

Abstract
As more and more dental practitioners are focusing on implant-supported fixed restorations, some clinicians favor the use of cement retained restorations while others consider screw-retained prosthesis to be the best choice. As both types of prostheses have certain advantages and disadvantages, clinicians should be aware of the limitations of each type. Screw-retained implant restorations have an advantage of predictable retention, retrievability and lack of potentially retained sub-gingival cement. However, a few disadvantages exist such as precise placement of the implant for optimal and esthetic location of the screw access hole and obtaining passive fit. On the other hand, cement retained restorations eliminates unaesthetic screw access holes; have passive fit of castings; reduce stress to splinted implants because of minor misfit of the framework; reduced complexity of lab procedures; enhanced esthetics; reduced cost factors and non disrupted morphology of the occlusal table. This case report presents the replacement of missing left central incisor using screw-retained implant prosthesis due to palatal trajectory of the implant placement and inadequate abutment height for retention of cement retained prosthesis.
Keywords: Dental implants, Implant prosthesis, Screw retained implant prosthesis, Cement retained implant prosthesis
Introduction
Generally, single missing tooth in the maxillary anterior region are best restored with cement retained implant restoration. The only reason to use screw retained prosthesis would be if the implant’s long axis is too palatal in the anterior region or extremely limited inter-occlusal space that limits the vertical wall heights of abutments to provide adequate retention. The other reason can be mal-aligned implants, in which axial wall reduction becomes so extreme that in attempting to achieve parallelism, individual abutment retention is lost [1–3]. In these situations, screw-retained crown or bridge may be an alternative to a cement retained restoration. The main advantage of screw-retained restoration is retrievability. When an abutment loosens or any repair of the restoration becomes necessary, the restoration may be destroyed during the removal procedure if the cement seal cannot be easily broken in case of cement retained restoration. Any force applied to a restoration on a loosened abutment has the potential to damage the internal threads of the implant [4–7]. It also removes any complications which may arise due to the cement left into the peri implant sulcus causing inflammation associated with radiographic evidence of bone loss [8–11]. Cleaning, screw replacement and assessment of surrounding tissue is easily possible without any damage of crown or implant in screw retained prosthesis. Only a radiographic examination is required to verify the precise fit of the prostheses to the implant before proceeding to the final torquing of the fastening screw. Screw-retained restorations can be used in situations when limited inter-arch space dictates an abutment that would be shorter than 5 mm. Also, implants that are not parallel may require further preparation and tapering of their abutments to enable an ideal path of insertion of the prosthesis which may lack adequate retention for the cement-retained restoration [12, 13].
Case Report
A 24 year old male patient reported to the Department of Advanced Courses, Manipal College of Dental Sciences, Manipal with a Chief complain of missing tooth in the upper front region. On examination it was observed that the tooth missing was a maxillary left central incisor with the residual ridge showing adequate horizontal bone width. However vertical bone height was slightly deficient. Patient was undergoing for orthodontic treatment for correction of mal-aligned teeth since 8 months (Fig. 1). Occlusion exhibited Class I molar and cuspid relationships bilaterally. The overjet was 2 mm however overbite was more than 3 mm. Periodontal health of the all other teeth were good. The patient was healthy with no known medical issues.
Fig. 1.
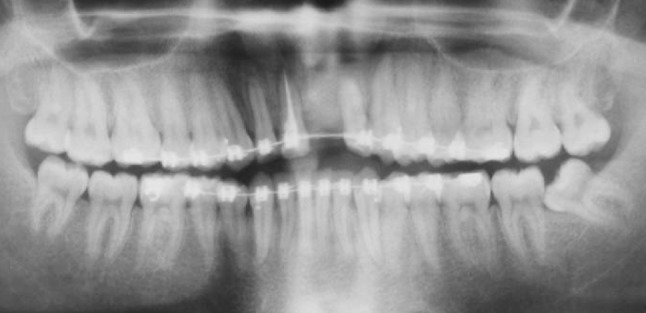
Pre-operative OPG showing orthodontic correction of mal-aligned teeth
Panoramic radiographic evaluation revealed sufficient bone for implant placement at missing maxillary left central incisor region. A regular platform NobelReplace™ Select implant fixture (Nobel Biocare™, Göteborg, Sweden) of 10 mm in length was selected.
Treatment Goals Were
To meet patient’s esthetic objectives in replacing the missing maxillary left central incisor.
Use interdisciplinary dentistry to complete an implant/crown restoration for maxillary central incisor without changing the surrounding periodontium to achieve maximum esthetics.
Establish a static occlusion after correction of mal-aligned teeth, which would allow the patient’s TMJs, muscles of mastication, and dentition to work harmoniously.
Orthodontic therapy was completed with correction of deep bite s well as sufficient space was maintained mesiodistally to allow the placement of implant at maxillary left central incisor region. After case acceptance, diagnostic casts were made and study models were mounted in the semi adjustable articulator. Diagnostic wax-up was done to visualize the contemplated final prosthodontic result.
The NobelReplace™ Select implant fixture (Nobel Biocare™, Göteborg, Sweden) size 4.3 × 10 mm was placed over the edentulous ridge of bone using a surgical guide, designed and fabricated according to the patient’s restorative needs. Standard protocol for implant placement was followed and it was tightened to 45 N cm, exhibiting excellent primary stability (Fig. 2). However implant was placed palatally due to slight bone deficiency at buccal cortical plate. Cover screw was placed and flap was sutured. A healing period of 4 months was allowed before restorative procedures were started.
Fig. 2.

Radiograph showing implant placement in region of 21
The patient returned 4 months after implant placement, and osseointegration was evaluated. The second stage surgery was performed and healing abutment was placed for 3 weeks to achieve healthy gingival biotype to enhance the emergence profile of the restoration (Fig. 3). The palatal trajectory of the implant placement resulted in severely limited space for prosthetic components, dictated a screw-retained prosthetic crown for this case. After 3 weeks, Nobel Biocare impression coping was placed on the implant and fixture level impression was made with polyether (Impregnum, 3M) impression material in a custom tray. A counter model with a bite registration was also taken to achieve occlusion. Color coded implant analog (Nobel Biocare) was attached to the impression coping (Nobel Biocare) and an implant cast was fabricated that incorporated a soft tissue gingival mask (Gingitech, Ivoclar Vivadent) with a type IV die stone (Kalrock). Abutment was fastened to the implant, at size corresponding to the implant diameter and tissue height. Plastic castable cylinder was incorporated into the wax pattern for the fabrication of porcelain-fused-to-metal framework. The framework was cast and tooth-colored porcelain was then applied to the framework to reproduce the teeth with appropriate selected shade (Fig. 4). Retaining screw was placed through the framework and threaded into the abutment. Proper abutment seating onto the implant fixture was verified radiographically before complete tightening (Fig. 5). The abutment screw was then tightened in graduations of force equal to 10, 20 N cm, and finally 30 N cm. Cotton pellet was placed over the screw head, and the access hole was sealed with composite resin. Crown was then checked for the esthetic appearance, and functional adaptability to the patient’s occlusal scheme (Fig. 6).
Fig. 3.

Healthy gingival biotype after removing healing abutment
Fig. 4.

Labial and palatal view of screw-retained implant prosthesis
Fig. 5.

Radiograph verifying the fit of prosthesis on implant
Fig. 6.

Intra oral view of screw-retained implant prosthesis
Discussion
A screw-retained implant prosthesis design was chosen for this case because of palatal placement of implant and shorter profile of the abutment due insufficient amount of available bone in the buccal region, which not only allowed for the reduced height of the metal framework in this area, but also necessitated screw fixation of the framework for adequate retention.
For screw retained implant-supported prostheses, it is important that screw should be torqued to 50–75 % of their yield strength to provide optimum clamping force. Fulcrums or pivot points are created at the edge where the abutment meets the head of the implant (Fig. 7). The torque that is applied to tighten the screw in screw-retained implant prosthesis is converted into tensile force (preload Fs × r). The upsetting masticatory Occlusal force (Fo), can be resolved into its component vertical (Fv) and horizontal forces (Fh). To maintain equilibrium, the resisting moment of the screw (Fs × r) must be greater than or equal to the sum of the moments created by the offset loading (Fv × L2 + Fh × L1). If there is an accurate fit between the head of the implant and abutment, a continuum of pivot points is created around the circumference. In this stable situation, vertical occlusal force will not stress the screw or cause screw loosening. However when inaccurate castings are screwed into implants, gaps are created and vertical loading over the implant head can compress the casting and cause screw loosening. In this situation, load is applied outside the pivot point (offset loading) that is of sufficient magnitude to overcome the clamping force of the screw [14–16].
Fig. 7.

Biomechanics of screw-retained prosthesis Tensile force on screw (Fs × r) must be > (Fv × L2 + Fh × L1)
Conclusion
A major benefit of a screw-retained prosthesis is retrievability. In addition, screw joint systems provide a great variety of transmucosal and prosthetic components, work well in patients with limited occlusal space, require no removal of subgingival cement, and cause no negative sequela when the cement is not removed. However, according to several studies screw-retained prosthesis requires precise positioning of the implant for optimal location of the screw access hole.
Contributor Information
Manawar Ahmad, Email: ahmad955mls@gmail.com.
B. Dhanasekar, Email: docdhana@hotmail.com
I. N. Aparna, Email: aparnaaniraghu@gmail.com
Hina Naim, Email: drhinaprostho@gmail.com.
References
- 1.Michalakis KX, Hirayama H, Garefis PD. Cement-retained versus screw retained implant restorations: a clinical review. Int J Oral Maxillofac Implants. 2003;18:719–728. [PubMed] [Google Scholar]
- 2.Hebel KS, Gajjar RC. Cement retained versus screw-retained implant restorations: achieving optimal occlusion and esthetics in implant dentistry. J Prosthet Dent. 1997;77:28–35. doi: 10.1016/S0022-3913(97)70203-8. [DOI] [PubMed] [Google Scholar]
- 3.Uludag B, Celik G. Fabrication of cement and screw retained multiunit implant restoration. J Oral Implantol. 2006;XXXII(Five):248–250. doi: 10.1563/811.1. [DOI] [PubMed] [Google Scholar]
- 4.Rajan M, Gunaseelan R. Fabrication of a cement and screw-retained implant prosthesis. J Prosthet Dent. 2004;92:578–580. doi: 10.1016/j.prosdent.2004.09.009. [DOI] [PubMed] [Google Scholar]
- 5.Valbao FP, Jr, Perez EG, Breda M. Alternative method for retention and removal of cement-retained implant prosthesis. J Prosthet Dent. 2001;86:181–183. doi: 10.1067/mpr.2001.115687. [DOI] [PubMed] [Google Scholar]
- 6.Doerr J. Simplified technique for retrieving implant restorations. J Prosthet Dent. 2002;88:352–353. doi: 10.1067/mpr.2002.128149. [DOI] [PubMed] [Google Scholar]
- 7.Okamoto M, Minagi S. Technique for removing a cemented superstructure from an implant abutment. J Prosthet Dent. 2002;87:241–242. doi: 10.1067/mpr.2002.119525. [DOI] [PubMed] [Google Scholar]
- 8.Pauletto N, Lahiffe BJ, Walton JN. Complications associated with excess cement around crowns on osseointegrated implants: a clinical report. Int J Oral Maxillofac Implants. 1999;14:865–868. [PubMed] [Google Scholar]
- 9.Weber HP, Kim DM, Ng MW, et al. Peri-implant soft-tissue health surrounding cement- and screw-retained implant restorations: a multi-center, 3 year prospective study. Clin Oral Implants Res. 2006;17:375–379. doi: 10.1111/j.1600-0501.2005.01232.x. [DOI] [PubMed] [Google Scholar]
- 10.Michalakis K, Pissiotis A, Hirayama H. Cement failure loads of 4 provisional luting agents used in cementation of implant-supported fixed partial dentures. Int J Oral Maxillofac Implants. 2000;15:545–549. [PubMed] [Google Scholar]
- 11.Squier R, Agar J, Duncan J, Taylor T. Retentiveness of dental cements used with metallic implant components. Int J Oral Maxillofac Implants. 2001;16:793–798. [PubMed] [Google Scholar]
- 12.Jorgensen KD. The relationship between retention and convergence angle in cemented veneer crowns. Acta Odontol Scand. 1955;13:35–40. doi: 10.3109/00016355509028171. [DOI] [PubMed] [Google Scholar]
- 13.Kaufman EG, Coelho DH, Collin L. Factors influencing the retention of cemented gold castings. J Prosthet Dent. 1961;11:487–498. doi: 10.1016/0022-3913(61)90232-3. [DOI] [Google Scholar]
- 14.Chee W, Felton DA, Johnson PF, Sullivan DY. Cemented versus screw retained prosthesis: Which is better? Int J Oral Maxillofac Implants. 1999;14:137–141. [PubMed] [Google Scholar]
- 15.Guichet DL, Caputo AA, Choi H, Sorensen JA. Load transfer in screw- and cement-retained implant fixed partial denture design. J Prosthet Dent. 1994;72:631. [PubMed] [Google Scholar]
- 16.Nissan J, Gross M, Shifman A, Assif D. Stress levels for well-fitting implant superstructures as a function of tightening force levels, tightening sequence, and different operators. J Prosthet Dent. 2001;86:20–23. doi: 10.1067/mpr.2001.115182. [DOI] [PubMed] [Google Scholar]