

Abstract
PURPOSE
To present a literature review on implant overdentures after a brief survey of bone loss after extraction of all teeth.
MATERIALS AND METHODS
Papers on alveolar bone loss and implant overdentures have been studied for a narrative review.
RESULTS
Bone loss of the alveolar process after tooth extraction occurs with great individual variation, impossible to predict at the time of extraction. The simplest way to prevent bone loss is to avoid extraction of all teeth. To keep a few teeth and use them or their roots for a tooth or root-supported overdenture substantially reduces bone loss. Jaws with implant-supported prostheses show less bone loss than jaws with conventional dentures. Mandibular 2-implant overdentures provide patients with better outcomes than do conventional dentures, regarding satisfaction, chewing ability and oral-health-related quality of life. There is no strong evidence for the superiority of one overdenture retention-system over the others regarding patient satisfaction, survival, peri-implant bone loss and relevant clinical factors. Mandibular single midline implant overdentures have shown promising results but long-term results are not yet available. For a maxillary overdenture 4 to 6 implants splinted with a bar provide high survival both for implants and overdenture.
CONCLUSION
In edentulous mandibles, 2-implant overdentures provide excellent long-term success and survival, including patient satisfaction and improved oral functions. To further reduce the costs a single midline implant overdenture can be a promising option. In the maxilla, overdentures supported on 4 to 6 implants splinted with a bar have demonstrated good functional results.
Keywords: Ball attachment, Early loading, Mandibular 2-implant overdenture, Maxillary implant overdenture, Single midline implant
INTRODUCTION
Old age was for long considered inevitably accompanied by the loss of teeth. The prevalence of edentulism is also strongly associated with ageing although it is now well known that teeth can be kept all the life in many individuals. The rate of edentulousness differs much between countries and it has declined dramatically during the last few decades in most countries.1,2 A nationwide study in Sweden over two decades showed that the prevalence of edentulism in subjects aged 55-84 years was 43% in 1980-81 and 14% in 2002. In the youngest age group (55-64 years) only 4% were edentulous in 2002.3 In a more recent study the prevalence of edentulism in 2012 among 70-year-old subjects in Sweden was only 3%.4 It is now well established that the loss of teeth is related to a number of factors, such as socio-economy, tradition, oral health resources, and not only to dental diseases.1,5
Until the introduction of osseointegrated implant-supported prostheses, complete dentures were the only available treatment for edentulous patients. A recent review concluded that in most societies, the need for complete dentures is not likely to reduce in the near future in spite of the dramatically improved therapeutic possibilities provided by osseointegrated dental implants. The edentulous people in the world belong to the poorest section of the population and implant treatment is unrealistic for them; for many even "low-tech" therapies like conventional dentures are beyond their reach.6
Brånemark and co-workers presented a fixed prosthesis on 5-6 implants as a viable treatment for edentulous jaws, and during many years this was the dominating concept with extremely successful long-term results.7,8,9 However, in the mid 1980's treatments with mandibular implant overdentures were introduced.10 Being less expensive and less complicated but yet successful, mandibular implant overdentures soon became popular in many countries.11,12 Maxillary implant overdentures on few implants have in general been found less successful than the mandibular 2-implant overdenture.13,14
It is the aim of this article to present a literature review on implant overdentures after a survey of bone loss after tooth extraction and prosthodontic treatment.
Literature
The literature on dental implants is increasing rapidly. In 2003 PubMed listed 6,800 titles, in 2014 the number had increased almost four times to 24,600. The number of publications on implant overdentures has also increased during these 11 years, from 780 to 1,800. It was not the purpose to make a systematic review of this literature, only to give a narrative review of some trends related to implant and root-supported overdentures reflected in selected publications, but starting with some aspects on the consequences of extraction of teeth.
Reduction of residual ridges
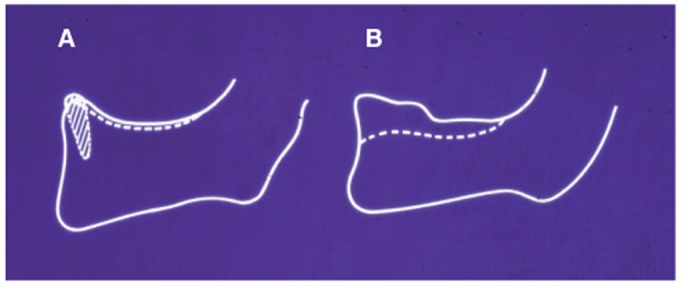
After tooth extraction the alveolar process is reduced due to bone loss, with great individual variation, which is impossible to predict at the time of extraction (Fig. 1).15 For many patients this can lead to severe problems for the retention of conventional dentures. A classical paper even characterized this reduction of the residual ridges as "a major oral disease entity".16 Is this relevant also in 2014? With respect to the fact that the majority of edentulous subjects will have to continue relying on complete dentures,6 the phenomenon of bone loss needs continuing consideration. The term bone resorption is not always adequate and it has been suggested that bone loss should be used instead.17
Fig. 1.

Tracings from profile radiographs of mandibular symphyseal region of 12 subjects 2 days, 5 years and 21 years after extraction of all teeth in the mandible (with permission from J Prosthet Dent15).
Even if the rate of edentulism is decreasing in most countries, a study in USA prognosticated that there would be an increase of the number of edentulous jaws to 38 million in 2020, mainly due to demographic reasons: people live longer and the number of elderly increases. In that paper, implants were not mentioned as an option for the edentulous subjects, only complete dentures.18 This can be interpreted as a consequence of the socio-economic situation of the edentulous people; this segment of the population is poor and not able to ask for implant treatment. As this is the situation in the richest country in the world, it is even worse in a global perspective.6,19
Numerous factors have been proposed to be of possible importance for bone loss in residual ridges (Table 1). No dominant factor has been identified. However, it is suggested that combinations of anatomic, metabolic, psychosocial, mechanical and yet unknown factors may be responsible but the mechanisms are not well understood.17,20
Table 1.
Factors of possible importance for bone loss in residual ridges
There are some possible ways to prevent or at any rate reduce the bone loss of residual ridges (Table 2). The simplest is of course to avoid extraction of all teeth. To keep a few teeth and use them or their roots for a tooth or root-supported overdenture has been shown to substantially reduce the bone loss in the mandible (Fig. 2).21 A classical textbook on root-supported overdentures describes a number of solutions which should be considered before the decision is made to extract all remaining teeth.22 There are many advantages of root or tooth supported overdentures compared to complete dentures such as improved denture stability and retention. There are relatively few studies on the survival of tooth and root supported overdentures but those available have demonstrated a wide range of survival rates, from very good to relatively poor results, and a great need for prosthetic maintenance.23 Nevertheless tooth or root supported overdentures are a therapeutic option that deserves more attention because of its obvious advantages compared to conventional complete dentures.
Table 2.
Ways to prevent or reduce bone loss of residual ridges
Fig. 2.
Comparison of bone loss in a patient with a root-supported overdenture (A) and a conventional complete denture (B) 5 years after extraction of teeth and insertion of dentures (with permission from J Prosthet Dent21).
Dental implants and bone loss in residual ridges
Jaws with implant-supported prostheses show less bone loss than jaws with conventional dentures, probably because of more adequate functional stimulus to the bone via implants than through dentures.11,24,25,26 Not only reduced bone loss but even bone apposition has been demonstrated in jaws with fixed implant-supported prostheses.26,27 This bone preserving effect of implant-supported prostheses should be included in the decision making for the edentulous mandible.
Mandibular implant overdentures
Several randomized control trials have demonstrated that implant overdentures provide patients with better outcomes than do conventional dentures, e.g. regarding satisfaction, chewing ability and oral-health-related quality of life. A mandibular implant overdenture on two implants is thus a well-established and effective option, also in a long-term perspective.11,28 It has even been suggested that it should become the first choice of treatment for the edentulous mandible.29,30 This is a tempting possibility but it has been criticized as unrealistic, mainly because of the fact that the edentulous patients are poor and cannot afford any implant treatment.6,19 It should also be remembered that the majority of complete denture wearers are quite satisfied with their predicament, both functionally and esthetically.4,31 More than a third of edentulous patients choose to stay with conventional dentures even when offered a mandibular implant overdenture free of charge.32
Retention system for implant overdentures
The retention systems for the 2-implant overdenture can be divided into splinted and unsplinted ones. The splinted systems use an interconnecting bar and a retentive clip; for the unsplinted implants there are several retention types available such as ball attachments and magnets. There is no strong evidence for the superiority of one system over the others regarding patient satisfaction, survival, periimplant bone loss and relevant clinical factors. Common to all systems is that they require substantial prosthodontic maintenance with time and cost implications, which should be included in the economic aspects of the treatment.33 However, irrespective of the differences between the retention systems, mandibular implant overdentures provide increased patient comfort and acceptance as well as oral function compared to complete dentures.11
Early loading
Early loading of mandibular implant overdentures at 6 weeks or even 2 weeks has been shown to be an effective treatment. Loading can be minimized by requesting the patients to eat only soft meals for the first few weeks11 Based on recent studies it has been concluded that early loading protocols produce equal outcomes as conventional loading and thus is a viable option in construction of mandibular overdentures.34,35 However, a recent systematic review concluded that although all three loading protocols (immediate, early and conventional loading) provide high survival rates, early and conventional loading protocols are still better documented than immediate loading and seem to result in fewer implant failures during the first year.36
Cost of treatment of edentulous jaws
When comparing the cost of different treatment options it is clear that the cheapest alternative is the conventional complete denture followed by the implant overdenture; a fixed implant-supported prosthesis is the most expensive. Economical aspects on prosthodontic treatment are rare but a few studies deserve to be mentioned. Long-term comparisons (over 9 and 15 years) have demonstrated that overdentures are a more cost-effective treatment compared to fixed prostheses.37 In a comparison of different types of overdentures it was shown that a construction using 4-implants was more expensive than one with 2 implants but required less aftercare over 8 years. Nevertheless, the authors concluded that the 2-implant bar-retained overdenture was most effective when considering other factors such as patient satisfaction, clinical implant performance and cost-effectiveness.38 Another study found that there was no difference in cost between 2- and 4-implant overdentures over 10 years. The 2-implant overdenture was therefore more cost-effective.39
It seems to be almost consensus in the literature today that in the mandible two implants are sufficient for the retention/support of an overdenture; this option is accompanied by excellent results also in the long run.28,30
Single midline implant
To reduce the cost of treatment a single midline implant has been tried to retain a mandibular implant overdenture (Fig. 3). An early 5-year study demonstrated good results with such an overdenture.40 These and similar results41 led to a suggestion to use the single midline implant overdenture as an inexpensive treatment for geriatric and other patients with low functional demands. During the last few years several short-term randomized clinical trials have been presented indicating an increased interest in the profession to evaluate this option.42,43,44,45 The results of these short-term studies have in general been assessed as promising but long-term observations are required for a firm conclusion regarding the clinical usefulness of mandibular overdentures supported by a single midline implant.
Fig. 3.
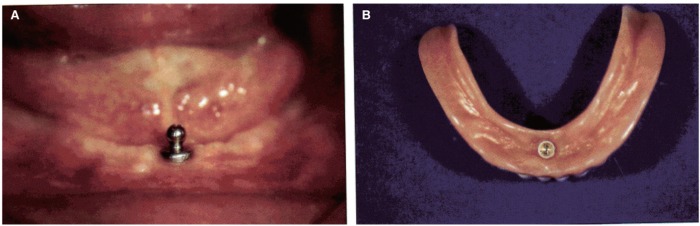
(A) Single implant with a ball attachment in an edentulous mandible to retain an overdenture. (B) The inner surface of the mandibular overdenture with retainer for the ball attachment (with permission from Int J Oral Maxillofac Implants41).
Maxilary implant overdenture
Implant overdentures in the maxilla have in general not been as successful as in the mandible, but the early poor results were probably partly due to the fact that maxillary implant overdentures often were made as a "rescue treatment" when a fixed prosthesis had failed. The results improved when maxillary implant overdentures were made as a planned treatment following strict protocols.13 Nevertheless it is evident that maxillary implant overdentures present a number of different challenges compared to the predictable benefits of mandibular 2-implant overdentures.46,47 Systematic reviews concluded that maxillary overdentures on 4 or more implants in a splinted construction provided high survival (> 95% for the first year) both for implants and overdenture.14,48 Long-term results regarding maxillary implant overdentures are still rare and when available often inconsistent.49 However, following the recommendation to use 4 or more implants splinted with a bar system a maxillary overdenture can be a successful treatment option (Fig. 4). Using four or less implants and a ball attachment system is in general less successful.
Fig. 4.
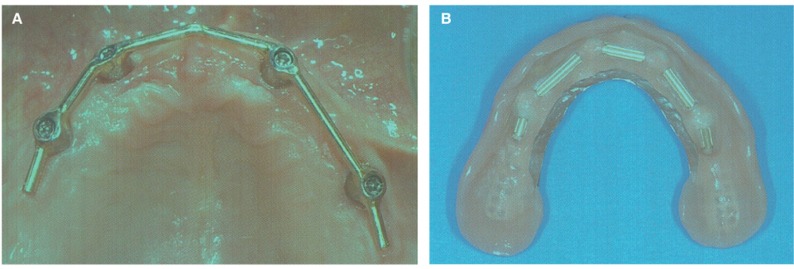
(A) Four implants in an edentulous maxilla splinted with a bar for an overdenture. (B) The inner surface of the maxillary overdenture showing the bar retainers fixed in the denture base material (with permission from Quintessence13).
Implant overdenture or fixed implant-suported prosthesis
Many factors influence the choice between a fixed and removable implant prosthesis in treatment of an edentulous patient. At the introduction of osseointegrated implants in Sweden in the 1970s, professor Brånemark7 suggested fixed prostheses as the first choice. This was also for long the policy among prosthodontists in Sweden. The great majority of implant treatments of edentulous mandibles consisted of fixed prosthesis, only a small part was implant overdentures according to a questionnaire study regarding year 2001.50 In this respect not much has changed during the last decade among prosthodontists in Sweden: in 2012 the ratio between fixed implant-supported prostheses overdentures in edentulous mandibles was 17 to 3, similar to the results 10 years earlier.51 The same type of questions presented to prosthodontists in 10 countries demonstrated a great variation of the use of implant overdentures in year 2001.12 In fact, the proportion of implant overdentures to fixed implant-supported prostheses regarding implant treatments of the edentulous mandible varied from 12% in Sweden to 93% in the Netherlands. In Korea the proportion was approximately 50/50% (Fig. 5). There is no current data published but it would be interesting to see the recent development internationally concerning the choice between overdenture or fixed prosthesis in implant treatment of the edentulous mandible.
Fig. 5.

Distribution of the use of implant overdentures (IODs) and fixed implant-supported prostheses (FISPs) for implant treatment of edentulous mandibles in 10 countries (with permission from Int J Prosthodont12).
DISCUSSION
The international interest in dental implants has developed almost exponentially during the last three decades, starting after the Toronto conference in 1982 when Professor Brånemark and his group from the University of Gothenburg presented their, by that time incredibly successful, results of treatment with osseointegrated implants.52 The originally predominant prescription of fixed implant prostheses has gradually been supplemented with other options, among which implant overdentures is the focus of this article. There is overwhelming evidence that implant overdentures are superior to conventional complete dentures in several aspects, especially for the edentulous mandible. It has therefore been suggested that, if possible, mandibular implant overdentures should be the first option for complete denture wearers with adaptation difficulties.29,30
Even if the prevalence of edentulism is decreasing in most countries there is still a great number of edentulous individuals needing treatment. A majority of them belong to the poorest segment of the population and cannot afford implant treatment; they will have to rely on complete dentures.6,19
For complete denture wearers with adaptation difficulties the mandibular denture is usually the most critical problem. Treating such patients with a fixed implant-supported prosthesis in the mandible but keeping the maxillary complete denture led to dramatic improvement of oral functions and "oral well-being" both in short- and long-term perspectives.9,53 The great functional improvement provided by a mandibular implant overdenture together with a maxillary complete denture is well established.11,28,30 A mandibular 2-implant overdenture is less expensive than a fixed implant-supported prosthesis and can therefor make implant treatment available to more edentulous patients. Another way to further reduce the cost of implant treatment and expand the benefits of it to more people is by using a single midline implant as support for a mandibular overdenture. This is a promising option according to shortterm studies but awaiting long-term evaluation.42,45
The stable and successful long-term results for 2-implant overdentures in the mandible cannot be transferred to the maxilla. A maxillary implant overdenture needs more support, preferably 4 to 6 implants splinted with a bar, to reach similar results as a 2-implant option in the mandible.
CONCLUSION
The bone loss of the alveolar process after tooth extraction occurs with great individual variation, impossible to predict at the time of extraction. The simplest way to prevent the bone loss is to avoid extraction of all teeth. To keep a few teeth for a tooth or root-supported overdenture has been shown to substantially reduce the bone loss.
In edentulous mandibles 2-implant overdentures provide excellent long-term success and survival, including patient satisfaction, improved oral functions and oral health related quality of life. To further reduce the costs a single midline implant overdenture can be a promising option. In the maxilla overdentures need to be supported on more than 2 implants; 4 to 6 implants splinted with a bar have demonstrated good functional results.
Footnotes
This article is a revised and updated version of a presentation given by the author at the Korean Academy of Prosthodontics Spring Scientific Meeting April 6, 2014.
References
- 1.Mojon P. The world without teeth: demographic trends. In: Feine JS, Carlsson GE, editors. Implant overdentures. The standard of care for edentulous patients. Chicago: Quintessence; 2003. pp. 3–14. [Google Scholar]
- 2.Müller F, Naharro M, Carlsson GE. What are the prevalence and incidence of tooth loss in the adult and elderly population in Europe? Clin Oral Implants Res. 2007;18:2–14. doi: 10.1111/j.1600-0501.2007.01459.x. [DOI] [PubMed] [Google Scholar]
- 3.Österberg T, Dey DK, Sundh V, Carlsson GE, Jansson JO, Mellström D. Edentulism associated with obesity: a study of four national surveys of 16 416 Swedes aged 55-84 years. Acta Odontol Scand. 2010;68:360–367. doi: 10.3109/00016357.2010.514721. [DOI] [PubMed] [Google Scholar]
- 4.Carlsson GE, Ekbäck G, Johansson A, Ordell S, Unell L. Is there a trend of decreasing prevalence of TMD-related symptoms with ageing among the elderly? Acta Odontol Scand. 2014 Mar 25; doi: 10.3109/00016357.2014.898787. [DOI] [PubMed] [Google Scholar]
- 5.Bouma J. On becoming edentulous. An investigation into dental and behavioural reasons for full mouth extractions. University of Groningen; 1987. Thesis. [Google Scholar]
- 6.Carlsson GE, Omar R. The future of complete dentures in oral rehabilitation. A critical review. J Oral Rehabil. 2010;37:143–156. doi: 10.1111/j.1365-2842.2009.02039.x. [DOI] [PubMed] [Google Scholar]
- 7.Brånemark PI, Hansson BO, Adell R, Breine U, Lindström J, Hallén O, Ohman A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977;16:1–132. [PubMed] [Google Scholar]
- 8.Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10:387–416. doi: 10.1016/s0300-9785(81)80077-4. [DOI] [PubMed] [Google Scholar]
- 9.Ekelund JA, Lindquist LW, Carlsson GE, Jemt T. Implant treatment in the edentulous mandible: a prospective study on Brånemark system implants over more than 20 years. Int J Prosthodont. 2003;16:602–608. [PubMed] [Google Scholar]
- 10.Zarb G, Jansson T, Jemt T. Other prosthodontic applications. In: Brånemark PI, Zarb GA, Albrektsson T, editors. Tissue-integrated prostheses: Osseointegration in clinical dentistry. Chicago: Quintessence; 1985. pp. 283–292. [Google Scholar]
- 11.Feine JS, Carlsson GE, editors. Implant overdentures. The standard of care for edentulous patients. Chicago: Quintessence; 2003. [Google Scholar]
- 12.Carlsson GE, Kronström M, de Baat C, Cune M, Davis D, Garefis P, Heo SJ, Jokstad A, Matsuura M, Närhi T, Ow R, Pissiotis A, Sato H, Zarb GA. A survey of the use of mandibular implant overdentures in 10 countries. Int J Prosthodont. 2004;17:211–217. [PubMed] [Google Scholar]
- 13.Mericske-Stern R. Prosthodontic management of maxillary and mandibular overdentures. In: Feine JS, Carlsson GE, editors. Implant overdentures. The standard of care for edentulous patients. Chicago: Quintessence; 2003. pp. 83–98. [Google Scholar]
- 14.Slot W, Raghoebar GM, Vissink A, Huddleston Slater JJ, Meijer HJ. A systematic review of implant-supported maxillary overdentures after a mean observation period of at least 1 year. J Clin Periodontol. 2010;37:98–110. doi: 10.1111/j.1600-051X.2009.01493.x. [DOI] [PubMed] [Google Scholar]
- 15.Bergman B, Carlsson GE. Clinical long-term study of complete denture wearers. J Prosthet Dent. 1985;53:56–61. doi: 10.1016/0022-3913(85)90066-6. [DOI] [PubMed] [Google Scholar]
- 16.Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971;26:266–279. doi: 10.1016/0022-3913(71)90069-2. [DOI] [PubMed] [Google Scholar]
- 17.Lerner UH. The biology of bone remodeling in jaw bones with and without teeth. In: Molin Thorén M, Gunne J, editors. Textbook of removable prosthodontics. The Scandinavian approach. Copenhagen: Munksgaard; 2012. pp. 51–60. [Google Scholar]
- 18.Douglass CW, Shih A, Ostry L. Will there be a need for complete dentures in the United States in 2020? J Prosthet Dent. 2002;87:5–8. doi: 10.1067/mpr.2002.121203. [DOI] [PubMed] [Google Scholar]
- 19.Owen PC. Appropriatech: prosthodontics for the many, not just for the few. Int J Prosthodont. 2004;17:261–262. [PubMed] [Google Scholar]
- 20.Carlsson GE. Responses of jawbone to pressure. Gerodontology. 2004;21:65–70. doi: 10.1111/j.1741-2358.2004.00005.x. [DOI] [PubMed] [Google Scholar]
- 21.Crum RJ, Rooney GE., Jr Alveolar bone loss in overdentures: a 5-year study. J Prosthet Dent. 1978;40:610–613. doi: 10.1016/0022-3913(78)90054-9. [DOI] [PubMed] [Google Scholar]
- 22.Preiskel HW. Overdentures made easy. A guide to implant and root supported prostheses. London: Quintessence; 1996. [Google Scholar]
- 23.Verma R, Joda T, Brägger U, Wittneben JG. A systematic review of the clinical performance of tooth-retained and implant-retained double crown prostheses with a follow-up of ≥ 3 years. J Prosthodont. 2013;22:2–12. doi: 10.1111/j.1532-849X.2012.00905.x. [DOI] [PubMed] [Google Scholar]
- 24.Sennerby L, Carlsson GE, Bergman B, Warfvinge J. Mandibular bone resorption in patients treated with tissue-integrated prostheses and in complete-denture wearers. Acta Odontol Scand. 1988;46:135–140. doi: 10.3109/00016358809004759. [DOI] [PubMed] [Google Scholar]
- 25.Davis WH, Lam PS, Marshall MW, Dorchester W, Hochwald DA, Kaminishi RM. Using restorations borne totally by anterior implants to preserve the edentulous mandible. J Am Dent Assoc. 1999;130:1183–1189. doi: 10.14219/jada.archive.1999.0372. [DOI] [PubMed] [Google Scholar]
- 26.von Wowern N, Gotfredsen K. Implant-supported overdentures, a prevention of bone loss in edentulous mandibles? A 5-year follow-up study. Clin Oral Implants Res. 2001;12:19–25. doi: 10.1034/j.1600-0501.2001.012001019.x. [DOI] [PubMed] [Google Scholar]
- 27.Wright PS, Glantz PO, Randow K, Watson RM. The effects of fixed and removable implant-stabilised prostheses on posterior mandibular residual ridge resorption. Clin Oral Implants Res. 2002;13:169–174. doi: 10.1034/j.1600-0501.2002.130207.x. [DOI] [PubMed] [Google Scholar]
- 28.Vercruyssen M, Marcelis K, Coucke W, Naert I, Quirynen M. Long-term, retrospective evaluation (implant and patient-centred outcome) of the two-implants-supported overdenture in the mandible. Part 1: survival rate. Clin Oral Implants Res. 2010;21:357–365. doi: 10.1111/j.1600-0501.2009.01849.x. [DOI] [PubMed] [Google Scholar]
- 29.Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, Head T, Lund JP, MacEntee M, Mericske-Stern R, Mojon P, Morais J, Naert I, Payne AG, Penrod J, Stoker GT, Jr, Tawse-Smith A, Taylor TD, Thomason JM, Thomson WM, Wismeijer D. The McGill Consensus Statement on Overdentures. Montreal, Quebec, Canada. May 24-25, 2002. Int J Prosthodont. 2002;15:413–414. [PubMed] [Google Scholar]
- 30.Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant retained overdentures-a review of the literature supporting the McGill and York consensus statements. J Dent. 2012;40:22–34. doi: 10.1016/j.jdent.2011.08.017. [DOI] [PubMed] [Google Scholar]
- 31.Berg E, Nesse H. Missing teeth. In: Molin Thorén M, Gunne J, editors. Textbook of removable prosthodontics. The Scandinavian approach. Copenhagen: Munksgaard; 2012. pp. 19–31. [Google Scholar]
- 32.Walton JN, MacEntee MI. Choosing or refusing oral implants: a prospective study of edentulous volunteers for a clinical trial. Int J Prosthodont. 2005;18:483–488. [PubMed] [Google Scholar]
- 33.Naert I. The influence of attachment systems on implant-retained mandibular overdentures. In: Feine JS, Carlsson GE, editors. Implant overdentures. The standard of care for edentulous patients. Chicago: Quintessence; 2003. pp. 99–109. [Google Scholar]
- 34.Ma S, Tawse-Smith A, Thomson WM, Payne AG. Marginal bone loss with mandibular two-implant overdentures using different loading protocols and attachment systems: 10-year outcomes. Int J Prosthodont. 2010;23:321–332. [PubMed] [Google Scholar]
- 35.Rutkunas V, Mizutani H, Puriene A. Conventional and early loading of two-implant supported mandibular overdentures. A systematic review. Stomatologija. 2008;10:51–61. [PubMed] [Google Scholar]
- 36.Schimmel M, Srinivasan M, Herrmann FR, Müller F. Loading protocols for implant-supported overdentures in the edentulous jaw: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2014;29:271–286. doi: 10.11607/jomi.2014suppl.g4.4. [DOI] [PubMed] [Google Scholar]
- 37.Attard NJ, Zarb GA, Laporte A. Long-term treatment costs associated with implant-supported mandibular prostheses in edentulous patients. Int J Prosthodont. 2005;18:117–123. [PubMed] [Google Scholar]
- 38.Wismeijer D, Stoker GT. Caomparison of treatment strategies for implant overdentures. In: Feine JS, Carlsson GE, editors. Implant overdentures. The standard of care for edentulous patients. Chicago: Quintessence; 2003. pp. 61–70. [Google Scholar]
- 39.Meijer HJ, Raghoebar GM, Batenburg RH, Visser A, Vissink A. Mandibular overdentures supported by two or four endosseous implants: a 10-year clinical trial. Clin Oral Implants Res. 2009;20:722–728. doi: 10.1111/j.1600-0501.2009.01710.x. [DOI] [PubMed] [Google Scholar]
- 40.Cordioli G, Majzoub Z, Castagna S. Mandibular overdentures anchored to single implants: a five-year prospective study. J Prosthet Dent. 1997;78:159–165. doi: 10.1016/s0022-3913(97)70120-3. [DOI] [PubMed] [Google Scholar]
- 41.Krennmair G, Ulm C. The symphyseal single-tooth implant for anchorage of a mandibular complete denture in geriatric patients: a clinical report. Int J Oral Maxillofac Implants. 2001;16:98–104. [PubMed] [Google Scholar]
- 42.Walton JN, Glick N, Macentee MI. A randomized clinical trial comparing patient satisfaction and prosthetic outcomes with mandibular overdentures retained by one or two implants. Int J Prosthodont. 2009;22:331–339. [PubMed] [Google Scholar]
- 43.Alsabeeha NH, Payne AG, De Silva RK, Thomson WM. Mandibular single-implant overdentures: preliminary results of a randomised-control trial on early loading with different implant diameters and attachment systems. Clin Oral Implants Res. 2011;22:330–337. doi: 10.1111/j.1600-0501.2010.02004.x. [DOI] [PubMed] [Google Scholar]
- 44.Cheng T, Sun G, Huo J, He X, Wang Y, Ren YF. Patient satisfaction and masticatory efficiency of single implant-retained mandibular overdentures using the stud and magnetic attachments. J Dent. 2012;40:1018–1023. doi: 10.1016/j.jdent.2012.08.011. [DOI] [PubMed] [Google Scholar]
- 45.Kronstrom M, Davis B, Loney R, Gerrow J, Hollender L. A prospective randomized study on the immediate loading of mandibular overdentures supported by one or two implants; a 3 year follow-up report. Clin Implant Dent Relat Res. 2014;16:323–329. doi: 10.1111/cid.12006. [DOI] [PubMed] [Google Scholar]
- 46.Roccuzzo M, Bonino F, Gaudioso L, Zwahlen M, Meijer HJ. What is the optimal number of implants for removable reconstructions? A systematic review on implant-supported overdentures. Clin Oral Implants Res. 2012;23:229–237. doi: 10.1111/j.1600-0501.2012.02544.x. [DOI] [PubMed] [Google Scholar]
- 47.Osman RB, Payne AG, Ma S. Prosthodontic maintenance of maxillary implant overdentures: a systematic literature review. Int J Prosthodont. 2012;25:381–391. [PubMed] [Google Scholar]
- 48.Raghoebar GM, Meijer HJ, Slot W, Slater JJ, Vissink A. A systematic review of implant-supported overdentures in the edentulous maxilla, compared to the mandible: How many implants? Eur J Oral Implantol. 2014;7:191–201. [PubMed] [Google Scholar]
- 49.Dudley J. Maxillary implant overdentures: current controversies. Aust Dent J. 2013;58:420–423. doi: 10.1111/adj.12116. [DOI] [PubMed] [Google Scholar]
- 50.Kronström M, Carlsson GE. Use of mandibular implant overdentures: treatment policy in prosthodontic specialist clinics in Sweden. Swed Dent J. 2003;27:59–66. [PubMed] [Google Scholar]
- 51.Ascher A, Carlsson GE, Kronström M. Use of implant-supported prostheses in edentulous mandibles among prosthodontists in Sweden. Swed Dent J. 2014 in press. [PubMed] [Google Scholar]
- 52.Zarb GA. Introduction to osseointegration in clinical dentistry. J Prosthet Dent. 1983;49:824. [Google Scholar]
- 53.Lindquist LW, Carlsson GE. Long-term effects on chewing with mandibular fixed prostheses on osseointegrated implants. Acta Odontol Scand. 1985;43:39–45. doi: 10.3109/00016358509064138. [DOI] [PubMed] [Google Scholar]