

Abstract
INTRODUCTION
Long term survivors of breast cancer are at risk of developing distant metastasis years after the initial treatment. We report a case of breast adenocarcinoma with colonic polyp metastases, as well as synchronous primary colonic adenocarcinoma and a gastric GIST.
PRESENTATION OF CASE
An 83 year old female underwent colonoscopy for rectal bleeding. This showed a primary colonic adenocarcinoma, a pedunculated polyp in the ascending colon and two polyps in the sigmoid colon. A staging CT scan did not show distant metastasis, but revealed a small gastric GIST which was managed conservatively. A right hemicolectomy showed a T3N0 colonic adenocarcinoma and a polyp contained metastatic adenocarcinoma from a breast primary. The patient had undergone surgery 30 years ago for an invasive lobular carcinoma. Further clinical assessment demonstrated an impalpable grade II Invasive ductal carcinoma in the contralateral breast. She was started on hormonal treatment and at 18 months follow-up, she was well with stable disease.
DISCUSSION
Invasive lobular cancer is the most common histological type of breast cancer that metastasizes to the colon. There is no consensus on the management of breast cancer metastasis to the gastrointestinal tract. Co-existence of a GIST and an adenocarcinoma at two separate locations is uncommon. These are two different cancer entities and it is unclear whether these two are related by as causal relationship.
CONCLUSION
This is a rare case of three distinct tumours; association between them is unlikely. However, the case highlights the importance of a multidisciplinary approach to cancer treatment.
1. Introduction
Breast cancer is one of the most common cancers affecting women and the second leading cause of cancer death.1 About 60% of patients with breast cancer have lymph node or distant metastasis at the time of diagnosis but generally GI metastasis occurs 4–5 year after diagnosis.2 The incidence of extrahepatic gastrointestinal metastasis reported in autopsy studies varies from 6% to 18% with stomach being the most commonly affected organ followed by colon and rectum.3 Breast cancer metastasis to the colon usually presents as a mass lesion but cases with synchronous breast and colon cancer have been reported in the literature.4
Adenocarcinomas and GIST represent distinct oncological entities and there is no association between GIST and tumours of other histological types except in patients with Neurofibromatosis type I, Carneys triad and familial GIST.5 Co-existence of a GIST and an adenocarcinoma at two separate locations in the gastrointestinal tract is extremely uncommon.
We report an interesting case of breast adenocarcinoma with metastasis to a colonic polyp and synchronous colonic adenocarcinoma and a gastric GIST.
2. Case report
An 83 year old female with no significant family history presented to the colorectal clinic with per rectal bleed and underwent a colonoscopy which showed two pedunculated polyps in the sigmoid colon and two large malignant looking “kissing” polyps in the ascending colon (Fig. 1). Both sigmoid colon polyps were excised endoscopically but the ascending colon polyps were not amenable to endoscopic resection. The proximal sigmoid colon polyp showed moderately differentiated adenocarcinoma arising in a tubulovillous adenoma which was completely excised. Sections from the other sigmoid polyp showed poorly differentiated signet ring adenocarcinoma which was positive for CK-7, e-cadherin, weakly positive for oestrogen receptors and negative for CDX2 and CK-20 (Figs. 2 and 3), raising the suspicion of a metastatic adenocarcinoma likely to be upper gastrointestinal in origin.
Fig. 1.
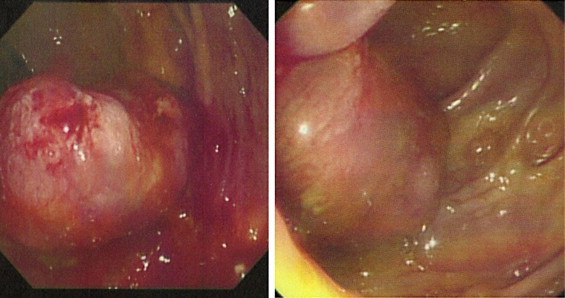
Endoscopic appearance of polyp in ascending colon.
Fig. 2.
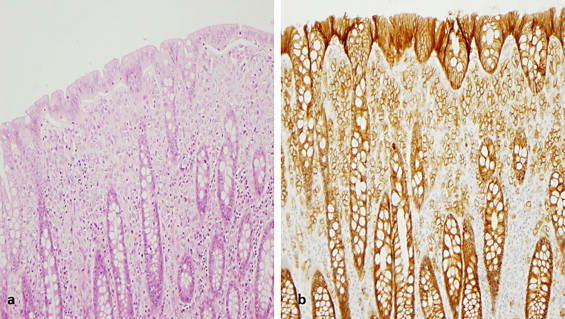
(a) H&E staining showing infiltration of neoplastic cells in the lamina propria. (b) Immunohistochemistry demonstrating weak positivity of neoplastic cells with E-cadherin.
Fig. 3.

Immunohistochemistry demonstrating (a) weak positivity of neoplastic cells in lamina propria with ER and (b) negativity with CDX-2.
A staging CT scan showed thickening in the gastric antrum but there was no evidence of distant metastases. A gastroscopy with an endoscopic ultrasound was undertaken which showed a 3 cm antral lesion, biopsies of which were consistent with a low grade submucosal GIST. The patient was asymptomatic from the GIST and given her age, the multi-disciplinary team decided to manage this conservatively.
She underwent a right hemicolectomy for the ascending colon neoplasms. Histology of the resected hemicolon specimen confirmed a moderately differentiated T3N0 (Dukes B) adenocarcinoma of the colon. In the resected specimen five other polyps were noted, four of which were tubular adenomas; however, one polyp contained metastatic adenocarcinoma of appearances very similar to the sigmoid colon polyp, testing positive for CK7, e-cadherin and oestrogen receptors. In view of the established diagnosis of a gastric GIST with no evidence of an upper GI adenocarcinoma, review of these slides raised the possibility of metastasis from a primary breast tumour. The patient had already undergone a unilateral mastectomy with axillary clearance 30 years ago for an invasive lobular carcinoma. Surveillance imaging demonstrated an impalpable grade II Invasive ductal carcinoma in the contralateral breast which was ER positive and Her-2 negative. Her case was again discussed in the multidisciplinary meeting and she was started on hormonal treatment. At 18 months follow-up, she was well with stable disease in her breast and stomach and there was no evidence of recurrence of the colonic cancer.
3. Discussion
Breast cancer is one of the malignancies that metastasize to the gastrointestinal tract along with melanoma, ovarian and bladder cancer.6 The most frequent sites of GI tract metastasis are stomach and small intestine while colonic involvement is rare. The time interval between primary breast cancer and gastrointestinal involvement may range from synchronous presentation to as long as 30 years but reverse is also true, with the GI manifestation preceding a diagnosis of breast cancer.7–9 Lobular cancer is the most common histological type of breast cancer that metastasizes to the colon; its pattern of spread shows particular affinity to the gastrointestinal system, gynaecological organs and peritoneum. Liver, lung and brain metastasis are more frequent in ductal carcinoma.10
Gastrointestinal metastases from breast cancer are usually associated with extensive spread but our patient had metastases in two colonic polyps only. The endoscopic appearance of colonic metastasis may mimic primary colon cancer but in this case, the distal sigmoid polyp metastasis was pedunculated with a long stalk which is an extremely unusual appearance for intralumenal metastasis. The diagnosis can only be confirmed by histological evaluation which may be complicated by the signet ring appearance of lobular carcinoma but immunohistochemical techniques are helpful in differentiating between primary and secondary lesions. Metastatic breast cancer with intestinal involvement represents evidence of systemic spread but because of its rarity, there is no consensus on the management of such lesions.11 There are reports to suggest a favourable response when systemic treatment alone or in adjunct to surgery is given to patients with breast cancer and gastrointestinal involvement.12
An interesting aspect of our case was synchronous presentation of colon adenocarcinoma and a gastric GIST with the breast cancer. GISTs are commonly found in the stomach but co-existence of GIST and adenocarcinoma at two separate locations in the gastrointestinal tract is uncommon.13 In one study, 20% of patients with GIST were found to have other types of cancer14 but it seems likely that this is was a chance finding rather than a predisposition as the genetic pathways are different for the two tumours. A possible explanation is the metallothioneins which are associated with protection against DNA damage, apoptosis, cell survival and oxidative stress.15 The synchronous presentation of breast cancer is difficult to explain based on metallothioneins as they are down regulated in colorectal cancers but over expressed in breast cancer.16 To our knowledge, there is no evidence to suggest a common factor in tumourogenesis of these pathologically distinct cancers.
4. Conclusion
This is a rare case of three tumours on presentation; the association between them is unknown. Metastatic breast cancer to the colon is a rare entity and clinicians should have a high index of suspicion for metastatic disease in patients who have a history of breast cancer and present with new gastrointestinal lesion. The case described above also highlights the importance of being aware of the particular co-existence of a GIST with other adenocarcinomas and the importance of a multidisciplinary approach to cancer treatment.
Conflict of interest
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Sadaf Jafferbhoy: collected data and drafted part of the manuscript.
Hugh Paterson: helped in writing up and reviewing the manuscript.
Paul Fineron reviewed the manuscript.
References
- 1.Tohfe M., Shami P., Aftimos G., Saade M. Gastrointestinal metastases from breast cancer: a case report. South Med J. 2003;96:624–625. doi: 10.1097/01.SMJ.0000053252.38588.B8. [DOI] [PubMed] [Google Scholar]
- 2.Harris J.R., Morrow M., Norton L. Malignant tumours of the breast. In: DeVita V.T. Jr., Hellman S., Rosenberg S.A., editors. Cancer: principles & practice of oncology. 5th ed. Lippincott-Raven; Philadelphia, PA: 1997. pp. 1457–1616. [Google Scholar]
- 3.Cervi G., Vettoreto N., Vinco A., Cervi E., Vilanacci V., Griolatto P. Rectal localization of metastatic breast cancer-report of a case. Dis Colon Rectum. 2001;44(3):453–455. doi: 10.1007/BF02234749. [DOI] [PubMed] [Google Scholar]
- 4.Higgins L., Robertson I., Khan W., Barry K. Synchronous breast and colon cancer: factors determining treatment strategy. BMJ Case Rep. 2013;(July):10. doi: 10.1136/bcr-2013-009450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gonçalves R1, Linhares E., Albagli R., Valadão M., Vilhena B., Romano S. Occurrence of other tumpurs in atients with GIST. Surg Oncol. 2010;19(4):e140–e143. doi: 10.1016/j.suronc.2010.06.004. [DOI] [PubMed] [Google Scholar]
- 6.Washington K., McDonagh D. Secondary tumours of gastrointestinal tract: surgical pathologic findings and comparison with autopsy series. Mod Pathol. 1995;8:427–433. [PubMed] [Google Scholar]
- 7.Schwarz R.E., Klimstra D.S., Turnbull A.D. Metastatic breast cancer masquerading as gastrointestinal primary. Am J Gastroenterol. 1998;93:111–114. doi: 10.1111/j.1572-0241.1998.111_c.x. [DOI] [PubMed] [Google Scholar]
- 8.Clavien P.A., Laffer U., Torhost J., Harder F. Gastro-intestinal metastases as first clinical manifestation of the dissemination of a breast cancer. Eur J Surg Oncol. 1990;16:121–126. [PubMed] [Google Scholar]
- 9.Benfiguig A., Anciaux M.L., Eugene C.L., Benkemoun G., Etienne J.C. Gastric metastasis of breast cancer occurring after a cancer free interval of 30 years. Ann Gastrenterol Hepatol. 1992;28:175–177. [PubMed] [Google Scholar]
- 10.Borst M.J., Ingold J.A. Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast. Surgery. 1993;114:637–641. [PubMed] [Google Scholar]
- 11.Law W.L., Chu K.W. Scirrhous colonic metastasis from ductal carcinoma of the breast: report of a case. Dis Colon Rectum. 2003;46:1424–1427. doi: 10.1007/s10350-004-6762-3. [DOI] [PubMed] [Google Scholar]
- 12.Yanagisawa K., Yamamoto M., Ueno E., Ohkounchi N. Synchronous rectal metastasis from invasive lobular carcinoma of the breast. J Gastroenterol Hepatol. 2007;22:601–602. doi: 10.1111/j.1440-1746.2006.04671.x. [DOI] [PubMed] [Google Scholar]
- 13.Gopal S.V., Langcake M.E., Johnston E., Salisbury E.L. Synchronous association of small bowel stromal tumour with colonic adenocarcinoma. ANZ J Surg. 2008;78:827–828. doi: 10.1111/j.1445-2197.2008.04669.x. [DOI] [PubMed] [Google Scholar]
- 14.Pandurengan R.K., Dumont A.G., Araujo D.M., Ludwig J.A., Ravi V., Patel S. Survival of patients with multiple primary malignancies: a study of 783 patients with gastrointestinal stromal tumor. Ann Oncol. 2010;21(10):2107–2111. doi: 10.1093/annonc/mdq078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cherian M.G., Jayasurya A., Bay B.H. Metallothioneins in human tumours and potential roles in carcinogenesis. Mutat Res. 2003;533:201–209. doi: 10.1016/j.mrfmmm.2003.07.013. [DOI] [PubMed] [Google Scholar]
- 16.Pedersen M.Ø., Larsen A., Stoltenberg M., Penkowa M. The role of metallothionein in oncogenesis and cancer prognosis. Prog Histochem Cytochem. 2009;44:29–64. doi: 10.1016/j.proghi.2008.10.001. [DOI] [PubMed] [Google Scholar]