

Abstract
Background
The purpose of this study was to enumerate the annual morbidity and mortality incidence and estimate the direct and indirect costs associated with occupational injuries and illnesses in Bangkok in 2008. In this study, data on workmen compensation claims and costs from the Thai Workmen Compensation Fund, Social Security Office of Ministry of Labor, were aggregated and analyzed.
Methods
To assess costs, this study focuses on direct costs associated with the payment of workmen compensation claims for medical care and health services.
Results
A total of 52,074 nonfatal cases of occupational injury were reported, with an overall incidence rate of 16.9 per 1,000. The incidence rate for male workers was four times higher than that for female workers. Out of a total direct cost of $13.87 million, $9.88 million were for medical services and related expenses and $3.98 million for compensable reimbursement. The estimated amount of noncompensated lost earnings was an additional $2.66 million.
Conclusion
Occupational injuries and illnesses contributed to the total cost; it has been estimated that workers' compensation covers less than one-half to one-tenth of this cost.
Keywords: costs, occupational injury, workplace injury
1. Introduction
The global burden of occupational injuries and illnesses is substantial, particularly in developing countries. Rates of occupational injury fatalities, for example, are estimated to be at least two to five times higher in the developing regions of the world, compared to North America and Western Europe [1]. The associated medical and disability costs are also considerable. In the USA, the total costs associated with occupational injury and illness in 1992 were estimated to be $171 billion, including directly accountable costs of $65 billion and a larger component of indirect costs ($106 billion) [2–4]. According to Workers' Compensation: Benefits, Coverage, and Costs in 2008, the total medical expense was $29.1 billion and total cash benefit $28.6 billion [5]. Estimated costs have been less well characterized in developing countries, because there are usually no large, centralized record systems that include health conditions having an occupational cause. Record systems in Thailand, however, allow opportunities to assess the scope of occupational morbidity, mortality, and associated costs for a large sector of the population.
In the past 4 decades, the economy in Thailand has changed from a mainly agriculture base to a broader array of manufacturing and services sectors that now account for about 80% of the country's annual expansion of GDP [6]. In 2007, the total workforce in Thailand was estimated to be 35.7 million people (∼56% of the total population). The major employment sectors in the workforce included agriculture (47%), manufacturing (18%), and industrial service (21%). However, only 9.1 million (∼25%) of the total workforce was employed in the formal sector that was covered by the Thai Workmen Compensation Fund (WCF) [7].
In 1996, more than half of the 12,325 firms, inspected by Thailand's Ministry of Labor and Social Welfare, were found to have violated Thai occupational and safety regulations (n = 7,015; 57%) [8]. In 1996, 246,616 cases of occupational injuries in the formal sector were insured by the WCF, at a rate of 40 per 1,000 workers. However, the rate of occupational injuries has declined since then, with a rate of 21 per 1,000 workers being reported in 2008. The rate of permanent or temporal disability (>3 days) was 6 per 1,000 workers [9].
The Thai WCF was set up according to the Workmen's Compensation Act (1994). According to the WCF, the purpose of compensation costs is to replace the employer's liability when employees are injured, sick, or disabled or when they die from work-related injuries and illnesses from employment-based claims based on risks and types of industrial classifications [9]. This funding covers all establishments with at least one employee after 2002. It is the employer's sole liability to contribute an insurance premium to the WCF each year. Employees are eligible to claim compensation benefits, consisting of medical services, monthly indemnities, rehabilitation, or funeral grants, for work-related illnesses or injuries [9]. The employer contribution rate varies from 0.2% to 1.0% of employee wages, based on the risk rating for the type of establishment classified by the Thailand Standard Industrial Classification (TSIC) [10]. No published studies have estimated the costs of occupational injuries and illnesses in Thailand. The main purpose of this study was to estimate the annual incidence of morbidity and mortality, and calculate the direct costs and forgone (uncompensated) earnings associated with occupational injuries and illnesses in Bangkok in 2008. To achieve these aims, researchers examined the actual compensation claims of workmen and claim related reimbursements by the WCF, Social Security Office of the Ministry of Labor. These workplace injury costs are useful for a number of reasons. They provide a compact, comprehensive, and stable measure for describing a diverse range of injuries and illnesses. They also allow us to better understand differences between incidence rates and costs of occupational morbidity and mortality, and provide a baseline for future comparisons.
2. Materials and methods
Data were collected for the 11 social security offices (SSOs) covering 50 districts of Bangkok, Thailand, which consisted of all occupational injuries, illnesses, and fatalities, along with the costs associated with direct payment of medical and related claims by the WCF, Social Security Office of the Ministry of Labor, for the year 2008. This study mainly focused on the direct costs associated with occupational claims, in cases of both morbidity and mortality, in terms of medical expenses, rehabilitation costs, funeral compensation costs, and work compensation costs for lost earnings. In addition, the researchers estimated indirect costs of forgone earnings. All costs in Thai Baht (THB) were converted into US dollar values (US $) ($1 = 31 THB, as of 2013).
2.1. Incidence data management and costing data
The TSIC divides occupations into 140 subgroups. However, this study used only nine major main occupational groups: legislators and managers, professionals, technicians, clerks, service workers, agricultural workers, craftsmen, plant and machine operators, and elementary workers. Similarly, the major industrial types were classified into 15 groups based on an aggregation of 243 subgroups used in the TSIC.
Direct medical costing data related to payment information included health service utilization and costs, including hospital inpatient and outpatient costs, transportation and ambulance, drugs and laboratory tests, medical equipment and disposable supplies, rehabilitation services, and physicians' and nurses' salaries. In addition, compensable costs for rehabilitation, monthly disability allowances, and funeral costs were included (Table 1).
Table 1.
Costs associated with occupational injuries and illnesses, according to Thai Labor Act Number 18 (1–4) and Number 19 [8]
| Cost category | Component | Description |
|---|---|---|
| Direct | ||
| Medical and emergency services | Medical cost | Hospital inpatient/outpatient |
| Transport/ambulance | ||
| Physicians, nurses, etc. | ||
| Drugs/laboratory tests | ||
| Counseling | ||
| Rehabilitation cost | ||
| Nonmedical | Work compensation cost | Types I–IV∗ |
| Funeral cost | ||
| Indirect | ||
| Forgone earning loss† | Work compensation cost | Types I–IV |
Type I: paid 60% monthly allowance for temporary disability >3 days (paid for a maximum of 1 year); type II: paid 60% monthly allowance for permanent partial disability (paid for a maximum of 10 years); type III: paid 60% monthly allowance for permanent total disability (paid for a maximum of 15 years); and type IV: paid 60% monthly allowance for death (paid for a maximum of 8 years).
Estimated costs according to different types of work compensation costs (type I–IV).
The estimated costs for wage compensation were calculated using the national salary base for each subgroup of minimum wage (male = 7,854 THB and female = 7,338 THB). It should be noted that this study did not take into account costs related to foster care, administrative, and legal services for estimating the total direct costs. In addition, this study did not take into consideration all indirect costs, for instance, costs associated with loss of investment, life insurance, macroeconomics, and health-related decline in quality of life.
In this study, the researchers estimated indirect costs only for forgone earnings losses, based on the average of compensation reimbursements for fatalities and injuries according to Thai Labor Act Number 18 (types 1–4) and Number 19, by measuring the value of time lost due to absence from work or reduced productivity. Indirect costs have been calculated based on each type of compensation claims, including temporary disability >3 days, permanent partial disability, permanent total disability, and death. For each type of claim (defined below), the injured worker receives 60% of the monthly allowance, for the allowed coverage duration. The indirect cost of forgone wages was estimated to be approximately two-thirds of wage compensation (i.e., the uncompensated 40% of monthly allowance).
2.2. Definitions
Workers included in the data set are defined as insured persons under article 33 of the Thai Labor Act who pay premium insurance, which provides entitlement to benefits under the Social Security Act B.E. 2533 that was amended by the Social Security Act.
Under article 39, an insured person is one who has been an insured person under article 33 and whose insurance has subsequently ceased [article 38(2)] and s/he notifies the area SSO for his/her intention to continue to be an insured person.
Compensable forgone earning losses based on Thai Labor Act Number 18 (1–4) and Number 19 are classified into four types (when an employee suffers from injuries or sickness or disappears, the employer shall pay monthly indemnity to the employee or the person entitled to compensation under Article 20): type I, 60% of the monthly wages in case the employee is unable to work for more than 3 consecutive days, irrespective of whether the employee has lost an organ or not—the payment should be made from the 1st day until the employee is unable to work, but not exceeding 1 year; type II, 60% of the monthly wages in case the employee has lost certain organs of the body—the payment should be made according to the category of the organs lost and for the period as specified by the Announcement of the Ministry of Labor and Social Welfare, but not exceeding 10 years; type III, 60% of the monthly wages where the employee suffers from disablement—the payment should be according to the type of disablement and for the period as specified by the Announcement of the Ministry of Labor and Social Welfare, but not exceeding 15 years; type IV, 60% of the monthly wages in case of the death of employee or disappearance—payment for a period of 8 years. In case of suffering from injuries or sickness, causing loss of organs or the working capability of certain part of an organ, the indemnity should be calculated on the basis of the percentage of the period specified for loss of organs or working capability of those organs, as specified by the Announcement of the Ministry of Labor and Social Welfare. However, this Compensation Act is not applicable to employees or government officials of the central, provincial, and local administrations; employees of nonprofit organizations; and employees of state enterprises [9].
3. Results
In Bangkok's database of the workmen compensation claims during the year 2008, there were 130,969 insured firms (129,988 employers) and 3,083,023 active, covered employees, which accounted for 40% of firms (n = 323,526) and 36% of insured employees (n = 8,135,606) in the whole country (Table 2). In Bangkok, 50 districts are classified into 11 SSOs. The majority of the labor workforce was between 20 years and 40 years of age (72%; n = 2,227,866), with a ratio of male to female employees of 1.002:1. Insured workers aged <25 years accounted for almost 18% of the labor workforce.
Table 2.
Description of insured persons of Bangkok province and their percentages, 2008
| Descriptive characteristics | Number | % |
|---|---|---|
| Gender | ||
| Male | 1,543,761 | 50.07 |
| Female | 1,539,261 | 49.93 |
| Age (y) | ||
| 15–19 | 99,074 | 3.21 |
| 20–24 | 447,849 | 14.53 |
| 25–29 | 726,933 | 23.58 |
| 30–34 | 597,524 | 19.38 |
| 35–39 | 455,560 | 14.78 |
| 40–44 | 338,705 | 10.99 |
| 45–49 | 218,489 | 7.09 |
| 50–54 | 121,901 | 3.95 |
| 55–59 | 57,189 | 1.85 |
| >60 | 19,800 | 0.64 |
| Total | 3,083,023 | 100.00 |
Rates of occupational accidents and injuries were found to be highest in SSO area number 7, with 39 cases per 1,000. The area with the second highest rate was SSO area number 10, with 25 cases per 1,000. These areas were located in the outskirts of Bangkok and included major intensive labor industries such as construction, automobile and transportation equipment, and metal product industries (Fig. 1).
Fig. 1.
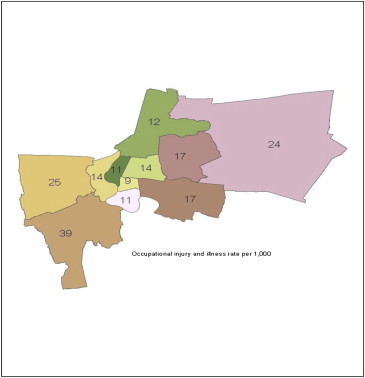
Occupational injury and illness rate (per 1,000) in various Social Security Office areas, 2008.
A total of 52,074 nonfatal cases of occupational injury or illness were reported in Bangkok during 2008, with an overall incidence rate of 16.9 cases per 1,000 insured workers (Table 3). The overall incidence rate for male workers was nearly four times higher than that for female workers. The overall incidence rate decreased with age, and ranged from 30.4 per 1,000 among teen workers to 12.4–13.7 per 1,000 among workers aged 55 years or older. After excluding milder cases that had no permanent disability and no more than 3 days of work loss, the incidence rate of moderate and severe cases was relatively uniform across most age groups (age ≥20 years, rate 4.2 per 1,000) but was more than twice as high among teen workers (8.4 per 1,000). Considering cases of any severity, the incidence rates were relatively low among professional workers, managers, and legislators (≤1 per 1,000); moderate among technicians, clerks, and agricultural workers (4–5 per 1,000); relatively high among service workers, elementary workers, and craftsmen (21–29 per 1,000); and highest among plant and machine operators (40 per 1,000). The proportion of moderate and more severe cases was higher among technicians and clerks (36% of cases) than among all other occupational groups (23–29%); however, as noted, their overall incidence was still relatively moderate.
Table 3.
Numbers and incidence rates of nonfatal occupational injuries and illnesses in Bangkok, 2008
| Severity∗ |
Rate (per 1,000 workers) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Number of cases | Lost work (no permanent disability) |
Permanent disability |
Lost work >3 d or disability(% of cases) | All cases | Lost work >3 d or disability | ||
| 0–3 d | >3 d (type I) | Partial (type II) | Total (type III) | |||||
| All cases | 52,074 | 38,773 | 12,197 | 1,092 | 12 | 26 | 16.9 | 4.3 |
| Sex | ||||||||
| Male | 41,270 | 30,740 | 9,703 | 815 | 12 | 26 | 26.7 | 6.8 |
| Female | 10,804 | 8,033 | 2,494 | 277 | 0 | 26 | 7.0 | 1.8 |
| Age (y) | ||||||||
| 15–19 | 3,015 | 2,179 | 747 | 87 | 2 | 28 | 30.4 | 8.4 |
| 20–24 | 9,005 | 6,929 | 1,934 | 142 | 0 | 23 | 20.1 | 4.6 |
| 25–29 | 11,589 | 8,840 | 2,552 | 193 | 4 | 24 | 15.9 | 3.8 |
| 30–34 | 9,884 | 7,493 | 2,208 | 182 | 1 | 24 | 16.5 | 4.0 |
| 35–39 | 7,443 | 5,540 | 1,717 | 183 | 3 | 26 | 16.3 | 4.2 |
| 40–44 | 5,061 | 3,635 | 1,304 | 122 | 0 | 28 | 14.9 | 4.2 |
| 45–49 | 3,122 | 2,115 | 924 | 82 | 1 | 32 | 14.3 | 4.6 |
| 50–54 | 1,973 | 1,394 | 513 | 65 | 1 | 29 | 16.2 | 4.7 |
| 55–59 | 710 | 463 | 221 | 26 | 0 | 35 | 12.4 | 4.3 |
| >60 | 272 | 185 | 77 | 10 | 0 | 32 | 13.7 | 4.4 |
| Occupational group | ||||||||
| Legislators and managers | 216 | 156 | 56 | 4 | 0 | 28 | 0.9 | 0.3 |
| Professionals | 132 | 94 | 38 | 0 | 0 | 29 | 0.3 | 0.1 |
| Technicians | 1,963 | 1,257 | 670 | 36 | 0 | 36 | 4.5 | 1.6 |
| Clerks | 1,726 | 1,109 | 580 | 36 | 1 | 36 | 4.6 | 1.6 |
| Agricultural workers | 57 | 44 | 12 | 1 | 0 | 23 | 3.7 | 0.8 |
| Service workers | 8,301 | 6,245 | 1,984 | 69 | 3 | 25 | 21.2 | 5.3 |
| Elementary workers | 9,888 | 7,361 | 2,387 | 137 | 3 | 26 | 26.7 | 6.8 |
| Craftsmen | 13,068 | 9,952 | 2,874 | 241 | 1 | 24 | 28.8 | 6.9 |
| Plant and machine operators | 16,723 | 12,555 | 3,596 | 568 | 4 | 25 | 40.2 | 10.0 |
| Size of establishment† | ||||||||
| Small | 35,258 | 25,586 | 8,790 | 877 | 5 | 27 | 17.0 | 4.7 |
| Medium | 6,033 | 4,773 | 1,168 | 90 | 2 | 21 | 15.4 | 3.2 |
| Large | 10,783 | 8,414 | 2,239 | 125 | 5 | 22 | 17.5 | 3.8 |
Costs associated with occupational injuries and illnesses according to Thai Labor Act Number 18 (1–4) and Number 19.
Small: number of employees <200; medium: number of employees 200–500; and large: number of employees >500.
Of a total direct cost of $13.87 million in 1 year (2008), $9.88 million were for medical services and related expenses such as drugs and X-ray, and $3.98 million for compensable reimbursement under Labor Act article 33 and article 39. Rehabilitation expenses were much lower—$5,893 (Table 4). The estimated amount of noncompensated (forgone) lost earnings was an additional $2.66 million, amounting to a total accountable direct and indirect cost of $16.53 million. Median and mean statistics revealed different patterns, suggesting the presence of differences at the higher-cost end of cost distributions. For example, median overall costs per case were comparable for male and female workers, but the mean costs of medical care and wage compensation were 1.3–1.5 times higher for male workers. In general, costs per case increased with age, primarily reflecting the cost of wage compensation. The costs of medical care were highest in the 40–54-year-old age group and lower for younger and older age groups.
Table 4.
Accountable costs of nonfatal occupational injuries and illnesses in Bangkok, 2008 (US $)
| Characteristics | Direct costs |
Uncompensated lost earnings (estimated) | Grand total | Average costs (per case) |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Medical expense | Rehabilitation expense | Compensation for lost earnings | Total (direct) | Median and interquartile interval∗ | Mean medical expense | Mean compensation for lost earnings† | ||||
| All cases | 9,883,896 | 5,839 | 3,984,862 | 13,874,597 | 2,656,575 | 16,531,172 | 57 | [10–104] | 190 | 300 |
| Sex | ||||||||||
| Male | 8,445,061 | 4,625 | 3,324,994 | 11,774,744 | 2,216,663 | 13,991,407 | 58 | [11–106] | 205 | 316 |
| Female | 1,438,693 | 1,227 | 659,790 | 2,099,649 | 439,860 | 2,539,509 | 52 | [7–97] | 133 | 238 |
| Age (y) | ||||||||||
| 15–19 | 595,011 | 0 | 253,169 | 848,180 | 168,779 | 1,016,959 | 56 | [8–104] | 197 | 303 |
| 20–24 | 1,473,302 | 498 | 422,208 | 1,896,003 | 281,472 | 2,177,475 | 55 | [12–98] | 164 | 203 |
| 25–29 | 1,425,746 | 690 | 695,280 | 2,121,714 | 463,520 | 2,585,234 | 54 | [11–97] | 123 | 253 |
| 30–34 | 1,719,679 | 1,364 | 631,220 | 2,352,293 | 420,813 | 2,773,106 | 56 | [12–100] | 174 | 264 |
| 35–39 | 1,264,258 | 1,506 | 704,587 | 1,970,385 | 469,725 | 2,440,110 | 56 | [11–101] | 170 | 370 |
| 40–44 | 1,741,245 | 0 | 426,179 | 2,167,424 | 284,119 | 2,451,543 | 60 | [6–114] | 344 | 299 |
| 45–49 | 880,273 | 943 | 438,541 | 1,319,701 | 292,361 | 1,612,062 | 65 | [7–123] | 282 | 435 |
| 50–54 | 580,223 | 340 | 251,928 | 832,507 | 167,952 | 1,000,459 | 77 | [0–188] | 294 | 435 |
| 55–59 | 146,426 | 513 | 119,096 | 266,002 | 79,397 | 345,399 | 73 | [4–142] | 206 | 482 |
| >60 | 57,586 | 0 | 42,654 | 100,240 | 28,436 | 128,676 | 114 | [57–171] | 212 | 490 |
| Occupational group | ||||||||||
| Legislators and managers | 344,863 | 0 | 41,994 | 386,857 | 27,996 | 414,853 | 95 | [0–450] | 1,597 | 700 |
| Professionals | 14,246 | 0 | 8,818 | 23,064 | 5,879 | 28,943 | 49 | [3–96] | 108 | 232 |
| Technicians | 408,218 | 527 | 210,366 | 619,111 | 140,244 | 759,355 | 62 | [9–115] | 208 | 298 |
| Clerks | 1,348,347 | 352 | 236,891 | 1,585,590 | 157,927 | 1,743,517 | 69 | [0–155] | 781 | 384 |
| Agricultural workers | 31,262 | 0 | 5,325 | 36,588 | 3,550 | 40,138 | 76 | [0–156] | 548 | 410 |
| Service workers | 1,291,849 | 621 | 453,562 | 1,746,032 | 302,375 | 2,048,407 | 56 | [11–102] | 156 | 221 |
| Elementary workers | 1,450,297 | 1,708 | 675,201 | 2,127,205 | 450,134 | 2,577,339 | 53 | [10–96] | 147 | 267 |
| Craftsmen | 1,963,489 | 1,092 | 726,643 | 2,691,224 | 484,429 | 3,175,653 | 55 | [12–98] | 150 | 233 |
| Plant and machine operators | 3,025,133 | 1,551 | 1,632,010 | 4,658,693 | 1,088,007 | 5,746,700 | 59 | [5–113] | 181 | 392 |
| Size of establishment‡ | ||||||||||
| Small | 5,930,338 | 3,503 | 2,390,917 | 8,324,758 | 1,593,945 | 9,918,703 | 59 | [10–104] | 168 | 247 |
| Medium | 1,482,584 | 876 | 597,729 | 2,081,190 | 398,486 | 2,479,676 | 53 | [21–87] | 246 | 474 |
| Large | 2,470,974 | 1,460 | 996,216 | 3,468,649 | 664,144 | 4,132,793 | 56 | [22–97] | 229 | 421 |
Interquartile range = 25th and 75th percentiles.
Mean cost, but considering only the potentially compensable cases with disability or >3 days' work loss.
Small: number of employees <200; medium: number of employees 200–500; and large: number of employees >500.
The costs per case revealed surprising patterns across the occupational groups (Table 4). The highest costs were observed in the legislator and manager group, which paradoxically had a relatively low incidence rate of injury or illness. Their costs of medical care were more than seven times higher than the mean cost, and compensation costs were more than twice as high. The next highest medical costs were seen among service workers and the relatively small group of agricultural workers, at two to four times the mean cost. The mean costs of medical care and compensation in other high-incidence occupations were closer to the overall means.
A total of 186 fatal occupational injuries and illnesses were reported, at a rate of 6 per 100,000. The total cost for reimbursed compensation was approximately $3 million, with an average cost of $15,729 per case. Compensable costs reimbursed to male workers were higher than those were reimbursed to female workers. The total costs of fatality were highest in the age group of 35–39 years, whereas these costs for above 40-year-olds were less than those for 20–24-year-olds. The occupational group at a high risk of fatality consisted of labor workers. However, the highest reimbursed compensation costs were for legislators and managers, which averaged $29,922 per case (Table 5). Compensable reimbursement costs due to occupational fatality were $2.8 million on average and accounted for $15,131 per case. However, on average, the estimated costs were higher for male than for female workers ($17,029 vs. $15,909; Table 5).
Table 5.
Numbers, incidence rates, and costs of fatal occupational injuries and illnesses in Bangkok, 2008 (US $)
| Characteristics | No. of cases∗ | Rate (per 100,000 workers) | Direct costs |
Uncompensated lost earnings (estimated) | Grand total | Average costs (per case) |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Funeral | Compensation for lost earnings | Total (direct) | Median and interquartile intervals | Mean funeral expense | Mean compensation for lost earning | ||||||
| All cases | 186 | 6.0 | 111,217 | 2,814,284 | 2,925,501 | 1,950,334 | 4,875,835 | 13,794 | [399–14,193] | 598 | 15,131 |
| Sex | |||||||||||
| Male | 155 | 10.0 | 104,041 | 2,639,475 | 2,743,516 | 1,829,011 | 4,572,527 | 14,289 | [125–14,414] | 671 | 17,029 |
| Female | 11 | 0.7 | 7,173 | 175,003 | 182,176 | 121,451 | 303,627 | 11,060 | [1,036–12,096] | 652 | 15,909 |
| Age (y) | |||||||||||
| 15–19 | 9 | 9.1 | 8,458 | 146,925 | 155,383 | 103,589 | 258,972 | 11,087 | [3,649–24,736] | 940 | 16,325 |
| 20–24 | 19 | 4.2 | 16,734 | 373,315 | 390,049 | 260,033 | 650,082 | 12,806 | [0–12,997] | 881 | 19,648 |
| 25–29 | 15 | 2.1 | 13,161 | 276,159 | 289,320 | 192,880 | 482,200 | 11,217 | [378–12,595] | 877 | 18,411 |
| 30–34 | 24 | 4.0 | 18,530 | 475,818 | 494,348 | 329,565 | 823,913 | 11,218 | [7,473–18,691] | 772 | 19,826 |
| 35–39 | 24 | 5.3 | 16,833 | 488,933 | 505,766 | 337,177 | 842,943 | 13,847 | [12,917–26,764] | 701 | 20,372 |
| 40–44 | 42 | 12.4 | 13,705 | 343,123 | 356,828 | 237,885 | 594,713 | 18,033 | [0–19,681] | 326 | 8,170 |
| 45–49 | 16 | 7.3 | 10,054 | 297,769 | 307,823 | 205,215 | 513,038 | 14,272 | [7,657–21,929] | 628 | 18,611 |
| 50–54 | 12 | 9.8 | 9,615 | 303,252 | 312,867 | 208,578 | 521,445 | 15,354 | 11,152–32,506 | 801 | 25,271 |
| 55–59 | 3 | 5.2 | 2,958 | 77,107 | 80,065 | 53,377 | 133,442 | 13,794 | [9,370–23,164] | 986 | 25,702 |
| >60 | 2 | 10.1 | 1,167 | 20,317 | 21,484 | 14,323 | 35,807 | 10,742 | [0–11,371] | 584 | 10,159 |
| Occupational group | |||||||||||
| Legislator and managers | 7 | 2.9 | 4,143 | 209,455 | 213,598 | 142,399 | 355,997 | 35,479 | [0–37,739] | 592 | 29,922 |
| Professionals | 0 | 0.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Technicians | 9 | 2.0 | 6,558 | 217,204 | 223,762 | 149,175 | 372,937 | 18,042 | [9,655–27,967] | 729 | 24,134 |
| Clerks | 41 | 10.9 | 14,365 | 310,827 | 325,192 | 216,795 | 541,987 | 18,033 | [0–19,554] | 350 | 7,581 |
| Agricultural workers | 1 | 6.4 | 588 | 23,564 | 24,152 | 16,101 | 40,253 | 0 | 0 | 588 | 23,564 |
| Service workers | 24 | 6.1 | 18,948 | 475,638 | 494,586 | 329,724 | 824,310 | 421,229 | [0–55,371] | 790 | 19,818 |
| Elementary workers | 29 | 7.8 | 24,463 | 484,060 | 508,523 | 339,015 | 847,538 | 119,923 | [0–128,309] | 844 | 16,692 |
| Craftsmen | 27 | 5.9 | 22,287 | 553,083 | 575,370 | 383,580 | 958,950 | 220,147 | [0–271,601] | 825 | 20,485 |
| Plant and machine operators | 28 | 6.7 | 19,859 | 464,800 | 484,659 | 323,106 | 807,765 | 214,042 | [0–235,378] | 709 | 16,600 |
| Size of establishment † | |||||||||||
| Small | 116 | 116.0 | 66,730 | 1,688,570 | 1,755,301 | 1,170,200 | 2,925,501 | 12,794 | [399–14,193] | 575 | 14,557 |
| Medium | 17 | 17.0 | 16,683 | 422,143 | 438,825 | 292,550 | 731,375 | 12,001 | [856–10,193] | 981 | 24,832 |
| Large | 32 | 32.0 | 27,804 | 703,571 | 731,375 | 487,584 | 1,218,959 | 11,284 | [1,451–15,121] | 869 | 21,987 |
Costs associated with occupational injuries and illnesses according to Thai Labor Act Number 18 (1–4) and Number 19.
Small: number of employees <200; medium: number of employees (200–500); and large, number of employees >500.
The median of cost expenses per case was slightly high in firms with less than 100 employees. Specifically, the highest cost was found to be associated with firms with less than 100 employees (median = $68.72 per case). In general, male workers had higher cost expenses than female workers, except for firms with 20–100 employees (Fig. 2).
Fig. 2.

Median of total medical cost per case by firm size and gender, 2008. F, female; M, male.
Of all the industrial types classified by TSIC, mining and related industries were associated with the highest cost, which were almost twice the compensable costs per case in other industries (median = $120.37). Other industrial types were found to have similar medical expense costs (median = $ 58-66) (Fig. 3).
Fig. 3.
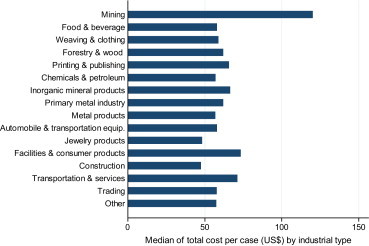
Median of total medical cost per case by industrial types, 2008.
In general, the six leading causes of occupational injuries and illnesses, including injured by cut or wounded by sharp, thrown, or falling objects, foreign material in eyes or eye injuries, falls, and car accidents: Fig. 4) were higher in male workers than in female workers. The highest cause of occupational injuries and illnesses was cut or wounded by sharp objects, at a rate of 6.5 per 1,000 for male workers and 2 per 1,000 for female workers. The body regions that were mostly injured were fingers, on average 6.5 per 1,000 for male and 2.1 per 1,000 for female workers. Other body regions injured were eyes, hands, feet, and multiple body parts. For leading causes and major injured body regions, male workers got injured more than female workers.
Fig. 4.
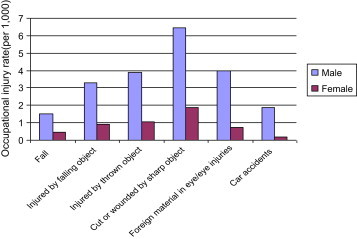
Six leading causes of occupational injuries and illnesses in Bangkok, 2008.
4. Discussion
Findings of this study suggest that occupational injuries and illnesses contribute to the total costs of health care and lost productivity in Bangkok. It is estimated that workers' compensation covers less than one-half to one-tenth of the costs of occupational injuries and illnesses, compared with payments of the SSO for nonoccupational injuries and illnesses ($246 million) [8]. These costs were approximately 18 times less than reimbursement from the SSO ($16.53 million). This study took into consideration only Bangkok SSO areas and, hence; the results could not be interpolated to national level. It should be noted that industrial types and job characteristics of workers in Bangkok may be different from other provinces. It should also be noted that approximately one-third of insured workers under the WCF in the whole country are from Bangkok (3.1 million out of 9.3 million) [9]. The researchers determined the data on occupational claims and compensable costs of insured workers under WCF during the year 2008. This study primarily focused on direct costs and estimated forgone (uncompensated) earnings. To our knowledge, this study represented the first attempt to estimate the costs of occupational injuries and illnesses in Thailand. The researchers did not attempt to estimate direct costs such as administrative and legal costs and indirect costs such as loss of productivity and health-related quality of life (pain/suffering/psychological problems).
Out of the total direct costs of $13.87 million for nonfatal occupational injuries and illnesses, $9.88 million (71%) were for medical care costs and $3.98 million (29%) for compensation for lost earnings. Only $5,839 was reimbursed for rehabilitation expenses (Table 4) which were associated with a few identified cases that were reported for partial and total disability (1,104 cases; 2%; Table 3). Costs of medical care were higher in the 40–54-year-old age group than that in other age groups, whereas compensation costs for lost earnings increased with age, associated with higher salary. In addition, legislators' and managers' claims of compensable medical expenses for occupational injuries and illnesses were higher than those of other occupational groups (median = $95 per case).
These costs were likely to be less than the actual costs because the researchers did not account for administrative and legal costs. In addition, these costs did not include indirect costs associated with pain and sufferings, as well as those associated with home health care provided by family members. In addition, this study did not account for medical costs and related expenses of injured workers who sought medical care and did not claim for occupational injuries and illnesses from the WCF. It is possible that occupational injured cases were under-reported. It was likely that a part of these expense costs was related to occupational injuries and illnesses, but was not claimed and confirmed by occupational physicians. It was also possible that employers did not report their injured workers as occupational and injuries cases to avoid a higher compensation contribution, using experience rate. Therefore, the costs of nonfatal occupational injuries and illnesses were likely to be under-reported and underestimated.
Interestingly, almost 80% of claimed workers were male. This was similar to the findings of a previous study by Thepaksorn et al [7] conducted between 2001 and 2004, using data from the Thai National Injury Surveillance System (85% male workers) and the Washington State Department of Labor and Industries in 2004 (70% male workers) [11]. This might be due to male workers performing high-risk tasks or occupations such as construction, machine operation, and transportation. In addition, the incidence rate was highest in the teenager group—30.4 per 1,000 for all cases and 8.4 per 1,000 for work loss for more than 3 days or disability. It is possible that they had less working skills and experience than other age groups. Similar to other age groups, male teenagers' claims for occupational injuries were four times higher than that of female teenagers (2,445 cases vs. 570 cases). The six leading causes of occupational injuries and illnesses were cut or wounded by sharp objects, injured by thrown objects, injured by falling objects, foreign materials in eyes or eye injuries, car accidents, and falls. The five major body regions that were injured were fingers, eyes, hands, feet, and multiple body parts.
In this study, only 2% (n = 1,233) were confirmed by occupational physicians as cases of occupational diseases and/or illnesses, including noise-induced hearing loss (20 cases), dust exposure (6 cases), infectious disease (1 case), traumatic injuries from lifting/moving (634 cases), traumatic injuries from ergonomic (175 cases), and skin diseases (397 cases). As mentioned above, it was possible that cases of occupational diseases and illnesses remained underdetermined and under-reported when data from occupational clinics were not accessed. In addition, occupational diseases and illnesses are generally required time for developing prognosis of diseases and for completed records. Claims of male workers for occupational diseases and illnesses were higher than those of female workers (221 cases vs. 176 cases).
Similar to nonfatal occupational injury claims, male workers' compensable claims for fatal occupational injuries were much higher than those of female workers (14 times). This rate was similar to fatal occupational injuries in the USA from 1980 to 1997 [12]. Specifically, compensation costs for lost earnings were highest in the 50–59-year-old age group, approximately $25,000 per case, similar to nonfatal occupational injuries and illnesses. In addition, legislators and managers claimed the highest compensations, approximately $30,000 per case, for fatal occupational injuries.
Despite the fact that the incidence rates of occupational injuries were comparable with other studies [11,12], the researchers did not attempt to compare compensable costs due to occupational injuries and illnesses with those studies. There were differences among them in terms of labor costs, inflation rate, cost of living, and medical costs and related expenses. Generally, most previous studies estimated costs using only a number of cases multiplied by estimated costs for occupational injuries and illnesses [2,12–15]. For example, in the USA, the estimated 6,500 fatality and 13.2 million morbidly cases resulted in an estimated cost of $170.9 billion and accounted for 3% of the gross domestic product in 1992. A total of 5,214 fatal work injuries, and 3.7 million nonfatal workplace injuries and illnesses occurred in 2008. However, the frequency of reported nonfatal occupational injuries and illnesses (incidence rates) has declined every year since 1992 [5]. They also suggested that costs associated with occupational injuries and illnesses were large compared with those associated with other diseases [2].
In calculating costs for occupational injuries and illnesses, the researchers relied heavily on the actual compensable cost data of the WCF. In addition, this study determined only the incidence rate and costs of occupational injuries and illnesses in formal workers. It should be noted that the WCF covered only the industries registered under the Labor Act. Self-employed and agricultural workers were not covered. As mentioned above, the researchers suggested that actual occupational injury cases may be more than reported. As a result, compensable claims for nonoccupational cases of the SSO may be inflated. This study relied on data on medical expenses for the year 2008. For direct costs, therefore, the researchers could not capture the medical expenses if insured workers were undergoing medical care and treatment for disability in the following year. However, the incidence rate of occupational injuries and illnesses declined slightly between 2004 and 2009 [9]. Therefore, the estimated costs could be slightly over-estimated. In addition, only a few environmental and occupational clinics or trained occupational physicians were accessible in Bangkok. The quality of workmen's compensation health care services needs to be improved through crucial measures, such as increasing the number of occupational medicine clinics and occupational physicians in each province. The morbidity and fatality rates of occupational injuries in Bangkok may be different from those in other provinces. Bangkok was classified as an urban area, but most areas in other provinces were less urbanized. In addition, the types of industries were also different. A study comparing Bangkok and other provinces may resolve the differences between occupational injury rate and costs of occupational injuries. It would also be valuable to study specific groups related to incidence rate and costs such as teenager's injuries and illnesses and occupational diseases and illnesses.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgments
The authors thank Roongnapa Thongmuang, a social security analyst, for providing data on workmen compensation claims and costs and Pensri Trairat, Director of Research and Development Division, for assisting in acquiring data from the WCF, Social Security Office of Ministry of Labor.
Footnotes
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
- 1.Concha-Barrientos M., Nelson D.I., Driscoll T., Steenland N.K., Punnett L., Fingerhut M.A., Prüss-Üstün A., Leigh J., Tak S.W., Corvalan C. Comparative quantification of health risks: global and regional burden of diseases attributable to selected major risk factors. World Health Organization; Geneva: 2004. Selected occupational risk factors; pp. 1651–1801. [Google Scholar]
- 2.Leigh J.P., Markowitz S.B., Fahs M., Shin C., Landrigan P.J. Occupational injury and illness in the United States: estimates of costs, morbidity, and mortality. Arch Intern Med. 1997;157:1557–1568. [PubMed] [Google Scholar]
- 3.Leigh J.P., Cone J.E., Harrison R. Costs of occupational injuries and illnesses in California. Prev Med. 2001;32:393–406. doi: 10.1006/pmed.2001.0841. [DOI] [PubMed] [Google Scholar]
- 4.Miller T.R., Galbraith M. Estimating the costs of occupational injury in the United States. Accid Anal Prev. 1995;27(6):741–747. doi: 10.1016/0001-4575(95)00022-4. [DOI] [PubMed] [Google Scholar]
- 5.Sengupta I., Reno V., Burton J.F. National Academy of Social Insurance; Washington D.C.: 2010. Workers' compensation: benefits, coverage, and costs, 2008; pp. 33–36. [Google Scholar]
- 6.Office of the National Economic and Social Development Board [Internet] 2010. [cited 2011 May 2]. Available from: http://www.nesdb.go.th. [Google Scholar]
- 7.Thepaksorn P., Daniell W.E., Padungton C., Keifer M. Occupational accidents and injuries in Thailand. Int J Occup Environ Health. 2007;13(3):290–294. doi: 10.1179/oeh.2007.13.3.290. [DOI] [PubMed] [Google Scholar]
- 8.International Labor Organization Asian-Pacific Regional Network on Occupational Safety and Health Information [Internet] 2009. [cited 2011 May 2]. Available from: http://www.ilo.org/public/english/region/asro/bangkok/asiaosh/country/thailand/progact/index.htm. [Google Scholar]
- 9.Office of Workmen's Compensation Fund Social Security Office, Ministry of Labor [Internet] 2008 Mar 1. [cited 2011 May 2]. Available from: http://www.sso.go.th/english/ [Google Scholar]
- 10.Thai Industrial Standards Institute . 2004. Ministry of Industry [Internet] [cited 2011 May 4]. Available from: http://www.tisi.go.th/ [Google Scholar]
- 11.Department of Labor & Industries . 2005. Washington State [Internet] [cited 2011 May 10]. Available from: http://www.lni.wa.gov/ [Google Scholar]
- 12.Biddle E.A. The economic cost of fatal occupational injuries in the United States, 1980–97. Contemp Econ Policy. 2004;22(3):370–381. [Google Scholar]
- 13.Baker L.C., Krueger A.B. Medical costs in workers' compensation insurance. J Health Econ. 1995;14:531–549. doi: 10.1016/0167-6296(95)00020-8. [DOI] [PubMed] [Google Scholar]
- 14.Bernacki E.J., Tsai S.P. Ten years' experience using an integrated workers' compensation management system to control workers' compensation costs. J Occup Environ Med. 2003;45:508–515. doi: 10.1097/01.jom.0000063629.37065.0c. [DOI] [PubMed] [Google Scholar]
- 15.Neumark D., Johnson R.W., Bresnitz E.A., Frumkin H., Hodgson M., Needleman C. Costs of occupational injuries and illness in Pennsylvania. J Occup Med. 1991;33(9):971–976. [PubMed] [Google Scholar]