

Abstract
Herpes simplex esophagitis (HSE) is well documented in immunosuppressed patients. However, it is rare in the immunocompetent host. We present a case of HSE in a 21 year-old healthy lady who was admitted to our unit with dysphagia, odynophagia and chest pain. Clinical examination revealed mild epigastric tenderness and admission bloods including full blood picture, electrolytes and inflammatory markers were normal. She underwent an esophagogastroduodenoscopy (EGD) which revealed severe exudative, well-circumscribed ulcerations in her distal esophagus. Biopsies confirmed severe esophagitis with acute ulceration and subsequent polymerase chain reaction (PCR) confirmed herpes simplex virus (HSV) type 1. Subsequent assessment failed to identify an immune disorder. HSE should be suspected when faced with characteristic endoscopic findings, even if the patient is immunocompetent. When the diagnosis of HSE is confirmed, an immune deficiency should be sought.
Keywords: Herpes simplex, Esophagitis, Immuno-competent
INTRODUCTION
Herpes simplex esophagitis (HSE) in immunocompromised hosts is well documented in the literature[1,2]. It represents both reactivation of the virus during immunosuppression and primary infection, although the former is common[2]. HSE in immunocompetent adults is a rare but distinct clinical entity. Previously limited to anecdotal reports only, a recent literature review on HSE in immunocompetent hosts has identified 38 cases, mainly affecting young males[3].
CASE REPORT
A 21 year-old lady presented to our gastroenterology unit with an acute onset of dysphagia, odynophagia and retrosternal chest pain. Her symptoms were preceded by a possible acute food bolus obstruction one week previously. She was not able to tolerate any oral intake, prompting admission for intravenous hydration. There was no personal or family history of antecedent herpes simplex viral exposure. Apart from stable asthma, she was otherwise a fit and healthy young lady. Her only medication was Symbicort® inhaler (Astra Zeneca UK). On examination, she was apyrexic and there was no oral thrush or stomatitis. There was mild tenderness in her epigastrium. Her routine admission profile, full blood picture and inflammatory markers were all normal. An esophagogastroduodenoscopy (EGD) was performed and revealed severe distal exudative esophagitis with deep, circumscribed ulceration (Figure 1). The rest of the endoscopic examination was normal. Multiple esophageal biopsies were obtained and sent for both histopathology and viral culture.
Figure 1.
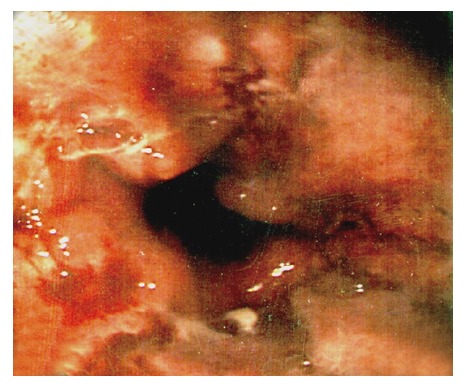
Distal esophagus.
Histopathology from the esophageal biopsy specimens was consistent with acute, severe inflammation, but no viral inclusion bodies, fungi or parasites were seen. However, biopsies were positive for herpes simplex virus (HSV) (type 1) DNA by polymerase chain reaction (PCR) confirming the diagnosis of Herpes simplex esophagitis (HSE).
Her symptoms were self-limiting and resolved completely within 48 h, aided with high dose proton-pump inhibitor and sucralfate. Treatment with acyclovir was not required. She had no risk factors for HIV infection and declined HIV testing.
DISCUSSION
HSE in immunocompetent hosts is a rare but distinct clinical entity. It may represent either a primary disease or reactivation of a latent infection. The typical patient is a young (< 40 years), healthy male[4] who presents with acute odynophagia, dysphagia or heartburn, with or without prodromal symptoms (fever, pharyngitis, respiratory symptoms) or oral lesions. Prior exposure to a family member with possible HSV lesions has been reported[4].
HSE has characteristic endoscopic appearances. In the early stage, vesicles are seen, which then slough to form discrete, circumscribed ulcers with raised edges. These lesions have punched-out or volcano-like appearances[4]. Cobblestoning can be seen due to clustering of these lesions. Exudates are present in a majority of cases[4,5]. Mucosal necrosis is seen in the late stage[6]. The distal or mid-esophagus is most commonly involved, although in some cases the entire esophagus is affected.
If HSE is clinically suspected, biopsies from the ulcer edges should be obtained for both histopathology and viral culture[7]. Virus isolation by cell culture has traditionally been considered the diagnostic ‘gold standard’ for herpes simplex infection. However, in recent years, HSV DNA PCR is fast becoming an invaluable tool in the diagnostic armamentarium of herpes simplex infection. In one of the earliest studies comparing PCR, viral culture and HSV antigen detection by enzyme immunoassay (EIA) in diagnosing genital herpes in a cohort of 194 patients, HSV was detected in 115 patients (59%) by PCR, 93 (48%) by cell culture and 75 (39%) by EIA. The sensitivity of culture to PCR was reported to be 80.9% (93/115) and that of EIA to PCR was 65.2% (75/115)[8]. This study showed that PCR is the most sensitive method compared to viral culture and EIA. Further comparative studies have confirmed that PCR is the most sensitive, cost effective, rapid and easiest diagnostic tool[9,10]. Improved technology in conventional PCR has led to the development of real-time PCR. The superiority of real-time PCR to conventional diagnostic modalities is the rapidity of diagnosis (2.5 h vs 4 h for EIA, 9 h for conventional PCR and 4 d for culture)[11,12]. This prompt diagnosis can help facilitate early initiation of antiviral treatment and, as such, can potentially become the diagnostic tool of choice in the near future. Serology is of limited value as a majority of healthy individuals will have a prior exposure to HSV, unless there is seroconversion.
HSE is generally a self-limiting condition but can be complicated by perforation[13] and bleeding[14]. Antiviral therapy, in the early stage, is advisable to hasten recovery and to achieve symptomatic relief within a short space of time, although currently there are no controlled trials on the effect of acyclovir therapy in healthy subjects[15]. Recurrence of this condition is rare.
We should have a high index of suspicion for HSE when faced with a young patient with odynophagia, dysphagia or heartburn who has distal ulcerative esophagitis without an obvious cause. Whenever HSE is diagnosed in an immunocompetent patient, a careful history and assessment for an immune disorder such as HIV infection is crucial.
Footnotes
S- Editor Zhu LH L- Editor Wang XL E- Editor Chen GJ
References
- 1.McBane RD, Gross JB. Herpes esophagitis: clinical syndrome, endoscopic appearance, and diagnosis in 23 patients. Gastrointest Endosc. 1991;37:600–603. doi: 10.1016/s0016-5107(91)70862-6. [DOI] [PubMed] [Google Scholar]
- 2.Buss DH, Scharyj M. Herpesvirus infection of the esophagus and other visceral organs in adults. Incidence and clinical significance. Am J Med. 1979;66:457–462. doi: 10.1016/0002-9343(79)91068-4. [DOI] [PubMed] [Google Scholar]
- 3.Ramanathan J, Rammouni M, Baran J, Khatib R. Herpes simplex virus esophagitis in the immunocompetent host: an overview. Am J Gastroenterol. 2000;95:2171–2176. doi: 10.1111/j.1572-0241.2000.02299.x. [DOI] [PubMed] [Google Scholar]
- 4.Galbraith JC, Shafran SD. Herpes simplex esophagitis in the immunocompetent patient: report of four cases and review. Clin Infect Dis. 1992;14:894–901. doi: 10.1093/clinids/14.4.894. [DOI] [PubMed] [Google Scholar]
- 5.Solammadevi SV, Patwardhan R. Herpes esophagitis. Am J Gastroenterol. 1982;77:48–50. [PubMed] [Google Scholar]
- 6.McDonald GB, Sharma P, Hackman RC, Meyers JD, Thomas ED. Esophageal infections in immunosuppressed patients after marrow transplantation. Gastroenterology. 1985;88:1111–1117. doi: 10.1016/s0016-5085(85)80068-8. [DOI] [PubMed] [Google Scholar]
- 7.Klotz DA, Silverman L. Herpes virus esophagitis, consistent with herpes simplex, visualized endoscopically. Gastrointest Endosc. 1974;21:71–73. doi: 10.1016/s0016-5107(74)73797-x. [DOI] [PubMed] [Google Scholar]
- 8.Slomka MJ, Emery L, Munday PE, Moulsdale M, Brown DW. A comparison of PCR with virus isolation and direct antigen detection for diagnosis and typing of genital herpes. J Med Virol. 1998;55:177–183. [PubMed] [Google Scholar]
- 9.Nahass GT, Goldstein BA, Zhu WY, Serfling U, Penneys NS, Leonardi CL. Comparison of Tzanck smear, viral culture, and DNA diagnostic methods in detection of herpes simplex and varicella-zoster infection. JAMA. 1992;268:2541–2544. [PubMed] [Google Scholar]
- 10.Coyle PV, Desai A, Wyatt D, McCaughey C, O'Neill HJ. A comparison of virus isolation, indirect immunofluorescence and nested multiplex polymerase chain reaction for the diagnosis of primary and recurrent herpes simplex type 1 and type 2 infections. J Virol Methods. 1999;83:75–82. doi: 10.1016/s0166-0934(99)00108-1. [DOI] [PubMed] [Google Scholar]
- 11.Weidmann M, Meyer-König U, Hufert FT. Rapid detection of herpes simplex virus and varicella-zoster virus infections by real-time PCR. J Clin Microbiol. 2003;41:1565–1568. doi: 10.1128/JCM.41.4.1565-1568.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Burrows J, Nitsche A, Bayly B, Walker E, Higgins G, Kok T. Detection and subtyping of Herpes simplex virus in clinical samples by LightCycler PCR, enzyme immunoassay and cell culture. BMC Microbiol. 2002;2:12. doi: 10.1186/1471-2180-2-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cronstedt JL, Bouchama A, Hainau B, Halim M, Khouqeer F, al Darsouny T. Spontaneous esophageal perforation in herpes simplex esophagitis. Am J Gastroenterol. 1992;87:124–127. [PubMed] [Google Scholar]
- 14.Chusid MJ, Oechler HW, Werlin SL. Herpetic esophagitis in an immunocompetent boy. Wis Med J. 1992;91:71–72. [PubMed] [Google Scholar]
- 15.Kurahara K, Aoyagi K, Nakamura S, Kuwano Y, Yamamoto C, Iida M, Fujishima M. Treatment of herpes simplex esophagitis in an immunocompetent patient with intravenous acyclovir: a case report and review of the literature. Am J Gastroenterol. 1998;93:2239–2240. doi: 10.1111/j.1572-0241.1998.00623.x. [DOI] [PubMed] [Google Scholar]