evaluated with use of the Association for the Advancement of Medical Instrumentation US national standard or the British Hypertension Society standard.128,129 A comprehensive list noting validation status is available online at www.dableducational.org. Unfortunately, monitors that have not undergone validation testing or US Food and Drug Administration clearance can be sold in the United States, and few have been formally validated in children.130 Child-specific issues include the need for lightweight devices appropriate for smaller bodies, proper cuff sizing to ensure that the cuff width is ≈40% of the midarm circumference, and device tolerance of excessive motion.101a For auscultatory devices, users should ascertain whether the fourth or fifth Korotkoff sound is being used to estimate DBP and should be aware that no normative data are available for auscultatory ABPM.131,132 Although oscillometric devices may be easier to use and have fewer erroneous readings, oscillometric BP measurement also has inherent limitations, as reflected in the generally lower ratings on British Hypertension Society protocol evaluation.108 Nevertheless, most centers that perform ABPM in children and adolescents use oscillometric devices. These issues are summarized in Table 1.
Table 1.
Pros and Cons of Oscillometric Versus Auscultatory Ambulatory BP Devices
| Oscillometric | Auscultative |
|---|---|
Pros:
|
Pros:
|
Cons:
|
Cons:
|
BP indicates blood pressure.
Frequency of Measurement and Accounting for Activity
Expert opinion in pediatric ABPM recommends that at least 1 or 2 valid readings should be obtained per hour over the entire 24 hours (including during sleep) to consider an ABPM study to be adequate/interpretable. In routine clinical practice, it may be acceptable to consider as “interpretable” some ABPM studies that do not meet this high standard. Ideally, monitors should be programmed to obtain readings every 15 to 20 minutes, although some decrease in frequency during sleep is acceptable. Patient diaries are critical tools in the proper use of ABPM and should at minimum record the sleep times, nap times, and periods of physical activity.133,134
Interpretation software allows for customization of diurnal patterns and exclusion of selected readings gleaned ideally from accurate diary entries. Without specific day/night notation, automatic nighttime divisions may be set that range anywhere from a 9 PM to midnight start time and from a 6 to 9 AM wake time, with some algorithms excluding the readings obtained during these “buffer” periods.111 The use of inappropriate day/night divisions can lead to substantial mis-classification.133 Alternatively, patient-independent activity monitor–derived notation of diurnal cycles may be superior to patient notation.135 Activity period BPs are shown to be captured reliably on ABPM in general, although some specialists recommend avoidance of contact sports or vigorous exercise during ABPM.134,136 One study found that for each 1-unit increase in physical activity recorded by wrist actigraph, there were increases in SBP, DBP, and heart rate on ABPM of 0.02 mm Hg, 0.01 mm Hg, and 0.02 bpm, respectively.137 Recording on a school day may also be helpful, because weekend days may produce lower ABPM results.138
Editing Data and Calculations
Interpretation of ABPM studies is usually based on a combination of criteria, including mean SBP or DBP and BP loads. First, outlier data are filtered out by various automated approaches to minimize the observer bias inherent in users selecting particular measurements139,140; however, these automated filters may not be appropriate for young children, so caution is advised. Then, mean SBP and DBP are calculated for the entire 24-hour period, as well as the wake and sleep periods, with software that allows the user to define the diurnal transitions.141 BP load is then calculated as the proportion of readings above a threshold (usually the pediatric 95th percentile). Dipping is defined as the percentage drop from mean daytime to mean nighttime levels.
More complicated calculations of circadian BP rhythms have also been attempted in pediatric patients. One group used Fourier analysis to define circadian (24-hour) and ultradian (6-, 8- and 12-hour) BP rhythms in 938 healthy school children aged 5 to 18 years.142 When these methods were applied to children and adolescents with stage 2 to 4 CKD, a lower amplitude of circadian and all ultradian BP and heart rate rhythms (P<0.01) was found than in the healthy cohort.143 BP variability can also be calculated. Compared with mean BP values, BP variance over long- and short-term periods may be a better reflection of consequential biological dysfunction in BP regulatory mechanisms, such as alterations in the sympathetic nervous system.144 The standard deviation of BP during a 24-hour ABPM provides an account of short-term BP variability, whereas visit-to-visit BP variation is posited to reflect long-term variability.145–147 More long-term variability predicts LVH and cardiovascular events such as stroke,60,147 whereas short-term BP variability is associated with LVH in children.148 Another parameter calculated from ABPM is the AASI (see preceding section on target-organ damage). In adults, the AASI correlates with arterial stiffness (pulse-wave velocity)149 and predicts cardiovascular mortality.150 In children, the AASI was found to be elevated in hypertensive children.54,151 Although interesting, these advanced calculations remain feasible only in a research setting.
Interpretation
The standard parameters of mean BP level, load, and dipping are compared against normative pediatric values to determine normal or elevated BP. The smoothed age- and sex-specific 95th percentiles of Wühl et al,81 which were calculated from the original data from Soergel et al,111 are the preferred reference data (Appendix Tables A1 through A4). Differences in normative standards can lead to variability in diagnosis.108,133,152 BP loads in excess of 25% are generally considered abnormal, with increased loads associated with LVH.38,153 The circadian BP decline from day to night, termed dipping, should be ≥10%.154
Reproducibility
Although few studies of reproducibility of ABPM have been conducted in pediatric patients,155–157 most experts agree there is a moderate to strong correlation seen in serial ABPM measurement.158 Furthermore, ABPM is superior to casual BP measurement both in identifying children with target-organ damage and in determining adequate antihypertensive therapy, thus supporting the superiority of an ABPM-derived assignment of hypertension compared with casual BP in children, as in adults.34,41,148,157,159–164 However, outcome data linking ABPM in childhood or adolescence to cardiovascular disease in adulthood are not yet available.
Recommendations for Standard Application of ABPM in Pediatrics
The preceding sections have outlined the advantages of ABPM in specific clinical situations in the evaluation and management of pediatric hypertension, as well as the rationale for modification of the prior recommendations for interpretation of ABPM studies in children and adolescents. Although there remain some uncertainties with respect to ABPM in pediatrics,112 its benefits likely outweigh the uncertainties in most patients, particularly for initial diagnosis. Additionally, there are clearly disease states in which ABPM has been shown to be particularly useful, as summarized in Table 2 and discussed further in the online-only Data Supplement.
Table 2.
Conditions in Which ABPM May Be Particularly Helpful*
| Condition | Relevance of ABPM |
|---|---|
| Secondary hypertension | Elevated load, abnormal dipping and variability |
| Chronic kidney disease | Prevalence of hypertension, masked hypertension, association with target- organ changes and disease progression |
| Types 1 and 2 diabetes mellitus | Abnormal circadian variation, association with microalbuminuria and vascular changes |
| Obesity | Masked hypertension, correlation between BMI and hypertension severity, abnormal dipping, association with target-organ damage |
| Sleep apnea | Hypertension severity, abnormal circadian variation |
| Genetic syndromes Neurofibromatosis type 1 Turner syndrome Williams syndrome |
Abnormal BP patterns indicating secondary cause of hypertension, especially renal artery stenosis and aortic coarctation |
| Treated patients with hypertension | Response to antihypertensive medications and/or lifestyle changes |
| Hypertension research | Reduction in subject number in drug trials |
ABPM indicates ambulatory blood pressure monitoring; BMI, body mass index; and BP, blood pressure.
For a detailed discussion and references, see the online-only Data Supplement.
What follows is a synthesis of our recommendations for pediatric ABPM in list form, which we hope will prove useful to clinicians who obtain ABPM studies in children and adolescents.
-
Indications for routine performance of ABPM include the following:
-
To confirm the diagnosis of hypertension in a patient with hypertension according to casual BP measurements
Determine whether sustained hypertension or WCH exists
To evaluate for the presence of MH when there is a clinical suspicion of hypertension but normal or prehypertensive casual measurements
-
To assess BP patterns in high-risk patients
Assess for abnormal circadian variation in BP, such as blunted dipping or isolated sleep hypertension in patients with diabetes mellitus, CKD, solid organ transplants, and severe obesity with or without sleep-disordered breathing.
Assess the severity and persistence of BP elevation in patients at high risk for hypertensive target-organ damage.
-
To evaluate effectiveness of drug therapy for hypertension
Confirm BP control in treated patients, especially those with secondary forms of hypertension.
Evaluate for apparent drug-resistant hypertension.
Determine whether symptoms can be attributed to drug-related hypotension.
-
-
An ABPM device suitable for use in children should be selected.
Only devices that have been validated according to Association for the Advancement of Medical Instrumentation or British Hypertension Society standards should be used.
An oscillometric or auscultatory technique can be used.
Appropriate cuff sizes as recommended in the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents101a must be available for the device selected.
-
A standard approach to obtaining ABPM readings should be used.
ABPM should only be performed by personnel with specific training in the application of the device and interpretation of ABPM data in pediatric patients.
Monitors should be applied to the nondominant arm unless contraindicated (presence of a permanent dialysis access), or if a significant BP discrepancy between the extremities exists, the monitor should be placed on the arm with the higher BP.
Devices should be programmed to record BP every 15 to 20 minutes during waking hours and every 20 to 30 minutes during sleep.
After application, BP measured with the device should be compared with resting, clinic BP by the same technique used by the ambulatory device (auscultatory or oscillometric).
Patients should be instructed to record antihypertensive medication administration, activity, sleep, and wake times in a diary.
-
A sufficient number of valid BP recordings are needed for a study to be considered interpretable.
Minimum of 1 reading per hour, including during sleep
At least 40 to 50 readings for a full 24-hour report
65% to 75% of all possible BP readings for a partial day report (depends on frequency of recording programmed into the monitor)
-
ABPM recordings should be edited for outlying values.
Data should be inspected visually for gross inconsistencies that fall considerably outside the normal ranges for awake or asleep BP and heart rate for the patient’s age.
-
Values that fall outside of the following range should be discarded:
SBP 60 to 220 mm Hg
DBP 35 to 120 mm Hg
Heart rate 40 to 180 bpm
Pulse pressure 40 to 120 mm Hg
Ideally, the above limits should be programmed into the ABPM software to minimize subjective editing of ABPM data.
Any resting BP measurements made with the ABPM device immediately after application of the device should also be edited out.
-
Standard calculations should be reported.
Mean ambulatory SBP and DBP during the entire 24-hour awake and sleep periods.
BP load (percentage of readings above the ambulatory 95th percentile) for both SBP and DBP during the entire 24-hour awake and sleep periods.
Dipping (percent day/night difference) should be determined ([mean awake BP-mean sleep BP]/mean awake BP×100) for both SBP and DBP.
-
ABPM levels should be interpreted with appropriate pediatric normative data.
ABPM values should be compared with sex- and height-specific data obtained in large pediatric populations using similar techniques3 and not with resting BP levels.
A suggested schema for staging ABPM is included in Table 3. These are consensus rather than evidence-based recommendations because of a lack of pediatric cardiovascular outcome data based on ABPM.
Table 3.
Suggested Revised Schema for Staging of Ambulatory BP Levels in Children
| Classification | Office BP* | Mean Ambulatory SBP or DBP†,‡ | SBP or DBP Load, %‡,§ |
|---|---|---|---|
| Normal BP | <90th %tile | <95th %tile | <25 |
| White coat hypertension | ≥95th %tile | <95th %tile | <25 |
| Prehypertension | ≥90th %tile or >120/80 mm Hg | <95th %tile | ≥25 |
| Masked hypertension | <95th %tile | >95th %tile | ≥25 |
| Ambulatory hypertension|| | >95th %tile | >95th %tile | 25–50 |
| Severe ambulatory hypertension (at risk for end-organ damage) | >95th %tile | >95th %tile | >50 |
%tile indicates percentile; BP, blood pressure; DBP, diastolic blood pressure; and SBP, systolic blood pressure.
Based on National High Blood Pressure Education Program Task Force normative data.101a
Based on normative pediatric ABPM values in Appendix Tables A1 through A4.
For either the wake or sleep period of the study, or both.
For patients with elevated load but normal mean ambulatory BP and office BP that is either normal (<90th percentile) or hypertensive (≥95th percentile), no specific ambulatory BP classification can be assigned based on current evidence and expert consensus. These “unclassified” patients should be evaluated on a case-by-case basis, taking into account the presence of secondary hypertensiona or multiple cardiovascular risk factors.
Some clinicians may prefer the term sustained hypertension rather than ambulatory hypertension.
Interpretation of ABPM Studies
Building on an earlier proposed classification scheme by Lurbe et al,108 the 2008 AHA statement issued suggested criteria for classification of children as normotensive, white coat hypertensive, prehypertensive, masked hypertensive, and hypertensive.3 These recommended classifications incorporated the office BP reading and the mean ambulatory SBP. Of note, this scheme is different from that used to analyze ABPM studies in adults, which uses fixed BP levels as normal/abnormal, does not include a prehypertension category, and considers a slightly higher BP load of 30% to be abnormal.165
Since publication of the AHA statement in 2008, the field of pediatric ABPM has continued to advance rapidly, and several issues have arisen with respect to the suggested classification scheme in that document. Some of these issues have been raised formally through peer-reviewed publications in the pediatric hypertension literature, and some have become apparent as practitioners have attempted to apply the classification scheme clinically. These issues and potential solutions will be addressed in the following sections.
Prehypertension
Several concerns have been raised regarding the definition of prehypertension in the 2008 AHA statement. First, the definition mistakenly states that the office BP cut point for prehypertension is a BP >95th percentile, but the actual definition by the National High Blood Pressure Education Program is that prehypertension is office BP ≥90th percentile and <95th percentile, or >120/80 mm Hg.101a Thus, we have changed the definition of prehypertension in the classification scheme to office BP ≥90th percentile or >120/80 mm Hg, mean ambulatory BP <95th percentile but elevated BP loads.
The second concern with prehypertension as defined in the 2008 AHA statement is the lack of clinical evidence as to whether this actually corresponds to prehypertension as defined by the National High Blood Pressure Education Program. Only 1 recent study has examined ambulatory BP in pediatric patients with prehypertension based on office BP.78 Although the investigators demonstrated that prehypertensive patients had higher ambulatory BP than normotensive patients, they did not use the 2008 AHA criteria to classify the ambulatory BP studies and did not report whether the mean ambulatory BP values of the prehypertensive patients were <95th percentile according to pediatric ambulatory BP criteria. Interestingly, some of the patients with office prehypertension were indeed hypertensive by ABPM, a finding that would actually classify them as having MH.
Finally, as noted above, there is no corresponding concept of prehypertension when it comes to ABPM in adults. This may be related to the lack of incorporation of BP load into the analysis of ambulatory BP studies in adults in the more recent AHA recommendations for BP measurement.166 However, many pediatric hypertension experts believe that prehypertension on casual BP recordings with elevated load, despite normal means, may represent a higher-risk pattern. Therefore, we have decided to keep this category in the revised classification scheme.
Diastolic Hypertension
The classification scheme outlined in the 2008 AHA statement suggests that children undergoing ABPM should be classified on the basis of clinic and ambulatory SBP. Yet in routine clinical use of ABPM, it is apparent that some children have isolated diastolic hypertension. The frequency and significance of this are unknown; however, in at least 1 study, diastolic hypertension on ABPM has been shown to potentially signal the presence of underlying secondary causes of hypertension.167 This would be consistent with single-center studies that used office BP measurements, which have shown that children with primary hypertension tend to have isolated SBP elevation,168,169 and with a recent multicenter study that showed a high prevalence of DBP elevation in younger children with secondary hypertension.170 These data suggest that diastolic hypertension is important to identify from a diagnostic standpoint and suggest that DBP elevation should also be incorporated into the classification.
However, there are some issues related to ambulatory DBP that should be considered. Many ambulatory BP devices use the oscillometric technique, which has been shown to be less accurate in measuring DBP than SBP.171,172 Although this may not be true for all devices, it may in fact be responsible for the remarkable lack of DBP variation that was seen in the German pediatric ambulatory BP database (Figure).112 On the other hand, all indirect methods of BP measurement have inaccuracies for both SBP and DBP compared with direct intra-arterial measurements,173 so perhaps the widely held belief that automated devices are less accurate for DBP than SBP is erroneous.
One additional issue is that the DBP values found in the German pediatric ambulatory databases are fairly high: ≈80 to 81 mm Hg for the awake 90th percentile and 82 to 84 mm Hg for the awake 95th percentile (these are similar for boys and girls and, as noted above, are similar regardless of height).3 For younger children especially, sustained DBP above this value would almost certainly be considered hypertensive by most clinicians, and if one believes that the actual normative values should be lower than this for younger children, one would potentially miss patients with hypertension if DBP elevation were not included in the classification scheme. Thus, we have incorporated DBP into the revised ambulatory BP classification scheme.
Nocturnal Hypertension
Nocturnal hypertension has significant prognostic implications in certain patient populations, including adults and children with CKD and diabetes mellitus.80,174–178 It has also been cited as the most significant predictor of cardiovascular outcome in hypertensive adults.179 Furthermore, isolated nocturnal hypertension occurs commonly in other clinical situations in which ABPM has proven useful, particularly in solid organ transplantation.180
It is clear from these data that nocturnal hypertension is an important variable that should be incorporated into any ambulatory BP classification scheme. Thus, we believe that even patients with isolated abnormalities of sleep BP on ABPM should be considered as having MH and that abnormalities of sleep BP should be given the same weight as abnormalities of awake BP.
Mean Arterial Pressure
The majority of devices used to perform ABPM use the oscillometric technique, which directly measures mean arterial pressure (MAP) and back-calculates SBP and DBP by use of manufacturer-specific software algorithms. The resultant calculated SBP and DBP values have been shown to vary significantly compared with SBP and DBP values obtained by auscultation.173,181 It may be more appropriate to use MAP to classify the results of ABP studies, because this is the one BP parameter that is measured directly by most devices used to perform ABPM in children. Furthermore, treatment guided by ambulatory MAP has been shown to reduce the rate of progression of CKD in the recently published Effect of Strict Blood Pressure Control and ACE Inhibition on the Progression of CRF in Pediatric Patients (ESCAPE) trial,182 which further highlights the importance of this ambulatory BP parameter.
However, additional evidence would likely be needed before MAP could be adopted as the standard for classifying ambulatory BP studies. Most recent publications on ABPM and outcomes have reported their results based on ambulatory SBP and DBP. We have included the full German data set, including MAP values (Appendix Tables A1 through A4). We encourage investigators to begin examining the relationship between ambulatory MAP and both intermediate and long-term outcomes so that sufficient evidence can be generated to fully evaluate the possibility of incorporating MAP into the classification scheme.
Severe Ambulatory Hypertension
This diagnosis should be evaluated in the context of the mean ambulatory BP level. For instance, a subject with a mean BP level that is mildly elevated (eg, consistently at the 96th percentile) may have an increased load of >50%, but this may not represent as high a risk as the subject with load >50% and mean BP at significantly higher than the 95th percentile (eg, in the 99th percentile) or with “spikes” of BP to extremely high levels.
Uncategorized Patients
The classification scheme in the 2008 AHA statement does not provide guidance on how to categorize patients with 2 related patterns on ABPM: (1) office BP ≥95th percentile, normal mean ambulatory BP, and elevated BP loads; and (2) normal office BP (<90th percentile), normal mean ambulatory BP, but elevated ambulatory BP loads. Should these children be considered normotensive or masked hypertensive?
How to approach such “unclassified patients” probably depends on whether or not one agrees that the concept of BP load is a valid parameter to consider. BP load was initially adopted enthusiastically as a predictor of hypertensive target-organ damage,183 but more recent studies have not relied on BP load, and the most recent AHA guidelines for analysis of ABPM studies in adults do not incorporate BP load.166
Interestingly, the investigators of the Chronic Kidney Disease in Children study have decided to classify these children as having MH,178,184 which may be justifiable in patients with CKD, but further study is needed to validate this approach in other populations. We would recommend approaching such patients on a case-by-case basis, taking into account the presence or absence of underlying secondary causes of hypertension or specific cardiovascular risk factors.
Revised ABPM Classification
Although further study is needed to answer some of the above questions, we do believe that the classification scheme in the 2008 AHA statement can be simply modified to address some of the more obvious issues, including what to do about DBP, isolated nocturnal BP elevation, and the correct identification of children with prehypertension. We have summarized these modifications in Table 3.
Conclusions and Future Directions
Although much experience with pediatric ABPM has been gained since publication of the 2008 AHA scientific statement, much more work needs to be done. Specifically, there is an urgent need for more comprehensive normative ABPM data across sex, race, and age. Devices that can measure DBP more accurately may be useful in determining the true increase in DBP over age, because current norms indicate a flat DBP curve (Figure).112 Better data linking ABPM patterns to target-organ damage are also needed to improve our characterization of BP, because children with abnormal load, dipping, or a circadian pattern may be at risk for cardiovascular disease despite normal ABPM mean levels. Finally, additional data evaluating the efficacy of ABPM in measuring the effect of interventions and effectiveness of ABPM-driven BP control in reversing target-organ damage are needed.
Supplementary Material
Appendix
Table A1.
Normal Values for Ambulatory BP (mm Hg) for Healthy Boys by Height
| BP Percentile | Height, cm
|
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 120 | 125 | 130 | 135 | 140 | 145 | 150 | 155 | 160 | 165 | 170 | 175 | 180 | 185 | |
| 24-h SBP | ||||||||||||||
| 50th | 104.5 | 105.3 | 106.2 | 107.2 | 108.3 | 109.5 | 110.9 | 112.5 | 114.2 | 116.1 | 118.0 | 119.7 | 121.5 | 123.2 |
| 75th | 109.2 | 110.1 | 111.1 | 112.1 | 113.3 | 114.6 | 116.1 | 117.7 | 119.5 | 121.4 | 123.2 | 125.0 | 126.6 | 128.2 |
| 90th | 113.8 | 114.8 | 115.9 | 116.9 | 118.2 | 119.5 | 121.0 | 122.6 | 124.4 | 126.3 | 128.1 | 129.8 | 131.3 | 132.8 |
| 95th | 116.8 | 117.8 | 118.9 | 120.0 | 121.2 | 122.5 | 124.0 | 125.7 | 127.4 | 129.3 | 131.1 | 132.6 | 134.1 | 135.5 |
| 99th | 122.9 | 123.9 | 125.0 | 126.1 | 127.3 | 128.6 | 130.1 | 131.7 | 133.4 | 135.2 | 136.8 | 138.2 | 139.4 | 140.5 |
| Daytime SBP | ||||||||||||||
| 50th | 110.8 | 111.1 | 111.5 | 112.0 | 112.7 | 113.7 | 115.1 | 116.8 | 118.6 | 120.6 | 122.6 | 124.4 | 126.2 | 128.0 |
| 75th | 116.2 | 116.5 | 116.9 | 117.4 | 118.0 | 119.0 | 120.4 | 122.1 | 124.2 | 126.4 | 128.4 | 130.3 | 132.2 | 134.1 |
| 90th | 121.7 | 121.9 | 122.2 | 122.5 | 123.0 | 123.9 | 125.3 | 127.1 | 129.4 | 131.9 | 134.1 | 136.1 | 138.0 | 139.9 |
| 95th | 125.2 | 125.3 | 125.5 | 125.7 | 126.0 | 126.9 | 128.3 | 130.2 | 132.7 | 135.3 | 137.6 | 139.6 | 141.6 | 143.5 |
| 99th | 132.6 | 132.4 | 132.2 | 132.0 | 132.1 | 132.8 | 134.2 | 136.3 | 139.1 | 142.2 | 144.7 | 146.8 | 148.6 | 150.5 |
| Nighttime SBP | ||||||||||||||
| 50th | 93.6 | 94.6 | 95.6 | 96.7 | 97.9 | 99.0 | 100.1 | 101.3 | 102.6 | 104.1 | 105.6 | 107.2 | 108.7 | 110.2 |
| 75th | 98.6 | 99.8 | 101.0 | 102.3 | 103.6 | 104.7 | 105.9 | 107.1 | 108.4 | 109.9 | 111.5 | 113.1 | 114.6 | 116.1 |
| 90th | 103.3 | 104.8 | 106.3 | 107.8 | 109.3 | 110.6 | 111.8 | 113.0 | 114.3 | 115.7 | 117.2 | 118.8 | 120.3 | 121.8 |
| 95th | 106.3 | 107.9 | 109.7 | 111.4 | 113.0 | 114.4 | 115.7 | 116.8 | 118.1 | 119.4 | 120.9 | 122.4 | 123.9 | 125.3 |
| 99th | 112.1 | 114.2 | 116.5 | 118.7 | 120.8 | 122.5 | 123.8 | 124.9 | 126.0 | 127.1 | 128.4 | 129.6 | 131.0 | 132.2 |
| 24-h DBP | ||||||||||||||
| 50th | 65.6 | 65.9 | 66.1 | 66.4 | 66.6 | 66.9 | 67.1 | 67.2 | 67.3 | 67.5 | 67.6 | 67.8 | 68.0 | 68.2 |
| 75th | 69.7 | 69.9 | 70.2 | 70.4 | 70.6 | 70.8 | 71.0 | 71.1 | 71.2 | 71.3 | 71.5 | 71.7 | 71.8 | 71.9 |
| 90th | 73.9 | 74.1 | 74.2 | 74.4 | 74.5 | 74.7 | 74.8 | 74.8 | 74.9 | 75.1 | 75.3 | 75.4 | 75.5 | 75.6 |
| 95th | 76.7 | 76.8 | 76.9 | 76.9 | 77.0 | 77.1 | 77.1 | 77.2 | 77.3 | 77.5 | 77.7 | 77.8 | 77.9 | 78.0 |
| 99th | 82.7 | 82.5 | 82.3 | 82.1 | 81.9 | 81.8 | 81.8 | 81.8 | 81.9 | 82.2 | 82.5 | 82.7 | 82.9 | 83.0 |
| Daytime DBP | ||||||||||||||
| 50th | 72.3 | 72.3 | 72.2 | 72.1 | 72.1 | 72.1 | 72.1 | 72.1 | 72.2 | 72.3 | 72.6 | 72.8 | 73.1 | 73.4 |
| 75th | 76.5 | 76.4 | 76.3 | 76.2 | 76.0 | 76.0 | 75.9 | 75.9 | 76.0 | 76.2 | 76.5 | 76.8 | 77.2 | 77.5 |
| 90th | 80.2 | 80.1 | 79.9 | 79.7 | 79.5 | 79.4 | 79.3 | 79.3 | 79.4 | 79.7 | 80.0 | 80.5 | 80.9 | 81.3 |
| 95th | 82.4 | 82.2 | 82.0 | 81.8 | 81.5 | 81.4 | 81.2 | 81.2 | 81.3 | 81.7 | 82.1 | 82.6 | 83.1 | 83.6 |
| 99th | 86.5 | 86.2 | 85.9 | 85.6 | 85.2 | 85.0 | 84.8 | 84.8 | 85.0 | 85.4 | 86.0 | 86.6 | 87.3 | 87.9 |
| Nighttime DBP | ||||||||||||||
| 50th | 54.3 | 54.8 | 55.1 | 55.5 | 55.8 | 56.0 | 56.2 | 56.2 | 56.3 | 56.5 | 56.7 | 56.9 | 57.1 | 57.3 |
| 75th | 57.6 | 58.2 | 58.8 | 59.2 | 59.6 | 59.9 | 60.1 | 60.2 | 60.2 | 60.3 | 60.5 | 60.6 | 60.8 | 60.9 |
| 90th | 60.7 | 61.4 | 62.1 | 62.7 | 63.2 | 63.5 | 63.7 | 63.8 | 63.8 | 63.9 | 63.9 | 64.0 | 64.1 | 64.2 |
| 95th | 62.6 | 63.4 | 64.2 | 64.8 | 65.4 | 65.8 | 66.0 | 66.0 | 66.0 | 66.0 | 66.1 | 66.1 | 66.1 | 66.2 |
| 99th | 66.2 | 67.2 | 68.2 | 69.0 | 69.7 | 70.1 | 70.4 | 70.4 | 70.3 | 70.3 | 70.2 | 70.1 | 70.0 | 69.9 |
| 24-h MAP | ||||||||||||||
| 50th | 77.5 | 78.1 | 78.7 | 79.3 | 79.9 | 80.5 | 81.1 | 81.7 | 82.3 | 83.1 | 83.9 | 84.7 | 85.5 | 86.3 |
| 75th | 81.8 | 82.4 | 83.0 | 83.5 | 84.1 | 84.6 | 85.2 | 85.9 | 86.6 | 87.3 | 88.1 | 89.0 | 89.8 | 90.7 |
| 90th | 86.3 | 86.7 | 87.2 | 87.6 | 88.0 | 88.5 | 89.1 | 89.7 | 90.3 | 91.1 | 91.9 | 92.7 | 93.5 | 94.3 |
| 95th | 89.3 | 89.6 | 89.9 | 90.2 | 90.5 | 90.9 | 91.4 | 91.9 | 92.6 | 93.3 | 94.0 | 94.8 | 95.6 | 96.4 |
| 99th | 95.9 | 95.7 | 95.5 | 95.4 | 95.4 | 95.6 | 95.9 | 96.3 | 96.7 | 97.4 | 98.0 | 98.7 | 99.4 | 100.1 |
| Daytime MAP | ||||||||||||||
| 50th | 83.8 | 84.1 | 84.3 | 84.5 | 84.7 | 85.0 | 85.4 | 85.8 | 86.4 | 87.1 | 88.0 | 89.0 | 90.0 | 91.0 |
| 75th | 88.5 | 88.7 | 88.9 | 89.0 | 89.1 | 89.4 | 89.6 | 90.1 | 90.7 | 91.6 | 92.6 | 93.7 | 94.9 | 96.1 |
| 90th | 92.9 | 93.0 | 93.1 | 93.1 | 93.1 | 93.2 | 93.4 | 93.8 | 94.5 | 95.4 | 96.5 | 97.7 | 99.0 | 100.3 |
| 95th | 95.6 | 95.6 | 95.6 | 95.5 | 95.5 | 95.5 | 95.7 | 96.0 | 96.7 | 97.7 | 98.8 | 100.1 | 101.4 | 102.8 |
| 99th | 101.0 | 100.7 | 100.5 | 100.2 | 99.9 | 99.7 | 99.8 | 100.1 | 100.8 | 101.7 | 102.9 | 104.3 | 105.7 | 107.1 |
| Nighttime MAP | ||||||||||||||
| 50th | 66.8 | 67.6 | 68.3 | 69.0 | 69.6 | 70.1 | 70.6 | 71.2 | 71.9 | 72.7 | 73.6 | 74.5 | 75.4 | 76.2 |
| 75th | 71.0 | 71.9 | 72.7 | 73.4 | 73.9 | 74.4 | 74.9 | 75.4 | 76.0 | 76.8 | 77.6 | 78.3 | 79.1 | 79.8 |
| 90th | 75.9 | 76.6 | 77.3 | 77.9 | 78.3 | 78.6 | 78.9 | 79.2 | 79.7 | 80.3 | 80.9 | 81.5 | 82.1 | 82.7 |
| 95th | 79.5 | 80.0 | 80.5 | 80.9 | 81.2 | 81.3 | 81.4 | 81.5 | 81.9 | 82.3 | 82.8 | 83.3 | 83.8 | 84.3 |
| 99th | 88.4 | 88.1 | 87.8 | 87.6 | 87.2 | 86.7 | 86.3 | 86.0 | 86.0 | 86.1 | 86.3 | 86.5 | 86.8 | 87.0 |
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; and SBP, systolic blood pressure. Modified from Wuhl et al81 with permission of the publisher. Copyright © 2002, Lippincott Williams & Wilkins, Inc.
Table A2.
Normal Values for Ambulatory BP (mm Hg) for Healthy Girls by Height
| BP Percentile | Height, cm
|
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 120 | 125 | 130 | 135 | 140 | 145 | 150 | 155 | 160 | 165 | 170 | 175 | |
| 24-h SBP | ||||||||||||
| 50th | 104.0 | 105.0 | 106.0 | 106.8 | 107.6 | 108.7 | 109.9 | 111.2 | 112.4 | 113.7 | 115.0 | 116.4 |
| 75th | 108.2 | 109.3 | 110.3 | 111.2 | 112.1 | 113.2 | 114.6 | 115.9 | 117.0 | 118.0 | 119.2 | 120.4 |
| 90th | 112.0 | 113.2 | 114.3 | 115.3 | 116.2 | 117.4 | 118.7 | 120.0 | 121.0 | 121.8 | 122.8 | 123.8 |
| 95th | 114.3 | 115.6 | 116.7 | 117.7 | 118.7 | 119.9 | 121.2 | 122.5 | 123.3 | 124.1 | 124.9 | 125.8 |
| 99th | 118.8 | 120.1 | 121.3 | 122.4 | 123.4 | 124.6 | 126.0 | 127.1 | 127.7 | 128.2 | 128.8 | 129.3 |
| Daytime SBP | ||||||||||||
| 50th | 110.0 | 110.5 | 111.0 | 111.6 | 112.2 | 113.1 | 114.3 | 115.6 | 117.0 | 118.3 | 119.8 | 121.2 |
| 75th | 114.4 | 115.0 | 115.7 | 116.3 | 117.0 | 118.1 | 119.4 | 120.7 | 121.9 | 123.1 | 124.2 | 125.3 |
| 90th | 118.2 | 119.0 | 119.7 | 120.4 | 121.3 | 122.5 | 123.9 | 125.2 | 126.4 | 127.3 | 128.1 | 128.9 |
| 95th | 120.4 | 121.3 | 122.1 | 122.9 | 123.8 | 125.1 | 126.5 | 127.9 | 129.1 | 129.8 | 130.5 | 131.0 |
| 99th | 124.5 | 125.5 | 126.4 | 127.4 | 128.5 | 129.9 | 131.5 | 133.0 | 134.0 | 134.5 | 134.8 | 135.0 |
| Nighttime SBP | ||||||||||||
| 50th | 95.0 | 95.7 | 96.4 | 96.9 | 97.5 | 98.1 | 98.9 | 100.0 | 101.1 | 102.2 | 103.4 | 104.6 |
| 75th | 99.4 | 100.3 | 101.2 | 101.9 | 102.6 | 103.4 | 104.4 | 105.5 | 106.4 | 107.3 | 108.2 | 109.2 |
| 90th | 103.3 | 104.4 | 105.5 | 106.5 | 107.5 | 108.5 | 109.5 | 110.5 | 111.2 | 111.8 | 112.4 | 113.1 |
| 95th | 105.6 | 106.9 | 108.1 | 109.3 | 110.4 | 111.6 | 112.7 | 113.6 | 114.1 | 114.4 | 114.8 | 115.3 |
| 99th | 109.8 | 111.5 | 113.1 | 114.7 | 116.2 | 117.7 | 118.9 | 119.5 | 119.6 | 119.4 | 119.3 | 119.4 |
| 24-h DBP | ||||||||||||
| 50th | 65.9 | 65.9 | 66.0 | 66.1 | 66.2 | 66.3 | 66.5 | 66.7 | 67.0 | 67.4 | 68.0 | 68.6 |
| 75th | 68.6 | 68.9 | 69.2 | 69.5 | 69.8 | 70.1 | 70.4 | 70.6 | 70.7 | 71.0 | 71.3 | 71.6 |
| 90th | 70.9 | 71.4 | 71.9 | 72.4 | 72.9 | 73.4 | 73.8 | 74.0 | 74.1 | 74.2 | 74.4 | 74.5 |
| 95th | 72.2 | 72.8 | 73.4 | 74.1 | 74.7 | 75.3 | 75.7 | 76.0 | 76.1 | 76.2 | 76.2 | 76.2 |
| 99th | 74.6 | 75.3 | 76.2 | 77.1 | 77.9 | 78.7 | 79.3 | 79.7 | 79.9 | 79.9 | 79.9 | 79.7 |
| Daytime DBP | ||||||||||||
| 50th | 73.2 | 72.8 | 72.4 | 72.1 | 71.8 | 71.7 | 71.8 | 72.0 | 72.4 | 73.1 | 73.9 | 74.8 |
| 75th | 76.9 | 76.6 | 76.4 | 76.2 | 76.1 | 76.1 | 76.1 | 76.2 | 76.4 | 76.8 | 77.3 | 77.8 |
| 90th | 80.1 | 79.9 | 79.8 | 79.8 | 79.7 | 79.8 | 79.9 | 79.9 | 79.9 | 80.0 | 80.2 | 80.5 |
| 95th | 81.9 | 81.8 | 81.8 | 81.8 | 81.9 | 82.0 | 82.0 | 82.0 | 82.0 | 81.9 | 82.0 | 82.0 |
| 99th | 85.3 | 85.3 | 85.4 | 85.6 | 85.8 | 85.9 | 86.0 | 85.9 | 85.7 | 85.4 | 85.2 | 84.9 |
| Nighttime DBP | ||||||||||||
| 50th | 55.4 | 55.3 | 55.1 | 54.8 | 54.6 | 54.4 | 54.3 | 54.4 | 54.6 | 54.9 | 55.1 | 55.4 |
| 75th | 59.5 | 59.5 | 59.4 | 59.3 | 59.1 | 58.9 | 58.8 | 58.7 | 58.8 | 58.9 | 61.0 | 59.3 |
| 90th | 63.1 | 63.3 | 63.4 | 63.4 | 63.3 | 63.1 | 63.0 | 62.9 | 62.9 | 62.9 | 66.9 | 63.1 |
| 95th | 65.2 | 65.5 | 65.7 | 65.8 | 65.8 | 65.7 | 65.6 | 65.5 | 65.5 | 65.5 | 70.8 | 65.5 |
| 99th | 69.1 | 69.6 | 70.1 | 70.4 | 70.6 | 70.8 | 70.8 | 70.7 | 70.7 | 70.6 | 79.0 | 70.4 |
| 24-h MAP | ||||||||||||
| 50th | 77.2 | 77.8 | 78.3 | 78.7 | 79.2 | 79.7 | 80.2 | 80.8 | 81.5 | 82.3 | 83.1 | 84.0 |
| 75th | 80.6 | 81.2 | 81.8 | 82.4 | 82.9 | 83.5 | 84.1 | 84.7 | 85.3 | 85.9 | 86.6 | 87.4 |
| 90th | 83.6 | 84.2 | 84.9 | 85.5 | 86.1 | 86.7 | 87.3 | 87.9 | 88.4 | 88.9 | 89.5 | 90.1 |
| 95th | 85.3 | 86.0 | 86.7 | 87.4 | 88.0 | 88.6 | 89.2 | 89.7 | 90.2 | 90.6 | 91.1 | 91.7 |
| 99th | 88.5 | 89.2 | 89.9 | 90.6 | 91.3 | 91.9 | 92.5 | 93.0 | 93.3 | 93.6 | 94.0 | 94.5 |
| Daytime MAP | ||||||||||||
| 50th | 83.3 | 83.7 | 84.0 | 84.1 | 84.3 | 84.5 | 84.9 | 85.5 | 86.2 | 87.0 | 88.0 | 88.9 |
| 75th | 87.4 | 87.9 | 88.2 | 88.5 | 88.7 | 88.9 | 89.3 | 89.8 | 90.3 | 90.9 | 91.6 | 92.2 |
| 90th | 90.9 | 91.5 | 91.9 | 92.2 | 92.4 | 92.7 | 93.0 | 93.4 | 93.7 | 94.1 | 94.5 | 94.9 |
| 95th | 92.9 | 93.6 | 94.0 | 94.4 | 94.6 | 94.9 | 95.1 | 95.4 | 95.6 | 95.8 | 96.1 | 96.4 |
| 99th | 96.6 | 97.4 | 97.9 | 98.3 | 98.6 | 98.8 | 99.0 | 99.0 | 99.0 | 99.0 | 99.0 | 99.1 |
| Nighttime MAP | ||||||||||||
| 50th | 68.0 | 68.2 | 68.4 | 68.5 | 68.7 | 69.0 | 69.3 | 69.8 | 70.4 | 71.2 | 72.0 | 72.8 |
| 75th | 72.6 | 72.7 | 72.9 | 73.0 | 73.2 | 73.5 | 73.9 | 74.3 | 74.8 | 75.4 | 76.1 | 76.9 |
| 90th | 76.8 | 76.9 | 77.0 | 77.2 | 77.4 | 77.7 | 78.0 | 78.3 | 78.6 | 79.1 | 79.6 | 80.3 |
| 95th | 79.5 | 79.4 | 79.6 | 79.7 | 79.9 | 80.2 | 80.4 | 80.6 | 80.8 | 81.2 | 81.6 | 82.2 |
| 99th | 84.6 | 84.4 | 84.5 | 84.6 | 84.8 | 85.0 | 85.0 | 85.0 | 85.0 | 85.0 | 85.3 | 85.6 |
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; and SBP, systolic blood pressure. Modified from Wuhl et al81 with permission of the publisher. Copyright © 2002, Lippincott Williams & Wilkins, Inc.
Table A3.
Normal Values for Ambulatory BP (mm Hg) for Healthy Boys by Age
| BP Percentile | Age, y
|
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
| 24-h SBP | ||||||||||||
| 50th | 104.6 | 105.5 | 106.3 | 107.0 | 107.7 | 108.8 | 110.4 | 112.6 | 115.1 | 117.8 | 120.6 | 123.4 |
| 75th | 109.0 | 110.0 | 111.0 | 111.9 | 112.8 | 114.1 | 115.9 | 118.2 | 120.9 | 123.7 | 126.5 | 129.4 |
| 90th | 113.4 | 114.7 | 115.8 | 116.8 | 117.9 | 119.2 | 121.2 | 123.7 | 126.4 | 129.3 | 132.1 | 134.9 |
| 95th | 116.4 | 117.7 | 118.9 | 120.0 | 121.1 | 122.5 | 124.6 | 127.1 | 129.9 | 132.7 | 135.5 | 138.2 |
| 99th | 122.7 | 124.1 | 125.4 | 126.6 | 127.7 | 129.2 | 131.4 | 134.0 | 136.9 | 139.5 | 142.0 | 144.5 |
| Daytime SBP | ||||||||||||
| 50th | 111.1 | 111.5 | 111.9 | 112.2 | 112.6 | 113.4 | 114.9 | 117.0 | 119.5 | 122.3 | 125.3 | 128.2 |
| 75th | 115.7 | 116.3 | 116.8 | 117.3 | 117.9 | 118.8 | 120.5 | 122.9 | 125.6 | 128.5 | 131.5 | 134.6 |
| 90th | 120.1 | 120.9 | 121.6 | 122.2 | 122.9 | 124.0 | 125.9 | 128.4 | 131.2 | 134.2 | 137.3 | 140.4 |
| 95th | 122.9 | 123.8 | 124.6 | 125.3 | 126.1 | 127.3 | 129.3 | 131.8 | 134.7 | 137.7 | 140.8 | 143.9 |
| 99th | 128.5 | 129.6 | 130.6 | 131.5 | 132.3 | 133.7 | 135.8 | 138.6 | 141.5 | 144.4 | 147.4 | 150.4 |
| Nighttime SBP | ||||||||||||
| 50th | 95.0 | 95.5 | 96.1 | 96.7 | 97.3 | 98.1 | 99.4 | 101.2 | 103.4 | 105.8 | 108.3 | 110.9 |
| 75th | 99.2 | 100.2 | 101.1 | 102.0 | 102.9 | 103.9 | 105.3 | 107.1 | 109.3 | 111.9 | 114.4 | 116.9 |
| 90th | 103.4 | 104.9 | 106.2 | 107.5 | 108.5 | 109.6 | 111.0 | 112.8 | 115.0 | 117.5 | 120.0 | 122.5 |
| 95th | 106.3 | 108.0 | 109.6 | 111.0 | 112.1 | 113.2 | 114.6 | 116.3 | 118.6 | 121.0 | 123.4 | 125.9 |
| 99th | 112.3 | 114.6 | 116.7 | 118.4 | 119.6 | 120.7 | 121.9 | 123.4 | 125.5 | 127.8 | 130.1 | 132.3 |
| 24-h DBP | ||||||||||||
| 50th | 65.3 | 65.7 | 66.1 | 66.3 | 66.5 | 66.6 | 66.9 | 67.2 | 67.4 | 67.7 | 68.1 | 68.6 |
| 75th | 68.8 | 69.3 | 69.6 | 69.9 | 70.0 | 70.2 | 70.5 | 70.8 | 71.0 | 71.4 | 71.8 | 72.3 |
| 90th | 72.2 | 72.6 | 73.0 | 73.2 | 73.3 | 73.4 | 73.7 | 74.0 | 74.3 | 74.6 | 75.1 | 75.6 |
| 95th | 74.4 | 74.8 | 75.1 | 75.2 | 75.3 | 75.4 | 75.7 | 75.9 | 76.2 | 76.6 | 77.0 | 77.5 |
| 99th | 78.9 | 79.0 | 79.1 | 79.1 | 79.1 | 79.1 | 79.3 | 79.6 | 79.9 | 80.2 | 80.7 | 81.3 |
| Daytime DBP | ||||||||||||
| 50th | 72.2 | 72.4 | 72.5 | 72.5 | 72.3 | 72.1 | 72.0 | 72.0 | 72.2 | 72.5 | 73.0 | 73.5 |
| 75th | 75.9 | 76.1 | 76.3 | 76.4 | 76.2 | 76.0 | 76.0 | 76.0 | 76.2 | 76.5 | 77.0 | 77.6 |
| 90th | 79.1 | 79.3 | 79.7 | 79.8 | 79.7 | 79.5 | 79.5 | 79.5 | 79.7 | 80.0 | 80.6 | 81.3 |
| 95th | 81.0 | 81.3 | 81.6 | 81.8 | 81.7 | 81.5 | 81.5 | 81.6 | 81.7 | 82.1 | 82.8 | 83.5 |
| 99th | 84.5 | 84.8 | 85.2 | 85.5 | 85.4 | 85.3 | 85.3 | 85.4 | 85.6 | 86.1 | 86.8 | 87.7 |
| Nighttime DBP | ||||||||||||
| 50th | 55.0 | 55.3 | 55.5 | 55.7 | 55.8 | 55.8 | 55.9 | 56.0 | 56.3 | 56.5 | 56.8 | 57.1 |
| 75th | 58.5 | 59.1 | 59.5 | 59.8 | 60.0 | 60.0 | 60.0 | 60.1 | 60.3 | 60.5 | 60.7 | 60.9 |
| 90th | 62.3 | 63.2 | 63.8 | 64.2 | 64.3 | 64.2 | 64.1 | 64.1 | 64.1 | 64.2 | 64.3 | 64.3 |
| 95th | 65.1 | 66.1 | 66.8 | 67.1 | 67.1 | 66.9 | 66.7 | 66.5 | 66.5 | 66.5 | 66.4 | 66.4 |
| 99th | 71.6 | 72.7 | 73.5 | 73.5 | 73.2 | 72.6 | 71.9 | 71.4 | 71.1 | 70.8 | 70.6 | 70.3 |
| 24-h MAP | ||||||||||||
| 50th | 77.4 | 77.9 | 78.7 | 79.3 | 79.7 | 80.2 | 80.8 | 81.7 | 82.7 | 83.8 | 85.1 | 86.4 |
| 75th | 81.4 | 81.9 | 82.7 | 83.4 | 83.8 | 84.3 | 85.0 | 85.9 | 86.9 | 88.0 | 89.3 | 90.5 |
| 90th | 85.5 | 86.0 | 86.8 | 87.4 | 87.9 | 88.3 | 88.9 | 89.7 | 90.6 | 91.6 | 92.7 | 93.9 |
| 95th | 88.3 | 88.7 | 89.5 | 90.0 | 90.4 | 90.8 | 91.3 | 91.9 | 92.7 | 93.7 | 94.7 | 95.7 |
| 99th | 94.3 | 94.6 | 95.1 | 95.4 | 95.6 | 95.7 | 95.8 | 96.2 | 96.7 | 97.3 | 98.1 | 98.9 |
| Daytime MAP | ||||||||||||
| 50th | 83.5 | 84.1 | 84.5 | 84.8 | 84.9 | 85.0 | 85.3 | 85.9 | 86.8 | 88.0 | 89.4 | 90.8 |
| 75th | 87.5 | 88.2 | 88.8 | 89.2 | 89.4 | 89.5 | 89.9 | 90.6 | 91.5 | 92.7 | 94.2 | 95.7 |
| 90th | 91.3 | 92.1 | 92.8 | 93.3 | 93.5 | 93.7 | 94.0 | 94.7 | 95.6 | 96.8 | 98.3 | 99.8 |
| 95th | 93.6 | 94.5 | 95.3 | 95.8 | 96.1 | 96.2 | 96.5 | 97.1 | 98.0 | 99.2 | 100.6 | 102.1 |
| 99th | 98.2 | 99.2 | 100.1 | 100.7 | 101.0 | 101.0 | 101.2 | 101.6 | 102.4 | 103.4 | 104.7 | 106.1 |
| Nighttime MAP | ||||||||||||
| 50th | 66.7 | 67.7 | 68.6 | 69.2 | 69.7 | 70.0 | 70.5 | 71.2 | 72.1 | 73.1 | 74.0 | 74.9 |
| 75th | 70.5 | 71.7 | 72.8 | 73.5 | 74.1 | 74.5 | 75.0 | 75.6 | 76.4 | 77.2 | 78.0 | 78.6 |
| 90th | 74.7 | 76.0 | 77.2 | 78.1 | 78.6 | 78.9 | 79.3 | 79.7 | 80.3 | 80.8 | 81.3 | 81.7 |
| 95th | 77.6 | 79.0 | 80.2 | 81.1 | 81.6 | 81.8 | 82.0 | 82.3 | 82.6 | 82.9 | 83.2 | 83.4 |
| 99th | 84.1 | 85.7 | 86.9 | 87.6 | 87.8 | 87.7 | 87.4 | 87.1 | 86.9 | 86.8 | 86.6 | 86.4 |
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; and SBP, systolic blood pressure. Modified from Wuhl et al81 with permission of the publisher. Copyright © 2002, Lippincott Williams & Wilkins, Inc.
Table A4.
Normal Values for Ambulatory BP (mm Hg) for Healthy Girls by Age
| BP Percentile | Age, y
|
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
| 24-h SBP | ||||||||||||
| 50th | 102.8 | 104.1 | 105.3 | 106.5 | 107.6 | 108.7 | 109.7 | 110.7 | 111.8 | 112.8 | 113.8 | 114.8 |
| 75th | 107.8 | 109.1 | 110.4 | 111.5 | 112.6 | 113.6 | 114.7 | 115.7 | 116.7 | 117.6 | 118.4 | 119.2 |
| 90th | 112.3 | 113.7 | 115.0 | 116.1 | 117.2 | 118.2 | 119.2 | 120.2 | 121.2 | 121.9 | 122.6 | 123.2 |
| 95th | 114.9 | 116.4 | 117.7 | 118.9 | 120.0 | 121.1 | 122.1 | 123.0 | 123.9 | 124.5 | 125.0 | 125.6 |
| 99th | 119.9 | 121.5 | 123.0 | 124.3 | 125.5 | 126.5 | 127.5 | 128.4 | 129.0 | 129.5 | 129.7 | 130.0 |
| Daytime SBP | ||||||||||||
| 50th | 108.4 | 109.5 | 110.6 | 111.5 | 112.4 | 113.3 | 114.2 | 115.3 | 116.4 | 117.5 | 118.6 | 119.6 |
| 75th | 113.8 | 114.9 | 115.9 | 116.8 | 117.6 | 118.5 | 119.5 | 120.6 | 121.7 | 122.6 | 123.5 | 124.3 |
| 90th | 118.3 | 119.5 | 120.6 | 121.5 | 122.4 | 123.3 | 124.3 | 125.3 | 126.4 | 127.2 | 127.9 | 128.5 |
| 95th | 120.9 | 122.2 | 123.3 | 124.3 | 125.2 | 126.2 | 127.2 | 128.2 | 129.2 | 129.9 | 130.4 | 130.9 |
| 99th | 125.6 | 127.1 | 128.4 | 129.6 | 130.6 | 131.7 | 132.7 | 133.7 | 134.5 | 135.0 | 135.2 | 135.4 |
| Nighttime SBP | ||||||||||||
| 50th | 94.8 | 95.6 | 96.2 | 96.8 | 97.5 | 98.2 | 99.0 | 99.7 | 100.5 | 101.3 | 102.0 | 102.9 |
| 75th | 100.2 | 101.1 | 101.8 | 102.5 | 103.2 | 104.0 | 104.7 | 105.2 | 105.8 | 106.3 | 106.8 | 107.3 |
| 90th | 105.3 | 106.3 | 107.2 | 108.0 | 108.8 | 109.5 | 110.1 | 110.4 | 110.7 | 110.9 | 111.0 | 111.2 |
| 95th | 108.4 | 109.6 | 110.6 | 111.5 | 112.3 | 113.0 | 113.5 | 113.6 | 113.7 | 113.6 | 113.5 | 113.5 |
| 99th | 114.5 | 116.0 | 117.3 | 118.4 | 119.3 | 119.9 | 120.1 | 119.8 | 119.4 | 118.8 | 118.2 | 117.8 |
| 24-h DBP | ||||||||||||
| 50th | 65.5 | 65.6 | 65.8 | 65.9 | 66.0 | 66.2 | 66.4 | 66.6 | 67.0 | 67.2 | 67.5 | 67.7 |
| 75th | 68.9 | 69.1 | 69.2 | 69.3 | 69.5 | 69.8 | 70.0 | 70.4 | 70.8 | 71.1 | 71.2 | 71.4 |
| 90th | 72.1 | 72.2 | 72.3 | 72.4 | 72.6 | 72.9 | 73.2 | 73.7 | 74.1 | 74.4 | 74.6 | 74.7 |
| 95th | 74.0 | 74.1 | 74.2 | 74.2 | 74.4 | 74.7 | 75.1 | 75.6 | 76.1 | 76.4 | 76.6 | 76.7 |
| 99th | 77.6 | 77.6 | 77.6 | 77.6 | 77.7 | 78.0 | 78.4 | 79.1 | 79.7 | 80.1 | 80.4 | 80.5 |
| Daytime DBP | ||||||||||||
| 50th | 72.6 | 72.6 | 72.4 | 72.2 | 72.0 | 71.8 | 71.8 | 72.1 | 72.4 | 72.8 | 73.2 | 73.5 |
| 75th | 76.7 | 76.6 | 76.5 | 76.3 | 76.0 | 75.9 | 75.9 | 76.2 | 76.5 | 76.8 | 77.0 | 77.2 |
| 90th | 80.2 | 80.2 | 80.0 | 79.8 | 79.5 | 79.3 | 79.4 | 79.6 | 80.0 | 80.2 | 80.3 | 80.3 |
| 95th | 82.3 | 82.2 | 82.1 | 81.8 | 81.5 | 81.3 | 81.4 | 81.6 | 82.0 | 82.2 | 82.2 | 82.1 |
| 99th | 86.1 | 86.0 | 85.8 | 85.5 | 85.2 | 85.0 | 85.0 | 85.3 | 85.6 | 85.7 | 85.6 | 85.4 |
| Nighttime DBP | ||||||||||||
| 50th | 56.4 | 55.9 | 55.5 | 55.1 | 54.8 | 54.6 | 54.3 | 54.2 | 54.3 | 54.5 | 54.9 | 55.3 |
| 75th | 61.1 | 60.6 | 60.1 | 59.7 | 59.4 | 59.2 | 58.9 | 58.7 | 58.7 | 58.7 | 58.8 | 59.1 |
| 90th | 65.6 | 65.1 | 64.6 | 64.1 | 63.8 | 63.7 | 63.4 | 63.1 | 62.9 | 62.8 | 62.8 | 62.8 |
| 95th | 68.5 | 67.9 | 67.4 | 66.9 | 66.6 | 66.5 | 66.2 | 65.9 | 65.6 | 65.4 | 65.3 | 65.2 |
| 99th | 74.2 | 73.6 | 72.9 | 72.4 | 72.2 | 72.0 | 71.8 | 71.4 | 71.1 | 70.7 | 70.3 | 70.0 |
| 24-h MAP | ||||||||||||
| 50th | 77.5 | 78.0 | 78.4 | 78.8 | 79.2 | 79.6 | 80.2 | 80.9 | 81.5 | 82.2 | 82.7 | 83.0 |
| 75th | 81.2 | 81.7 | 82.1 | 82.5 | 82.9 | 83.3 | 84.0 | 84.7 | 85.4 | 86.0 | 86.5 | 86.8 |
| 90th | 84.6 | 85.0 | 85.4 | 85.7 | 86.1 | 86.5 | 87.1 | 87.9 | 88.6 | 89.2 | 89.7 | 89.9 |
| 95th | 86.6 | 87.0 | 87.3 | 87.6 | 87.9 | 88.3 | 88.9 | 89.7 | 90.5 | 91.0 | 91.5 | 91.7 |
| 99th | 90.5 | 90.8 | 90.9 | 91.0 | 91.2 | 91.6 | 92.2 | 93.0 | 93.7 | 94.2 | 94.6 | 94.8 |
| Daytime MAP | ||||||||||||
| 50th | 83.7 | 83.9 | 84.0 | 84.1 | 84.2 | 84.4 | 84.7 | 85.2 | 85.9 | 86.5 | 87.1 | 87.7 |
| 75th | 88.2 | 88.3 | 88.4 | 88.4 | 88.4 | 88.5 | 88.9 | 89.4 | 90.1 | 90.8 | 91.4 | 91.9 |
| 90th | 92.2 | 92.2 | 92.2 | 92.1 | 92.0 | 92.1 | 92.4 | 93.0 | 93.6 | 94.3 | 94.8 | 95.4 |
| 95th | 94.6 | 94.5 | 94.4 | 94.2 | 94.1 | 94.2 | 94.4 | 95.0 | 95.6 | 96.2 | 96.8 | 97.3 |
| 99th | 99.0 | 98.7 | 98.5 | 98.2 | 97.9 | 97.9 | 98.1 | 98.6 | 99.2 | 99.7 | 100.2 | 100.7 |
| Nighttime MAP | ||||||||||||
| 50th | 68.7 | 68.8 | 68.8 | 68.8 | 68.9 | 69.1 | 69.3 | 69.6 | 70.1 | 70.6 | 71.2 | 71.8 |
| 75th | 73.0 | 73.1 | 73.1 | 73.2 | 73.4 | 73.6 | 73.8 | 74.1 | 74.5 | 74.9 | 75.4 | 75.9 |
| 90th | 76.9 | 77.0 | 77.1 | 77.2 | 77.4 | 77.6 | 77.8 | 78.0 | 78.3 | 78.6 | 78.9 | 79.3 |
| 95th | 79.2 | 79.4 | 79.6 | 79.7 | 79.8 | 80.1 | 80.2 | 80.3 | 80.5 | 80.7 | 80.9 | 81.2 |
| 99th | 83.8 | 84.1 | 84.2 | 84.3 | 84.5 | 84.6 | 84.7 | 84.6 | 84.6 | 84.6 | 84.6 | 84.7 |
BP indicates blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; and SBP, systolic blood pressure. Modified from Wuhl et al81 with permission of the publisher. Copyright © 2002, Lippincott Williams & Wilkins, Inc.
Disclosures
Writing Group Disclosures
| Writing Group Member |
Employment | Research Grant |
Other Research Support |
Speakers’ Bureau/ Honoraria |
Expert Witness |
Ownership Interest |
Consultant/ Advisory Board |
Other |
|---|---|---|---|---|---|---|---|---|
| Joseph T. Flynn | Seattle Children’s Hospital | None | None | None | None | None | None | None |
| Stephen R. Daniels | University of Colorado | None | None | None | None | None | None | None |
| Laura L. Hayman | University of Massachusetts | None | None | None | None | None | None | None |
| David M. Maahs | University of Colorado, Denver | Abbott Diabetes Care†; Eli Lilly & Co† | None | None | None | None | None | None |
| Brian W. McCrindle | The Hospital for Sick Children | None | None | None | None | None | None | None |
| Mark Mitsnefes | Cincinnati Children’s Hospital | None | None | None | None | None | None | None |
| Elaine M. Urbina | Cincinnati Children’s Hospital | NHLBI† | None | None | None | None | None | None |
| Justin P. Zachariah | Boston’s Children’s Hospital Heart Foundation/Harvard Medical School |
None | None | None | None | None | None | None |
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives $10 000 or more during any 12-month period, or 5% or more of the person’s gross income; or (2) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
Significant.
Reviewer Disclosures
| Reviewer | Employment | Research Grant |
Other Research Support |
Speakers’ Bureau/ Honoraria |
Expert Witness |
Ownership Interest |
Consultant/ Advisory Board |
Other |
|---|---|---|---|---|---|---|---|---|
| Rae-Ellen W. Kavey | University of Rochester | None | None | None | None | None | None | None |
| Karen L. Redwine | Arkansas Children’s Hospital | UAMS Translational Research Institute (KL2RR029883/1UL1RR029884)† | None | None | None | None | None | None |
| Joshua Samuels | University of Texas Health Science Center at Houston | None | None | None | None | None | None | None |
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all reviewers are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives $10 000 or more during any 12-month period, or 5% or more of the person’s gross income; or (2) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
Significant.
Footnotes
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This statement was approved by the American Heart Association Science Advisory and Coordinating Committee on December 20, 2013. A copy of the document is available at http://my.americanheart.org/statements by selecting either the “By Topic” link or the “By Publication Date” link. To purchase additional reprints, call 843-216-2533 or kelle.ramsay@wolterskluwer.com.
The online-only Data Supplement is available with this article at http://hyper.ahajournals.org/lookup/suppl/doi:10.1161/HYP.0000000000000007/-/DC1.
References
- 1.Portman RJ, Yetman RJ. Clinical uses of ambulatory blood pressure monitoring. Pediatr Nephrol. 1994;8:367–376. doi: 10.1007/BF00866367. [DOI] [PubMed] [Google Scholar]
- 2.Flynn JT, Urbina EM. Pediatric ambulatory blood pressure monitoring: indications and interpretations. J Clin Hypertens (Greenwich) 2012;14:372–382. doi: 10.1111/j.1751-7176.2012.00655.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Urbina E, Alpert B, Flynn J, Hayman L, Harshfield GA, Jacobson M, Mahoney L, McCrindle B, Mietus-Snyder M, Steinberger J, Daniels S. Ambulatory blood pressure monitoring in children and adolescents: recommendations for standard assessment: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the Council on Cardiovascular Disease in the Young and the Council for High Blood Pressure Research. Hypertension. 2008;52:433–451. doi: 10.1161/HYPERTENSIONAHA.108.190329. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva, Switzerland: World Health Organization; 2009. [Accessed February 17, 2014]. http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. [Google Scholar]
- 5.Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Judd SE, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Mackey RH, Magid DJ, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Mussolino ME, Neumar RW, Nichol G, Pandey DK, Paynter NP, Reeves MJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Wong ND, Woo D, Turner MB on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–e292. doi: 10.1161/01.cir.0000441139.02102.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kannel WB. Hypertensive risk assessment: cardiovascular risk factors and hypertension. J Clin Hypertens (Greenwich) 2004;6:393–399. doi: 10.1111/j.1524-6175.2004.03605.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Din-Dzietham R, Liu Y, Bielo MV, Shamsa F. High blood pressure trends in children and adolescents in national surveys, 1963 to 2002. Circulation. 2007;116:1488–1496. doi: 10.1161/CIRCULATIONAHA.106.683243. [DOI] [PubMed] [Google Scholar]
- 8.Muntner P, He J, Cutler JA, Wildman RP, Whelton PK. Trends in blood pressure among children and adolescents. JAMA. 2004;291:2107–2113. doi: 10.1001/jama.291.17.2107. [DOI] [PubMed] [Google Scholar]
- 9.Gurven M, Blackwell AD, Rodriguez DE, Stieglitz J, Kaplan H. Does blood pressure inevitably rise with age? Longitudinal evidence among forager-horticulturalists. Hypertension. 2012;60:25–33. doi: 10.1161/HYPERTENSIONAHA.111.189100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shi Y, de Groh M, Morrison H. Increasing blood pressure and its associated factors in Canadian children and adolescents from Canadian Health Measures Survey. BMC Public Health. 2012;12:388. doi: 10.1186/1471-2458-12-388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McNiece KL, Poffenbarger TS, Turner JL, Franco KD, Sorof JM, Portman RJ. Prevalence of hypertension and pre-hypertension among adolescents. J Pediatr. 2007;150:640–644. 644.e641. doi: 10.1016/j.jpeds.2007.01.052. [DOI] [PubMed] [Google Scholar]
- 12.Falkner B, Gidding SS, Portman R, Rosner B. Blood pressure variability and classification of prehypertension and hypertension in adolescence. Pediatrics. 2008;122:238–242. doi: 10.1542/peds.2007-2776. [DOI] [PubMed] [Google Scholar]
- 13.Freedman DS, Goodman A, Contreras OA, DasMahapatra P, Srinivasan SR, Berenson GS. Secular trends in BMI and blood pressure among children and adolescents: the Bogalusa Heart Study. Pediatrics. 2012;130:e159–e166. doi: 10.1542/peds.2011-3302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chiolero A, Bovet P, Paradis G, Paccaud F. Has blood pressure increased in children in response to the obesity epidemic? Pediatrics. 2007;119:544–553. doi: 10.1542/peds.2006-2136. [DOI] [PubMed] [Google Scholar]
- 15.Tracy RE, Newman WP, 3rd, Wattigney WA, Srinivasan SR, Strong JP, Berenson GS. Histologic features of atherosclerosis and hypertension from autopsies of young individuals in a defined geographic population: the Bogalusa Heart Study. Atherosclerosis. 1995;116:163–179. doi: 10.1016/0021-9150(95)05525-2. [DOI] [PubMed] [Google Scholar]
- 16.Homma S, Ishii T, Malcom GT, Zieske AW, Strong JP, Tsugane S, Hirose N. Histopathological modifications of early atherosclerotic lesions by risk factors: findings in PDAY subjects. Atherosclerosis. 2001;156:389–399. doi: 10.1016/s0021-9150(00)00669-9. [DOI] [PubMed] [Google Scholar]
- 17.Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. . Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. 2011;128(suppl 5):S213–S256. doi: 10.1542/peds.2009-2107C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Metoki H, Ohkubo T, Kikuya M, Asayama K, Obara T, Hara A, Hirose T, Hashimoto J, Totsune K, Hoshi H, Satoh H, Imai Y. Prognostic significance of night-time, early morning, and daytime blood pressures on the risk of cerebrovascular and cardiovascular mortality: the Ohasama study. J Hypertens. 2006;24:1841–1848. doi: 10.1097/01.hjh.0000242409.65783.fb. [DOI] [PubMed] [Google Scholar]
- 19.Juonala M, Magnussen CG, Venn A, Dwyer T, Burns TL, Davis PH, Chen W, Srinivasan SR, Daniels SR, Kahönen M, Laitinen T, Taittonen L, Berenson GS, Viikari JS, Raitakari OT. Influence of age on associations between childhood risk factors and carotid intima-media thickness in adulthood: the Cardiovascular Risk in Young Finns Study, the Childhood Determinants of Adult Health Study, the Bogalusa Heart Study, and the Muscatine Study for the international Childhood Cardiovascular Cohort (i3C) Consortium. Circulation. 2010;122:2514–2520. doi: 10.1161/CIRCULATIONAHA.110.966465. [DOI] [PubMed] [Google Scholar]
- 20.Koivistoinen T, Hutri-Kähönen N, Juonala M, Aatola H, Kööbi T, Lehtimäki T, Viikari JS, Raitakari OT, Kähönen M. Metabolic syndrome in childhood and increased arterial stiffness in adulthood: the Cardiovascular Risk in Young Finns Study. Ann Med. 2011;43:312–319. doi: 10.3109/07853890.2010.549145. [DOI] [PubMed] [Google Scholar]
- 21.Li X, Li S, Ulusoy E, Chen W, Srinivasan SR, Berenson GS. Childhood adiposity as a predictor of cardiac mass in adulthood: the Bogalusa Heart Study. Circulation. 2004;110:3488–3492. doi: 10.1161/01.CIR.0000149713.48317.27. [DOI] [PubMed] [Google Scholar]
- 22.Ayer JG, Harmer JA, Nakhla S, Xuan W, Ng MKC, Raitakari OT, Marks GB, Celermajer DS. HDL-cholesterol, blood pressure, and asymmetric dimethylarginine are significantly associated with arterial wall thickness in children. Arterioscler Thromb Vasc Biol. 2009;29:943–949. doi: 10.1161/ATVBAHA.109.184184. [DOI] [PubMed] [Google Scholar]
- 23.Urbina EM, Kimball TR, McCoy CE, Khoury PR, Daniels SR, Dolan LM. Youth with obesity and obesity-related type 2 diabetes mellitus demonstrate abnormalities in carotid structure and function. Circulation. 2009;119:2913–2919. doi: 10.1161/CIRCULATIONAHA.108.830380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Whincup PH, Gilg JA, Donald AE, Katterhorn M, Oliver C, Cook DG, Deanfield JE. Arterial distensibility in adolescents: the influence of adiposity, the metabolic syndrome, and classic risk factors. Circulation. 2005;112:1789–1797. doi: 10.1161/CIRCULATIONAHA.104.532663. [DOI] [PubMed] [Google Scholar]
- 25.Urbina EM, Kimball TR, Khoury PR, Daniels SR, Dolan LM. Increased arterial stiffness is found in adolescents with obesity or obesity-related type 2 diabetes mellitus. J Hypertens. 2010;28:1692–1698. doi: 10.1097/HJH.0b013e32833a6132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Reusz GS, Cseprekal O, Temmar M, Kis E, Cherif AB, Thaleb A, Fekete A, Szabó AJ, Benetos A, Salvi P. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension. 2010;56:217–224. doi: 10.1161/HYPERTENSIONAHA.110.152686. [DOI] [PubMed] [Google Scholar]
- 27.Lurbe E, Torro I, Garcia-Vicent C, Alvarez J, Fernández-Fornoso JA, Redon J. Blood pressure and obesity exert independent influences on pulse wave velocity in youth. Hypertension. 2012;60:550–555. doi: 10.1161/HYPERTENSIONAHA.112.194746. [DOI] [PubMed] [Google Scholar]
- 28.Urbina EM, Khoury PR, McCoy C, Daniels SR, Kimball TR, Dolan LM. Cardiac and vascular consequences of pre-hypertension in youth. J Clin Hypertens. 2011;13:332–342. doi: 10.1111/j.1751-7176.2011.00471.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sorof JM, Alexandrov AV, Cardwell G, Portman RJ. Carotid artery intimal-medial thickness and left ventricular hypertrophy in children with elevated blood pressure. Pediatrics. 2003;111:61–66. doi: 10.1542/peds.111.1.61. [DOI] [PubMed] [Google Scholar]
- 30.Urbina EM, Dolan LM, McCoy CE, Khoury PR, Daniels SR, Kimball TR. Relationship between elevated arterial stiffness and increased left ventricular mass in adolescents and young adults. J Pediatr. 2011;158:715–721. doi: 10.1016/j.jpeds.2010.12.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Verdecchia P, Carini G, Circo A, Dovellini E, Giovannini E, Lombardo M, Solinas P, Gorini M, Maggioni AP. Left ventricular mass and cardiovascular morbidity in essential hypertension: the MAVI study. J Am Coll Cardiol. 2001;38:1829–1835. doi: 10.1016/s0735-1097(01)01663-1. [DOI] [PubMed] [Google Scholar]
- 32.Lande MB, Meagher CC, Fisher SG, Belani P, Wang H, Rashid M. Left ventricular mass index in children with white coat hypertension. J Pediatr. 2008;153:50–54. doi: 10.1016/j.jpeds.2008.01.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hanevold C, Waller J, Daniels S, Portman R, Sorof J International Pediatric Hypertension Association. The effects of obesity, gender, and ethnic group on left ventricular hypertrophy and geometry in hypertensive children: a collaborative study of the International Pediatric Hypertension Association [published correction appears in Pediatrics. 2005;115:1118] Pediatrics. 2004;113:328–333. doi: 10.1542/peds.113.2.328. [DOI] [PubMed] [Google Scholar]
- 34.Stabouli S, Kotsis V, Rizos Z, Toumanidis S, Karagianni C, Constantopoulos A, Zakopoulos N. Left ventricular mass in normotensive, prehypertensive and hypertensive children and adolescents. Pediatr Nephrol. 2009;24:1545–1551. doi: 10.1007/s00467-009-1165-2. [DOI] [PubMed] [Google Scholar]
- 35.Wong LJ, Kupferman JC, Prohovnik I, Kirkham FJ, Goodman S, Paterno K, Sharma M, Brosgol Y, Pavlakis SG. Hypertension impairs vascular reactivity in the pediatric brain. Stroke. 2011;42:1834–1838. doi: 10.1161/STROKEAHA.110.607606. [DOI] [PubMed] [Google Scholar]
- 36.Lande MB, Kaczorowski JM, Auinger P, Schwartz GJ, Weitzman M. Elevated blood pressure and decreased cognitive function among school-age children and adolescents in the United States. J Pediatr. 2003;143:720–724. doi: 10.1067/S0022-3476(03)00412-8. [DOI] [PubMed] [Google Scholar]
- 37.Bliziotis IA, Destounis A, Stergiou GS. Home versus ambulatory and office blood pressure in predicting target organ damage in hypertension: a systematic review and meta-analysis. J Hypertens. 2012;30:1289–1299. doi: 10.1097/HJH.0b013e3283531eaf. [DOI] [PubMed] [Google Scholar]
- 38.Sorof JM, Cardwell G, Franco K, Portman RJ. Ambulatory blood pressure and left ventricular mass index in hypertensive children. Hypertension. 2002;39:903–908. doi: 10.1161/01.hyp.0000013266.40320.3b. [DOI] [PubMed] [Google Scholar]
- 39.McNiece KL, Gupta-Malhotra M, Samuels J, Bell C, Garcia K, Poffenbarger T, Sorof JM, Portman RJ. Left ventricular hypertrophy in hypertensive adolescents: analysis of risk by 2004 National High Blood Pressure Education Program Working Group staging criteria. Hypertension. 2007;50:392–395. doi: 10.1161/HYPERTENSIONAHA.107.092197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ster giou GS, Giovas PP, Kollias A, Rarra VC, Papagiannis JD, Vazeou A. Relationship of home blood pressure with target-organ damage in children and adolescents. Hypertens Res. 2011;34:640–644. doi: 10.1038/hr.2011.10. [DOI] [PubMed] [Google Scholar]
- 41.Brady TM, Fivush B, Flynn JT, Parekh R. Ability of blood pressure to predict left ventricular hypertrophy in children with primary hypertension. J Pediatr. 2008;152:73–78. 78.e71. doi: 10.1016/j.jpeds.2007.05.053. [DOI] [PubMed] [Google Scholar]
- 42.Richey PA, Disessa TG, Hastings MC, Somes GW, Alpert BS, Jones DP. Ambulatory blood pressure and increased left ventricular mass in children at risk for hypertension. J Pediatr. 2008;152:343–348. doi: 10.1016/j.jpeds.2007.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Maggio AB, Aggoun Y, Marchand LM, Martin XE, Herrmann F, Beghetti M, Farpour-Lambert NJ. Associations among obesity, blood pressure, and left ventricular mass. J Pediatr. 2008;152:489–493. doi: 10.1016/j.jpeds.2007.10.042. [DOI] [PubMed] [Google Scholar]
- 44.Amin R, Somers VK, McConnell K, Willging P, Myer C, Sherman M, McPhail G, Morgenthal A, Fenchel M, Bean J, Kimball T, Daniels S. Activity-adjusted 24-hour ambulatory blood pressure and cardiac remodeling in children with sleep disordered breathing. Hypertension. 2008;51:84–91. doi: 10.1161/HYPERTENSIONAHA.107.099762. [DOI] [PubMed] [Google Scholar]
- 45.O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK, Jr Cardiovascular Health Study Collaborative Research Group. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med. 1999;340:14–22. doi: 10.1056/NEJM199901073400103. [DOI] [PubMed] [Google Scholar]
- 46.Khattar RS, Acharya DU, Kinsey C, Senior R, Lahiri A. Longitudinal association of ambulatory pulse pressure with left ventricular mass and vascular hypertrophy in essential hypertension. J Hypertens. 1997;15:737–743. doi: 10.1097/00004872-199715070-00005. [DOI] [PubMed] [Google Scholar]
- 47.Lengyel S, Katona E, Zatik J, Molnár C, Paragh G, Fülesdi B, Páll D. The impact of serum homocysteine on intima-media thickness in normotensive, white-coat and sustained hypertensive adolescents. Blood Pressure. 2012;21:39–44. doi: 10.3109/08037051.2011.575577. [DOI] [PubMed] [Google Scholar]
- 48.Kamarck TW, Polk DE, Sutton-Tyrrell K, Muldoon MF. The incremental value of ambulatory blood pressure persists after controlling for methodological confounds: associations with carotid atherosclerosis in a healthy sample. J Hypertens. 2002;20:1535–1541. doi: 10.1097/00004872-200208000-00016. [DOI] [PubMed] [Google Scholar]
- 49.Stabouli S, Kotsis V, Papamichael C, Constantopoulos A, Zakopoulos N. Adolescent obesity is associated with high ambulatory blood pressure and increased carotid intimal-medial thickness. J Pediatr. 2005;147:651–656. doi: 10.1016/j.jpeds.2005.06.008. [DOI] [PubMed] [Google Scholar]
- 50.Litwin M, Niemirska A, Sladowska J, Antoniewicz J, Daszkowska J, Wierzbicka A, Wawer ZT, Grenda R. Left ventricular hypertrophy and arterial wall thickening in children with essential hypertension. Pediatr Nephrol. 2006;21:811–819. doi: 10.1007/s00467-006-0068-8. [DOI] [PubMed] [Google Scholar]
- 51.Páll D, Juhász M, Lengyel S, Molnár C, Paragh G, Fülesdi B, Katona E. Assessment of target-organ damage in adolescent white-coat and sustained hypertensives. J Hypertens. 2010;28:2139–2144. doi: 10.1097/HJH.0b013e32833cd2da. [DOI] [PubMed] [Google Scholar]
- 52.Lande MB, Carson NL, Roy J, Meagher CC. Effects of childhood primary hypertension on carotid intima media thickness: a matched controlled study. Hypertension. 2006;48:40–44. doi: 10.1161/01.HYP.0000227029.10536.e8. [DOI] [PubMed] [Google Scholar]
- 53.Krmar RT, Balzano R, Jogestrand T, Cedazo-Minguez A, Englund MS, Berg UB. Prospective analysis of carotid arterial wall structure in pediatric renal transplants with ambulatory normotension and in treated hypertensive recipients. Pediatr Transplant. 2008;12:412–419. doi: 10.1111/j.1399-3046.2007.00837.x. [DOI] [PubMed] [Google Scholar]
- 54.Simonetti GD, Von Vigier RO, Wühl E, Mohaupt MG. Ambulatory arterial stiffness index is increased in hypertensive childhood disease. Pediatr Res. 2008;64:303–307. doi: 10.1203/PDR.0b013e31817d9bc5. [DOI] [PubMed] [Google Scholar]
- 55.Suláková T, Janda J, Cerná J, Janštová V, Feber J. Assessment of arterial stiffness from ambulatory blood pressure monitoring in children with diabetes mellitus type-1 (DMT1) J Hum Hypertens. 2012;26:357–364. doi: 10.1038/jhh.2011.38. [DOI] [PubMed] [Google Scholar]
- 56.Zhu H, Yan W, Ge D, Treiber FA, Harshfield GA, Kapuku G, Snieder H, Dong Y. Cardiovascular characteristics in American youth with prehypertension. Am J Hypertens. 2007;20:1051–1057. doi: 10.1016/j.amjhyper.2007.05.009. [DOI] [PubMed] [Google Scholar]
- 57.Aggoun Y, Farpour-Lambert NJ, Marchand LM, Golay E, Maggio ABR, Beghetti M. Impaired endothelial and smooth muscle functions and arterial stiffness appear before puberty in obese children and are associated with elevated ambulatory blood pressure. Eur Heart J. 2008;29:792–799. doi: 10.1093/eurheartj/ehm633. [DOI] [PubMed] [Google Scholar]
- 58.Mitsnefes MM, Kimball TR, Witt SA, Glascock BJ, Khoury PR, Daniels SR. Abnormal carotid artery structure and function in children and adolescents with successful renal transplantation. Circulation. 2004;110:97–101. doi: 10.1161/01.CIR.0000133412.53089.26. [DOI] [PubMed] [Google Scholar]
- 59.Cahan A, Ben-Dov IZ, Mekler J, Bursztyn M. The role of blood pressure variability in misdiagnosed clinic hypertension. Hypertens Res. 2011;34:187–192. doi: 10.1038/hr.2010.190. [DOI] [PubMed] [Google Scholar]
- 60.Parati G, Faini A, Valentini M. Blood pressure variability: its measurement and significance in hypertension. Curr Hypertens Rep. 2006;8:199–204. doi: 10.1007/s11906-006-0051-6. [DOI] [PubMed] [Google Scholar]
- 61.Gustavsen PH, Hoegholm A, Bang LE, Kristensen KS. White coat hypertension is a cardiovascular risk factor: a 10-year follow-up study. J Hum Hypertens. 2003;17:811–817. doi: 10.1038/sj.jhh.1001643. [DOI] [PubMed] [Google Scholar]
- 62.Kavey RE, Kveselis DA, Atallah N, Smith FC. White coat hypertension in childhood: evidence for end-organ effect. J Pediatr. 2007;150:491–497. doi: 10.1016/j.jpeds.2007.01.033. [DOI] [PubMed] [Google Scholar]
- 63.Litwin M, Niemirska A, Ruzicka M, Feber J. White coat hypertension in children: not rare and not benign? J Am Soc Hypertens. 2009;3:416–423. doi: 10.1016/j.jash.2009.10.002. [DOI] [PubMed] [Google Scholar]
- 64.Litwin M, Simonetti GD, Niemirska A, Ruzicka M, Wühl E, Schaefer F, Feber J. Altered cardiovascular rhythmicity in children with white coat and ambulatory hypertension. Pediatr Res. 2010;67:419–423. doi: 10.1203/PDR.0b013e3181d00b5b. [DOI] [PubMed] [Google Scholar]
- 65.Páll D, Lengyel S, Komonyi E, Molnár C, Paragh G, Fülesdi B, Katona E. Impaired cerebral vasoreactivity in white coat hypertensive adolescents. Eur J Neurol. 2011;18:584–589. doi: 10.1111/j.1468-1331.2010.03209.x. [DOI] [PubMed] [Google Scholar]
- 66.Kouidi E, Fahadidou-Tsiligiroglou A, Tassoulas E, Deligiannis A, Coats A. White coat hypertension detected during screening of male adolescent athletes. Am J Hypertens. 1999;12:223–226. doi: 10.1016/s0895-7061(98)00186-1. [DOI] [PubMed] [Google Scholar]
- 67.Steinthorsdottir SD, Eliasdottir SB, Indridason OS, Agustsdottir IM, Palsson R, Edvardsson VO. Prevalence of hypertension in 9- to 10-year-old Icelandic school children. J Clin Hypertens (Greenwich) 2011;13:774–779. doi: 10.1111/j.1751-7176.2011.00496.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Suláková T, Janda J, Cerná J, Janstová V, Suláková A, Slaný J, Feber J. Arterial HTN in children with T1DM: frequent and not easy to diagnose. Pediatr Diabetes. 2009;10:441–448. doi: 10.1111/j.1399-5448.2009.00514.x. [DOI] [PubMed] [Google Scholar]
- 69.Sorof JM, Poffenbarger T, Franco K, Portman R. Evaluation of white coat hypertension in children: Importance of the definitions of normal ambulatory blood pressure and the severity of casual hypertension. Am J Hypertens. 2001;14:855–860. doi: 10.1016/s0895-7061(01)02180-x. [DOI] [PubMed] [Google Scholar]
- 70.Lurbe E, Torro I, Alvarez V, Nawrot T, Paya R, Redon J, Staessen JA. Prevalence, persistence, and clinical significance of masked hypertension in youth. Hypertension. 2005;45:493–498. doi: 10.1161/01.HYP.0000160320.39303.ab. [DOI] [PubMed] [Google Scholar]
- 71.Stabouli S, Kotsis V, Toumanidis S, Papamichael C, Constantopoulos A, Zakopoulos N. White-coat and masked hypertension in children: association with target-organ damage. Pediatr Nephrol. 2005;20:1151–1155. doi: 10.1007/s00467-005-1979-5. [DOI] [PubMed] [Google Scholar]
- 72.Furusawa ÉA, Filho UD, Junior DM, Koch VH. Home and ambulatory blood pressure to identify white coat and masked hypertension in the pediatric patient. Am J Hypertens. 2011;24:893–897. doi: 10.1038/ajh.2011.72. [DOI] [PubMed] [Google Scholar]
- 73.Matsuoka S, Awazu M. Masked hypertension in children and young adults. Pediatr Nephrol. 2004;19:651–654. doi: 10.1007/s00467-004-1459-3. [DOI] [PubMed] [Google Scholar]
- 74.Török K, Pálfi A, Szelényi Z, Molnár D. Circadian variability of blood pressure in obese children. Nutr Metab Cardiovasc Dis. 2008;18:429–435. doi: 10.1016/j.numecd.2007.02.012. [DOI] [PubMed] [Google Scholar]
- 75.Verberk WJ, Kessels AG, de Leeuw PW. Prevalence, causes, and consequences of masked hypertension: a meta-analysis. Am J Hypertens. 2008;21:969–975. doi: 10.1038/ajh.2008.221. [DOI] [PubMed] [Google Scholar]
- 76.Chaudhuri A, Sutherland SM, Begin B, Salsbery K, McCabe L, Potter D, Alexander SR, Wong CJ. Role of twenty-four-hour ambulatory blood pressure monitoring in children on dialysis. Clin J Am Soc Nephrol. 2011;6:870–876. doi: 10.2215/CJN.07960910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Di Salvo G, Castaldi B, Baldini L, Gala S, del Gaizo F, D’Andrea A, Limongelli G, D’Aiello AF, Scognamiglio G, Sarubbi B, Pacileo G, Russo MG, Calabrò R. Masked hypertension in young patients after successful aortic coarctation repair: Impact on left ventricular geometry and function. J Hum Hypertens. 2011;25:739–745. doi: 10.1038/jhh.2010.118. [DOI] [PubMed] [Google Scholar]
- 78.Fujita H, Matsuoka S, Awazu M. Ambulatory blood pressure in prehypertensive children and adolescents. Pediatr Nephrol. 2012;27:1361–1367. doi: 10.1007/s00467-012-2148-2. [DOI] [PubMed] [Google Scholar]
- 79.Lubrano R, Travasso E, Raggi C, Guido G, Masciangelo R, Elli M. Blood pressure load, proteinuria and renal function in pre-hypertensive children. Pediatr Nephrol. 2009;24:823–831. doi: 10.1007/s00467-008-1077-6. [DOI] [PubMed] [Google Scholar]
- 80.Lee SH, Kim JH, Kang MJ, Lee YA, Won Yang S, Shin CH. Implications of nocturnal hypertension in children and adolescents with type 1 diabetes. Diabetes Care. 2011;34:2180–2185. doi: 10.2337/dc11-0830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Wühl E, Witte K, Soergel M, Mehls O, Schaefer F German Working Group on Pediatric Hypertension. Distribution of 24-h ambulatory blood pressure in children: normalized reference values and role of body dimensions [published correction appears in J Hypertens. 2003;21:2205–2206] J Hypertens. 2002;20:1995–2007. doi: 10.1097/00004872-200210000-00019. [DOI] [PubMed] [Google Scholar]
- 82.Krzych LJ. Blood pressure variability in children with essential hypertension. J Hum Hypertens. 2007;21:494–500. doi: 10.1038/sj.jhh.1002172. [DOI] [PubMed] [Google Scholar]
- 83.Li Z, Snieder H, Su S, Harshfield GA, Treiber FA, Wang X. A longitudinal study of blood pressure variability in African-American and European American youth. J Hypertens. 2010;28:715–722. doi: 10.1097/HJH.0b013e328336ed5b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Bilge I, Poyrazoglu S, Bas F, Emre S, Sirin A, Gokalp S, Eryilmaz S, Hekim N, Darendeliler F. Ambulatory blood pressure monitoring and renal functions in term small-for-gestational age children. Pediatr Nephrol. 2011;26:119–126. doi: 10.1007/s00467-010-1646-3. [DOI] [PubMed] [Google Scholar]
- 85.Lurbe E, Redon J, Alvarez V, Durazo R, Gomez A, Tacons J, Cooper RS. Relationship between birth weight and awake blood pressure in children and adolescents in absence of intrauterine growth retardation. Am J Hypertens. 1996;9:787–794. doi: 10.1016/0895-7061(96)00058-1. [DOI] [PubMed] [Google Scholar]
- 86.Huxley RR, Shiell AW, Law CM. The role of size at birth and postnatal catch-up growth in determining systolic blood pressure: a systematic review of the literature. J Hypertens. 2000;18:815–831. doi: 10.1097/00004872-200018070-00002. [DOI] [PubMed] [Google Scholar]
- 87.Hovi P, Andersson S, Räikkönen K, Strang-Karlsson S, Järvenpää AL, Eriksson JG, Pesonen AK, Heinonen K, Pyhälä R, Kajantie E. Ambulatory blood pressure in young adults with very low birth weight. J Pediatr. 2009;156:54–59. e51. doi: 10.1016/j.jpeds.2009.07.022. [DOI] [PubMed] [Google Scholar]
- 88.Tenhola S, Rahiala E, Halonen P, Vanninen E, Voutilainen R. preeclampsia predicts elevated blood pressure in 12-year-old children: evaluation by ambulatory blood pressure monitoring. Pediatr Res. 2006;59:320–324. doi: 10.1203/01.pdr.0000196734.54473.e3. [DOI] [PubMed] [Google Scholar]
- 89.Salgado CM, Jardim PCBV, Teles FBG, Nunes MC. Low birth weight as a marker of changes in ambulatory blood pressure monitoring [article in English, Portuguese, Spanish] Arq Bras Cardiol. 2009;92:107–121. doi: 10.1590/s0066-782x2009000200007. [DOI] [PubMed] [Google Scholar]
- 90.Harshfield GA, Barbeau P, Richey PA, Alpert BS. Racial differences in the influence of body size on ambulatory blood pressure in youths. Blood Press Monit. 2000;5:59–63. [PubMed] [Google Scholar]
- 91.Harshfield GA, Treiber FA. Racial differences in ambulatory blood pressure monitoring-derived 24 h patterns of blood pressure in adolescents. Blood Press Monit. 1999;4:107–110. [PubMed] [Google Scholar]
- 92.Beatty DL, Matthews KA. Unfair treatment and trait anger in relation to nighttime ambulatory blood pressure in African American and white adolescents. Psychosom Med. 2009;71:813–820. doi: 10.1097/PSY.0b013e3181b3b6f8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Meininger JC, Liehr P, Chan W, Smith G, Mueller WH. Developmental, gender, and ethnic group differences in moods and ambulatory blood pressure in adolescents. Ann Behav Med. 2004;28:10–19. doi: 10.1207/s15324796abm2801_3. [DOI] [PubMed] [Google Scholar]
- 94.Harshfield GA, Alpert BS, Willey ES, Somes GW, Murphy JK, Dupaul LM. Race and gender influence ambulatory blood pressure patterns of adolescents. Hypertension. 1989;14:598–603. doi: 10.1161/01.hyp.14.6.598. [DOI] [PubMed] [Google Scholar]
- 95.Lurbe E, Alvarez V, Liao Y, Torro I, Cremades B, Redón J, Cooper R. Obesity modifies the relationship between ambulatory blood pressure and natriuresis in children. Blood Press Monit. 2000;5:275–280. doi: 10.1097/00126097-200010000-00005. [DOI] [PubMed] [Google Scholar]
- 96.Li AQ, Zhao ZY, Zhang LL, Lu FH, Yan ZH, Li YY, Chen H. Overweight influence on circadian variations of ambulatory blood pressure in Chinese adolescents. Clin Exp Hypertens. 2005;27:195–201. [PubMed] [Google Scholar]
- 97.Hurum H, Sulheim D, Thaulow E, Wyller VB. Elevated nocturnal blood pressure and heart rate in adolescent chronic fatigue syndrome. Acta Paediatr. 2011;100:289–292. doi: 10.1111/j.1651-2227.2010.02073.x. [DOI] [PubMed] [Google Scholar]
- 98.Urbina EM, Bao W, Pickoff AS, Berenson GS. Ethnic (black-white) contrasts in heart rate variability during cardiovascular reactivity testing in male adolescents with high and low blood pressure: the Bogalusa Heart Study. Am J Hypertens. 1998;11:196–202. doi: 10.1016/s0895-7061(97)00314-2. [DOI] [PubMed] [Google Scholar]
- 99.Oświecimska J, Ziora K, Adamczyk P, Roczniak W, Pikiewicz-Koch A, Stojewska M, Dyduch A. Effects of neuroendocrine changes on results of ambulatory blood pressure monitoring (ABPM) in adolescent girls with anorexia nervosa. Neuroendocrinol Lett. 2007;28:410–416. [PubMed] [Google Scholar]
- 100.Sethna CB, Leonard MB, Gallagher PR, Meyers KEC. Serum adiponectin levels and ambulatory blood pressure monitoring in pediatric renal transplant recipients. Transplantation. 2009;88:1030–1037. doi: 10.1097/TP.0b013e3181b9e1ec. [DOI] [PubMed] [Google Scholar]
- 101.Shatat IF, Freeman KD, Vuguin PM, Dimartino-Nardi JR, Flynn JT. Relationship between adiponectin and ambulatory blood pressure in obese adolescents. Pediatr Res. 2009;65:691–695. doi: 10.1203/PDR.0b013e31819ea776. [DOI] [PubMed] [Google Scholar]
- 101a.National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114:555–576. [PubMed] [Google Scholar]
- 102.Jones DP, Richey PA, Alpert BS, Li R. Serum uric acid and ambulatory blood pressure in children with primary hypertension. Pediatr Res. 2008;64:556–561. doi: 10.1203/PDR.0b013e318183fd7c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Shatat IF, Flynn JT. Relationships between renin, aldosterone, and 24-hour ambulatory blood pressure in obese adolescents. Pediatr Res. 2011;69:336–340. doi: 10.1203/PDR.0b013e31820bd148. [DOI] [PubMed] [Google Scholar]
- 104.Li R, Richey PA, DiSessa TG, Alpert BS, Jones DP. Blood aldosterone-to-renin ratio, ambulatory blood pressure, and left ventricular mass in children. J Pediatr. 2009;155:170–175. doi: 10.1016/j.jpeds.2009.02.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Samuels JA, Franco K, Wan F, Sorof JM. Effect of stimulants on 24-h ambulatory blood pressure in children with ADHD: a double-blind, randomized, cross-over trial. Pediatr Nephrol. 2006;21:92–95. doi: 10.1007/s00467-005-2051-1. [DOI] [PubMed] [Google Scholar]
- 106.Stowe CD, Gardner SF, Gist CC, Schulz EG, Wells TG. 24-Hour ambulatory blood pressure monitoring in male children receiving stimulant therapy. Ann Pharmacother. 2002;36:1142–1149. doi: 10.1345/aph.1A367. [DOI] [PubMed] [Google Scholar]
- 107.Savoca MR, MacKey ML, Evans CD, Wilson M, Ludwig DA, Harshfield GA. Association of ambulatory blood pressure and dietary caffeine in adolescents. Am J Hypertens. 2005;18:116–120. doi: 10.1016/j.amjhyper.2004.08.011. [DOI] [PubMed] [Google Scholar]
- 108.Lurbe E, Sorof JM, Daniels SR. Clinical and research aspects of ambulatory blood pressure monitoring in children. J Pediatr. 2004;144:7–16. doi: 10.1016/j.jpeds.2003.09.050. [DOI] [PubMed] [Google Scholar]
- 109.Wühl E, Hadtstein C, Mehls O, Schaefer F ESCAPE Trial Group. Home, clinic, and ambulatory blood pressure monitoring in children with chronic renal failure. Pediatr Res. 2004;55:492–497. doi: 10.1203/01.PDR.0000106863.90996.76. [DOI] [PubMed] [Google Scholar]
- 110.Díaz LN, Garin EH. Comparison of ambulatory blood pressure and task force criteria to identify pediatric hypertension. Pediatr Nephrol. 2007;22:554–558. doi: 10.1007/s00467-006-0372-3. [DOI] [PubMed] [Google Scholar]
- 111.Soergel M, Kirschstein M, Busch C, Danne T, Gellermann J, Holl R, Krull F, Reichert H, Reusz GS, Rascher W. Oscillometric twenty-four-hour ambulatory blood pressure values in healthy children and adolescents: a multicenter trial including 1141 subjects. J Pediatr. 1997;130:178–184. doi: 10.1016/s0022-3476(97)70340-8. [DOI] [PubMed] [Google Scholar]
- 112.Flynn JT. Ambulatory blood pressure monitoring in children: imperfect yet essential. Pediatr Nephrol. 2011;26:2089–2094. doi: 10.1007/s00467-011-1984-9. [DOI] [PubMed] [Google Scholar]
- 113.Vaughan CJ, Murphy MB. The use of ambulatory blood pressure monitoring in the evaluation of racial differences in blood pressure. J Cardiovasc Risk. 1994;1:132–135. doi: 10.1177/174182679400100205. [DOI] [PubMed] [Google Scholar]
- 114.Harshfield GA, Alpert BS, Pulliam DA, Somes GW, Wilson DK. Ambulatory blood pressure recordings in children and adolescents. Pediatrics. 1994;94:180–184. [PubMed] [Google Scholar]
- 115.O’Sullivan JJ, Derrick G, Griggs P, Foxall R, Aitkin M, Wren C. Ambulatory blood pressure in schoolchildren. Arch Dis Child. 1999;80:529–532. doi: 10.1136/adc.80.6.529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Lurbe E, Redon J, Liao Y, Tacons J, Cooper RS, Alvarez V. Ambulatory blood pressure monitoring in normotensive children. J Hypertens. 1994;12:1417–1423. [PubMed] [Google Scholar]
- 117.Varda NM, Gregoric A. Twenty-four-hour ambulatory blood pressure monitoring in infants and toddlers. Pediatr Nephrol. 2005;20:798–802. doi: 10.1007/s00467-005-1857-1. [DOI] [PubMed] [Google Scholar]
- 118.Gellermann J, Kraft S, Ehrich JH. Twenty-four-hour ambulatory blood pressure monitoring in young children. Pediatr Nephrol. 1997;11:707–710. doi: 10.1007/s004670050371. [DOI] [PubMed] [Google Scholar]
- 119.Prisant LM, Bottini PB, Carr AA. Ambulatory blood pressure monitoring: methodologic issues. Am J Nephrol. 1996;16:190–201. doi: 10.1159/000168998. [DOI] [PubMed] [Google Scholar]
- 120.Agarwal R, Light RP. The effect of measuring ambulatory blood pressure on nighttime sleep and daytime activity: implications for dipping. Clin J Am Soc Nephrol. 2010;5:281–285. doi: 10.2215/CJN.07011009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Martikainen S, Pesonen AK, Feldt K, Jones A, Lahti J, Pyhala R, Heinonen K, Kajantie E, Eriksson J, Räikkönen K. Poor sleep and cardiovascular function in children. Hypertension. 2011;58:16–21. doi: 10.1161/HYPERTENSIONAHA.111.172395. [DOI] [PubMed] [Google Scholar]
- 122.Mezick EJ, Hall M, Matthews KA. Sleep duration and ambulatory blood pressure in black and white adolescents. Hypertension. 2012;59:747–752. doi: 10.1161/HYPERTENSIONAHA.111.184770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Deleted in proof.
- 124.Sinha MD, Booth CJ, Reid CJ. Factors affecting success of blood pressure measurements during ambulatory blood pressure monitoring in children with renal disease. Cardiol Young. 2011;21:310–316. doi: 10.1017/S1047951110002003. [DOI] [PubMed] [Google Scholar]
- 125.Khan IA, Gajaria M, Stephens D, Balfe JW. Ambulatory blood pressure monitoring in children: a large center’s experience. Pediatr Nephrol. 2000;14:802–805. doi: 10.1007/s004679900291. [DOI] [PubMed] [Google Scholar]
- 126.Giordano U, Meta R, Fintini D, Turchetta A, Brufani C, Calzolari A. Usefulness of ambulatory blood pressure monitoring and head-up tilt test in the evaluation of paediatric syncope. Cardiol Young. 2011;21:89–93. doi: 10.1017/S1047951110001551. [DOI] [PubMed] [Google Scholar]
- 127.King-Schultz L, Weaver AL, Cramer CH. Correlation of blood pressure readings from 6-hour intervals with the daytime period of 24-hour ambulatory blood pressure monitoring in pediatric patients. J Clin Hypertens (Greenwich) 2012;14:396–400. doi: 10.1111/j.1751-7176.2012.00641.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Association for the Advancement of Medical Instrumentation/American National Standard. Manual, electronic, or automated sphygmomanometers: non-invasive blood pressure monitoring equipment: medical electrical equipment: part 2–30: particular requirements for the basic safety and essential performance of automated non-invasive sphygmomanometers. Arlington, VA: AAMI; 2009. [Google Scholar]
- 129.O’Brien E, Petri J, Littler W, de Swiet M, Padfield PL, Altman DG, Bland M, Coats A, Atkins N. The British Hypertension Society protocol for the evaluation of blood pressure measuring devices. J Hypertens. 1993;11(suppl 2):S43–S62. doi: 10.1097/00004872-199306000-00013. [DOI] [PubMed] [Google Scholar]
- 130.Jones DP, Richey PA, Alpert BS. Validation of the AM5600 ambulatory blood pressure monitor in children and adolescents. Blood Press Monit. 2008;13:349–351. doi: 10.1097/MBP.0b013e3283102cfe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Elkasabany AM, Urbina EM, Daniels SR, Berenson GS. Prediction of adult hypertension by K4 and K5 diastolic blood pressure in children: the Bogalusa Heart Study. J Pediatr. 1998;132:687–692. doi: 10.1016/s0022-3476(98)70361-0. [DOI] [PubMed] [Google Scholar]
- 132.Hammond IW, Urbina EM, Wattigney WA, Bao W, Steinmann WC, Berenson GS. Comparison of fourth and fifth Korotkoff diastolic blood pressures in 5 to 30 year old individuals: the Bogalusa Heart Study. Am J Hypertens. 1995;8:1083–1089. doi: 10.1016/0895-7061(95)00230-M. [DOI] [PubMed] [Google Scholar]
- 133.Jones HE, Sinha MD. The definition of daytime and nighttime influences the interpretation of ABPM in children. Pediatr Nephrol. 2011;26:775–781. doi: 10.1007/s00467-011-1791-3. [DOI] [PubMed] [Google Scholar]
- 134.Portman RJ, Yetman RJ, MSW Efficacy of 24-hour ambulatory blood pressure monitoring in children. J Pediatr. 1991;118:842–849. doi: 10.1016/s0022-3476(05)82193-6. [DOI] [PubMed] [Google Scholar]
- 135.Eissa MA, Poffenbarger T, Portman RJ. Comparison of the actigraph versus patients’ diary information in defining circadian time periods for analyzing ambulatory blood pressure monitoring data. Blood Press Monit. 2001;6:21–25. doi: 10.1097/00126097-200102000-00004. [DOI] [PubMed] [Google Scholar]
- 136.Jacoby AC, Fixler DE, Torres EJ. Limitations of an oscillometric ambulatory blood pressure monitor in physically active children. J Pediatr. 1993;122:231–236. doi: 10.1016/s0022-3476(06)80118-6. [DOI] [PubMed] [Google Scholar]
- 137.Eissa MAH, Meininger JC, Nguyen TQ, Chan W. The relationship of ambulatory blood pressure to physical activity in a tri-ethnic population of obese and nonobese adolescents. Am J Hypertens. 2007;20:140–147. doi: 10.1016/j.amjhyper.2006.07.008. [DOI] [PubMed] [Google Scholar]
- 138.Framme J, Dangardt F, Mårild S, Osika W, Währborg P, Friberg P. 24-h systolic blood pressure and heart rate recordings in lean and obese adolescents. Clin Physiol Funct Imaging. 2006;26:235–239. doi: 10.1111/j.1475-097X.2006.00679.x. [DOI] [PubMed] [Google Scholar]
- 139.Lambert PC, Abrams KR, Jones DR, Halligan AW, Shennan A. Analysis of ambulatory blood pressure monitor data using a hierarchical model incorporating restricted cubic splines and heterogeneous within-subject variances. Stat Med. 2001;20:3789–3805. doi: 10.1002/sim.1172. [DOI] [PubMed] [Google Scholar]
- 140.Winnicki M, Canali C, Mormino P, Palatini P. Ambulatory blood pressure monitoring editing criteria: is standardization needed? Hypertension and Ambulatory Recording Venetia Study (HARVEST) group, Italy. Am J Hypertens. 1997;10:419–427. [PubMed] [Google Scholar]
- 141.Kennedy SE, Mackie FE, Rosenberg AR, Craig E, Kainer G. Agreement on reporting of ambulatory blood pressure monitoring in children. Pediatr Nephrol. 2005;20:1766–1768. doi: 10.1007/s00467-005-2066-7. [DOI] [PubMed] [Google Scholar]
- 142.Hadtstein C, Wühl E, Soergel M, Witte K, Schaefer F German Study Group for Pediatric Hypertension. Normative values for circadian and ultradian cardiovascular rhythms in childhood. Hypertension. 2004;43:547–554. doi: 10.1161/01.HYP.0000116754.15808.d8. [DOI] [PubMed] [Google Scholar]
- 143.Wühl E, Hadtstein C, Mehls O, Schaefer F ESCAPE Trial Group. Ultradian but not circadian blood pressure rhythms correlate with renal dysfunction in children with chronic renal failure. J Am Soc Nephrol. 2005;16:746–754. doi: 10.1681/ASN.2004070537. [DOI] [PubMed] [Google Scholar]
- 144.Gilardini L, Parati G, Sartorio A, Mazzilli G, Pontiggia B, Invitti C. Sympathoadrenergic and metabolic factors are involved in ambulatory blood pressure rise in childhood obesity. J Hum Hypertens. 2008;22:75–82. doi: 10.1038/sj.jhh.1002288. [DOI] [PubMed] [Google Scholar]
- 145.Pickering TG, Harshfield GA, Kleinert HD, Blank S, Laragh JH. Blood pressure during normal daily activities, sleep, and exercise: comparison of values in normal and hypertensive subjects. JAMA. 1982;247:992–996. [PubMed] [Google Scholar]
- 146.Harshfield GA, Pickering TG, Kleinert HD, Blank S, Laragh JH. Situational variations of blood pressure in ambulatory hypertensive patients. Psychosom Med. 1982;44:237–245. doi: 10.1097/00006842-198207000-00002. [DOI] [PubMed] [Google Scholar]
- 147.Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlöf B, Sever PS, Poulter NR. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010;375:895–905. doi: 10.1016/S0140-6736(10)60308-X. [DOI] [PubMed] [Google Scholar]
- 148.Richey PA, Disessa TG, Somes GW, Alpert BS, Jones DP. Left ventricular geometry in children and adolescents with primary hypertension. Am J Hypertens. 2010;23:24–29. doi: 10.1038/ajh.2009.164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Li Y, Wang J-G, Dolan E, Gao P-J, Guo H-F, Nawrot T, Stanton AV, Zhu D-L, O’Brien E, Staessen JA. Ambulatory arterial stiffness index derived from 24-hour ambulatory blood pressure monitoring. Hypertension. 2006;47:359–364. doi: 10.1161/01.HYP.0000200695.34024.4c. [DOI] [PubMed] [Google Scholar]
- 150.Dolan E, Thijs L, Li Y, Atkins N, McCormack P, McClory S, O’Brien E, Staessen JA, Stanton AV. Ambulatory arterial stiffness index as a predictor of cardiovascular mortality in the Dublin outcome study. Hypertension. 2006;47:365–370. doi: 10.1161/01.HYP.0000200699.74641.c5. [DOI] [PubMed] [Google Scholar]
- 151.Vincenti M, von Vigier RO, Wühl E, Mohaupt MG, Simonetti GD. The ambulatory arterial stiffness index is not affected by night-time blood pressure characteristics. J Hum Hypertens. 2009;23:680–682. doi: 10.1038/jhh.2009.25. [DOI] [PubMed] [Google Scholar]
- 152.Jones DP, Richey PA, Alpert BS. Comparison of ambulatory blood pressure reference standards in children evaluated for hypertension. Blood Press Monit. 2009;14:103–107. doi: 10.1097/MBP.0b013e32832ce11e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.White WB, Dey HM, Schulman P. Assessment of the daily blood pressure load as a determinant of cardiac function in patients with mild-to-moderate hypertension. Am Heart J. 1989;118:782–795. doi: 10.1016/0002-8703(89)90593-0. [DOI] [PubMed] [Google Scholar]
- 154.Wilson DK, Sica DA, Miller SB. Ambulatory blood pressure nondipping status in salt-sensitive and salt-resistant black adolescents. Am J Hypertens. 1999;12:159–165. doi: 10.1016/s0895-7061(98)00234-9. [DOI] [PubMed] [Google Scholar]
- 155.Krmar RT, Berg UB. Long-term reproducibility of routine ambulatory blood pressure monitoring in stable pediatric renal transplant recipients. Am J Hypertens. 2005;18:1408–1414. doi: 10.1016/j.amjhyper.2005.05.018. [DOI] [PubMed] [Google Scholar]
- 156.Barnes VA, Johnson MH, Dekkers JC, Treiber FA. Reproducibility of ambulatory blood pressure measures in African-American adolescents. Ethn Dis. 2002;12(S3):101–106. [PMC free article] [PubMed] [Google Scholar]
- 157.Harshfield GA, Treiber FA, Davis H, Johnson M, Slavens GA, Thompson W. Temporal stability of ambulatory blood pressure and heart rate in youths. Blood Press Monit. 1999;4:87–90. [PubMed] [Google Scholar]
- 158.Lurbe E, Redon J. Reproducibility and validity of ambulatory blood pressure monitoring in children. Am J Hypertens. 2002;15:69S–73S. doi: 10.1016/s0895-7061(01)02300-7. [DOI] [PubMed] [Google Scholar]
- 159.Ward A, Hansen P. Accuracy and Reproducibility of Ambulatory Blood Pressure Recorder Measurements During Rest and Exercise. New York, NY: Springer-Verlag; 1984. [Google Scholar]
- 160.van der Steen MS, Lenders JW, Graafsma SJ, den Arend J, Thien T. Reproducibility of ambulatory blood pressure monitoring in daily practice. J Hum Hypertens. 1999;13:303–308. doi: 10.1038/sj.jhh.1000808. [DOI] [PubMed] [Google Scholar]
- 161.Palatini P, Mormino P, Canali C, Santonastaso M, De Venuto G, Zanata G, Pessina AC. Factors affecting ambulatory blood pressure reproducibility: results of the HARVEST trial: Hypertension and Ambulatory Recording Venetia Study. Hypertension. 1994;23:211–216. doi: 10.1161/01.hyp.23.2.211. [DOI] [PubMed] [Google Scholar]
- 162.Zakopoulos NA, Nanas SN, Lekakis JP, Vemmos KN, Kotsis VT, Pitiriga VC, Stamatelopoulos SF, Moulopoulos SD. Reproducibility of ambulatory blood pressure measurements in essential hypertension. Blood Press Monit. 2001;6:41–45. doi: 10.1097/00126097-200102000-00007. [DOI] [PubMed] [Google Scholar]
- 163.Wang X, Poole JC, Treiber FA, Harshfield GA, Hanevold CD, Snieder H. Ethnic and gender differences in ambulatory blood pressure trajectories: results from a 15-year longitudinal study in youth and young adults. Circulation. 2006;114:2780–2787. doi: 10.1161/CIRCULATIONAHA.106.643940. [DOI] [PubMed] [Google Scholar]
- 164.Li Z, Snieder H, Harshfield GA, Treiber FA, Wang X. A 15-year longitudinal study on ambulatory blood pressure tracking from childhood to early adulthood. Hypertens Res. 2009;32:404–410. doi: 10.1038/hr.2009.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Pickering T. Recommendations for the use of home (self) and ambulatory blood pressure monitoring: American Society of Hypertension Ad Hoc Panel. Am J Hypertens. 1996;9:1–11. doi: 10.1016/0895-7061(95)00341-x. [DOI] [PubMed] [Google Scholar]
- 166.Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Jones DW, Kurtz T, Sheps SG, Roccella EJ. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the subcommittee of professional and public education of the American Heart Association Council on High Blood Pressure Research. Circulation. 2005;111:697–716. doi: 10.1161/01.CIR.0000154900.76284.F6. [DOI] [PubMed] [Google Scholar]
- 167.Flynn JT. Differentiation between primary and secondary hypertension in children using ambulatory blood pressure monitoring. Pediatrics. 2002;110:89–93. doi: 10.1542/peds.110.1.89. [DOI] [PubMed] [Google Scholar]
- 168.Flynn JT, Alderman MH. Characteristics of children with primary hypertension seen at a referral center. Pediatr Nephrol. 2005;20:961–966. doi: 10.1007/s00467-005-1855-3. [DOI] [PubMed] [Google Scholar]
- 169.Sorof JM, Turner J, Franco K, Portman RJ. Characteristics of hypertensive children identified by primary care referral compared with school-based screening. J Pediatr. 2004;144:485–489. doi: 10.1016/j.jpeds.2003.12.047. [DOI] [PubMed] [Google Scholar]
- 170.Flynn J, Zhang Y, Solar-Yohay S, Shi V. Clinical and demographic characteristics of children with hypertension. Hypertension. 2012;60:1047–1054. doi: 10.1161/HYPERTENSIONAHA.112.197525. [DOI] [PubMed] [Google Scholar]
- 171.Graves JW, Grossardt BR, Gullerud RE, Bailey KR, Feldstein J. The trained observer better predicts daytime ABPM diastolic blood pressure in hypertensive patients than does an automated (Omron) device. Blood Press Monit. 2006;11:53–58. doi: 10.1097/01.mbp.0000200480.26669.72. [DOI] [PubMed] [Google Scholar]
- 172.Skirton H, Chamberlain W, Lawson C, Ryan H, Young E. A systematic review of variability and reliability of manual and automated blood pressure readings. J Clin Nurs. 2011;20:602–614. doi: 10.1111/j.1365-2702.2010.03528.x. [DOI] [PubMed] [Google Scholar]
- 173.Smulyan H, Safar ME. Blood pressure measurement: retrospective and prospective views. Am J Hypertens. 2011;24:628–634. doi: 10.1038/ajh.2011.22. [DOI] [PubMed] [Google Scholar]
- 174.Ettinger LM, Freeman K, DiMartino-Nardi JR, Flynn JT. Microalbuminuria and abnormal ambulatory blood pressure in adolescents with type 2 diabetes mellitus. J Pediatr. 2005;147:67–73. doi: 10.1016/j.jpeds.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 175.Fan HQ, Li Y, Thijs L, Hansen TW, Boggia J, Kikuya M, Björklund-Bodegård K, Richart T, Ohkubo T, Jeppesen J, Torp-Pedersen C, Dolan E, Kuznetsova T, Stolarz-Skrzypek K, Tikhonoff V, Malyutina S, Casiglia E, Nikitin Y, Lind L, Sandoya E, Kawecka-Jaszcz K, Imai Y, Ibsen H, O’Brien E, Wang J, Staessen JA International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes Investigators. Prognostic value of isolated nocturnal hypertension on ambulatory measurement in 8711 individuals from 10 populations. J Hypertens. 2010;28:2036–2045. doi: 10.1097/HJH.0b013e32833b49fe. [DOI] [PubMed] [Google Scholar]
- 176.Lurbe E, Redon J, Kesani A, Pascual JM, Tacons J, Alvarez V, Batlle D. Increase in nocturnal blood pressure and progression to microalbuminuria in type 1 diabetes. N Engl J Med. 2002;347:797–805. doi: 10.1056/NEJMoa013410. [DOI] [PubMed] [Google Scholar]
- 177.Redon J, Plancha E, Swift PA, Pons S, Muñoz J, Martinez F. Nocturnal blood pressure and progression to end-stage renal disease or death in nondiabetic chronic kidney disease stages 3 and 4. J Hypertens. 2010;28:602–607. doi: 10.1097/HJH.0b013e328333fe4d. [DOI] [PubMed] [Google Scholar]
- 178.Samuels J, Ng D, Flynn JT, Mitsnefes M, Poffenbarger T, Warady BA, Furth S Chronic Kidney Disease in Children Study Group. Ambulatory blood pressure patterns in children with chronic kidney disease. Hypertension. 2012;60:43–50. doi: 10.1161/HYPERTENSIONAHA.111.189266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Hansen TW, Li Y, Boggia J, Thijs L, Richart T, Staessen JA. Predictive role of the nighttime blood pressure. Hypertension. 2011;57:3–10. doi: 10.1161/HYPERTENSIONAHA.109.133900. [DOI] [PubMed] [Google Scholar]
- 180.McGlothan KR, Wyatt RJ, Ault BH, Hastings MC, Rogers T, DiSessa T, Jones DP. Predominance of nocturnal hypertension in pediatric renal allograft recipients. Pediatr Transplant. 2006;10:558–564. doi: 10.1111/j.1399-3046.2006.00521.x. [DOI] [PubMed] [Google Scholar]
- 181.Amoore JN. Oscillometric sphygmomanometers: a critical appraisal of current technology. Blood Press Monit. 2012;17:80–88. doi: 10.1097/MBP.0b013e32835026b0. [DOI] [PubMed] [Google Scholar]
- 182.Wühl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, Zurowska A, Testa S, Jankauskiene A, Emre S, Caldas-Afonso A, Anarat A, Niaudet P, Mir S, Bakkaloglu A, Enke B, Montini G, Wingen AM, Sallay P, Jeck N, Berg U, Caliskan S, Wygoda S, Hohbach-Hohenfellner K, Dusek J, Urasinski T, Arbeiter K, Neuhaus T, Gellermann J, Drozdz D, Fischbach M, Moller K, Wigger M, Peruzzi L, Mehls O, Schaefer F ESCAPE Trial Group. Strict blood-pressure control and progression of renal failure in children. N Engl J Med. 2009;361:1639–1650. doi: 10.1056/NEJMoa0902066. [DOI] [PubMed] [Google Scholar]
- 183.White WB. Blood pressure load and target organ effects in patients with essential hypertension. J Hypertens Suppl. 1991;9:S39–41. [PubMed] [Google Scholar]
- 184.Mitsnefes M, Flynn J, Cohn S, Samuels J, Blydt-Hansen T, Saland J, Kimball T, Furth S, Warady B CKiD Study Group. Masked hypertension associates with left ventricular hypertrophy in children with CKD. J Am Soc Nephrol. 2010;21:137–144. doi: 10.1681/ASN.2009060609. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.