

Abstract
Humans are exposed to viruses everywhere they live, play, and work. Yet people’s beliefs about viruses may be confused or inaccurate, potentially impairing their understanding of scientific information. This study used semi-structured interviews to examine people’s beliefs about viruses, vaccines, and the causes of infectious disease. We compared people at different levels of science expertise: middle school students, teachers, and professional virologists. The virologists described more entities involved in microbiological processes, how these entities behaved, and why. Quantitative and qualitative analyses revealed distinctions in the cognitive organization of several concepts, including infection and vaccination. For example, some students and teachers described viral replication in terms of cell division, independent of a host. Interestingly, most students held a mental model for vaccination in which the vaccine directly attacks a virus that is present in the body. Our findings have immediate implications for how to communicate about infectious disease to young people.
Keywords: viruses, vaccines, mental models, expertise, public understanding of science and health, infectious disease
Introduction
Viral diseases create health concerns around the globe. For example, influenza epidemics cause 3–5 million cases of severe illness and an estimated half million deaths worldwide each year (Stohr, 2002; World Health Organization [WHO], 2009). In the United States alone, estimates indicate that more than a million people are infected with HIV, with one in five unaware of their condition (Centers for Disease Control and Prevention (CDC), 2008; UNAIDS, 2010). Genital human papillomavirus (HPV) infection, now the most common sexually transmitted disease in the United States, has an overall prevalence rate of over 25% in both men and women, with an estimated 6 million individuals newly infected every year (Dunne et al., 2007; Dunne, Nielson, Stone, Markowitz, & Giuliano, 2006). Such viruses place an enormous burden on productivity and healthcare (Gasparini, Amicizia, Lai, & Panatto, 2012; Marchisio, Baggi, Bianchini, Principi, & Esposito, 2012), and an immeasurable toll on those whose lives are directly affected.
A crucial development in managing viral disease has been the development and widespread availability of vaccines (Oldstone, 1998). Yet, people’s beliefs about viruses, vaccines, and the causes of infectious disease can affect their acceptance of scientific information. In the U.S., a growing number of parents are declining the Measles, Mumps, and Rubella (MMR) vaccine for their children, partly in response to false claims about its link to autism (Smith, Ellenberg, Bell, & Rubin, 2008). Unscientific messages about vaccines are widespread, and actively promoted. For example, a recent billboard in Times Square, New York displayed a picture of a mother cradling her infant along with the message: “Vaccines: Know the risks.” and “Vaccination. Your Health. Your Family. Your Choice.” (Platts, 2011). While scientific progress in the management of viral diseases has been substantial, its impact depends on achieving a scientifically informed public capable of rejecting such anti-science propaganda.
How can educators increase people’s understanding of viruses, vaccines, and the causes of infectious disease? Simply presenting people with scientific evidence often doesn’t work, because adults and children form their own conceptualizations about the biological and physical world, using their observations, experiences, and background knowledge. These conceptions often deviate substantially from scientific models (diSessa, 2006, Carey, 1985; Chi, Slotta, & de Leeuw, 1994; Duschl, Schweingruber, & Shouse, 2007; Vosniadou & Brewer, 1992). Although most children and adults in the United States are taught biological models of illness, involving germs and viruses as the cause (Lakshmi & Gelman, 2004; Sigelman, 2012), belief formation is also influenced by cultural and developmental factors that provide moral, mystical, or common sense explanations for illness (Hejmadi, Rozin, & Siegal, 2004; Lakshmi & Gelman, 2004; Lakshmi & Gelman, 2004; Legare & Gelman 2008; Zhu, Liu, & Tardif, 2009). Sigelman (2012), for example, found that U.S. children up to 8th grade provided cold weather explanations more often than germ-based explanations for the common cold.
People’s naïve beliefs about science are resistant to change and may persist even in the face of inconsistent evidence (Chinn & Brewer, 1993; Chi, Slotta, & de Leeuw, 1994; Sigelman, 2012; Stein, Hernandez, & Anggoro, 2010). Thus, directly confronting these beliefs and introducing a coherent scientific framework is vital in early instruction (Au & Romo, 1996; Chi & Roscoe, 2002; Chinn & Brewer, 1993; diSessa, 2006; Singer, Nielsen, & Schweingruber, 2012; Stein, Hernandez, & Anggoro, 2010; Vosniadou, 1994). In the case of virology, little is known about people’s beliefs about the microbiology of viruses and vaccines. What do viruses do inside the body? Why do they make us sick? What are vaccines, and how do they work? Identifying people’s answers to questions such as these is an important first step toward creating instruction that will correct and replace naïve beliefs (Singer et al., 2012). This was the main aim of our research.
Present study
This study examined people’s microbiological-level beliefs about viruses, vaccines, and the causes of infectious disease in three groups with different levels of science experience: middle school students, middle or high school teachers (primarily science teachers), and expert virologists. Middle school students represent the group with the least experience, although these students do encounter scientific information about viruses in school. Teachers represent an intermediate level of experience: some are engaged in explaining virology concepts to students while others represent educated, but not expert, adults. The virology experts represent the highest level of experience, and their responses provide a standard against which to compare the other two groups.
Our research approach was intended to identify the mental models of participants—their causal explanations of the microbiological activity of viruses and vaccines. In mental models research (e.g., Chi et al., 1994; Gentner & Stevens, 1983; Vosniadou, 1994; Vosniadou & Brewer, 1994) interviews are typically used to elicit causal explanations from the participant. The interviewer asks generative questions (cf. Vosniadou, 1994), which require the participants to explain phenomena that they cannot directly observe. Participants’ explanations can be used to create causal diagrams or illustrations that capture the structure and content of their mental models. For example, Vosniadou and Brewer (1994) identified several distinct mental models that children have about the shape of the Earth, including a “hollow sphere” model in which humans inhabit Earth’s interior, and the sky exists only above. This model is causal in nature, because the hypothesized properties of the Earth provide an explanation for the child’s observations, such as the apparent flatness of the Earth, and the limited range of sky that is visible from Earth’s surface.
In the present research we conducted individual structured interviews with middle school students, teachers, and experts. Interviews probed participants’ beliefs about eight key topics, which were identified through a collaborative process involving the researchers and a virology expert. The topics were intended to cover fundamental concepts related to the microbiological activity of viruses and vaccines, including: (1) the external appearance of the virus, (2) the external appearance of the host cell, (3) the contents of the virus, (4) the contents of the host cell, (5) the replicated virus, (6) the impact of the virus on the immune system, (7) the immune cell, and (8) vaccination.
Our analyses involved quantitative and qualitative techniques to explore the depth, breadth, and structure of the explanations provided by each group. Our quantitative analyses drew on the Structure-Behavior-Function (SBF) framework used in prior research on expert knowledge (e.g., Hmelo-Silver & Pfeffer, 2004; see also Chi, De Leeuw, Chiu, & LaVancher, 1994). The framework provides a way of capturing differences in knowledge between individuals or groups by analyzing their representations of a complex process or system in terms of structures (the elements of a system), behaviors (the activity of an element), and functions (the purpose of an element in a system). By applying this framework to our participants’ responses, we can more specifically identify differences in knowledge between the groups. Previous research has found that experts possess more knowledge about the functions of entities in their domain of expertise (Hmelo-Silver & Pfeffer, 2004; Medin, Lynch & Coley, 1997). Thus, we predicted that people with greater expertise in virology would be more likely to describe the various interview topics at a functional level. Our qualitative analyses aimed to visually represent participants’ mental models for various interview topics in the form of causal diagrams. Using the virologist’s mental models as a standard, we aimed to identify common areas of understanding as well as misconceptions about the microbiology of viruses.
Method
Participants
Our methods and analyses aligned with Hmelo-Silver and Pfeffer (2004), who investigated mental models of aquaria across different levels of expertise: middle school students (n=11), pre-service teachers (n=11), and experts (n=8). We used their sample sizes (which are typical for mental models research; Singer et al., 2012) as a guideline for our own. Our participants were 13 ninth grade students and 18 teachers from an urban school district in Nebraska, and 7 domain experts in virology. All were paid for their participation. Half of the teachers taught at the middle school level and half taught at the high school level. The majority of the teachers (13 of 18) taught science as their primary subject. Each of the virology experts possessed an advanced graduate or medical degree and over 10 years of experience working in virology. Participants were selected on the basis of their participation in a two-week immersive program, the Omaha Science Media Project (http://www.worldofviruses.unl.edu/osmp.shtml), in which students and teachers created videos and radio programs while spending time in virology research laboratories.
Materials
An interview protocol guided the interviewer to cover the eight main topic areas listed above. The protocol contained prompts to encourage the participant to discuss these topics and to probe the participant’s responses more deeply for structural, behavioral, and functional beliefs. For example, the section of the interview about the external appearance of the virus was initiated by asking the participant to describe what a virus looks like. If the participant stated that a virus has “parts on the outside,” then they would be asked to describe what the parts look like, what they do, and what purpose they serve. Prompts for each of the eight key topics are listed in the Appendix. The protocol also helped to ensure that participants discussed the topics in roughly the same order and at a comparable level of detail, while at the same time providing enough flexibility to allow us to capture variations in participants’ mental models.
The interviews were recorded using a digital video camera with a microphone. The student interviews were conducted in a quiet room during their participation in the Omaha Science Media Project. The teachers were interviewed before the program in a convenient location, such as their home or office. Experts were interviewed in their office or lab.
Procedure
A trained experimenter interviewed each participant individually. The participant was seated across from the interviewer, and the camera was focused on the participant. At the onset of the interview, the participant was told: “This conversation is for me to find out what you think about viruses. This isn’t about whether your ideas are right or wrong – many of the questions that I’ll ask don’t have a right or wrong answer. I’m just interested in your ideas. Even if you feel you are uncertain, I’d like to hear what’s on your mind. I might ask you to expand on some of your answers, just so that I have a clearer idea about what you are saying.” The interviewer never provided feedback about the accuracy of the participant’s responses; however, the interviewer was instructed to elicit a high level of detail from the participant, and to use prompts when necessary. Each interview began with the same question: what is a virus? The interviews then proceeded on to each of the eight key topics in the order specified above, using the prompts shown in the Appendix when needed. When the participant responded to all of the experimenter’s follow up questions about a topic, or stated that he/she had provided as much detail as they could, a new topic was introduced. There was no standard way to transition to a new interview topic. If a topic had already been mentioned, the interviewer might say: “Let’s bring back the topic of…” If a topic had not been mentioned, they might say: “Let’s move on to the topic of…” Each interview lasted from 60 to 90 minutes.
Data coding
Audio from each interview was transcribed and coded using a system created and refined by two primary researchers and a virologist. The coding captured each participant’s discussion of the eight key topics identified above. To explore expertise-related differences in the depth of their explanations, we coded participants’ responses for the presence of structural, behavioral, and functional descriptions (cf. Hmelo-Silver & Pfeffer, 2004). For example, if a participant mentioned the specific contents of the virus (e.g., “chemicals, proteins, and germs”, or “nucleic acid, DNA, and RNA”), then this was response was coded as giving a structural description of this topic. If participants described how the contents acted (e.g., “DNA splits”, or “DNA uses the enzymes of the host cell”), then we coded their responses as providing a behavioral description. These responses were considered behavioral because they describe the mechanism through which a function, i.e., virus replication, is accomplished. Finally, if participants described the purpose or role of a behavior or structure (e.g., “splitting allows the virus to reproduce”, or “the virus DNA uses the host DNA to replicate”), then their utterance was coded as a functional description.
Two independent research assistants scored each interview for the presence or absence of structures, behaviors, and functions with high reliability (Cohen’s Kappa = .88). Disagreements between the coders were resolved through discussions involving one of the primary researchers.
Our qualitative analyses involved identifying the causal claims that participants made about each topic. We created causal schematic diagrams to display the various entities—such as the virus and host cell—and parts—such as the virus DNA/RNA and the host cell receptors—that participants discussed. The entities and parts are connected in the diagrams through the relations that the participants stated, including causal, spatial, and featural relations. The resulting causal diagrams can be taken as a representation of a specific mental model for a topic.
Results
Quantitative analyses
To explore expertise-related differences in explanatory depth, we computed the mean number of structures, behaviors, and functions discussed by each group across the eight key topics from the coding system. These means are shown in Table 1. It is important to note that we did not consider the scientific accuracy of the descriptions for this analysis, only the type of statement that was made. (The structure and accuracy of participants’ explanations is discussed in greater detail in the qualitative analyses section.)
Table 1.
Mean number of structures, behaviors, and functions in each group’s descriptions of the eight key topics.
| Group | N | Structures | Behaviors | Functions | Total |
|---|---|---|---|---|---|
| Students | 13 | 2.69 (1.18) | 2.92 (1.12) | 1.92 (1.19) | 2.51 (0.52) |
| Teachers | 18 | 3.56 (1.15) | 3.22 (1.44) | 3.33 (1.50) | 3.37 (0.17) |
| Experts | 7 | 5.86 (0.69) | 5.57 (1.71) | 4.43 (1.41) | 5.29 (0.76) |
| Total | 38 | 3.68 (1.54) | 3.55 (1.61) | 3.05 (1.59) |
Note. SDs in parentheses. Means are out of 8.0. Means for totals are weighted by the number of participants in each group.
A 3 (Group: student, teacher, expert) × 3 (Level of Description: structure, behavior, function) mixed factorial ANOVA was conducted. The analysis revealed a significant effect of Group, F(2, 35) = 17.29, p < .05, ηp2 = .50. Post hoc tests using Tukey’s HSD found that, across Level of Description, experts discussed more key topics (M = 5.29, SD = 0.76) than teachers (M = 3.37, SD = 0.17) and students (M = 2.51, SD = 0.52) (ps < .05). There was not a significant difference between the teachers and students. This result indicates that participants with greater expertise mentioned more of the relevant topics. There was also a significant main effect of Level of Description, F(2, 35) = 7.43, p < .05, ηp2 = .18. A linear contrast analysis found that, overall, participants described structures most often (M = 3.68, SD = 1.54), followed by behaviors (M = 3.55, SD = 1.61), and functions (M = 3.05, SD = 1.59), F(1, 35) = 9.41, p < .05, ηp2 = .21. Thus, when participants discussed the structure of some entity or part, they described its behavior more often than its function. The Group × Level of Description interaction was only marginally significant, F(2, 35) = 2.34, p < .10, ηp2 = .12, likely due to the relatively low power (.65) for detecting this particular effect. We predicted that the groups with more experience would provide a greater number of functional descriptions. While the number of functional descriptions did increase with the group’s level of experience, Table 1 shows that this pattern appeared at the structural and behavioral levels as well. Thus, the marginal Group × Level of Description interaction is more likely due to differences in the number of structural, behavioral, and functional descriptions within each group. As Table 1 shows, both the student and expert groups provided relatively fewer descriptions at the deeper levels (behavioral and functional), whereas teachers discussed structure, behaviors, and functions about equally often. Importantly, these findings are not attributable to differences in the length of the interviews between groups. There was no significant difference in the average number of words per interview between students (M = 6806, SD = 1521), teachers (M = 6313, SD = 545), and experts (M = 7118, SD = 1297), F(2, 35) = 1.58, p = .22, ηp2 = .08.
It is also interesting to examine the explanatory levels of description for each topic separately to identify specific topics that were discussed in greater depth by each group. Table 2 shows the proportion of students, teachers, and experts who discussed each key topic at the structural, behavioral, and functional levels. The bolded and underlined regions indicate a topic that over a third of the participants in a group discussed at a given level. Prior researchers have used this criterion to establish group-level models of understanding (e.g., Lynch & Medin, 2006). Using this criterion leads to several new insights. For example, Table 2 indicates that the students discussed certain topics (the virus contents, the immune cell, and vaccines) more often than other topics, suggesting that these topics are more central to the students’ understanding. The teachers tended to discuss the same topics as the students; however, the teachers discussed functions for each topic, whereas students tended to discuss function only for vaccines. This result indicates greater depth in the teachers’ explanations. In addition, the teachers discussed the topic of the replicated virus, especially its behavior and function, suggesting that teachers provided more complete explanations of the replication process. In contrast to students and teachers, the experts described almost every topic at multiple levels and often covered all three levels. The virologists’ explanations were thus broader, deeper, and more coherent than the other groups’ explanations.
Table 2.
Proportion of participants who discussed the key topics at each level of description.
| Interview topic | Students | Teachers | Experts | ||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| S | B | F | S | B | F | S | B | F | |
| 1. Virus appearance | .23 | .15 | .08 | .39 | .28 | .28 | 1.0 | .57 | .57 |
| 2. Host appearance | .15 | .08 | .08 | .17 | .00 | .00 | .43 | .29 | .00 |
| 3. Virus contents | .85 | .38 | .31 | .83 | .72 | .67 | 1.0 | 1.0 | 1.0 |
| 4. Host contents | .46 | .08 | .00 | .61 | .22 | .17 | 1.0 | .29 | .14 |
| 5. Replicated virus | .00 | .31 | .00 | .06 | .56 | .44 | .57 | .86 | .43 |
| 6. Virus/immune system | .00 | .62 | .31 | .00 | .22 | .39 | .00 | .86 | .43 |
| 7. Immune cell | .54 | .46 | .23 | .50 | .29 | .44 | .86 | .71 | .86 |
| 8. Vaccine | .46 | .85 | .92 | 1.0 | .83 | .94 | 1.0 | 1.0 | 1.0 |
Note. S, B, and F stand for the structural, behavioral, and functional levels of description respectively. Bolded and underlined numbers indicate a proportion greater than 33%.
In addition to showing the topics that participants discussed, Table 2 also shows that participants, regardless of their expertise, seldom described the external appearance of the host cell and its contents. This finding may be attributable to how viral infection and replication were discussed. Participants generally described the virus and the contents of the virus as active agents, and placed the host in the passive role. Descriptions of virushost interactions were therefore likely to emphasize the behavior and function of the virus rather than the host.
Qualitative analyses
These analyses focus on the topics that all three groups discussed at multiple levels of detail: the virus contents, the immune cell, and vaccines. Although the groups tended to discuss each of these topics in depth, this does not imply that they provided qualitatively similar descriptions; in fact there were substantial differences in their explanations. To capture these qualitative differences, one of the primary investigators examined the interview transcripts to identify different types of explanations for each topic. Of primary interest were the different causal mechanisms that participants mentioned in their explanations of virus replication, immune response, and vaccination. These differences represent fundamental differences in the mental models around which these topics are organized cognitively. When a causal description was common to at least three participants, it was represented as a diagram. Following conventions within the psychological literature (e.g., Glymour, 2001), entities in the causal diagrams were represented as boxes, and relations were represented as directed arrows (note that different kinds of relations are represented, including causal and spatial relations). Figure 1 provides examples. The diagrams represent an attempt to capture the common structure of different explanations; some details and variations in wording were removed in the process. Two independent coders used the causal diagrams to classify the participants’ responses for each of three topics (if the participant in fact discussed the topics). The coders were instructed to identify the causal diagram that best fit the participant’s explanation. Coders also could respond that there was no good fit. The coders classified the causal explanations with high reliability (Cohen’s Kappa = .89). Disagreements between the coders were resolved through discussion.
Figure 1.
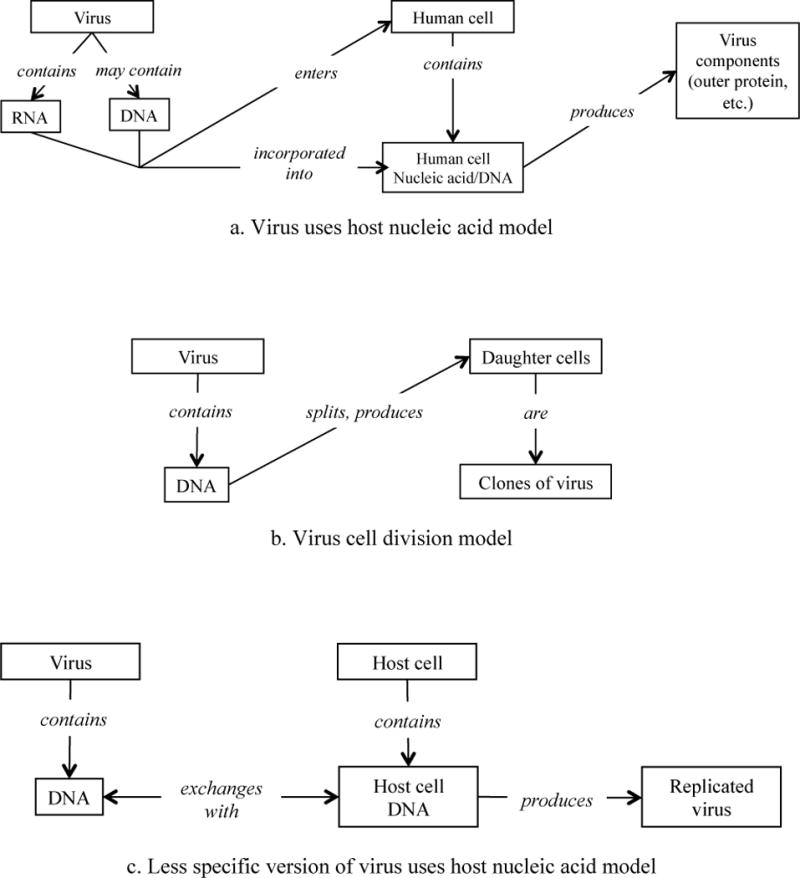
Mental models of virus replication.
Contents of the virus
Table 2 shows that participants in each group frequently provided structural descriptions of the contents of the virus. Each expert mentioned nucleic acid (or DNA and RNA, specifically) in his or her structural description of the contents of the virus. Most teachers (11 of 18) mentioned either DNA or RNA in their structural descriptions; however, several teachers described the virus contents as “protein,” “pure sickness,” “cellular parts,” or “poison.” In comparison, 6 of 13 students mentioned either DNA or RNA, and several described the contents of the virus as “cells,” “a nucleus,” “bacteria,” “chemicals,” or “harmful stuff.” Thus, although a high proportion of the teachers and students gave structural descriptions, only 46% of the students and 61% of the teachers incorporated the concepts of DNA or RNA in their mental model, as all experts did.
Table 2 also shows that the frequency of behavioral and functional descriptions for this topic increased with experience level. The experts’ behavioral descriptions focused on interactions between the contents of the virus and the host cell, e.g., “the nucleic acid of the virus incorporates itself into the nucleic acid of the human cell,” or “the virus utilizes the host cell’s enzymes.” These behavioral descriptions related primarily to the function of replication: “to make more viruses,” or “to replicate nucleic acid,” etc. For example, one expert said:
A virus has RNA on the inside and some have DNA…When [the virus nucleic acid] gets into the cell it incorporates itself into the nucleic acid of the human cell. So it’s using the human cell and it’s using its code to tell that cell to make [the virus] coat, outer protein and everything else.
A causal diagram representing this typical expert explanation is presented in Figure 1a, the “virus uses host nucleic acid” model.
Six of the 18 teachers provided causal explanations that were similar to the experts’. Examples of teachers’ explanations are, “viruses reproduce by exchanging a part of their RNA with the host organism’s,” and “[the virus] takes over the machinery of the host cell to make more copies of itself.” These responses fit the “virus uses host nucleic acid” model. However, three teachers described an alternative mechanism for replication—e.g., “DNA splits to reproduce virus,” “it starts dividing and multiplying,” or “virus reproduces like molecular replication.” For example, one teacher stated:
Viruses reproduce by splitting…the [virus’] DNA lines up, splits and so there’s two what they call daughter cells and they’re identical cells. So that’s how they reproduce. They just kind of make clones of themselves and copies.
This type of response is represented in Figure 1b, the “virus cell division” model. This mental model was also held by 6 of the 13 students, making it the most common model within the student group.
Five teachers described the behavior of the virus broadly, without specifying the mechanism through which the virus replicates. Although generally consistent with the “virus uses host nucleic acid” model, these responses lacked important structural and behavioral details. Four of the 13 students provided similar explanations. A response of this kind is represented in the following student statement, shown in Figure 1c:
Viruses contain DNA…Viruses reproduce when they switch off DNA with the [host] cell…it takes the DNA from it and makes another body with it. And then it keeps doing that. The virus takes the DNA…and makes a whole new body.
Immune cells
Participants in the three groups expressed similar ideas about the structure, behavior and function of immune cells. Participants at each experience level mentioned “T cells,” “white blood cells,” “antibodies,” and “antigens.” Only the virologists mentioned “B cells,” “macrophages,” and “natural killer cells.” Thus, the experts’ mental models were more conceptually complex. The following excerpt is from one expert’s description the immune cells:
Typically the body reacts by trying to generate antibodies specific to the virus and also generate T cells to attack the cells that are infected with the virus…to try to eradicate virus and virus infected cells…T cells and macrophages go to the site of infection to try to mop up the infection.
Teachers and students provided similar descriptions but posed them in more general terms. Their descriptions often lacked the distinctions between the behavior and function of the different types of immune cells described by the experts. For example:
The white cells identify [the virus], then destroy it… (Teacher)
It goes to the target [i.e., virus] cell and…[the immune cell] comes and like feels it and it’s like, ‘oh, that’s foreign’ and it tries to kill it.”(Student)
Vaccines
Table 2 shows that vaccines were the topic described in the most detail across the three groups. Unlike most of the other topics, participants described vaccines most often at the functional level, focusing on the role of the vaccine inside the body. The experts and teachers described vaccines similarly across the three levels of description. Consider the following excerpts:
A vaccine is really an artificial means of stimulating the immune system to protect you against some infectious agent…You find out what part of the viral particle could be part of the virulence factor of the virus and you try to find a way to stimulate the immune system to knock that out. (Expert)
A vaccine…is a small amount of the virus that they are putting into your body to hope that your body will take that and make antibodies, if I’m thinking correctly, against that disease. So that if you come in contact with [the virus] you will not get it. (Teacher)
The structure of the vaccine was described variously as “a replica of the virus” (Expert), “a viral particle that could be part of the virulence factor of the virus” (Expert), “a diluted type of virus” (Teacher), or “a weaker form of the virus” (Teacher). In describing the behavior of the vaccine, each expert mentioned either the immune system or antibodies, e.g., “the vaccine stimulates the immune system.” Many of the teachers mentioned this same behavior, but in more general terms, such as “teaches your body to fight the virus,” or “gives your body a preview of the virus.” At the functional level, both the virologists and teachers mentioned preparation to fight or prevent future infection, e.g., “you will have antibodies specific to clear up the virus” (Expert), or “a vaccine helps your body to recognize the virus and help fight it” (Teacher). Overall, the experts and teachers held the “vaccine stimulates immune system” model in Figure 2a.
Figure 2.
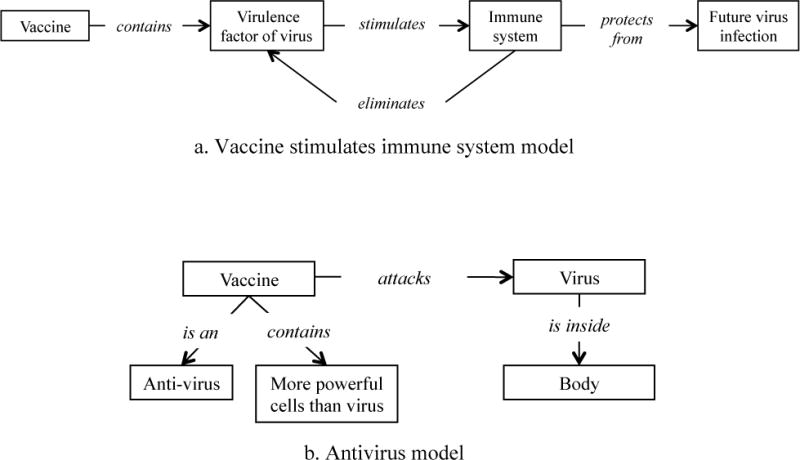
Mental models of vaccines.
The students’ functional descriptions of vaccines were similar to the teachers’ and experts’; for example, “prevents body from getting virus,” or “helps fight off that virus before it gets to your system.” Students’ structural and behavioral descriptions, however, revealed two different mental models for how vaccines carry out this function. Four students described vaccines similarly to the experts and teachers (the “vaccine stimulates immune system” model). However, 7 of the 13 students described a vaccine as an antivirus, which works by “attacking the virus in the body,” or “creating a barrier from the virus.” This belief was also reflected in these students’ structural descriptions, which included “a chemical, anti-version of the virus,” or “liquid, antibodies.” Thus, rather than preparing the immune system to fight infection, many students thought that vaccines fought infections directly. The following excerpt from a student interview captures this belief:
A vaccine…is like an anti-version of the virus…a vaccine works the same way viruses attack our cells…I think the chemicals or whatever they inject has cells to it…and those are more powerful than the virus itself and it attacks the virus in the body. (Student)
This “antivirus” mental model is represented in Figure 2b.
Topics discussed exclusively by the experts
Table 2 reveals that the experts more often discussed the external appearance of the virus and the host cell than the other two groups did. These topics were mentioned in the context of explanations of how the virus attaches itself to the host cell. Most of the experts mentioned that many viruses have a “protein coat,” “attachment proteins,” or “lipid coat,” which can attach to a specific host cell’s receptors. As one expert put it:
The reason [the virus and host] are linked is that over long periods of time the virus has evolved into a cellular protein or a series of cellular proteins, as the door. And it would be senseless to use something like the door to walk into a room where there’s not a party going on. And so the virus has learned to go only into the rooms with the party…
The experts mentioned several different mechanisms of attachment and entry, including puncturing, penetrating, or fusing to the host cell. Each group’s interview responses were coded for the presence of descriptions of attachment. All seven experts mentioned attachment, compared to 11 of 18 teachers and 3 of 13 students. The experts’ frequent description of attachment indicates a greater level of coherence between their mental models of the various stages of infection. As the above quote illustrates, the experts were also sensitive to the fact that virus attachment is specific to the properties of the host cell. Thus, only certain cells can become infected.
Discussion
Our main goal was to examine people’s mental models of viruses, vaccines, and infectious disease at different levels of expertise. An analysis of student, teacher, and expert explanations of these topics yielded several main findings. As expected, the experts discussed more topics than either the students or teachers did. The experts also provided more descriptions across each level of detail—structural, behavioral, and functional. Our finding differs from Hmelo-Silver and Pfeffer (2004), who discovered expertise-related differences in functional knowledge only. This discrepancy is perhaps because the domain that we investigated involves more invisible entities than the domain that Hmelo-Silver and Pfeffer (2004) investigated (aquariums). Novices may have little structural knowledge of viruses, vaccines, and other such entities, because these structures cannot be observed with the naked eye. All three groups provided relatively rich descriptions of the contents of viruses (and how viruses replicate), immune cells, and vaccines. Teachers’ and students’ explanations of these topics often aligned with the experts’ explanations, but were less detailed. In some cases, however, the teachers and students had entirely different mental models. Strikingly, many students described virus replication in terms of cell division rather than as a result of the interaction with the host. Furthermore, students described vaccines as a sort of antivirus or virus-killing antibiotic, with vaccination acting to treat a preexisting infection.
Understanding that biological entities are involved in illness—as opposed to environmental factors such as cold weather, or psychological factors such as morality—is a crucial step toward scientific proficiency. Yet, a sophisticated understanding of these topics requires understanding the microbiological activity of viruses and vaccines. Our research finds that students, and even a few teachers, held misconception about these topics. Many students explained virus replication as cell division, omitting key entities, such as the host cell, and processes, such as the virus attaching to the host cell receptors. The “antivirus” mental model of vaccines was also common among students. Again, key entities and processes were missing—this model does not include the immune system and its response to the vaccine. Thinking of vaccines as a treatment for infection may also lead a person to misunderstand the long-term and beneficial effects of vaccination.
If people have inaccurate mental models of viruses and vaccines, then simply presenting them with correct scientific information may be ineffective. This approach is unlikely to lead people to abandon their naïve models (Au & Romo, 1996; Chi et al., 1994; Chinn & Brewer, 1993; Singer et al., 2012; Vosniadou, 2002). For example, telling a student that a virus needs a host to survive may not change their belief that viruses reproduce through cell division. The student could interpret the statement by thinking that the virus consumes the host cell, perhaps using it as fuel in its reproductive process. Likewise, a student could interpret the information that vaccination has an effect on the immune system within the antivirus mental model. For instance, the student may incorporate the new information by thinking that the virus hides in the immune system, so the vaccine must target the immune system to rid it of infection.
Educational interventions benefit by directly addressing people’s preexisting concepts and beliefs, and by attempting to replace or refine them to support a deeper understanding (Au et al., 2008; diSessa, 2006; Singer et al., 2012). An overarching goal of our project was to contribute to this educational approach. Au and Romo (1996) provide an example of how children’s misconception that HIV is a nonbiological entity can be confronted and corrected. The researchers attempted to replace this misconception with a causally coherent biological framework for AIDS infection. The research involved a lesson that described the AIDS virus as a living thing that can only infect a person and make them sick when it is alive. Children in their experimental condition were taught that the AIDS virus reproduces quickly in the blood of a person, stays alive but reproduces slowly in saliva, and dies quickly in water or air. Compared to children who received more standard instruction, those who learned the causally coherent biological framework showed better comprehension of the mechanisms underlying infection and better ability to reason about AIDS transmission.
One reason why it is difficult to understand viruses and vaccines is because their structures and behaviors are invisible to the naked eye. A potentially powerful way to introduce a scientific framework in such cases is through analogy (Gentner 1989; Jee et al., 2010; Markman & Gentner, 2000; Vosniadou & Schommer, 1989). Vosniadou and Schommer (1989), for example, found that young children (around ages 6 and 8) had better retention and understanding of an expository text about the immune system’s response to infection when the process was described using an analogy (“An infection is like a war”). Analogies could also help to explain particular aspects of the infection process that few non-experts may know about, such as the attachment of the virus to the host cell. For example, an expert from the present study explained attachment by comparing it to opening a door to a room: the virus evolved to “go only into the rooms with the party.” Analogies are not only useful for getting learning off the ground. In fact, people with extensive expertise often use within-domain analogies to explain and reason about new discoveries in their field (Dunbar, 1997). For people with an understanding of infection, an analogy between infection and vaccination may address incorrect mental models like the “antivirus” model of vaccination. Knowledge of how infection stimulates the immune system to produce antibodies could be used to better understand how vaccination guards against future illness. An important caveat with analogical instruction is that all analogies break down at some point. To reap maximum benefit from an analogy, instructors could point out its limitations and provide supplemental instruction (Jee et al., 2010).
Educational interventions must also be sensitive to the underlying ontologies that shape people’s concepts and beliefs about biology. Research on conceptual development finds that children draw on their knowledge of humans to reason about other biological entities, often explaining behavior in terms of intentionality (Carey, 1985; Hatano & Inagaki, 1997; Kelemen, 1999). We find evidence of intention-based thinking in our study; for example, one student stated that an immune cell “feels [the virus] and it’s like, ‘oh, that’s foreign,’ and it tries to kill it.” Intention-based explanations often precede, and may provide a foundation for, the acquisition of mechanistic causal understanding (Hatano & Inagaki, 1997; Kelemen, 1999), but people may never reach this level of understanding, and, even if they do, they may revert back to intention-based anthropomorphic reasoning later in life (Bangerter, 2000; Epley, Waytz, & Cacioppo, 2007; Green & Clémence, 2008; Kelemen & Rosset, 2009). Slotta and Chi (2006) found that directly confronting students’ ontological frameworks helps them to understand difficult topics in science. This relates to our earlier point about analogy. Although intention-based explanations may provide a useful device for novice learners, instructors must explain the limits of these explanations, and provide instruction about the true causal mechanisms.
In addition to situating viruses within a biological framework, supporting learning using analogies, and confronting students’ ontological misconceptions, instruction could connect different levels of description: structures, behaviors, and functions. The experts in the present study demonstrated an understanding of these connections for a range of topics; the teachers for fewer topics; but the students rarely described the topics at the functional level, and when they did, they were often inaccurate. The connection between structure, behavior, and function may be especially critical to understanding why different viruses (e.g., HIV, HPV, influenza virus, etc.) affect the body in different ways. The relation between a virus and its host, and the process of attachment, are crucial to this understanding. For example, all of the experts discussed the lock-and-key relationship between virus and host, but the teachers and students did so much less frequently. Future educational interventions should take into account such gaps in people’s knowledge and their consequences for understanding related topics.
There are several important limitations of our study. Our sample was mainly one of convenience. Thus, the extent to which our findings are representative of middle school students and teachers in general is unclear, and this is an important issue to be addressed in future research. Likewise, it would be interesting to include populations that were not part of the present study, such as, adults who are not teachers (i.e., average laypersons). How do their mental models compare to students and teachers? We are also aware of the inherent limitations of our interview method. By requiring participants to articulate their beliefs, we are unable to assess knowledge that may be implicitly stored (Roediger, 1990). Recent research finds that even when people state scientifically accepted views, they may still hold naïve theories that exert an influence on their behavior and thought (Kelemen & Rosset, 2009; Shtulman & Valcarcel, 2012). Thus, future research should assess mental models through multiple measures, including implicit measures.
Conclusion
Our study revealed several ways in which beliefs about the nature of viruses, infectious disease, and vaccines differ between people with different levels of scientific experience. The results indicate that non-experts may hold complex, but scientifically incorrect, mental models of how viruses reproduce, cause disease, etc. Our interest in this topic arose from the observation that people’s beliefs about viruses, vaccines, and the causes of infectious disease can have an important influence their ability to understand and retain scientific information (Au & Romo, 1996 Chinn & Brewer, 1993; Vosniadou, 1994). Understanding these mental models provides a crucial first step toward being able to confront and correct misconceptions that hamper progress toward a scientifically literate public.
Acknowledgments
Funding
This research was supported by the Omaha Schools Foundation and the “World of Viruses” and “Biology of Human” projects funded by the National Institutes of Health through the Science Education Partnership Award Grants Nos. R25RR024267 and R25OD010506. Its content is solely the responsibility of the authors and does not necessarily represent the official views of NIH.
Appendix: Interview prompts for the key topics
| Topic | Interview Prompts |
|---|---|
| 1. External appearance of the virus | What does a virus look like? |
| 2. External appearance of the host cell | * What does a host cell look like? |
| 3. Contents of the virus | Does a virus contain anything? If so, what? |
| 4. Contents of the host cell | * Does a host cell contain anything? If so, what? |
| 5. Replicated virus | What happens after the virus replicates? |
| 6. Impact of virus on immune system | How does the immune system react when a person is infected with a virus? |
| 7. Immune cell | Describe the immune cells that respond to infection. What do they do? |
| 8. Vaccination | What is a vaccine? How do vaccines work? |
Note.
This topic was prompted only when the participant spontaneously mentioned the presence of a host cell.
References
- Au TK, Chan CK, Chan TK, Cheung MK, Ho JY, Ip GW. Folkbiology meets microbiology: A study of conceptual and behavioral change. Cognitive Psychology. 2008;57:1–19. doi: 10.1016/j.cogpsych.2008.03.002. [DOI] [PubMed] [Google Scholar]
- Au TK, Romo LF. Building a coherent conception of HIV transmission: a new approach to AIDS education. In: Medin D, editor. The Psychology of Learning and Motivation. Vol. 35. San Diego: Academic; 1996. pp. 193–241. [Google Scholar]
- Bangerter A. Transformation between scientific and social representations of conception: The method of serial reproduction. British Journal of Social Psychology. 2000;39(4):521–535. doi: 10.1348/014466600164615. [DOI] [PubMed] [Google Scholar]
- Carey S. Conceptual change in childhood. Cambridge, MA: MIT Press; 1985. [Google Scholar]
- Centers for Disease Control and Prevention (CDC) HIV Prevalence Estimates—United States, 2006. Morbidity and Mortality Weekly Report. 2008;57(39):1073–1076. [PubMed] [Google Scholar]
- Chi MT, De Leeuw N, Chiu MH, LaVancher C. Eliciting self-explanations improves understanding. Cognitive Science. 1994;18(3):439–477. [Google Scholar]
- Chi MTH, Roscoe RD. The processes and challenges of conceptual change. In: Limon M, Mason L, editors. Reconsidering conceptual change: Issues in theory and practice. Dordrecht, The Netherlands: Kluwer Academic; 2002. pp. 3–27. [Google Scholar]
- Chi MTH, Slotta JD, de Leeuw N. From things to processes: A theory of conceptual change for learning science concepts. Learning and Instruction. 1994;4:27–43. [Google Scholar]
- Chinn CA, Brewer WF. The role of anomalous data in knowledge acquisition: A theoretical framework and implications for science instruction. Review of Educational Research. 1993;63:1–49. [Google Scholar]
- diSessa AA. Knowledge in pieces. In: Forman G, Pufall P, editors. Constructivism in the computer age. Hillsdale, NJ: Erlbaum; 1988. pp. 49–70. [Google Scholar]
- Dunbar K. How scientists think: On-line creativity and conceptual change in science. In: Ward TB, Smith SM, Vaid J, editors. Creative thought: An investigation of conceptual structures and processes. American Psychological Association; 1997. pp. 461–493. [Google Scholar]
- Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: A systematic review of the literature. The Journal of Infectious Diseases. 2006;194(8):1044–57. doi: 10.1086/507432. [DOI] [PubMed] [Google Scholar]
- Dunne EF, Unger ER, Sternberg M, McQuillan G, Swan DC, Patel SS, Markowitz LE. Prevalence of HPV infection among females in the United States. JAMA: The Journal of the American Medical Association. 2007;297(8):813–9. doi: 10.1001/jama.297.8.813. [DOI] [PubMed] [Google Scholar]
- Duschl RA, Schweingruber HA, Shouse AW, editors. Taking science to school: Learning and teaching science in grades K-8. Washington, DC: National Academies Press; 2007. [Google Scholar]
- Epley N, Waytz A, Cacioppo JT. On seeing human: A three-factor theory of anthropomorphism. Psychological Review. 2007;114(4):864–886. doi: 10.1037/0033-295X.114.4.864. [DOI] [PubMed] [Google Scholar]
- Gasparini R, Amicizia D, Lai PL, Panatto D. Clinical and socioeconomic impact of seasonal and pandemic influenza in adults and the elderly. Human Vaccines & Immunotherapeutics. 2012;8(1):21–8. doi: 10.4161/hv.8.1.17622. [DOI] [PubMed] [Google Scholar]
- Gentner D. The mechanisms of analogical learning. In: Vosniadou S, Ortony A, editors. Similarity and analogical reasoning. London: Cambridge University Press; 1989. pp. 199–241. [Google Scholar]
- Gentner D, Stevens AL, editors. Mental models. Lawrence Erlbaum; 1983. [Google Scholar]
- Glymour C. The mind’s arrows: Bayes nets and graphical causal models in psychology. MIT Press; 2001. [Google Scholar]
- Green EG, Clémence A. Discovery of the faithfulness gene: A model of transmission and transformation of scientific information. British Journal of Social Psychology. 2008;47(3):497–517. doi: 10.1348/014466607X248912. [DOI] [PubMed] [Google Scholar]
- Hatano G, Inagaki K. Qualitative changes in intuitive biology. European Journal of Psychology of Education. 1997;12(2):111–130. [Google Scholar]
- Hejmadi A, Rozin P, Siegal M. Out of contact, always in contact: Contagious essence and conceptions of purification in American and Hindu Indian children. Developmental Psychology. 2004;40:467–476. doi: 10.1037/0012-1649.40.4.467. [DOI] [PubMed] [Google Scholar]
- Hmelo-Silver CE, Pfeffer MG. Comparing expert and novice understanding of a complex system from the perspective of structures, behaviors, and functions. Cognitive Science. 2004;1:127–138. [Google Scholar]
- Jee BD, Uttal DH, Gentner D, Manduca C, Shipley T, Sageman B, Ormand CJ, Tikoff B. Analogical thinking in geoscience education. Journal of Geoscience Education. 2010;58:2–13. [Google Scholar]
- Kelemen D. Why are rocks pointy? Children’s preference for teleological explanations of the natural world. Developmental Psychology. 1999;35(6):1440–1452. doi: 10.1037//0012-1649.35.6.1440. [DOI] [PubMed] [Google Scholar]
- Kelemen D, Rosset E. The human function compunction: Teleological explanation in adults. Cognition. 2009;111(1):138–143. doi: 10.1016/j.cognition.2009.01.001. [DOI] [PubMed] [Google Scholar]
- Lakshmi R, Gelman S. A Cross-Cultural Developmental Analysis of Children’s and Adults’ Understanding of Illness in South Asia (India) and the United States. Journal of Cognition and Culture. 2004;4(2):293–317. [Google Scholar]
- Legare CH, Gelman SA. Bewitchment, biology, or both: The co-existence of natural and supernatural explanatory frameworks across development. Cognitive Science. 2008;32:607–642. doi: 10.1080/03640210802066766. [DOI] [PubMed] [Google Scholar]
- Lynch E, Medin D. Explanatory models of illness: A study of within-culture variation. Cognitive Psychology. 2006;53(4):285–309. doi: 10.1016/j.cogpsych.2006.02.001. [DOI] [PubMed] [Google Scholar]
- Marchisio P, Baggi E, Bianchini S, Principi N, Esposito S. Clinical and socioeconomic impact of pediatric seasonal and pandemic influenza. Human Vaccines & Immunotherapeutics. 2012;8(1):17–20. doi: 10.4161/hv.8.1.18145. [DOI] [PubMed] [Google Scholar]
- Markman AB, Gentner D. Structure-mapping in the comparison process. American Journal of Psychology. 2000;113(4):501–538. [PubMed] [Google Scholar]
- Medin DL, Lynch EB, Coley JD, Atran S. Categorization and reasoning among tree experts: Do all roads lead to Rome? Cognitive Psychology. 1997;32:49–96. doi: 10.1006/cogp.1997.0645. [DOI] [PubMed] [Google Scholar]
- Oldstone MBA. Viruses, plagues and history. Oxford University Press. World of Viruses, University of Nebraska; 1998. [Google Scholar]
- Platts M. Doctors demand the removal of anti-vaccine ad from Times Square. The Guardian. 2011 Apr 18; Available at (accessed March 27, 2012): http://www.guardian.co.uk/science/blog/2011/apr/18/anti-vaccine-advertisementtimes-square.
- Roediger HL. Implicit memory: Retention without remembering. American Psychologist. 1990;45(9):1043. doi: 10.1037//0003-066x.45.9.1043. [DOI] [PubMed] [Google Scholar]
- Shtulman A, Valcarcel J. Scientific knowledge suppresses but does not supplant earlier intuitions. Cognition. 2012;124(2):209–215. doi: 10.1016/j.cognition.2012.04.005. [DOI] [PubMed] [Google Scholar]
- Sigelman CK. Age and Ethnic Differences in Cold Weather and Contagion Theories of Colds and Flu. Health Education & Behavior. 2012;39(1):67–76. doi: 10.1177/1090198111407187. [DOI] [PubMed] [Google Scholar]
- Singer SR, Nielsen NR, Schweingruber HA, editors. Discipline-Based Education Research: Understanding and Improving Learning in Undergraduate Science and Engineering. National Academies Press; 2012. [Google Scholar]
- Slotta JD, Chi MT. Helping students understand challenging topics in science through ontology training. Cognition and Instruction. 2006;24(2):261–289. [Google Scholar]
- Smith MJ, Ellenberg SS, Bell LM, Rubin DM. Media coverage of the measles–mumps–rubella vaccine and autism controversy and its relationship to MMR immunization rates in the United States. Pediatrics. 2008;121:836–843. doi: 10.1542/peds.2007-1760. [DOI] [PubMed] [Google Scholar]
- Stein NL, Hernandez MW, Anggoro FK. A theory of coherence and complex learning in the physical sciences: What works (and what doesn’t) In: Stein NL, Raudenbush S, editors. Developmental cognitive science goes to school. New York, NY: Routledge; 2010. pp. 87–112. [Google Scholar]
- Stohr K. Influenza?WHO cares. The Lancet Infectious Diseases. 2002;2(9):517–517. doi: 10.1016/S1473-3099(02)00366-3. [DOI] [PubMed] [Google Scholar]
- UNAIDS. Global report: UNAIDS report on the global AIDS epidemic 2010. Geneva, Switzerland: 2010. Retrieved from http://www.unaids.org/globalreport/documents/20101123_GlobalReport_full_en.pdf. [Google Scholar]
- Vosniadou S. Capturing and modeling the process of conceptual change. Learning and Instruction. 1994;4(1):45–69. [Google Scholar]
- Vosniadou S. Mental models in conceptual development. In: Magnani L, Nersessian N, editors. Model-Based Reasoning: Science, Technology, Values. New York: Kluwer Academic Press; 2002. pp. 353–368. [Google Scholar]
- Vosniadou S. International handbook of research on conceptual change. New York: Routledge; 2008. [Google Scholar]
- Vosniadou S, Brewer W. Mental models of the earth: A study of conceptual change in childhood. Cognitive Psychology. 1992;24:535–586. [Google Scholar]
- World Health Organization [WHO] Influenza (Seasonal): Fact Sheet #211. World Health Organization; 2009. Retrieved from http://www.who.int/mediacentre/factsheets/fs211. [Google Scholar]
- Zhu L, Liu G, Tardif T. Chinese children’s explanations for illness. International Journal of Behavioral Development. 2009;33:516–519. [Google Scholar]