

Abstract
Background:
Oral health is an important component of general health and is associated with the development of a healthy personality. The malocclusion has been shown to affects oral health, leads to increased prevalence of dental caries and may result in temporo-mandibular joint disorders. Hence, the present study was conducted to evaluate the malocclusion in subjects reporting for orthodontic treatment among Saudi population in Asser region by using Dental Aesthetic Index (DAI).
Materials and Methods:
A cross-sectional survey was designed. A total of 162 study samples was participated in the study. A pre-designed proforma was used to evaluate various parameters determining malocclusion and DAI was used.
Results:
The mean age of 27.07 ± 9.76 years. The mean DAI score of the study participants was 27.27 ± 13.83. Maximum (75%) of the participants had Angle’s Class I molar relation followed by Angle’s Class II and II. Comparison of mean over jet and DAI score in the various age groups using one-way ANOVA there was a statistically significant difference in the mean DAI score between the participants in the various age groups.
Conclusion:
Knowing the prevalence of malocclusion in a community is of utmost importance, so that appropriate steps can be taken to prevent and treat the dentofacial irregularities.
Keywords: Dental Aesthetic Index, Kingdom of Saudi Arabia, malocclusion, prevalence
Introduction
Oral health is an important component of general health and is associated with the development of a healthy personality. In modern times, much focus is laid upon the development of orofacial disorders and treatment of the resulting malocclusions.1,2 The evaluation of different types of malocclusions existing within a population is important in order to plan orthodontic treatment and determine the resources required for the service.1,3 Measuring and recording the severity and prevalence of malocclusion are important as it can be used as an epidemiological tool for preventive procedures and evaluating the occlusal status of subjects in the community and establishing the treatment priority.1,4 It is essential to know the prevalence of malocclusion in any society, as it reveals the true extent of the problem and the general public can be educated, so that appropriate preventive and corrective measures can be instituted. Prevalence studies help the specialists in establishing proper preventive and treatment need in a given region.1
The malocclusion can be defined as an occlusion in which there is a mal-relationship between the arches in any of the planes or in which there are anomalies in tooth position beyond the normal limits.5,6 The malocclusion may lead to the individual feeling uncomfortable in social contacts, losing career opportunities and hence being embarrassed by their facial appearance.6,7 The etiology of malocclusion could be genetic or environmental and/or combination of both the factors along with various local factors such as adverse oral habits, tooth anomalies, form and developmental position of teeth.6,8 The malocclusion has been shown to affects oral health, leads to increased prevalence of dental caries and may result in temporo-mandibular joint disorders.5,6 The prevalence of malocclusion varies from country to country and among different age and sex group.6 In Saudi Arabia, governmental sectors provide free orthodontic treatment for Saudi citizens thereby leading to increased burden of work on these health care providers.9
The Dental Aesthetic Index (DAI) is an orthodontic index used on socially defined aesthetic norms has got regression equation that links the public’s perceptions of dental aesthetics with the objective physical measurements of the occlusal traits associated with malocclusion mathematically. The DAI has been found acceptable due to its simplicity, reproducibility and validity. It can be used as a practical tool for epidemiologists and other dental personnel for screening orthodontic treatment need.6,10-12
Hence, the present study was conducted to evaluate the malocclusion in subjects reporting for orthodontic treatment among Saudi populations in Asser region by using DAI.
Materials and Methods
A cross-sectional survey was designed. All study participants reporting to King Khalid University-College of Dentistry, Asser Central Hospital and Civil Hospital for orthodontic needs were recruited as study samples. A total of 162 study samples was participated in the study. Informed consent was obtained from all study participants, and ethical clearance was obtained from all the institutions.
A pre-designed proforma was used to evaluate malocclusion which consisted - demographic details, angles classification, overjet, overbite, cross bite (anterior and posterior), open bite, scissor bite, spacing, crowding, canine guidance, group guidance and DAI. Type-III clinical examination as recommended by American Dental Association (ADA) specification was followed. All three examiner involved in the study were calibrated, and inter examiner reliability was calculated using kappa statistics (κ = 0.94).
Statistical analysis
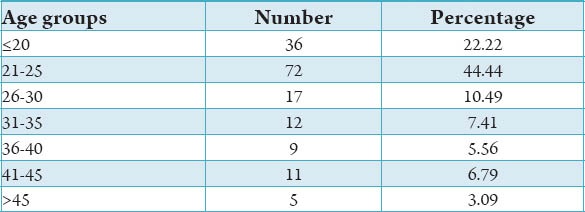
Data were entered in Excel 2010 and was analyzed using Statistical Package for Social Sciences 16.0. The frequency and percentage distribution of the study variables among the study participants was calculated (Graph 1). The association of the age with study variables was assessed using the Chi-square test. The mean overbite and DAI was tested using one-way analysis of variance (ANOVA) among the various age groups. P < 0.05 was considered to be statistically significant.
Graph 1.
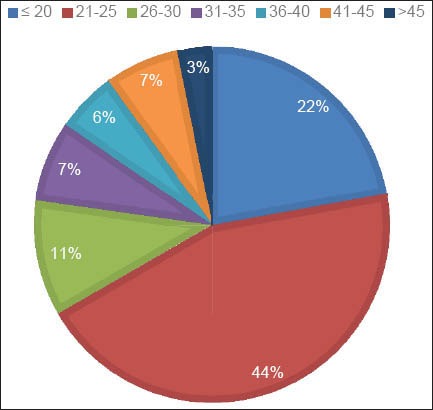
Age-wise distribution of the study population.
Results
A total of 162 participants was included in the study with a mean age of 27.07 ± 9.76 years. The mean DAI score of the study participants was 27.27 ± 13.83. Table 1 shows the distribution of the study variables among study participants. Maximum (75%) of the participants had Angle’s Class I molar relation followed by Angle’s Class II and III. Only 20% had anterior cross bite whereas 30.2% had posterior cross bite. Maximum participants had an overbite of 0-4 mm. Only 8% of participants had open bite whereas about 5% had scissor bite. Around 40% of the participants showed crowding in their dentition. Spacing in the dentition was found among 42% of the participants. Table 2 shows the association of the study parameters with age of the study participants using the Chi-square test. There was no statistically significant association found between age and any of the study parameters. Table 3 shows a comparison of mean over jet and DAI score in the various age groups using one-way ANOVA there was a statistically significant difference in the mean DAI score between the participants in the various age groups (P < 0.05) (Table 4 and Graph 2).
Table 1.
Distribution of the study variables within the study participants.
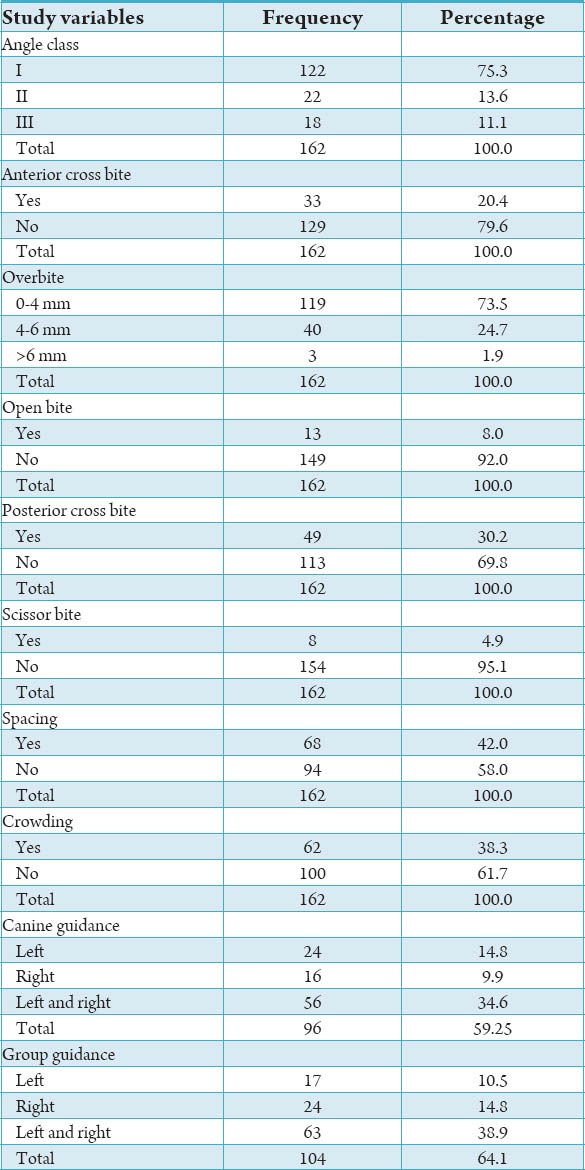
Table 2.
Association of study variables with age groups using Chi-square test.
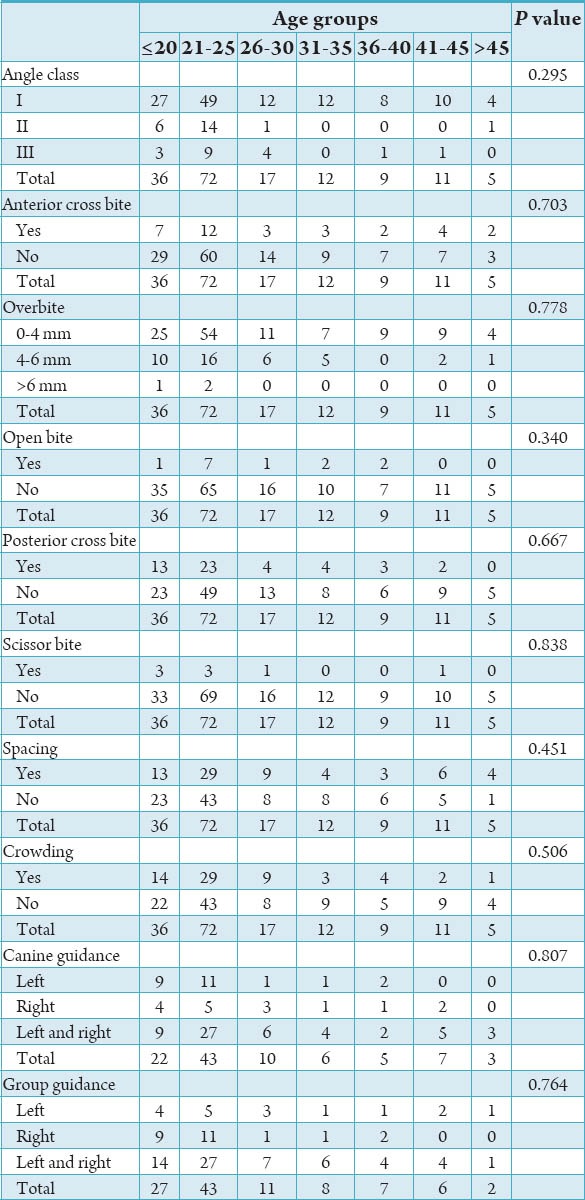
Table 3.
Comparison of mean over jet and DAI score in the various age groups using one-way ANOVA.
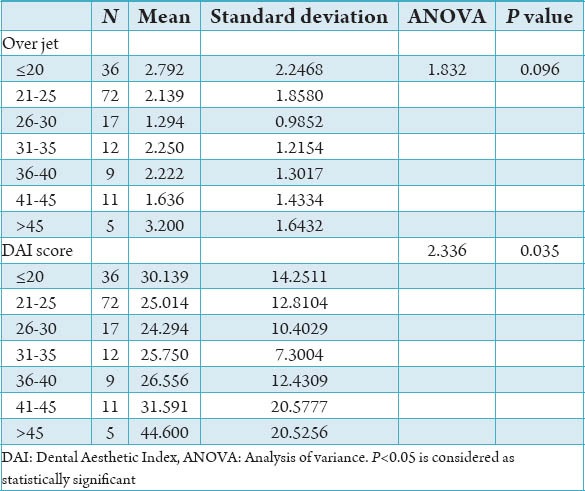
Table 4.
Age-wise distribution of the study participants.
Graph 2.
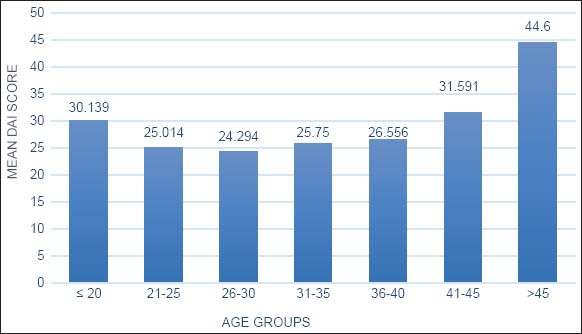
Mean Dental Aesthetic Index scores at various age groups.
Discussion
A large number of indices to assess malocclusion have been developed for the estimation of orthodontic treatment need in particular populations or communities, for patients who can be treated in a certain dental care system and to establish priorities when resources are limited. It is a controversial view as to which individual characteristics and occlusal features should be assessed in order to evaluate the orthodontic treatment need,13 however, the various malocclusion indices used in epidemiological studies of malocclusion in different countries have innumerable similarities and evaluation criteria. Such indices include the DAI (1986)14 and the Index of Orthodontic Treatment Need (1989).15 The DAI links the clinical and esthetic components mathematically in a regression equation to arrive at a single mark, which combines the physical and esthetic aspects of the occlusion using ten evaluation criteria. It is based on a social acceptability scale of occlusal conditions16 and has been used in many studies to determine orthodontic treatment need in different countries.17-22 A DAI scale that divided the continuous index score defined by the equation into four malocclusion severity levels was established and is readily usable and has been extensively used in orthodontic care programmes or malocclusion prevalence studies.12,23 It was included in the World Health Organization Oral Health Survey Methods (1997). The DAI is based on dental aesthetics, but is does not include functional considerations or potential risks to the dentition that could be functionally detrimental to the individual, but are not aesthetically significant.12,13,23
The majority of patients who attended for orthodontic treatment were of the younger age groups. These findings were similar to those of Al-Balkhi and Al-Zahrani.24 This is consistent with the fact that youngsters are highly concerned about their appearance even though the malocclusion may or may not affect their functional ability. A lower percent of adult patients attended the clinics that may be due to a lower rate of referral of adults for orthodontic care by clinicians as well as the fact that adults are more concerned by the functional rather than the aesthetic aspect of their dentition.
The frequency distribution of Angle’s types of malocclusion among the study samples was in close agreement with that reported by Al-Balkhi and Al-Zahrani,24 al-Emran et al.25 and Nashashibi et al.26 The Class I molar relationship type was the most frequently observed, followed by Class II and Class III and it was the most predominant feature of Saudi Arabian patients attending for orthodontic treatment. Almost half the patients attending for orthodontic treatment were found to have crowding or arch length insufficiency. The crowding was more commonly seen in the anterior arch segment than posterior, and this was in agreement with previous studies of the Saudi population.24-26 Nevertheless, the percentage of crowding in this study was higher. The dental spacing was similar to those reported by Al-Balkhi and Al-Zahrani,24 al-Emran et al.25 and Nashashibi et al.26
In Saudi Arabia, governmental sectors provide free orthodontic treatment for Saudi citizens thereby leading to increased burden of work on these health care providers.9 The planning orthodontic services and estimating the required resources and manpower requires meticulous evaluation of self-perceived and normative need for orthodontic treatment as well as other factors affecting these needs such as social, demographic, and psychosocial factors.24,27 Unnecessary referrals by general practitioners increase the burden on the healthcare system and lengthy waiting lists for orthodontic treatment can be eliminated by limiting free treatment to patients only with severe malocclusions that affect the patient’s function and aesthetics.28,29 It may also help to predict patients’ level of interest and motivation toward the orthodontic treatment, create awareness by planning educational programs in schools. It can also influence media to increase patient’s awareness and to overcome obstacles and barriers in seeking treatment.9,30
The limitations of the present study include a small sample size and lack of a comparison group. Further studies are recommended to include a larger sample size with various socio-demographic being taken into consideration as well as comparison studies with various populations across the world.
Conclusion
Knowing the prevalence of malocclusion in a community is of utmost importance so that appropriate steps can be taken to prevent and treat the dentofacial irregularities. Malocclusion is prevalent in Saudi Arabia and is a serious concern to the dental fraternity.
Footnotes
Source of Support: Nil
Conflict of Interest: None
References
- 1.Anita G, Kumar GA, Reddy V, Reddy TP, Rao MS, Wankhade SB. Dental Aesthetic Index of school students in Telangana region - An epidemiological study. J Int Oral Health. 2013;5(6):55–60. [PMC free article] [PubMed] [Google Scholar]
- 2.Das UM, Beena JP, Azher U. Oral health status of 6- and 12-year-old school going children in Bangalore city: An epidemiological study. J Indian Soc Pedod Prev Dent. 2009;27(1):6–8. doi: 10.4103/0970-4388.50809. [DOI] [PubMed] [Google Scholar]
- 3.Ajayi EO. Prevalence of malocclusion among school going children in Benin City, Nigeria: A peer-review. J Biomed Sci. 2008;7(1&2):5–11. [Google Scholar]
- 4.Uğur T, Ciğer S, Aksoy A, Telli A. An epidemiological survey using the Treatment Priority Index (TPI) Eur J Orthod. 1998;20(2):189–93. doi: 10.1093/ejo/20.2.189. [DOI] [PubMed] [Google Scholar]
- 5.Housten WJ. 4th ed. Oregon, USA: The Stonebridge Publishers; 2000. Walther's Orthodontic Notes. [Google Scholar]
- 6.Shivakumar KM, Chandu GN, Subba Reddy VV, Shafiulla MD. Prevalence of malocclusion and orthodontic treatment needs among middle and high school children of Davangere city, India by using Dental Aesthetic Index. J Indian Soc Pedod Prev Dent. 2009;27(4):211–8. doi: 10.4103/0970-4388.57655. [DOI] [PubMed] [Google Scholar]
- 7.Klages U, Bruckner A, Zentner A. Dental aesthetics, self-awareness, and oral health-related quality of life in young adults. Eur J Orthod. 2004;26(5):507–14. doi: 10.1093/ejo/26.5.507. [DOI] [PubMed] [Google Scholar]
- 8.Miitchell L, Carter NE, Doubleday B. 2nd ed. Oxford, UK: Oxford University Press; 2001. An Introduction to Orthodontics. [Google Scholar]
- 9.Hassan AH. Orthodontic treatment needs in the western region of Saudi Arabia: A research report. Head Face Med. 2006;2:2. doi: 10.1186/1746-160X-2-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cons NC, Jenny J, Kohout FJ, Songpaisan Y, Jotikastira D. Utility of the Dental Aesthetic Index in industrialized and developing countries. J Public Health Dent. 1989;49(3):163–6. doi: 10.1111/j.1752-7325.1989.tb02054.x. [DOI] [PubMed] [Google Scholar]
- 11.WHO. 4th ed. New Delhi: AITBS Publishers and Distributors®; 1999. WHO - Oral Health Survey, Basic Methods. [Google Scholar]
- 12.Jenny J, Cons NC. Establishing malocclusion severity levels on the Dental Aesthetic Index (DAI) scale. Aust Dent J. 1996;41(1):43–6. doi: 10.1111/j.1834-7819.1996.tb05654.x. [DOI] [PubMed] [Google Scholar]
- 13.Richmond S, O’Brien KD, Roberts CT, Andrews M. Dentists variation in the determination of orthodontic treatment need. Br J Orthod. 1994;21(1):65–8. doi: 10.1179/bjo.21.1.65. [DOI] [PubMed] [Google Scholar]
- 14.Cons NC, Jenny J, Kohout FJ. Iowa City, USA: College of Dentistry, University of Iowa, Iowa City; 1986. DAI: The Dental Aesthetic Index. [Google Scholar]
- 15.Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11(3):309–20. doi: 10.1093/oxfordjournals.ejo.a035999. [DOI] [PubMed] [Google Scholar]
- 16.Jenny J, Cons NC, Kohout FJ, Frazier PJ. Test of a method to determine socially acceptable occlusal conditions. Community Dent Oral Epidemiol. 1980;8(8):424–33. doi: 10.1111/j.1600-0528.1980.tb01322.x. [DOI] [PubMed] [Google Scholar]
- 17.Ansai T, Miyazaki H, Katoh Y, Yamashita Y, Takehara T, Jenny J, et al. Prevalence of malocclusion in high school students in Japan according to the Dental Aesthetic Index. Community Dent Oral Epidemiol. 1993;21(5):303–5. doi: 10.1111/j.1600-0528.1993.tb00779.x. [DOI] [PubMed] [Google Scholar]
- 18.Baca-Garcia A, Bravo M, Baca P, Baca A, Junco P. Malocclusions and orthodontic treatment needs in a group of Spanish adolescents using the Dental Aesthetic Index. Int Dent J. 2004;54(3):138–42. doi: 10.1111/j.1875-595x.2004.tb00269.x. [DOI] [PubMed] [Google Scholar]
- 19.Bernabé E, Flores-Mir C. Orthodontic treatment need in Peruvian young adults evaluated through Dental Aesthetic Index. Angle Orthod. 2006;76(3):417–21. doi: 10.1043/0003-3219(2006)076[0417:OTNIPY]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 20.Esa R, Razak IA, Allister JH. Epidemiology of malocclusion and orthodontic treatment need of 12-13-year-old Malaysian schoolchildren. Community Dent Health. 2001;18(1):31–6. [PubMed] [Google Scholar]
- 21.Estioko LJ, Wright FA, Morgan MV. Orthodontic treatment need of secondary schoolchildren in Heidelberg, Victoria: An epidemiologic study using the Dental Aesthetic Index. Community Dent Health. 1994;11(3):147–51. [PubMed] [Google Scholar]
- 22.Otuyemi OD, Ogunyinka A, Dosumu O, Cons NC, Jenny J, Kohout FJ, et al. Perceptions of dental aesthetics in the United States and Nigeria. Community Dent Oral Epidemiol. 1998;26(6):418–20. doi: 10.1111/j.1600-0528.1998.tb01981.x. [DOI] [PubMed] [Google Scholar]
- 23.Manzanera D, Montiel-Company JM, Almerich-Silla JM, Gandía JL. Diagnostic agreement in the assessment of orthodontic treatment need using the Dental Aesthetic Index and the Index of Orthodontic Treatment Need. Eur J Orthod. 2010;32(2):193–8. doi: 10.1093/ejo/cjp084. [DOI] [PubMed] [Google Scholar]
- 24.Al-Balkhi K, Al-Zahrani A. Saudi Dent J. 3. Vol. 6. Riyadh: King Saud University; 1994. The pattern of malocclusions in Saudi Arabian patients attending for orthodontic treatment at the college of dentistry; pp. 138–44. [Google Scholar]
- 25.al-Emran S, Wisth PJ, Böe OE. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18(5):253–5. doi: 10.1111/j.1600-0528.1990.tb00070.x. [DOI] [PubMed] [Google Scholar]
- 26.Nashashibi I, Darwish SK, El Khalifa R. Prevalence of malocclusion and treatment needs in Riyadh (Saudi Arabia) Odontostomatol Trop. 1983;6(4):209–14. [PubMed] [Google Scholar]
- 27.Jones WB. Malocclusion and facial types in a group of Saudi Arabian patients referred for orthodontic treatment: A preliminary study. Br J Orthod. 1987;14(3):143–6. doi: 10.1179/bjo.14.3.143. [DOI] [PubMed] [Google Scholar]
- 28.Burden DJ, Pine CM. Self-perception of malocclusion among adolescents. Community Dent Health. 1995;12(2):89–92. [PubMed] [Google Scholar]
- 29.Chew MT, Aw AK. Appropriateness of orthodontic referrals: Self-perceived and normative treatment needs of patients referred for orthodontic consultation. Community Dent Oral Epidemiol. 2002;30(6):449–54. doi: 10.1034/j.1600-0528.2002.00017.x. [DOI] [PubMed] [Google Scholar]
- 30.Grzywacz I. The value of the aesthetic component of the Index of Orthodontic Treatment Need in the assessment of subjective orthodontic treatment need. Eur J Orthod. 2003;25(1):57–63. doi: 10.1093/ejo/25.1.57. [DOI] [PubMed] [Google Scholar]