

Abstract
BACKGROUND
Acne vulgaris has high prevalence, disturbing quality of life during adolescence.
OBJECTIVES
To measure dissastifaction and acne in 18-year-old male individuals and its associated factors.
METHODS
A questionnaire was applied by trained interviewers to all boys during selection for the military service. Dissatisfaction and acne was evaluated using a self-administered face scale. Facial, prestrernal and dorsal acne were evaluated separately.
RESULTS
A total of 2,200 adolescents, aged 18 years, were interviewed. Among these, 1,678 had acne on the face and 974 (54.05%) showed some degree of dissatisfaction. Regarding the impact of acne located on the chest, 326 out of 686 adolescents (47.52%) reported dissatisfaction. For acne located on the back, 568 out of 1,103 affected individuals (51.50%) showed dissatisfaction. Facial / dorsal acne and dissatisfaction were statistically associated with lower income, lower education levels and with non-whites. Presternal acne and dissatisfaction were statistically asssociated with lower income and lower education levels.
CONCLUSION
This population-based study found a high prevalence of acne on the face, back and chest, with high rates of dissatisfaction.
Keywords: Acne vulgaris, Adolescent psychology, Epidemiology
INTRODUCTION
Acne vulgaris or juvenile acne has a high prevalence among adolescents of both sexes.1 Lesion intensity is variable, disturbing quality of life during adolescence and triggering or worsening emotional problems, mainly because the face, upper neck and trunk are the most commonly affected areas of the body.1-3
Skin diseases such as psoriasis, atopic eczema and acne can interfere substantially with social and occupational functioning and result in impairment of quality of life.4 The social and psychological morbidity that occurs in patients with common conditions of the skin can be ignored or not properly addressed, and thus underestimated by healthcare professionals.4-8
In the literature, only one study exists that covers exclusively the male population, but in this case, the authors have evaluated the most frequent diseases of the skin, and not just acne. This study carried out by Bashir K et al. assessed 114 military men with dermatological diseases and found that depression was frequent among men suffering from illnesses such as urticaria, pruritus, acne vulgaris and psoriasis.4
The impact of acne on psychological parameters and implications for acne treatment are not fully understood. Therefore, this population-based study is justifiably because acne is a highly prevalent disease, with great emotional and social impact.
MATERIAL AND METHODS
Military Service is mandatory for all Brazilian males when they turn eighteen. A questionnaire was applied by trained interviewers to all young men who presented for military service selection in the city of Pelotas. This questionnaire included questions on diet, smoking, skin color, family structure, socio-economic level and specific questions about active acne or scars. Individuals with acne answered questions on how they felt about this condition and its location (face, chest and back). Dissatisfaction with acne was evaluated using a self-administered face scale, characterized by an intervallic, visual five-point scale, composed of stylized faces that consisted of a circle, with eyes that did not change, and a mouth that varied from a line (representing indifference), to a semi-circle facing downward (showing sadness and dissatisfaction) (Figure 1). This evaluation method was chosen because it was easy to understand and use.
FIGURE 1.
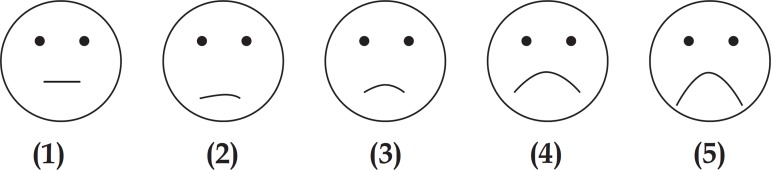
Scale of figures used in the questionnaire, the first demonstrating indifference to the outcome and the other four representing different degrees of dissatisfaction
For the association analysis, samples were divided into "indifferent to the outcome" (when they ticked face 1), and "some degree of dissatisfaction" (those who ticked faces 2, 3, 4 and 5). Schooling was divided into quartiles; the first quartile included those with lower educational levels. The socioeconomic level was divided according to the ABEP (Brazilian Association of Market Research Companies), where E stands for the lower level and A, the upper. Both variables were analyzed with the linear tendency test. Skin color was dichotomized into whites and nonwhites, and the Pearson`s chi square test was used.
Individuals with mental disabilities or who were unable to respond to the questionnaire were excluded.
The statistical analysis was carried out using Stata software. This study was approved by the Research Ethics Committee of the institution. All participants signed an informed consent form.
RESULTS
A total of 2,200 adolescents, aged 18 years, were interviewed. The sample is described in table 1.
TABLE 1.
Sample description
| Variables | N | (%) | |
|---|---|---|---|
| Skin color | |||
| Whites | 1.552 | (70.5) | |
| Non-whites | 648 | (29.5) | |
| Schooling (years of study) | |||
| First quartile (0-7 years) | 687 | (31.2) | |
| Second quartile (8 years) | 449 | (20.4) | |
| Third quartile (9-10 years) | 566 | (25.7) | |
| Forth quartile (11-12 years) | 498 | (22.6) | |
| Socioeconomic Level | |||
| A and B | 997 | (46.0) | |
| C | 1.086 | (50.1) | |
| D and E | 86 | (3.96) | |
Regarding facial acne, 704 (41.95%) were indifferent; for dorsal acne, 535 (48.50%) marked face 1; while 360 (52.48%) showed indifference with respect to presternal acne. Table 2 displays the answers in the 5 different degrees.
TABLE 2.
Number of individuals with different acne subtypes, who marked; face 1 - indifference, faces 2 to 5 - dissatisfaction
| Face 1 (indifference) | Face 2 | Face 3 | Face 4 | Face 5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Facial acne | 704 | (41.95%) | 574 | (34.21%) | 276 | (16.45%) | 77 | (4.59%) | 47 | (2.80%) |
| Dorsal acne | 535 | (48.50%) | 323 | (29.28%) | 162 | (14.69%) | 62 | (5.62%) | 21 | (1.90%) |
| Presternal acne | 360 | (52.48%) | 197 | (28.72%) | 88 | (12.83%) | 22 | (3.21%) | 19 | (2.77%) |
Analyses of associated factors
Facial Acne- when associations were made with the schooling quartiles, in the first quartile, 66.04% were dissatisfied with acne on the face, 60.52% in the second, 53.27% in the third, while in the fourth quartile, the group with the highest schooling level, 51.82% were dissatisfied. A linear trend test revealed a statistically significant association (p < 0.001). The lower the educational level, the more concerned adolescents were about having facial acne (Table 3).
TABLE 3.
Association of dissatisfaction with schooling and socioeconomic level, distributed according to location of the acne (facial, dorsal, presternal).
| Schooling quartiles | Socioeconomic classes | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1º | 2º | 3º | 4º | p | A | B | C | D | p | |
| Facial acne | 315 | 210 | 236 | 213 | 0.001* | 48 | 388 | 485 | 34 | 0.004* |
| 66.04% | 60.52% | 53.27% | 51.82% | 42.86% | 56.98% | 60.70% | 58.62% | |||
| Dorsal acne | 164 | 111 | 162 | 162 | 0.001* | 32 | 231 | 281 | 18 | 0.003* |
| 59.64% | 50.45% | 51.10% | 45.02% | 41.03% | 48.63% | 55.53% | 60.00% | |||
| Presternal acne | 105 | 68 | 73 | 80 | <0.001* | 17 | 137 | 154 | 16 | |
| 60.69% | 48.23% | 41.24% | 41.03% | 37.78% | 45.51% | 50.33% | 59.26% | 0.035* | ||
Linear tendency test
The skin color analysis was dichotomized into whites and non-whites. Among whites, 55.74% showed some degree of dissatisfaction, and 64.37% among non-whites. This difference was statistically significant (p = 0.002) (Table 4).
TABLE 4.
Association of dissatisfaction with skin color.
| Whites with dissatisfaction | Non-whites with dissatisfaction | p | |
|---|---|---|---|
| Facial acne | 685 | 289 | |
| 55.74% | 64.37% | 0.002 ** | |
| Dorsal acne | 415 | 153 | |
| 49.40% | 58.17% | 0.013 ** | |
| Presternal acne | 244 | 82 | |
| 46.21% | 51.90% | 0.238 ** |
Chi Square test
The association with the presence of facial acne and socioeconomic status showed that: 58.62% from level D were dissatisfied, while the equivalent figures were 60.70% for level C, 56.98% for level B and 42.86% for level A. This association was statistically significant (p = 0.004) (Table 3).
Pre-external acne- regarding schooling: in the first quartile, 60.69% reported dissatisfaction, 48.23% in the second, 41.24% in the third, while in the fourth quartile (the group with the highest educational levels), 41.03% were unsatisfied. Thus, individuals with lower levels of education presented a higher degree of dissatisfaction (p < 0.001) (Table 3).
In relation to skin color, 46.21% of the whites reported dissatisfaction, compared with 51.90% of non-whites. This association was not statistically significant (p = 0.238) (Table 4).
As regards socioeconomic levels, 59.26% from level D showed dissatisfaction, while the equivalent figures were 50.33% for level C, 45.51% for level B and 37.78% for level A. This association was statistically significant (p=0.035) (Table 3).
Acne on the back- schooling level, in the first quartile 59.64% said they had some degree of dissatisfaction, in the second 50.45%, in the third 51.10% and in the fourth quartile 45.02%. Therefore, the lower the schooling level, the more concerned adolescents will be about acne on their backs. This association was statistically significant (p = 0.001) (Table 3).
Whites were more dissatisfied with the presence of acne on the back than non-whites (p=0.013). Among whites, 49.40% said they had some degree of dissatisfaction, while among non-whites it was 58.17% (Table 4).
As for the socioeconomic level, 60% from level D had some degree of dissatisfaction, compared with 55.53% for level C, 48.63% for level B, and 41.03% for level A. Again, adolescents from the lower social classes were more concerned about acne, with a statistical significance (p = 0.003) (Table 3).
DISCUSSION
Acne is a highly prevalent disease among adolescents and young adults. Studies indicate that up to 95% of men and 83% of women are affected by it until they reach their twenties.9 In approximately 10% of cases, acne becomes severe.6,10,11
Adolescence is a period of physical, emotional and social changes.3,6 It is a transition and adaptation phase, in which adolescents form new relationships, friendly and romantic, and begin to acquire a new status in society.11 This is the exact period that acne appears. Despite being considered a cosmetic and temporary problem, the sequelae of acne can be permanent in the lives of individuals affected by it.8,10 Such a potentially disfiguring condition, acne can result in low self-esteem or be reinforced by insensitive comments and experiences of inter-personal rejection.12,13
This population-based study found a higher prevalence of acne on the face, back and chest, respectively.
With respect to location, individuals with acne on the face exhibited higher rates of dissatisfaction with their appearance: 58.04% reported some degree of dissatisfaction, while 51.49% were dissatisfied with acne on their back, and 47.52% with acne on their chest. In the literature, only one article stratified cases according to lesion topography. The results found were similar to ours, although the study only comprised 145 individuals.9
When our results were analyzed in relation to skin color, non-whites with acne on the face and back were more affected than whites. For individuals with acne on the chest, the result was not significant, which can be explained by the smaller number of individuals in this group. Again, the aforementioned study obtained similar results: non-whites suffer more from acne.9
When socioeconomic and schooling levels were analyzed, irrespective of topography, individuals of lower education and income categories felt more affected by the presence of acne. This could be explained by the greater difficulty of disadvantaged classes to access treatment.
Skin appearance is important for the individual's self-image and social interaction.11,12 In adolescence, acne vulgaris is the most common skin disease, and its effects on appearance can lead to changes in body image, which in turn, may result in anger, fear, shame, anxiety, depression, embarrassment, bullying and stigmatization of individuals in a group.2,13-20 Lack of confidence, social withdrawal, feelings of insecurity and inferiority, limited employment opportunities, difficulties at work and in interpersonal relationships, and suicidal ideation are also related to the effects of changes in individuals with acne.2,5,6,10,16
This study is justified due to the high prevalence of juvenile acne and the proven emotional impact that this disease causes.21-24 There are no studies focusing on the male population. In addition, our sample comprised 2,200 men and it is considered a population-based study, hitherto unavailable in any other published work, with Brazilian samples. In this study, gender and age are not variables, representing a limitation of this study.
The impact caused by acne can be more severe for patients than doctors believe; therefore, it is important to focus the evaluation on the individual's subjectivity, not only on the objectivity of the skin lesion.
CONCLUSION
This population-based study found a high prevalence of acne on the face, back and chest, with high rates of dissatisfaction.
Footnotes
Conflict of interest: None
Financial funding: None
Work performed at the Universidade Católica de Pelotas (UCPel) - Pelotas (RS), Brazil.
How to cite this article: Isaacsson VCS, Almeida Jr HL, Duquia RP, Breunig JA, Souza PRM. Dissatisfaction and acne vulgaris on male adolescents and associated factors. An Bras Dermatol. 2014;89(4):576-9.
REFERENCES
- 1.Sampaio SAP, Rivitti EA. Sampaio SAP, Rivitti EA. Dermatologia. São Paulo: Artes Médicas; 1998. Foliculoses; pp. 291–306. [Google Scholar]
- 2.Do JE, Cho SM, In SI, Lim KY, Lee S, Lee ES. Psychosocial Aspects of Acne Vulgaris: A Community-based Study with Korean Adolescents. Ann Dermatol. 2009;21:125–129. doi: 10.5021/ad.2009.21.2.125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Féton-Danou N. Psychological impact of acne vulgaris. Ann Dermatol Venereol. 2010;137:S62–S65. doi: 10.1016/S0151-9638(10)70028-4. [DOI] [PubMed] [Google Scholar]
- 4.Rapp DA, Brenes GA, Feldman SR, Fleischer AB, Jr, Graham GF, Dailey M, et al. Anger and acne: implications for quality of life, patient satisfaction and clinical care. Br J Dermatol. 2004;151:183–189. doi: 10.1111/j.1365-2133.2004.06078.x. [DOI] [PubMed] [Google Scholar]
- 5.Magin P, Adams J, Heading G, Pond D, Smith W. Psychological sequelae of acne vulgaris: results of a qualitative study. Can Fam Physician. 2006;52:978–979. [PMC free article] [PubMed] [Google Scholar]
- 6.Hassan J, Grogan S, Clark-Carter D, Richards H, Yates VM. The individual health burden of acne: appearance-related distress in male and female adolescents and adults with back, chest and facial acne. J Health Psychol. 2009;14:1105–1118. doi: 10.1177/1359105309342470. [DOI] [PubMed] [Google Scholar]
- 7.Ayer J, Burrows N. Acne: more than skin deep. Postgrad Med J. 2006;82:500–506. doi: 10.1136/pgmj.2006.045377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Halvorsen JA, Stern RS, Dalgard F, Thoresen M, Bjertness E, Lien L. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2011;131:363–370. doi: 10.1038/jid.2010.264. [DOI] [PubMed] [Google Scholar]
- 9.Bashir K, Dar NR, Rao SU. Depression in adult dermatology outpatients. J Coll Physicians Surg Pak. 2010;20:811–813. [PubMed] [Google Scholar]
- 10.Green L. The effect of skin conditions on patients' quality of life. Nurs Stand. 2010;25:48–55. doi: 10.7748/ns2010.11.25.9.48.c8078. [DOI] [PubMed] [Google Scholar]
- 11.Dunn LK, O'Neill JL, Feldman SR. Acne in adolescents: quality of life, self-esteem, mood, and psychological disorders. Dermatol Online J. 2011;17:1–1. [PubMed] [Google Scholar]
- 12.Bowe WP, Leyden JJ, Crerand CE, Sarwer DB, Margolis DJ. Body dysmorphic disorder symptoms among patients with acne vulgaris. J Am Acad Dermatol. 2007;57:222–230. doi: 10.1016/j.jaad.2007.03.030. [DOI] [PubMed] [Google Scholar]
- 13.Costa A, Alchorne MMA, Goldschmidt MCB. Etiopathogenic features of acne vulgaris. An Bras Dermatol. 2008;83:451–459. [Google Scholar]
- 14.Costa A, Alchorne MMA, Michalany NS, Lima HC. Acne vulgaris: a pilot study to assess an oral treatment with essential fatty acids using clinical, digital, and pathological analyses. An Bras Dermatol. 2007;82:129–134. [Google Scholar]
- 15.Sobral JF, Filho, Nunesmaia HGS, Fonseca ESVB, Damiäo RS. Epidemiological and genetic aspects of acne vulgaris in university of Joäo Pessoa - PB. An Bras Dermatol. 1993;68:225–228. [Google Scholar]
- 16.Costa A, Lage D, Moisés TA. Acne and diet: truth or myth? An Bras Dermatol. 2010;85:346–353. doi: 10.1590/s0365-05962010000300008. [DOI] [PubMed] [Google Scholar]
- 17.Almeida HL, Jr, Nudelmann L, Göebel J, Janovik N, Hein J. Vellus hair cysts presenting as an atypical acneiform eruption. An Bras Dermatol. 2011;86:789–790. doi: 10.1590/s0365-05962011000400027. [DOI] [PubMed] [Google Scholar]
- 18.Fried RG, Wechsler A. Psychological problems in the acne patient. Dermatol Ther. 2006;19:237–240. doi: 10.1111/j.1529-8019.2006.00079.x. [DOI] [PubMed] [Google Scholar]
- 19.Ali G, Mehtab K, Sheikh ZA, Ali HG, Abdel Kader S, Mansoor H, et al. Beliefs and perceptions of acne among a sample of students from Sindh Medical College, Karachi. J Pak Med Assoc. 2010;60:51–54. [PubMed] [Google Scholar]
- 20.Smithard A, Glazebrook C, Williams HC. Acne prevalence, knowledge about acne and psychological morbidity in mid- adolescence: a community-based study. Br J Dermatol. 2001;145:274–279. doi: 10.1046/j.1365-2133.2001.04346.x. [DOI] [PubMed] [Google Scholar]
- 21.Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, Katsambas A. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol. 2012;87:862–869. doi: 10.1590/S0365-05962012000600007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tejada Cdos S, Mendoza-Sassi RA, Almeida HL, Jr, Figueiredo PN, Tejada VF. Impact on the quality of life of dermatological patients in southern Brazil. An Bras Dermatol. 2011;86:1113–1121. doi: 10.1590/s0365-05962011000600008. [DOI] [PubMed] [Google Scholar]
- 23.Ribas J, Oliveira CMPB, Ribeiro JCS. Acne vulgaris and well-being in medical students. An Bras Dermatol. 2008;83:520–525. [Google Scholar]
- 24.Taborda MLVV, Weber MB, Freitas ES. Assessment of the prevalence of psychological distress in patients with psychocutaneous disorder dermatoses. An Bras Dermatol. 2005;80:351–354. [Google Scholar]