

Abstract
INTRODUCTION
Intestinal malrotation is a rare congenital anomaly, and acute appendicitis associated with intestinal malrotation is extremely rare.
PRESENTATION OF CASE We report a rare case of a 47-year-old Japanese woman diagnosed with barium-related perforated appendicitis associated with intestinal malrotation. We used a transumbilical single-incision laparoscopic approach to resect the appendix, and the procedure was completed successfully without perioperative complications.
DISCUSSION
To our knowledge, single-incision laparoscopic surgery for appendicitis associated with intestinal malrotation has not been reported yet. In cases with mobile cecum such as this one, mobilization from inflammatory adhesion of the surrounding structures is easy.
CONCLUSION
We conclude that transumbilical single-incision laparoscopic appendectomy is a simple and less invasive method for treating appendicitis associated with intestinal malrotation.
Keywords: Single-incision, Laparoscopy, Transumbilical, Appendectomy, Appendicitis, Malrotation
Abbreviations: WBC, white blood cell; CT, computed tomography
1. Introduction
Intestinal malrotation is a rare congenital anomaly, and the classification of this abnormality includes various subtypes based on the stage of midgut rotation.1 However, from a practical viewpoint, we found it useful to apply a simplified categorization, including nonrotation, incomplete rotation, and reverse rotation. Most cases of malrotation are discovered in childhood, and the diagnosis is mostly incidental in adults.2 Further, in cases with indefinite symptoms, it is sometimes difficult to diagnose this pathology correctly.
Acute appendicitis is one of the most common conditions requiring emergency surgery. However, acute appendicitis associated with intestinal malrotation is extremely rare. Some case reports and reviews3 have referred to atypical symptoms such as left lower quadrant pain4 and ileus.5
The treatment for this condition is appendectomy. In recent years, laparoscopic appendectomy has gained popularity, but there are limited reports of single-incision appendectomies. Herein, we report a case of a patient with intestinal malrotation who presented with appendicitis, which we treated by a transumbilical single-incision laparoscopic appendectomy approach.
2. Case report
A 47-year-old woman with a 2-day history of epigastric pain was admitted to a local hospital. She had undergone double-contrast barium examination of her stomach 1 month earlier as a periodic checkup for gastric cancer. She had been using analgesic drugs for the treatment of colitis-like symptoms. Her symptoms did not improve, and she was transferred to the emergency department of our institution. The patient presented pain associated with nausea, low-grade fever (37.6 °C), and several episodes of vomiting. On physical examination, she had pain and defense on deep palpation of the periumbilical and lower abdominal regions. Laboratory tests showed an elevated WBC count (10,100/μL with 90% neutrophils) and a C-reactive protein level of 9.42 mg/dL with normal liver and renal function tests. A plain abdominal radiograph showed a radiopaque area in the center of the lower abdomen (Fig. 1).
Fig. 1.

Radiograph examination. Radiopaque objects in the middle lower abdomen (arrowhead).
Computed tomography (CT) with IV enhancement showed intestinal nonrotation findings, including right-sided small intestines, left-sided colon, and a midline-positioned appendix with barium retention near the cecum (Fig. 2). Nonrotation-type intestinal malrotation with ruptured appendicitis was diagnosed based on these findings. Usually, we performed a conventional three-port technique for standard laparoscopic appendectomy to facilitate the separation of the inflammatory adhesions of the appendix and mobilization of the ileocecal region. The appendix was dissected extracorporeally. However, we selected a single-incisional laparoscopic approach owing to the preoperative diagnosis of intestinal malrotation and because this approach required less ileocecal mobilization. The patient was transferred to the operating room for single-incisional laparoscopic appendectomy. For the single-incision laparoscopic surgery technique, the anesthetized patient was placed in the standard supine, crucifix, reverse-Trendelenburg position, with the surgeon on the patient's right side. A 2-cm vertical transumbilical incision was made, and an E•Z Access device designed exclusively for use with the LAP PROTECTOR™ mini-type (Hakko Co. Ltd., Tokyo, Japan) was used.6 A 10-mm 30° endoscope (Olympus, Tokyo, Japan) was used for intra-abdominal visualization. Another two 5-mm trocars were inserted through the umbilicus. We did not find a Ladd's band or any other GI malformation. After aspiration of dirty ascitic fluid, the appendix was detected behind the uterus. Blunt dissection was performed easily. Subsequently, the appendix was exteriorized and resected extracorporeally. Sufficient peritoneal lavage and drainage catheter insertion were also performed (Fig. 3). We did not perform any surgical intervention, such as Ladd's procedure, to address the malrotation. Pathological examination confirmed the diagnosis of barium appendicitis with perforation (Fig. 4). The patient was discharged 7 days later without any complications.
Fig. 2.

Computed tomography and reconstituted imaging. (a) Radiopaque objects in the deep pelvis (arrowhead). (b) Right-sided small intestines and left-sided colon. (c) Appendix (arrowhead) and cecum (arrow).
Fig. 3.
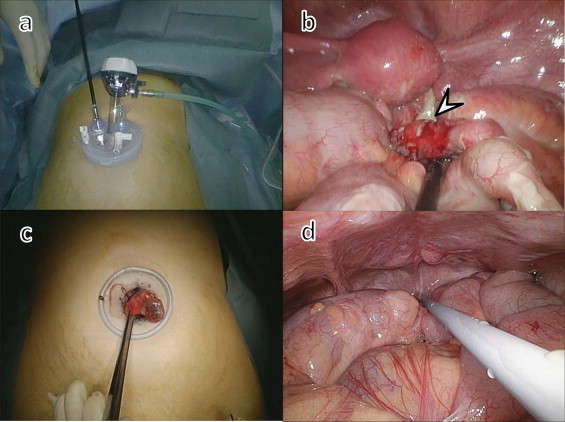
Representative photograph of surgical findings. (a) Laparoscopic settings. (b) Bluntly dissected appendix (arrowhead). (c) Appendix was removed through the transumbilical incision. (d) Sufficient peritoneal lavage.
Fig. 4.
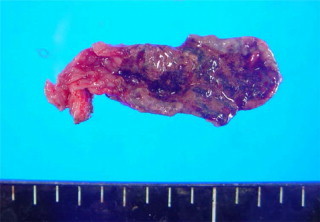
Macroscopic appearance of the resected specimen. Gangrenous appendix with white deposit (barium)
3. Discussion
Malrotation occurs in one of every 500 births, and most cases of malrotation are detected by 1 year of age. Because there are many asymptomatic cases in adults, the true incidence of malrotation is unknown. The most extensive study is attributed to Akbulut et al.3 who reviewed 95 cases of left-sided appendicitis and reported 23 cases of appendicitis associated with intestinal malrotation. Reports of 14 cases of laparoscopic surgery for appendicitis associated with intestinal malrotation are reviewed in Table 1.7–12
Table 1.
Reported cases of laparoscopic surgery for appendicitis associated with intestinal malrotation.
| Year | Author | Age | Gender | Laparoscopic procedure | Diagnostic modality | Ladd procedure | Complication |
|---|---|---|---|---|---|---|---|
| 2001 | Nicholas JM | 27 | M | Exploratory | CT | + | ND |
| 2003 | Tsumura H | 15 | F | ND | CT | + | ND |
| 2007 | Welte FJ | 46 | M | ND | CT | − | − |
| 2007 | Palanivelu C | 8 cases review | multiport | CT | + | − | |
| 2008 | Schwartz JH | 38 | M | ND | CT | − | − |
| 2009 | Bedoui R | 56 | M | multiport | CT | ND | − |
| 2012 | Chabel M | 15 | F | multiport | US/CT | − | − |
CT, computed tomography; US, ultrasonography; ND, not described.
Intestinal malrotation may present with atypical symptoms in cases of associated appendicitis, making the diagnosis very difficult. A scoring system using characteristic physical findings, such as the Alvarado score, does not provide sufficient sensitivity and specificity for the diagnosis. Exploratory laparoscopy has been used as a diagnostic treatment.13 Exploratory laparoscopy is also useful in terms of the transition to surgical treatment. However, CT has been performed in many cases to date. In many cases, preoperative diagnosis was possible by CT.
Appendectomy is the basic operative procedure for treating appendicitis. On the other hand, the Ladd procedure is the standard surgical treatment for intestinal malrotation. The Ladd procedure requires mobilization of the right colon and cecum by division of Ladd bands, and appendectomy is performed as an additional procedure. Our patient had a perforated appendicitis that required emergency treatment; therefore, appendectomy was the precedent procedure. Since our patient was asymptomatic up to adulthood, the recommendations for Ladd procedure are still controversial. Although, the safety of the laparoscopic Ladd procedure has been reported,14–16 the need for the procedure should be determined on a case-by-case basis.
The most significant characteristic of surgery in patients with malrotation is the absence of the appendix in its usual position in the right lower quadrant owing to the mobility of the ileocecal portion. The added difficulty of the surgical approach is attributable to this characteristic. In this case, the approach to the deep pelvis by laparotomy requires a large incision. However, the minimal invasiveness of laparoscopic surgery is advantageous and makes it possible to approach various lesions through a small incision. Furthermore, the appendix can be easily resected extracorporeally if it is identified because of the mobility of the ileocecal region.
In conventional laparoscopic appendectomy, the appendix dissection approach is broadly classified into extracorporeal dissection or intracorporeal dissection. In intracorporeal dissection, an end loop or stapler is used, whereas in extracorporeal dissection and laparotomy, special devices are not required. Alternatively, the mobilization of the ileocecal region is necessary. Single-incision laparoscopic appendectomy has technical limitations associated with the use of a stapler; therefore, mobilization of the ileocecal region and extracorporeal dissection are often performed. Some reports have mentioned that single-incision laparoscopic appendectomy is a useful and cost-effective surgical technique because it requires the use of fewer devices,17 although there are some opposing views.18,19
However, in cases of mobile cecum such as in the present case, the mobilization of the cecum from the surrounding inflammatory adhesions is easy.
4. Conclusion
In summary, we conclude that transumbilical single-incision laparoscopic appendectomy is a simple and less invasive method for treating appendicitis associated with a mobile cecum as typified by intestinal malrotation.
Conflict of interest
The authors declare that they have no conflicts of interest or competing interests.
Ethical approval
Written consent was obtained from the patient for publication of this case report and the accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Funding
None.
Authors’ contributions
TT participated in the treatment of the patient, collected case details, conducted a literature search, and drafted the manuscript. MK and KS helped to draft the manuscript. YH, ST, and KA participated in the treatment of the patient. All authors read and approved the final manuscript.
References
- 1.Kapfer S.A., Rappold J.F. Intestinal malrotation—not just the pediatric surgeon's problem. J Am Coll Surg. 2004;199:628–635. doi: 10.1016/j.jamcollsurg.2004.04.024. [DOI] [PubMed] [Google Scholar]
- 2.Zissin R., Rathaus V., Oscadchy A., Kots E., Gayer G., Shapiro-Feinberg M. Intestinal malrotation as an incidental finding on CT in adults. Abdom Imaging. 1999;24:550–555. doi: 10.1007/s002619900560. [DOI] [PubMed] [Google Scholar]
- 3.Akbulut S., Ulku A., Senol A., Tas M., Yagmur Y. Left-sided appendicitis: review of 95 published cases and a case report. World J Gastroenterol. 2010;16:5598–5602. doi: 10.3748/wjg.v16.i44.5598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Taslakian B., Issa G., Hourani R., Akel S. Left-sided appendicitis in children with congenital gastrointestinal malrotation: a diagnostic pitfall in the emergency department. BMJ Case Rep. 2013 doi: 10.1136/bcr-2013-009474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Welte F.J., Grosso M. Left-sided appendicitis in a patient with congenital gastrointestinal malrotation: a case report. J Med Case Rep. 2007;1:92. doi: 10.1186/1752-1947-1-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shibao K., Takagi T., Higure A., Yamaguchi K. A newly developed oval-shaped port device (E•Z ACCESS Oval Type) for use in reduced port surgery: initial clinical experiences with cholecystectomy. Surg Technol Int. 2013;23:75–79. [PubMed] [Google Scholar]
- 7.Nicholas J.M., Rozycki G.S. Special feature: image of the month. Diagnosis: acute left-sided appendicitis. Arch Surg. 2001;136:705–706. doi: 10.1001/archsurg.136.6.705. [DOI] [PubMed] [Google Scholar]
- 8.Tsumura H., Ichikawa T., Kagawa T., Nishihara M. Successful laparoscopic Ladd's procedure and appendectomy for intestinal malrotation with appendicitis. Surg Endosc. 2003;17:657–658. doi: 10.1007/s00464-002-4516-7. [DOI] [PubMed] [Google Scholar]
- 9.Palanivelu C., Rangarajan M., John S.J., Senthilkumar R., Madhankumar M.V. Laparoscopic appendectomy for appendicitis in uncommon situations: the advantages of a tailored approach. Singap Med J. 2007;48:737–740. [PubMed] [Google Scholar]
- 10.Schwartz J.H., Manco L.G. Left-sided appendicitis. J Am Coll Surg. 2008;206:590. doi: 10.1016/j.jamcollsurg.2007.05.019. [DOI] [PubMed] [Google Scholar]
- 11.Bedoui R., Ali Ouaer M., Nouira R., Dziri C. Acute left-sided appendicitis. Tunis Med. 2009;87:873–874. [PubMed] [Google Scholar]
- 12.Tawk C.M., Zgheib R.R., Mehanna S. Unusual case of acute appendicitis with left upper quadrant abdominal pain. Int J Surg Case Rep. 2012;3:399–401. doi: 10.1016/j.ijscr.2012.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ghritlaharey R.K., Budhwani K.S., Shrivastava D.K. Exploratory laparotomy for acute intestinal conditions in children: a review of 10 years of experience with 334 cases. Afr J Paediatr Surg. 2011;8:62–69. doi: 10.4103/0189-6725.78671. [DOI] [PubMed] [Google Scholar]
- 14.Draus J.M., Jr., Foley D.S., Bond S.J. Laparoscopic Ladd procedure: a minimally invasive approach to malrotation without midgut volvulus. Am Surg. 2007;73:693–696. [PubMed] [Google Scholar]
- 15.Palanivelu C., Rangarajan M., Shetty A.R., Jani K. Intestinal malrotation with midgut volvulus presenting as acute abdomen in children: value of diagnostic and therapeutic laparoscopy. J Laparoendosc Adv Surg Tech A. 2007;17:490–492. doi: 10.1089/lap.2006.0103. [DOI] [PubMed] [Google Scholar]
- 16.Stanfill A.B., Pearl R.H., Kalvakuri K., Wallace L.J., Vegunta R.K. Laparoscopic Ladd's procedure: treatment of choice for midgut malrotation in infants and children. J Laparoendosc Adv Surg Tech A. 2010;20:369–372. doi: 10.1089/lap.2009.0118. [DOI] [PubMed] [Google Scholar]
- 17.Deie K., Uchida H., Kawashima H., Tanaka Y., Masuko T., Takazawa S. Single-incision laparoscopic-assisted appendectomy in children: exteriorization of the appendix is a key component of a simple and cost-effective surgical technique. Pediatr Surg Int. 2013;29:1187–1191. doi: 10.1007/s00383-013-3373-x. [DOI] [PubMed] [Google Scholar]
- 18.Baik S.M., Hong K.S., Kim Y.I. A comparison of transumbilical single-port laparoscopic appendectomy and conventional three-port laparoscopic appendectomy: from the diagnosis to the hospital cost. J Korean Surg Soc. 2013;85:68–74. doi: 10.4174/jkss.2013.85.2.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Galatioto C., Guadagni S., Zocco G., Mazzilo M., Bagnato C., Lippolis P.V. Mesoappendix and appendix stump treatment in laparoscopic appendectomy: a retrospective study in 1084 patients. Ann Ital Chir. 2013;84:269–274. [PubMed] [Google Scholar]