

Abstract
Background and Objectives:
There is a paucity of information available on acute respiratory infection (ARI) among school children in India. This study was aimed to assess the prevalence and certain risk factors associated with ARI among school children.
Materials and Methods:
This cross-sectional study was conducted among 397 school children age group of 5-14 years in the seven schools of rural Puducherry, India. Data on socio-demographic characteristics and associated risk factors of ARI were collected by interview using pre-tested structured questionnaire. Data was analyzed by univariate and multiple logistic regression analysis.
Results:
Overall, 51.1% (203) of the subjects had at least one symptom of ARI in the preceding 2 weeks. The manifestations of ARI included allergic rhinitis (183, 46.1%), dry cough (75, 18.9%), throat pain and fever (54, 13.6%), wheezing (39, 9.8%) and ear discharge (28, 7.1%). About half of the subjects with ARI (52.2%) belonged to 5-9 year age group and females (52.3%). Mother's education, family history of allergic disorder and asthma, absence of smoke outlet in kitchen and windows in sleeping room were found to be significantly associated with ARI in univariate analysis (P < 0.05). Multiple logistic regression analysis showed that 5-9 years age group (odds ratio [OR] = 1.7), family history of allergic disorder (OR = 9.6) and asthma (OR = 5.2), presence of smoke outlet in kitchen (OR = 0.5), absence of windows in sleeping room (OR = 3.0) were found to have an independent association with the ARI. About 29.6% (60) of the subjects with ARI had accessed health care facility for treatment.
Conclusion:
ARI among school children is an important health problem. Interventions like provision of smoke outlets and windows in sleeping room may help in reduction of burden of ARI.
Keywords: Acute respiratory infection, India, Prevalence, School children
INTRODUCTION
Childhood acute respiratory infection (ARI) is a significant public health problem especially in developing countries. Robust epidemiological data is not available on its incidence in India.[1] As per World Health Organization estimates, ARI causes 3.9 million deaths throughout the world every year.[2] It is one of the important priority area for the concerned stakeholders in health sector especially in developing countries including India.
The occurrence of ARI is determined by the exposure to various risk factors. Air pollution is a risk factor for both acute and chronic respiratory disease.[3] One half of the world's population is exposed to high concentrations of solid fuel smoke that are produced by inefficient open fires, mainly in the rural areas of developing countries. Solid fuel smoke possesses the majority of the toxins found in tobacco smoke and has also been associated with a variety of diseases including ARI in children.[4] Globally, indoor air pollution from solid fuel use is responsible for 1.6 million deaths due to pneumonia, chronic obstructive pulmonary disease and lung cancer.[5] The highest exposures to second-hand smoke are found in Eastern Europe, the Western Pacific and South-East Asia, with more than 50% of some population groups exposed. More than 6 lakh deaths/year world-wide are caused by passive smoking, of which 1.65 lakh are among children.[6] Environmental factors such as overcrowding coupled with poor ventilation at homes and work places may make the health effects of indoor air pollution more pronounced. Exposure is particularly high among women and children, who spend most time near the domestic hearth.[5]
Very few studies have been conducted in India among 5-14 years age group, who will be vulnerable to ARI. Many of the studies were conducted among under-5 year age group children.[7,8] Studies of such nature will be useful to assess the magnitude of ARI and its determinants so that appropriate interventional measures can be taken at the community level. With this background, the study was planned to find out the pattern of respiratory problems and their association with various risk factors among school children of 5-14 years age in rural Puducherry.
MATERIALS AND METHODS
Setting
This cross-sectional study was conducted over a period of 1 year from February 2012 to January 2013 in the seven schools of the four villages attached to a Rural Health Center of Medical Institution in Puducherry. Four villages included viz., Ramanathapuram, Thondamanatham, Thuthipet and Pillayarkuppam.
Sample size estimation and sampling technique
The sample size was estimated to be 400 based on the assumption of prevalence of ARI as 20% and relative precision of 20%. School children of 5-14 years age group in the seven schools formed the study population. Subjects were selected proportional to the total number of children in each class of the selected schools. The students belonged to outside service areas were excluded from the study.
Method of data collection
Prior approval from the Director of Education, Government of Puducherry and headmasters of concerned schools was taken before initiating the study. The students were briefed about the objective of the study and their informed consent was taken for participation. A pre-tested structured questionnaire was used for data collection. The questionnaire was translated into Tamil and then back translated to English by independent experts to look for reliability of the questionnaire.
The children were interviewed by the investigator to find out the presence of any respiratory illness in the preceding 2 weeks of visit. In case of children <10 years, parents were contacted in their houses and the information was sought from them. Data on socio-demographic characteristics and associated risk factors that include family history of allergic disorder and asthma, fuel used for cooking, smoke outlet in the house, windows in living room, hey and pets in the house and smoking among family members in the house were collected. This was be followed by clinical examination of the subject. Children who require further evaluation and/or management were referred to rural health center.
Statistical analysis
The data entry and analysis was performed using Statistical Package for Social Sciences (SPSS) software package version 16. Univariate analysis was used to find out the association of socio-demographic and other risk factors with ARI. Multiple logistic regression analysis was carried out to elucidate the independent effect of confounding variables with ARI. P < 0.05 was taken as statistically significant.
RESULTS
A total of 397 subjects answered the questionnaire with a response rate of 99.3%. Of the 397 students, 199 (50.1%) belonged to 5-9 years age group and 198 (49.9%) belonged to 10-14 years age group. Females are comparatively higher in number (203, 51.1%) than males (194, 48.9%).
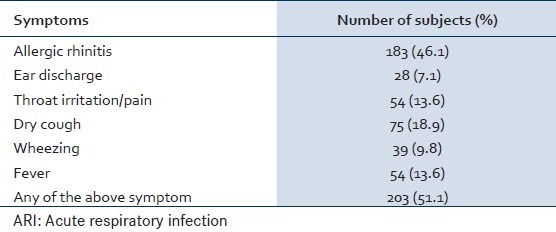
Overall, 51.1% (203) of the subjects had at least one symptom of ARI in the preceding 2 weeks of the interview. Nearly half of them (183, 46.1%) had allergic rhinitis symptoms that include nasal discharge, nasal block and lacrimation. Other symptoms each were present in about 10% of the subjects [Table 1]. About 29.6% (60) of the subjects with ARI had accessed health care facility for treatment.
Table 1.
Manifestations of ARIs among the subjects N = 397
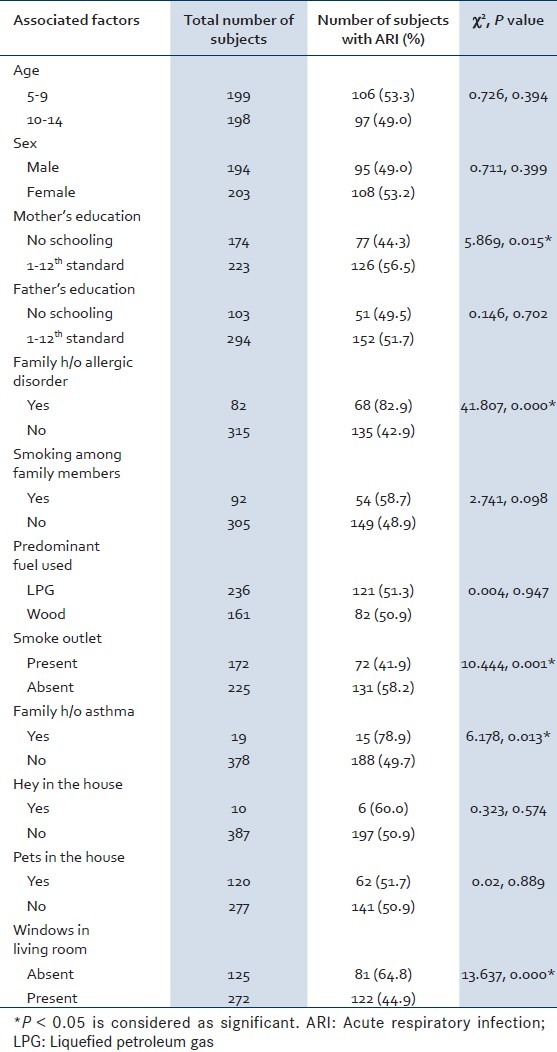
There was no significant association found between age and sex with ARI. However, education of the mother, family history of allergic disorder and asthma, absence of smoke outlet in kitchen and windows in sleeping room were found to be significantly associated with ARI in univariate analysis [Table 2].
Table 2.
Associated factors of ARI
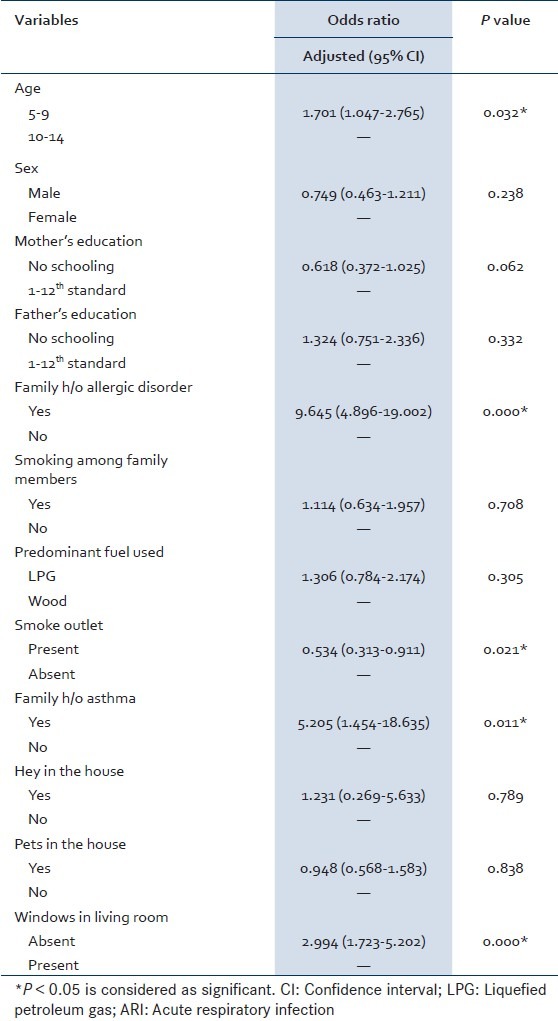
Multiple logistic regression analysis showed that 5-9 years age group (odds ratio [OR] = 1.7), family history of allergic disorder (OR = 9.6), family history of asthma (OR = 5.2), presence of smoke outlet in kitchen (OR = 0.5), absence of windows in sleeping room (OR = 3.0) were found to have an independent association with the ARI [Table 3].
Table 3.
Correlates of ARI: Multiple logistic regression analysis
DISCUSSION
There are few studies to determine the prevalence and risk factors of ARI among school children at global level. However, many studies were reported to assess the prevalence of wheezing among school children in India.[9,10,11,12] Many of the studies were reported to assess the prevalence of ARI among under-five children.[7,8] The fact that high prevalence of ARI and identification of certain important risk factors is a matter of concern. The high prevalence in our study may be due to the inclusion of allergic rhinitis as one of the component in ARI, which were not included in other studies. Furthermore, various factors including the operational definitions and instruments used for the survey, methodology adopted, differential exposure status of risk factors in different locations determines the prevalence of ARI. As majority of the cases of ARI belonged to certain high risk group, the priority should be given to adaptation of those preventive measures. Furthermore, the study findings can be used by the concerned authorities to develop appropriate interventional measures at community level.
A study from South India reported the prevalence of allergic rhinitis among school children as 18.5%.[11] A study in Jaipur city among children aged 5-15 years found that recurrent cough was 16.4% and wheezing was 8.4% in last 12 months period and family history of allergy and asthma was present in 3.1% and 10.9% of the subjects respectively.[13] The prevalence of ARI was similar in both sexes. It was comparatively more among younger age groups similar to another study.[14]
Although our study found that prevalence of ARI is more among those who use firewood, we could not find any association with it. But, prevalence was found significantly more among those who live in houses without smoke outlets and windows in living rooms similar to another study.[14] Studies showed that there was a significant association between the prevalence of wheezing and the presence of smokers in the family.[15] Haryana study in India found that factors associated with presence of symptoms of asthma were passive smoking and pets at home in contrast to our study.[9] This difference may be due to non-quantification of types of pets and smoking behavior among the household members. Family history of allergic disorders and asthma was found to be a risk factor similar to other study.[16] Prevalence of asthma was found to be higher in children having allergy or atopy than in children with no allergy or atopy.[17]
We could not find any association between ARI with some factors probably because of cross-sectional study nature and non-quantification of risk factors. Further analytical studies will explore the role of these factors. The study findings may not be generalized due to different socio-demographic characteristics and associated risk factors in different settings. Furthermore, diagnostic tests could not be conducted due to feasibility constraints.
CONCLUSION
ARI among school children is an important health problem in this area. This study gives valuable information on magnitude of the problem and certain risk factors, which can be utilized for preventive measures to be taken in future. Interventions like provision of smoke outlets and windows in sleeping room may help in reduction of burden of disease at community level.
ACKNOWLEDGMENTS
The present study was supported by Indian Association of Preventive and Social Medicine Epidemiological grant for the year 2011. We thank district educational authorities, headmasters of all the schools, parents and children participated in the study.
Footnotes
Source of Support: The present study was supported by Indian Association of Preventive and Social Medicine (IAPSM) Epidemiological grant for the year 2011.
Conflict of Interest: None declared.
REFERENCES
- 1.Mathew JL, Patwari AK, Gupta P, Shah D, Gera T, Gogia S, et al. Acute respiratory infection and pneumonia in India: A systematic review of literature for advocacy and action: UNICEF-PHFI series on newborn and child health, India. Indian Pediatr. 2011;48:191–218. doi: 10.1007/s13312-011-0051-8. [DOI] [PubMed] [Google Scholar]
- 2.World Health Report on ARI. 2002. [Last accessed on 2013 May 12]. Available from: http://www.who.int/whr/2002/en/index.html .
- 3.World Health Organization. Healthy environments for children. [Last accessed on 2013 May 03]. Available from: http://www.who.int/world-health-day/previous/2003/backgrounder/en/
- 4.Perez-Padilla R, Schilmann A, Riojas-Rodriguez H. Respiratory health effects of indoor air pollution. Int J Tuberc Lung Dis. 2010;14:1079–86. [PubMed] [Google Scholar]
- 5.World Health Organization. WHO Fact Sheets 2005. Geneva: World Health Organisation; 2005. Indoor air pollution and health. [Google Scholar]
- 6.World Health Organization. Worldwide burden of disease from exposure to second-hand smoke. [Last accessed on 2013 May 10]. Available from: http://www.who.int/quantifying_ehimpacts/publications/shsarticle2010/en/
- 7.Islam F, Sarma R, Debroy A, Kar S, Pal R. Profiling acute respiratory tract infections in children from Assam, India. J Glob Infect Dis. 2013;5:8–14. doi: 10.4103/0974-777X.107167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Savitha MR, Nandeeshwara SB, Pradeep Kumar MJ, ul-Haque F, Raju CK. Modifiable risk factors for acute lower respiratory tract infections. Indian J Pediatr. 2007;74:477–82. doi: 10.1007/s12098-007-0081-3. [DOI] [PubMed] [Google Scholar]
- 9.Pokharel PK, Kabra SK, Kapoor SK, Pandey RM. Risk factors associated with bronchial asthma in school going children of rural Haryana. Indian J Pediatr. 2001;68:103–6. doi: 10.1007/BF02722022. [DOI] [PubMed] [Google Scholar]
- 10.Chakravarthy S, Singh RB, Swaminathan S, Venkatesan P. Prevalence of asthma in urban and rural children in Tamil Nadu. Natl Med J India. 2002;15:260–3. [PubMed] [Google Scholar]
- 11.Narayana PP, Prasanna MP, Narahari SR, Guruprasad AM. Prevalence of asthma in school children in rural India. Ann Thorac Med. 2010;5:118–9. doi: 10.4103/1817-1737.62478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Awasthi S, Kalra E, Roy S, Awasthi S. Prevalence and risk factors of asthma and wheeze in school-going children in Lucknow, North India. Indian Pediatr. 2004;41:1205–10. [PubMed] [Google Scholar]
- 13.Narayanappa D, Rajani HS, Mahendrappa KB, Ravikumar VG. Prevalence of asthma in urban school children in Jaipur, Rajasthan. Indian Pediatr. 2012;49:835–6. doi: 10.1007/s13312-012-0188-0. [DOI] [PubMed] [Google Scholar]
- 14.Pal R, Dahal S, Pal S. Prevalence of bronchial asthma in Indian children. Indian J Community Med. 2009;34:310–6. doi: 10.4103/0970-0218.58389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ganesh Kumar S, Premarajan KC, Sarkar S, Sahu SK, Sahana, Ambika, et al. Prevalence and factors associated with asthma among school children in rural Puducherry, India. Curr Pediatr Res. 2012;16:159–63. [Google Scholar]
- 16.Jain A, Vinod Bhat H, Acharya D. Prevalence of bronchial asthma in rural Indian children: A cross sectional study from South India. Indian J Pediatr. 2010;77:31–5. doi: 10.1007/s12098-009-0308-6. [DOI] [PubMed] [Google Scholar]
- 17.Sharma S, Gupta RC, Dixit R, Sharma S, Gupta N. Prevalence of asthma in school children with allergic condition in rural areas of Ajmer, India. Chest. 2008;134:54001. [Google Scholar]