

Abstract
Liver transplantation and blood purification therapy, including plasmapheresis, hemodiafiltration, and bioartificial liver support, are the available treatments for patients with severe hepatic failure. Bioartificial liver support, in which living liver tissue is used to support hepatic function, has been anticipated as an effective treatment for hepatic failure. The two mainstream systems developed for bioartificial liver support are extracorporeal whole liver perfusion (ECLP) and bioreactor systems. Comparing various types of bioartificial liver in view of function, safety, and operability, we concluded that the best efficacy can be provided by the ECLP system. Moreover, in our subsequent experiments comparing ECLP and apheresis therapy, ECLP offers more ammonia metabolism than HD and HF. In addition, ECLP can compensate amino acid imbalance and can secret bile. A controversial point with ECLP is the procedure is labor intensive, resulting in high costs. However, ECLP has the potential to reduce elevated serum ammonia levels of hepatic coma patients in a short duration. When these problems are solved, bioartificial liver support, especially ECLP, can be adopted as an option in ordinary clinical therapy to treat patients with hepatic failure.
Keywords: Bioartificial liver support, Blood purification therapy, Extracorporeal liver perfusion, Bioreactor, Transgenic pig
INTRODUCTION
Organ replacement by artificial organ technologies has progressed remarkably in the past decades. The temporary replacement of heart and lung functions has permitted major improvements in cardiac surgery, and renal dialysis has revolutionized the prognosis in acute and chronic renal failure. However, the clinical treatment of fatal hepatic failure with living liver support systems has been far from satisfactory.
The liver is the chief metabolic and synthetic organ and it carries out more than 500 different functions that are difficult to replace by substitute methods. The destruction of homeostasis that is caused by hepatic failure results in a life crisis. This has promoted much research into living liver tissue support to perform various hepatic functions, however, the development of bioartificial liver support is remarkably delayed compared to the development of artificial kidney and artificial heart.
Liver transplantation and blood purification therapy, including plasmapheresis, hemodiafiltration, and bioartificial liver support, are the available treatments for patients with severe hepatic failure. Plasmapheresis involves separating and replacing the plasma of patients in hepatic failure and this treatment has confirmed beneficial effects for patients. Its major drawback lies in the cost of economic and medical resources because it requires a large volume of fresh frozen plasma. Bioartificial liver support, in which living liver tissue supports hepatic function, is anticipated to be an effective treatment for hepatic failure. This review focuses on the development of artificial and bioartificial liver support and evaluates the most desirable strategy for blood purification therapy for hepatic failure patients.
ARTIFICIAL LIVER SUPPORT
Table 1 shows the development of blood purification therapy for hepatic failure. The first extracorporeal perfusion treatments for hepatic failure were applications of artificial hepatic function devices. During the 1950s, hemodialysis was introduced as an optimal treatment for renal failure by removing uremic substances based on the theory of diffusion; that is, the solute substances move according to a concentration incline, and this treatment has prevailed in daily clinical medicine as a reliable therapy for renal failure patients. In 1958, hemodialysis was carried out on patients with hepatic failure in an attempt to remove the toxins thought to cause hepatic encephalopathy. Killey et al[1] reported an uncontrolled study of five patients with chronic hepatic failure, four of whom showed improvement in their metabolic encephalopathy, although long term survival was not achieved.
Table 1.
Development of blood purification therapyin the treatment of liver failure
| 1958 | Killey | Treatment of a hepatic coma patient using hemodialysis |
| 1958 | Schechter | Treatment of a hyperammonemia patient using an ion-exchange column |
| 1958 | Lee, Tink | Exchange transfusion |
| 1958 | Hori | Cross-hemodialysis using living dogs |
| 1965 | Yatzidis | Bilirubin adsorbent using activated charcoal |
| 1965 | Eisemann | Initial clinical use of ECLP using a resected porcine liver |
| 1967 | Burnell | Cross-hemodialysis between a patient in hepatic coma and a healthy donor |
| 1968 | Sabin | Plasma exchange (Plasmapheresis) |
| 1970 | Abouna | Clinical use of ECLP using a xenogeneic liver |
| 1976 | Opolon | Treatment of a patient with fulminant hepatitis using a dialyzer made of a polyacrilonitril membrane |
| 1976 | Knell, Dukes | Control of amino acid imbalance using BCAA solution |
| 1978 | Yamazaki | Incorporated system of plasmapheresis and hemodialysis |
| 1980 | Brunner | Bioreactor immobilized with hepatic enzymes |
| 1982 | Ozawa | Cross-hemodialysis using porcine and baboon livers |
| 1985 | Teraoka | XDHP and CPP using porcine liver |
| 1987 | Matsumura | Perfusion system of suspended rabbit hepatocytes |
| 1988 | Marguilis | Perfusion system of suspended porcine hepatocytes |
| 1992 | Yoshiba | Incorporated system of plasmapheresis and hemodiafiltration |
| 1993 | Demetriou | Bioreactor system of immobilized porcine hepatocytes |
| 1994 | Gerlach | Bioreactor system of immobilized hepatocytes |
| 2000 | Stange | Molecular adsorbent recirculating system (MARS) |
For more aggressive removal of protein bound molecules, two forms of mechanical liver support were developed: hemoperfusion and plasmaperfusion. One method involved an adsorbent device able to substitute some hepatic functions by removing toxic substances from the blood. In 1958, Schechter et al[2] introduced direct extracorporeal hemoperfusion over an ion-exchange resin matrices column (Dowex 50-X8), which achieved removal of blood ammonia and reversal of coma in 20% of patients. Also in 1958, Lee and Tink et al[3] reported the successful treatment of a patient in hepatic coma by exchange transfusions with fresh blood. This trial was based on the concept that the detoxification, regulation, and synthetic functions of the liver can be realized by exchanging the blood volume of a patient in hepatic failure. Neurologic improvements and survival were repeatedly suggested, but this conception was replaced later by the effective method of plasma exchange.
Considerable experience has been gained using activated charcoal as an adsorbent of possible toxins in the range of 500 to 5000 daltons in whole blood or plasma in patients in hepatic failure[4,5]. In 1965, Yatzidis et al[4] developed an activated charcoal column for removing serum bilirubin, which is still used for patients suffering from hyperbilirubinemia. Its initial primary side effects were platelet loss and anaphylaxy shock, which have been controlled by plasma separation or prostaglandin administration.
One of the most straightforward approaches to biological liver support is cross-circulation, which was reported in 1967 by Burnell et al[6]. In this technique, which is performed under general anesthesia, the circulation of patients with hepatic failure is directly connected to that of healthy human donors. One of three patients were reported to be fully recovered, but the donors suffered from severe adverse reactions during the procedure. It was demonstrated that liver support could be provided with an external liver, but the donor suffered serious toxic side effects from the hepatic failure blood, resulting in cessation of further trials.
Plasma exchange, or plasmapheresis, was introduced by Sabin et al[7] in 1968. This plasma separation technique, using either a centrifuge or a membrane, separated plasma that was then discarded and replaced by an equivalent volume of fresh plasma. Yamazaki et al[8] developed a combination technique of plasmapheresis and hemodialysis that proved effective for reversing hepatic coma and improving coagulation. A major problem with this method was the need for a large volume of normal plasma as a substitute.
The kidney produces urine mainly by filtration in glomeruli. A high quality membrane was needed to modify the dialyser to be equivalent to glomeruli. During the latter 1960s, Henderson et al[9] created a novel approach to the hemofiltration method by using a polysulfone membrane.
Considering cellulosic membranes that are permeable to small water-soluble molecules, in 1976, Opolon et al[10] used a polyacrylonitril membrane to improve the diffusive transfer of substances up to 15 000 daltons by removing medium-weight solutes and small peptides. In a clinical study of 24 patients with acute fulminant viral hepatitis, hemodialysis with this membrane achieved a coma reversal rate of 54%, but the survival times were not improved. An important conclusion from these experiments was that substances of less than 15 000 daltons in molecular weight were associated with metabolic encephalopathy. Also in 1976, Knell and Dukes et al[11] introduced reciprocal dialysis in which a dialysis fluid with an amino acid concentration identical to that of normal plasma was used to correct increased aromatic amino acids and decreased branched-chain amino acids.
Hemodialysis is effective in removing small sized molecules that are under 5000 in molecular weight, and hemofiltration is especially effective in removing larger sized molecules of 5000 to 10 000 in molecular weight. Thus, a combination therapy of hemodialysis and hemofiltration has the potential to be an ideal therapy for severe renal failure and hepatic failure. In 1977, Ota et al[12] developed the hemodiafiltration (HDF) method, in which a great deal of water, as much as 101, is removed and a physiological solution is supplied to adjust for the quantity of water removal. In this method, a dialyser consisting of a hollow fiber membrane with a larger pore size than is used in ordinary hemodialysis, enables removing larger molecules.
In an attempt to provide more specific detoxification therapy, immobilized enzyme systems were developed during the 1980s. In these systems, blood is perfused over liver enzymes that are either linked to an insoluble substrate or encapsulated in artificial cells[13,14]. It is desirable to control hyperammoniemia with a single column containing an immobilized enzyme, but these columns are costly and it is difficult to activate enzymes and keep them activated on request.
During the early 1990s, Yoshiba et al[15] consecutively treated 27 patients who had fulminant hepatitis by using plasma exchange in combination with continuous hemodiafiltration, using a high performance membrane (polymethylmetacrylate). Treatment was considered successful for 15 of 27 treated patients, who survived after a mean 16.1 sessions over a mean 19.3 d. The effectiveness of this method (55.6% survival) was attributed to its early application.
Stange and Mitzner et al[16] introduced a new dialysis method using their originally developed molecular adsorbent re-circulating system, and applied it to 26 patients with hepatorenal syndrome. They reported a significant decrease in serum bilirubin and creatinine levels in the treated groups, which enabled this procedure to be one of the most important options for treating hepatic failure.
BIOARTIFICIAL LIVER SUPPORT
The liver has more than 500 different functions, which are difficult to replace by one or a few substitute methods, and this has provoked much research into living liver tissue supporting hepatic functions. In 1958, Hori et al[17] conducted a primary trial of perfusion treatment using xenogeneic livers and a cross-hemodialysis method consisting of the blood circuits of a patient with cirrhosis and four living dogs. The circuits were separated by a semipermiable membrane, through which low and middle molecular weight waste products from the patient passed into the animals’ circuit to be metabolized by canine livers and absorbed into an ion-exchange resin matrix column (Figure 1). This treatment was applied to four patients with cirrhosis, one of whom recovered temporarily from hepatic coma after a remarkable decrease in serum ammonia levels.
Figure 1.
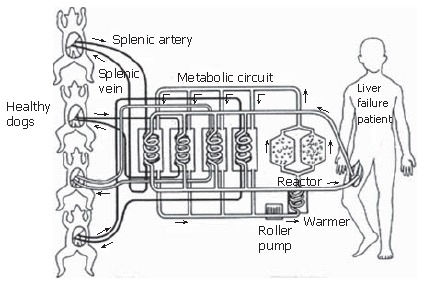
Cross dialysis treatment using four living dogs (Hori et al 1958).
After an initial clinical study by Eisemann et al[18] in 1965 using whole porcine liver for direct hemoperfusion, many research groups conducted clinical trials of extracorporeal liver perfusion (ECLP). Abouna et al[19] clarified that humans have immune responses to pig proteins and that anaphylactic reactions to liver from another species sometimes occurred.
In 1974 in Japan, aggressive clinical trials of ECLP were also performed. Kawamura et al[20] clinically applied ECLP using porcine liver for a hepatic coma patient suffering from acute phosphorus intoxication (Figure 2). Direct hemoperfusion was performed, however, the clinical status was so severe that the patient could not be saved. During the early 1980s, Ozawa et al[21] developed a cross hemodialysis method using resected porcine or baboon livers, which achieved an overall survival rate of 27% in 13 patients with severe hepatic failure (Figure 3). In 1985, Teraoka et al[22] used resected whole porcine liver to treat hepatic failure, with direct hemoperfusion for one patient and cross plasma perfusion for two patients (Figure 4).
Figure 2.

ECLP applied for acute phosphorus intoxication patient (Kawamura et al 1974).
Figure 3.
ECLP using baboon or porcine livers (Ozawa et al 1982).
Figure 4.
ECLP using porcine livers (Teraoka et al 1985).
In the 1990s, a renewed interest, based on experimental studies, led Fox et al[23] to use allogenic ECLP in the management of three patients with fulminant hepatic failure. They used human cadaveric livers, which improved the perfusion time to 72 h, resulting in two patients being successfully bridged to liver transplantation. Other trials were performed by Chiari[24], and Neuhaus[25] using porcine livers.
New trials of ECLP are being carried out using transgenic porcine livers. Levi et al[26] reported the first two cases of ECLP using transgenic porcine livers to overcome a potential immunologic barrier (hCD55/hCD59) and both were successfully bridged to liver transplantation. Xu performed a clinical trial of extracorporeal perfusion treatment using transgenic whole porcine liver in two patients, and reported no symptoms of porcine endogenous retrovirus (PERV) infection[27].
Another bioartificial liver support approach is the hybrid bioartificial liver system in which hepatocytes isolated with chelating solution and collagenase solution are cultured in artificial devices. In 1987, Matsumura et al[28] reported the first clinical use of a suspension-cultured hepatocyte system using a hemodialysis chamber in which about 100 g of cryopreserved rabbit hepatocytes (about 1 × 1010 cells) were seeded. A patient in hepatic failure underwent repetitive dialysis using these hepatocyte suspensions, which resulted in a 68% decrease in total serum bilirubin and improved mental status. However, no further clinical use of this system has been reported subsequently.
Hepatocytes are anchorage-dependent cells that must adhere to survive. Thus, hybrid bioartificial liver systems, incorporated with bioreactors immobilized with hepatocytes or a bioreactor system, have been developed and tested in primary clinical trials during the past 10 years. Demetriou et al[29] developed a hollow-fiber bioreactor system within which porcine hepatocytes are seeded in the extrafiber space. This system has been used in the treatment of about 200 patients with hepatic failure but there seems to be equivalent hepatocyte suspension as with other treatments with a doubtful number of intact cells. Gerlach et al[30] introduced another interesting bioreactor design, which is a three-dimensional woven capillary network bioreactor containing hepatocytes immobilized in the extrafiber spaces. This system was applied in nine patients using porcine hepatocytes, and in eight patients using human hepatocytes obtained from a cadaveric donor liver that was unsuitable for transplantation because of severe injury. In Italy, Flendrig and Van de Kerkhove et al[31] developed a bioreactor using polyester non-woven fabric. They reported promising results for its clinical use to treat hepatic coma in seven patients using porcine hepatocytes with perfusion periods of 8 to 35 h. Patzer et al[32] investigated the efficacy of hemoperfusion compared with plasma perfusion by using a hollow-fiber bioreactor, which is currently utilized for clinical use with porcine hepatocytes.
In Japan, many research groups are engaged in developing bioreactor systems. Uchino et al[33] developed a pioneering system, composed of 200 collagen-coated glass plates bearing monolayer cultured canine hepatocytes stacked in an acrylic resin box. The bioreactor design appeared to be efficient, but its labor-intensive assembly prevented its widespread use.
OUR DEVELOPMENTS
Our group has developed various types of the hepatic functioning units; i.e., ECLP or bioreactor systems, for bioartificial liver systems. We devised a bioreactor filled with hepatocytes that were immobilized on a collagen-coated non-woven polyester fabric that can accommodate 2-3 × 1010 viable hepatocytes per unit and allows direct contact between hepatocytes and perfused blood[34]. We also developed an original accommodation device of whole liver for extracorporeal perfusion in which the liver is placed in a physiological state that is supported by a special tube inserted into the inferior vena cava with pulsatory blood flow perfused by an artificial heart pump to dilate peripheral vessels and supply oxygenated whole blood to the peripheral liver tissue[35].
In bioartificial liver support in which xenogeneic liver tissue is used, it is necessary to establish a method for perfusing xenogeneic whole blood through a hepatic functioning unit without hyperacute rejection occurring. Therefore, we devised a method of xenogeneic direct hemoperfusion consisting of a leukocyte adsorbent column, an immunoglobulin adsorbent column, and a hepatic functioning unit[36]. Furthermore, we developed a method of cross plasma perfusion in which plasma exchange is carried out between the blood circuit of the patient’s side and that of the hepatic functioning unit through which immunologically free whole human blood is perfused in order to achieve epidemic safety for the patient. Comparing various types of bioartificial liver in our ex vivo perfusion experiments, we concluded that the best efficacy can be performed by the ECLP system in view of function, safety, and operability[37].
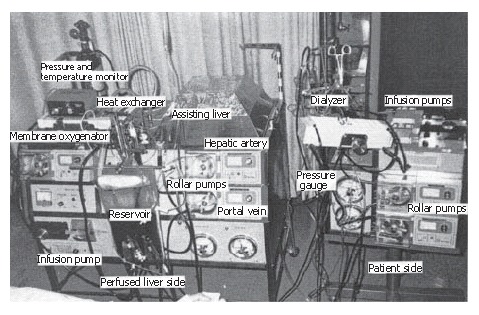
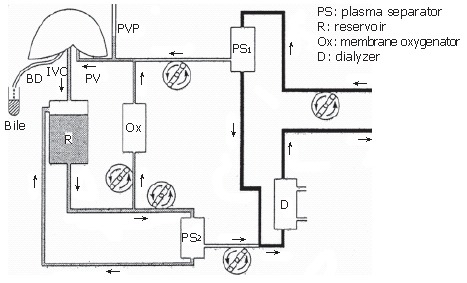
Furthermore, we performed perfusion experiments to compare efficacy between ECLP and apheresis therapy as hemodialysis (HD) and hemofiltration (HF). A Sangen strain pig was surgically induced to hepatic failure by side-to-side portocaval shunting and ligation of the entire hepatoduodenal ligament in the porta hepatis. HD was performed with a dialysate pump at 300-350 mL/min. HF was performed by a post-dilution method with a filtration pump at 2 L/h, a supplement pump at 0.5-1 L/h, and a dialysate pump at 1-1.5 L/h. A renal preservation device (RM3: Waters medical systems; Rochester, USA) was employed for ECLP in direct hemoperfusion (Figure 5). Perfusion treatment was initiated at 3 h after completion of the surgical induction of hepatic failure and continued for 3 h. As a result, in the hepatic failure control group with no treatment, serum ammonia levels increased continuously. In the HF group, it also increased continuously although the rate increase was restricted. In the HD group, it increased or gradually decreased depending on the particular case, and the average rate was almost zero. In the ECLP group, it decreased significantly, exhibiting the most superior efficacy of all the groups, and any kind of apheresis was apparently inferior to ECLP (Figure 6A). Regarding Fischer’s ratio, in the Control, HF, and HD groups, it decreased continuously, although the decreasing rate was restricted in the apheresis group probably due to dilution. In the ECLP group, it increased constantly. This result shows that ECLP containing living liver can compensate for an amino acid imbalance, but apheresis therapy using an artificial membrane cannot control the amino acid balance (Figure 6B). Furthermore, ECLP secreted bile approximately 10 mL/h during the perfusion treatment. In summary, ECLP has a higher metabolic function with ammonia than HD and HF, and ECLP can compensate amino acid imbalance and secret bile, while HD and HF cannot. ECLP has the potential to reduce elevated serum ammonia levels of hepatic coma patients in a short duration and can be one option to treat hepatic failure patients in ordinary clinical therapy.
Figure 5.

Ex vivo direct hemoperfusion experiment of ECLP (Naruse et al).
Figure 6.
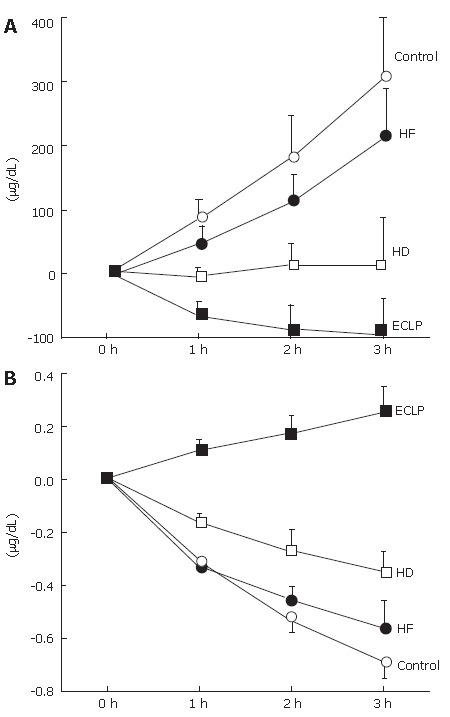
Comparison of efficacy between ECLP and apheresis therapy. (A): Ammonia; (B) Fischer’s ratio. ○: Control group; ●: Hemofiltration (HF) group; □:hemodialysis (HD) group; ■: ECLP group.
PERSPECTIVES
Many excellent systems of bioartificial liver support have been developed, in which ECLP is likely to become a most important procedure. On the other hand, xenogeneic protein influx into the patient during on-line perfusion in bioartificial liver support is an ongoing problem. Moreover, the social antagonism for zoonosis has consistently been raised as a controversial subject surrounding the use of xenogeneic organs for treating humans. However, zoonosis does not seem to be an essential problem except for an individual’s sense against treatment using animal tissue. Rather, the essential problem of bioartificial liver support is the high requirement of labor, resulting in high working costs. When these problems are solved, bioartificial liver support, especially ECLP, will greatly contribute to the treatment of patients suffering from severe hepatic failure, resulting in elevated human medicine and welfare.
Footnotes
S- Editor Liu Y L- Editor Lutze M E- Editor Lu W
References
- 1.Kiley JE, Pender JC, Welch HF, Welch CS. Ammonia intoxication treated by hemodialysis. N Engl J Med. 1958;259:1156–1161. doi: 10.1056/NEJM195812112592403. [DOI] [PubMed] [Google Scholar]
- 2.Schechter DC, Nealon TF, Gibbon JH. A simple extracorporeal device for reducing elevated blood ammonia levels; preliminary report. Surgery. 1958;44:892–897. [PubMed] [Google Scholar]
- 3.Lee C, Tink A. Exchange transfusion in hepatic coma: report of a case. Med J Aust. 1958;45:40–42. doi: 10.5694/j.1326-5377.1958.tb85989.x. [DOI] [PubMed] [Google Scholar]
- 4.Yatzidis H, Oreoploulos D, Triataphyllides D. Voudiclari S, Tsaparas N, Gavras C, Stavroulaki A. Treatment of severe barbiturate poisoning. Lancet. 1965;1:216–217. doi: 10.1016/s0140-6736(65)90698-7. [DOI] [PubMed] [Google Scholar]
- 5.Chang TM. Haemoperfusions over microencapsulated adsorbent in a patient with hepatic coma. Lancet. 1972;2:1371–1372. doi: 10.1016/s0140-6736(72)92821-8. [DOI] [PubMed] [Google Scholar]
- 6.Burnell JM, Dawborn JK, Epstein RB, Gutman RA, Leinbach GE, Thomas ED, Volwiler W. Acute hepatic coma treated by cross-circulation or exchange transfusion. N Engl J Med. 1967;276:935–943. doi: 10.1056/NEJM196704272761701. [DOI] [PubMed] [Google Scholar]
- 7.Sabin S, Merritt JA. Treatment of hepatic coma in cirrhosis by plasmapheresis and plasma infusion (plasma exchange) Ann Intern Med. 1968;68:1–7. doi: 10.7326/0003-4819-68-1-1. [DOI] [PubMed] [Google Scholar]
- 8.Yamazaki Z, Kanai F, Idezuki Y, Inoue N. Extracorporeal methods of liver failure treatment. Biomater Artif Cells Artif Organs. 1992;15:667–675. [PubMed] [Google Scholar]
- 9.Henderson LW, Parker HR, Schroeder JP, Frigon R, Sanfelippo ML. Continuous low flow hemofiltration with sorbent regeneration of ultrafiltrate. Trans Am Soc Artif Intern Organs. 1978;24:178–184. [PubMed] [Google Scholar]
- 10.Opolon P, Rapin JR, Huguet C, Granger A, Delorme ML, Boschat M, Sausse A. Hepatic failure coma (HFC) treated by polyacrylonitrile membrane (PAN) hemodialysis (HD) Trans Am Soc Artif Intern Organs. 1976;22:701–710. [PubMed] [Google Scholar]
- 11.Knell AJ, Dukes DC. Dialysis procedures in acute liver coma. Lancet. 1976;2:402–403. doi: 10.1016/s0140-6736(76)92412-0. [DOI] [PubMed] [Google Scholar]
- 12.Ota K, Suzuki T, Ozaku Y, Hoshino T, Agishi T, Sugino N. Short-time hemodiafiltration using polymethylmethacrylate hemodiafilter. Trans Am Soc Artif Intern Organs. 1978;24:454–457. [PubMed] [Google Scholar]
- 13.Brunner G, Tegtmeier F. Enzymatic detoxification using lipophilic hollow-fiber membranes: I. Glucuronidation reactions. Artif Organs. 1984;8:161–166. doi: 10.1111/j.1525-1594.1984.tb04266.x. [DOI] [PubMed] [Google Scholar]
- 14.Lavin A, Sung C, Klibanov AM, Langer R. Enzymatic removal of bilirubin from blood: a potential treatment for neonatal jaundice. Science. 1985;230:543–545. doi: 10.1126/science.4048947. [DOI] [PubMed] [Google Scholar]
- 15.Yoshiba M, Yamada H, Yoshikawa Y, Fujiwara K, Toda G, Oka H, Sanjo T, Yamazaki Z, Idezuki Y, Inoue N. Hemodiafiltration treatment of deep hepatic coma by protein passing membrane: case report. Artif Organs. 1986;10:417–419. doi: 10.1111/j.1525-1594.1986.tb02590.x. [DOI] [PubMed] [Google Scholar]
- 16.Stange J, Mitzner SR, Klammt S, Freytag J, Peszynski P, Loock J, Hickstein H, Korten G, Schmidt R, Hentschel J, et al. Liver support by extracorporeal blood purification: a clinical observation. Liver Transpl. 2000;6:603–613. doi: 10.1053/jlts.2000.7576. [DOI] [PubMed] [Google Scholar]
- 17.Kimoto S. The artificial liver: experiments and clinical application. Trans Am Soc Artif Intern Organs. 1959;5:102–112. [Google Scholar]
- 18.Eiseman B, Liem DS, Raffucci F. Heterologous liver perfusion in treatment of hepatic failure. Ann Surg. 1965;162:329–345. doi: 10.1097/00000658-196509000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Abouna GM, Boehmig HG, Serrou B, Amemiya H, Martineau G. Long-term hepatic support by intermittent multi-species liver perfusions. Lancet. 1970;2:391–396. doi: 10.1016/s0140-6736(70)90006-1. [DOI] [PubMed] [Google Scholar]
- 20.Kawamura A. Jinkouzouki. Japanese J Artif Organ. 2003;32:1–6. [Google Scholar]
- 21.Ozawa K, Kamiyama Y, Kimura K, Ukikusa M, Kono Y, Yamato T, Shimahara Y, Nakatani T, Asano M, Irie R, et al. The effects of heterologous liver cross-hemodialysis on adenylate energy charge of the remnant liver after major hepatic resection. Artif Organs. 1982;6:447–452. doi: 10.1111/j.1525-1594.1982.tb04142.x. [DOI] [PubMed] [Google Scholar]
- 22.Teraoka S, Honda H, Fuchinoue S, Oshima T, Agishi T, Ota T. Ex vivo liver perfusion for acute liver failure. Saishin-Igaku. 1987;42:1630–1639. [Google Scholar]
- 23.Fox IJ, Langnas AN, Fristoe LW, Shaefer MS, Vogel JE, Antonson DL, Donovan JP, Heffron TG, Markin RS, Sorrell MF. Successful application of extracorporeal liver perfusion: a technology whose time has come. Am J Gastroenterol. 1993;88:1876–1881. [PubMed] [Google Scholar]
- 24.Chari RS, Collins BH, Magee JC, DiMaio JM, Kirk AD, Harland RC, McCann RL, Platt JL, Meyers WC. Brief report: treatment of hepatic failure with ex vivo pig-liver perfusion followed by liver transplantation. N Engl J Med. 1994;331:234–237. doi: 10.1056/NEJM199407283310404. [DOI] [PubMed] [Google Scholar]
- 25.Neuhaus P, Blumhardt G. Extracorporeal liver perfusion: applications of an improved model for experimental studies of the liver. Int J Artif Organs. 1993;16:729–739. [PubMed] [Google Scholar]
- 26.Levy MF, Crippin J, Sutton S, Netto G, McCormack J, Curiel T, Goldstein RM, Newman JT, Gonwa TA, Banchereau J, et al. Liver allotransplantation after extracorporeal hepatic support with transgenic (hCD55/hCD59) porcine livers: clinical results and lack of pig-to-human transmission of the porcine endogenous retrovirus. Transplantation. 2000;69:272–280. doi: 10.1097/00007890-200001270-00013. [DOI] [PubMed] [Google Scholar]
- 27.Xu H, Sharma A, Okabe J, Cui C, Huang L, Wei YY, Wan H, Lei Y, Logan JS, Levy MF, et al. Serologic analysis of anti-porcine endogenous retroviruses immune responses in humans after ex vivo transgenic pig liver perfusion. ASAIO J. 2003;49:407–416. [PubMed] [Google Scholar]
- 28.Matsumura KN, Guevara GR, Huston H, Hamilton WL, Rikimaru M, Yamasaki G, Matsumura MS. Hybrid bioartificial liver in hepatic failure: preliminary clinical report. Surgery. 1987;101:99–103. [PubMed] [Google Scholar]
- 29.Rozga J, Holzman MD, Ro MS, Griffin DW, Neuzil DF, Giorgio T, Moscioni AD, Demetriou AA. Development of a hybrid bioartificial liver. Ann Surg. 1993;217:502–509; discussion 509- 511. doi: 10.1097/00000658-199305010-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gerlach JC, Encke J, Hole O, Müller C, Ryan CJ, Neuhaus P. Bioreactor for a larger scale hepatocyte in vitro perfusion. Transplantation. 1994;58:984–988. doi: 10.1097/00007890-199411150-00002. [DOI] [PubMed] [Google Scholar]
- 31.Flendrig LM, Calise F, Di Florio E, Mancini A, Ceriello A, Santaniello W, Mezza E, Sicoli F, Belleza G, Bracco A, et al. Significantly improved survival time in pigs with complete liver ischemia treated with a novel bioartificial liver. Int J Artif Organs. 1999;22:701–709. [PubMed] [Google Scholar]
- 32.Mazariegos GV, Patzer JF, Lopez RC, Giraldo M, Devera ME, Grogan TA, Zhu Y, Fulmer ML, Amiot BP, Kramer DJ. First clinical use of a novel bioartificial liver support system (BLSS) Am J Transplant. 2002;2:260–266. doi: 10.1034/j.1600-6143.2002.20311.x. [DOI] [PubMed] [Google Scholar]
- 33.Uchino J, Tsuburaya T, Kumagai F, Hase T, Hamada T, Komai T, Funatsu A, Hashimura E, Nakamura K, Kon T. A hybrid bioartificial liver composed of multiplated hepatocyte monolayers. ASAIO Trans. 1988;34:972–977. [PubMed] [Google Scholar]
- 34.Naruse K, Sakai Y, Lei G, Sakamoto Y, Kobayashi T, Puliatti C, Aronica G, Morale W, Leone F, Qiang S, et al. Efficacy of nonwoven fabric bioreactor immobilized with porcine hepatocytes for ex vivo xenogeneic perfusion treatment of liver failure in dogs. Artif Organs. 2001;25:273–280. [PubMed] [Google Scholar]
- 35.Naruse K, Sakai Y, Guo L, Natori T, Shindoh J, Karasawa Y, Iida Y, Kojima K, Michishita K, Makuuchi M. Development of a new extracorporeal whole-liver perfusion system. J Artif Organs. 2003;6:211–217. doi: 10.1007/s10047-003-0225-9. [DOI] [PubMed] [Google Scholar]
- 36.Naruse K, Sakai Y, Natori T, Guo L, Shindoh J, Iida Y, Michishita K, Karasawa Y, Kojima K, Makuuchi M. Xenogeneic direct hemoperfusion using whole swine liver for liver failure in dogs. J Surg Res. 2003;111:229–235. doi: 10.1016/s0022-4804(03)00045-3. [DOI] [PubMed] [Google Scholar]
- 37.Naruse K, Nagashima H, Sakai Y, Kokudo N, Makuuchi M. Development and perspectives of perfusion treatment for liver failure. Surg Today. 2005;35:507–517. doi: 10.1007/s00595-004-2980-5. [DOI] [PubMed] [Google Scholar]