

Abstract
Background:
Intelligence is the property of mind that encompasses many related abilities, such as the capacities to reason, plan, solve the problem, think, comprehend ideas, use languages and to learn. Intellectual level of a person influence the abilities to learn from experience, adapt to new situations, understand and handle abstract concepts, and use knowledge to manipulate one’s environment. This abstract thinking helps the child to maintain his/her oral hygiene in a better way.
Materials and Methods:
The present study was carried out on 252 children of 10-15 years old, reported to the out-patient Department of Pedodontics and Preventive Dentistry; of Teerthanker Mahaveer Dental College and Research Centre; Moradabad, in order to assess the relation between IQ of a child with dental caries and gingival disease. The statistical analysis was performed using Statistical Package for Social Sciences Version 15.0 statistical analysis software.
Results:
Statistically, there was a significant difference among different intelligence groups and the prevalence of moderate gingivitis (P < 0.001). Prevalence of caries was maximum among those with borderline intelligence (90.9%), and no significant association between level of intelligence and caries prevalence was observed (P = 0.572).
Conclusion:
There was a statistical significant relation between IQ and prevalence of moderate gingivitis and no significant relationship was observed between IQ and dental caries.
Keywords: Dental caries, gingival diseases, Wechsler intelligence scale
Introduction
Each child has unique traits of intelligence, which can be measured as intelligence quotient (IQ). Wechsler defined intelligence as “an individual’s ability to adapt and constructively solve problems in the environment.”1 Whereas, IQ is defined as the “Relative intelligence of an individual expressed as a score on a standardized test of intelligence.”2 Intellectual level of a person influence the abilities to learn from experience, adapt to new situations, understand and handle abstract concepts, and use knowledge to manipulate one’s environment.
Despite great improvements in the oral health of populations in several countries, global problems still persist. Oral diseases such as dental caries, periodontal disease, are one of the major public health problems. A bio-psychosocial model of disease is highly relevant to dentistry since most oral health problems can be prevented or controlled through preventive behaviours. Recent work illustrates the potential contribution of psychosocial factors in understanding the disease process, as well as improving caries risk prediction.3 The number of studies conducted to find the relationship of dental caries with different IQ showed conflicting results.4,5 A direct proportional relation was observed with IQ and dental caries. A study carried out in an orphanage showed a higher caries scores in average IQ subjects and an increase in IQ showed increase in caries scores.6
Intelligence can be expected to have a significant impact on children’s understanding of causes and consequences, information and instructions. It may also influence their ability to communicate feelings or distress and to behave adequately in the dental situation.7 Attention problems have been associated with refusal of dental treatment in children. Children with low IQ need significantly longer time to accept the dental treatment situation. Intelligence was found to be more strongly associated with children’s dental anxiety.8 High IQ may be more effective than a low IQ in moderating the level of cooperation during dental treatment of children.
In a country like India, the children are undergoing a multitude of experiences, and various influences are affecting them. Therefore, the developing needs and their basic interests are to be studied carefully. A proper psychological testing can only enable any sincere and effective steps in the development of any plans and strategies for children. Moreover, it is also important to know how young people with dental caries and gingivitis feel about themselves, which is integral to the development of a positive child-clinician relationship.
Nowadays, researches point out the need to consider the functional and psychosocial dimensions of oral health for the implementation and evaluation of public health dentistry interventions.9
However, yet there is a paucity of data relating IQ with dental caries and none in relation to gingival diseases in children. Hence, this study was undertaken to interrelate IQ with that of dental caries and gingivitis in children.
Materials and Methods
The present study was carried out on 252 children (126 male and 126 female) of 10-15 years of age, from the Department of Pedodontics and Preventive Dentistry; Teerthanker Mahaveer Dental College and Research Centre; Moradabad. All the children selected were with the following criteria:
Inclusion criteria
All the subject selected were medically fit, healthy and free of any systemic diseases (American Society of Anesthesiologists-I).
Children selected were of same socio-economic status and geographical distribution.
All selected children were on a vegetarian diet.
Children selected were free from any development disorder related to psychiatric illness.
All children were living with their respective family members.
Exclusion criteria
Children with any systemic disease or any kind of allergy or with any history of antibiotic consumption in the recent past.
Children with local factors that might affect gingival condition like lip incompetence, mouth breathing, orthodontic appliance, cleft lip or palate.
Children with the disorder like attention deficit hyperactivity disorder, obsessive-compulsive disorder, hyperkinetic child, etc.
Children with defective audio, speech or visual acuity.
Assessment of IQ was done with the help of Malin’s Intelligence Scale for Indian Children (Malin, 1969). This is an Indian adaptation of the well know Wechsler’s Intelligence Scale for Children (Wechsler, 1949). This test embraces all the advantages of the original scale along with several improvements and is the individual intelligence scale for children from 6 to 15 years. The advantage of Malin’s test is that both Hindi and English version of questionnaires are available, which have been standardized by Malin himself. This scale is used to assess both verbal and performance IQ of the children. Only four verbal tests (Information, Comprehension, Arithmetic and Similarities) and four performance IQ tests (Picture Completion, Block Design, Object Assembly, and Mazes) have been used for the purpose of the present study. The raw score was converted into the test quotient of each sub-test. Full scale IQ was obtained by adding both verbal and performance test result and dividing for the average.10
Recording of dental caries was done with the help of decayed missing filled (DMF)/dmf Index. DMF index introduced by Henry Klein, Carrole, Palmer and Knutson in 1938 all the permanent teeth are examined with the help of the mouth mirror, explorer and an airway syringe. DMF index this was described by Gruebbel in 1944, as an equivalent index to DMF index, for measuring dental caries in the primary dentition.11 Recording of gingival disease was done with the help of gingival index given by Loe and Sillness (1963). This index helps to assess the severity of gingivitis and its location in four possible areas.11
The statistical tools employed in the study are Chi-square test and Pearson’s coefficient of correlation.
Standardization of investigator
The investigator first received training in proper administration, scoring and interpretation of the above mentioned intelligence tests from a psychologist. After receiving the training, the investigator was calibrated for assessment of IQ by repeated sessions.
Results
A total of 252 children (126 males and 126 females) fulfilling the inclusion criteria and not falling into the domain of exclusion criteria were enrolled in the study. Gender wise distribution of children has been shown in Table 1. Age of children ranged from 10 to 15 years. Mean age of males was 12.31 ± 1.29 years, whereas that of females was 11.91 ± 1.30 years. Statistically, the difference between two genders was significant (P = 0.016).
Table 1.
Mean age and gender wise distribution of children.

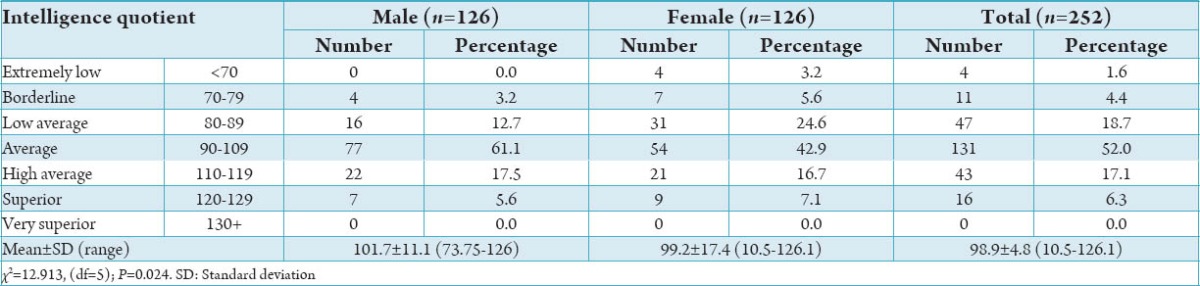
Majority of children had average IQ scores (52.0%), followed by those having low average scores (18.7%), high average scores (17.1%), superior (6.3%), borderline (4.4%) and extremely low (1.2%). None of the children had very superior IQ scores (0%). Overall mean IQ score was 98.9 ± 14.8 (range 10.5-126.1) (Table 2 and Graph 1).
Table 2.
Distribution of children according to their intelligence quotient.
Graph 1.
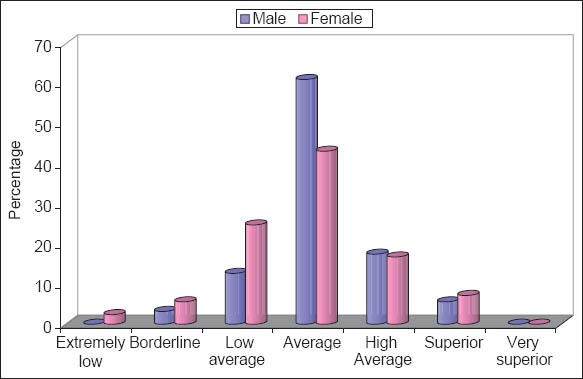
Distribution of children according to their intelligence quotient.
Majority of boys (61.1%) had average IQ scores, followed by those having high average (17.5%), low average (12.7%), superior (5.6%) and borderline scores (3.2%). None of the boys had extremely low or very superior scores (0%). Mean IQ score of boys was 101.7 ± 11.1 (range 73.75-126).
However, among girls, maximum had average (42.9%) IQ scores followed by those having low average (24.6%), high average (16.7%), superior (7.1%), borderline (5.6%) and extremely low (3.2%) IQ scores. None of the girls had very superior IQ scores. Mean IQ score of girls was 99.2 ± 17.4 (range 10.5-126.1). On comparing the data statistically, a significant difference in mean IQ scores of two genders was observed (P = 0.014). Majority of children had mild gingivitis (n = 151; 59.9%), followed by those having moderate gingivitis (n = 101; 40.1%). None of the children had severe gingivitis (n = 0; 0%). Mean Loe and Silness Index was 0.90 ± 0.36 (range 0.10-1.91) (Table 3 and Graph 2).
Table 3.
Distribution of children according to Loe and Silness Index.

Graph 2.
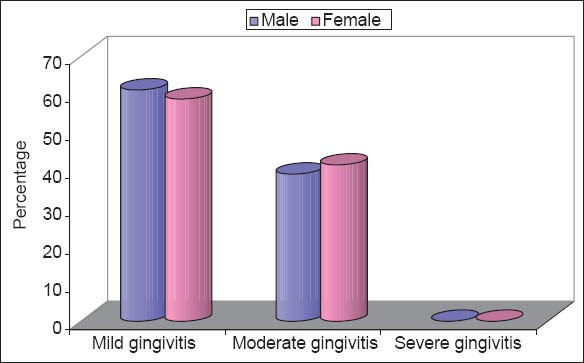
Distribution of children according to Loe and Silness Index.
Among boys, a total of 77 (61.1%) had mild gingivitis and remaining 49 (38.9%) had moderate gingivitis. Mean Loe and Silness Index of boys was 0.88 ± 0.36 (range 0.10-1.91), while among girls 74 (58.7%) had mild gingivitis and remaining 52 (41.3%) had moderate gingivitis. Mean Loe and Silness Index of girls was 0.91 ± 0.35 (range 0.21-1.90). Statistically, there was no significant difference in gingival disease status of two genders (P = 0.700).
More than two-third patients (n = 172; 68.3%) had dental caries. Remaining 80 (31.7%) patients had their teeth intact. Overall mean Decayed missing filled tooth (DMFT) score was 1.61 ± 1.64 (Table 4 and Graph 3). Among boys, prevalence of caries was 70.6%, while among girls this prevalence was 65.9%. Mean DMFT of boys was 1.58 ± 1.52, whereas the same among girls was 1.64 ± 1.75. Table 5 and Graph 4 shows prevalence of caries was maximum among those with borderline intelligence (90.9%) and minimum among those with extremely low intelligence (50%). Statistically, no significant association between level of intelligence and caries prevalence was observed (P = 0.572).
Table 4.
Distribution of children according to caries status.

Graph 3.
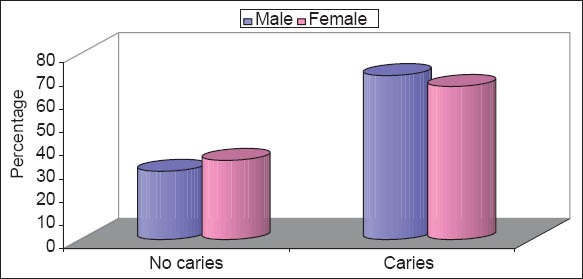
Distribution of children according to caries status.
Table 5.
Association of dental caries with intelligence.

Graph 4.
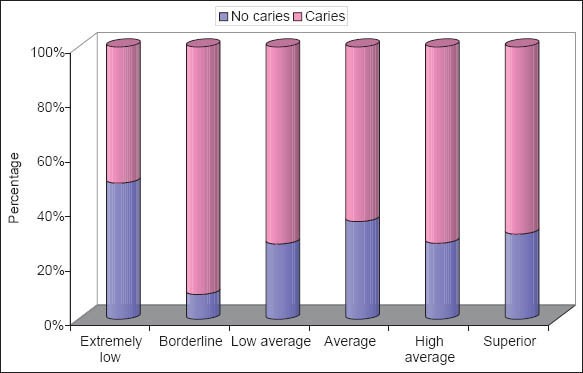
Association of dental caries with intelligence.
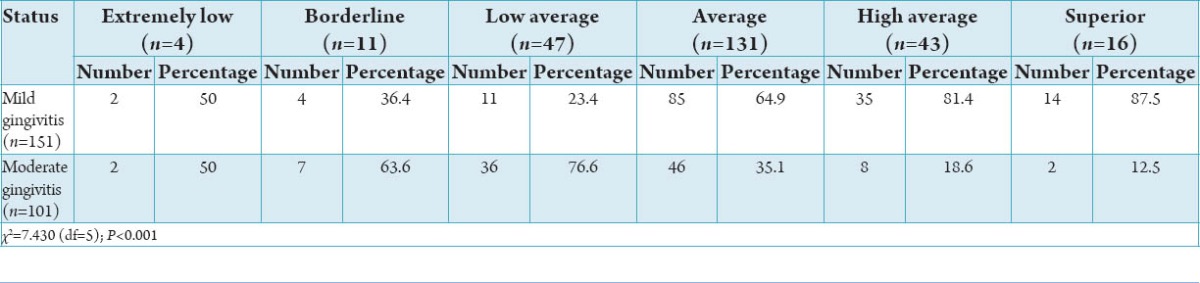
When compared to those with extremely low, borderline and low average intelligence status, prevalence of moderate gingivitis was lower among those with average, high average and superior intelligence. Statistically, there was a significant difference among different intelligence groups and the prevalence of moderate gingivitis (P < 0.001). (Graph 5).
Graph 5.
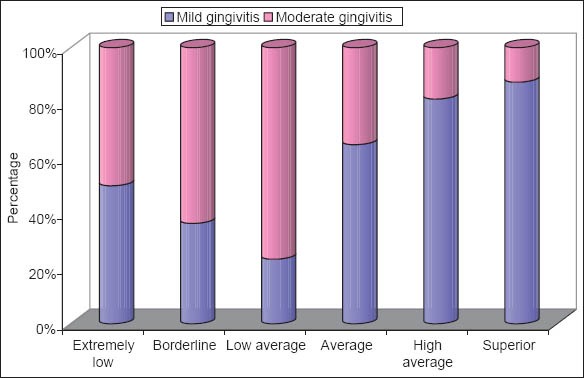
Association of gingivitis with intelligence.
Discussion
Dental caries and periodontal diseases are two major oral health concerns worldwide both diseases are of multifactorial in origin and abundance of research has been dedicated to know the etiological factors of these diseases. Many studies have tried to assess the relation between socio-behavioral factors and dental caries and few studies relating to periodontal diseases.12 Psychology plays an important role in determining a person’s behavior, but not many studies have been conducted in this regard. Psychology can be categorized under one or the other headings of intelligence, personality, temperament, maturity, curiosity, liking, study habits, adjustment functions, anxiety, developmental screening, creativity and others like frustration, general learning abilities, psychopathology, deprivation and helplessness.13
Hence, this cross-sectional comparative study was done among 252 children (126 males and 126 females) of 10-15 years old children, in order to assess the relation between IQ of a child with that of dental caries and gingival disease. There are only few studies relating dental caries with IQ. Whereas, no studies have been reported on gingivitis, and intelligence therefore comparisons could not be done. However, studies done in the past are varying in terms of mentally disabled children as samples, with different study criterion and different scales.
The mean age of subjects in the present study was 12.11 ± 1.3 years with an equal number of boys and girls.
In the present study, prevalence of IQ was noted as 4% of subjects were in extremely low level of IQ and all of them were girls. Highest number of subjects were in the average level (52%), followed by low average (18.7%), high average (17.1%), superior (6.3%) and borderline (4.4%) level of IQ. However, a high IQ levels were observed in studies conducted by Shankar et al. in 1983 (117.5 ± 19.4),14 and Bruckner and Hill in 1952 (121.6 ± 14.7)4 in normal children. Whereas, Virk et al.6 showed a lower score of IQ (88.75 ± 8.41) in socially handicapped orphan children. Intelligence is of great practical and social importance, and that genetics plays a bigger role than does environment in creating IQ differences among individuals.15 Some studies showed a correlation between dental fluorosis and intellectual ability.16,17 Children with probable developmental coordination disorder had an increased risk of mental health difficulties that, in part, were mediated through associated developmental difficulties, low verbal IQ, poor self-esteem, and bullying.18 IQ is a standardized measure of human intellectual capacity that takes into account a wide range of cognitive skills.19 And these skills are essential for the maintenance of oral hygiene, to become co-operative during treatments, being attentive to communication, respond and follow the counseling procedures (Table 6).
Table 6.
Association of gingivitis with intelligence.
In the present study, boys (101.7 ± 11.1) had a higher IQ score when compared with girls (99.2 ± 17.4), but both in average IQ level. When compared a significant difference was obtained. Since many of the more prestigious roles in society are associated with high IQ and the cultural background and role of women as home makers in our society restricts it later for them shifting their focus and attention.20 This let us know the compliance of girls being higher and behavior modification required is less.
In the present study, caries was more among borderline IQ cases when compared with others and was found to be non-significant (P = 0.572), then the level of caries decrease in the low average and average group further increasing in high average group, followed by again decrease in superior level of IQ. However, Shankar et al. showed a different relation that with increase in IQ there was an increase in dental caries.14 Our study results were similar to that of Bruckner and Hill in normal children4 and Virk et al. in orphan children.6 Steinberg and Zimmermann stated that institutionalized subnormal person with a lower IQ (20-49) had significantly lower caries score than the group of subjects with a higher IQ (≥50) and when graphed from lowest IQ to highest IQ, the caries score formed a bell-shaped curve with persons of an average IQ having the highest caries score.5 The present study results may be due to lack of cognitive skills, which are low in borderline intellectual levels, leading to non-compliance with oral hygiene maintenance and abnormal dietary habits. Various studies have been reported on people with low IQ levels and poor oral health status.21,22
In the present study, highest prevalence of mild gingivitis was obtained in superior group and least in low average group. Whereas, moderate gingivitis was seen more among the borderline, low average and extremely low IQ level children. There were no studies found in literature for comparison of our results. The above results of moderate gingivitis may be attributed to poor oral hygiene seen among the subjects having low IQ levels.23,24 However, presence of high prevalence of mild gingivitis in the higher IQ levels may be attributed to the subjects of our study coming from low socio-economic background with lack of access to oral hygiene materials and lack of knowledge-related to oral hygiene maintenance. Few studies have reported a high prevalence of gingivitis among low IQ mentally disabled children.25,26
The findings from this study should also be interpreted in light of some limitations. First, the sample addressed only to Moradabad on the purposive sampling basis; therefore, the results may not be generalized to larger population. Second, the non-equivalent group design used in the present study does not allow us to relate the different psychological variables and oral diseases in the study. Hence, further studies with larger sample size, with two or more groups, with other psychological domains on oral health status, with multi-centric studies should be conducted to have a clear picture of the influence of IQ on dental caries and gingivitis. This study can help in determining the cognitive behavior and perceptions of child with dental caries and gingival diseases. In turn, this will help the clinician to prioritize the needy part during the counseling process and alter the level of communication. The behavior management of patient can be delineated by understanding that domains of personality are to be managed.
Conclusion
The present study was conducted to explore the relation between IQ with dental and gingival status. Statistically, there was a significant difference among different intelligence groups and the prevalence of moderate gingivitis (P < 0.001). Prevalence of caries was maximum among those with borderline intelligence (90.9%) and no significant association between level of intelligence and caries prevalence was observed (P = 0.572). 68.3% had dental caries with overall mean DMFT score of 1.61 ± 1.64. Majority of children had mild gingivitis (n = 151; 59.9%) followed by those having moderate gingivitis (n = 101; 40.1%). Majority of children had average IQ scores (52.0%). The above study results can be utilized keeping in mind that positive construction of self is critical in the development of health enhancing behaviors and children are more likely to engage in health-enhancing behaviors if they have high levels of the above affective and cognitive skills. Children’s oral health promotion, and oral health programmed should incorporate IQ testing-approaches to promote better oral health and better child-clinician relationship.
Footnotes
Source of Support: Nil
Conflict of Interest: None
References
- 1.The Welchsler Intelligence Scales. [Last accessed on 2013 Mar 23]. Available from: http://www.iupui.edu/~flip/wechsler.html .
- 2.Definition from: Psychological Index Terms via Unified Medical Language System at the National Library of Medicine. [Last accessed on 2014 Aug 4]. Available from: http://ghr.nlm.nih.gov/glossary=intelligencequotient .
- 3.Reisine S, Litt M, Tinanoff N. A biopsychosocial model to predict caries in preschool children. Pediatr Dent. 1994;16(6):413–8. [PubMed] [Google Scholar]
- 4.Bruckner RJ, Hill TJ. Intelligence quotient and dental caries experience. J Dent Child. 1952;19:64–8. [Google Scholar]
- 5.Steinberg AD, Zimmerman S. The Lincoln dental caries study. I. The incidence of dental caries in persons with various mental disorders. J Am Dent Assoc. 1967;74(5):1002–7. doi: 10.14219/jada.archive.1967.0177. [DOI] [PubMed] [Google Scholar]
- 6.Virk P, Jain RL, Pathak A, Sharma U, Rajput JS. Inter-relationship of intelligence-quotient and self-concept with dental caries amongst socially handicapped orphan children. J Indian Soc Pedod Prev Dent. 2012;30(2):127–32. doi: 10.4103/0970-4388.99986. [DOI] [PubMed] [Google Scholar]
- 7.Rud B, Kisling E. The influence of mental development on children's acceptance of dental treatment. Scand J Dent Res. 1973;81(5):343–52. doi: 10.1111/j.1600-0722.1973.tb00337.x. [DOI] [PubMed] [Google Scholar]
- 8.Arnrup K, Broberg AG, Berggren U, Bodin L. Lack of cooperation in pediatric dentistry – The role of child personality characteristics. Pediatr Dent. 2002;24(2):119–28. [PubMed] [Google Scholar]
- 9.Paula JS, Leite IC, Almeida AB, Ambrosano GM, Pereira AC, Mialhe FL. The influence of oral health conditions, socioeconomic status and home environment factors on schoolchildren's self-perception of quality of life. Health Qual Life Outcomes. 2012;10:6. doi: 10.1186/1477-7525-10-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Malin AJ. Lucknow: Indian Psychological Corporation; 1969. Malin's Intelligence Scale for Indian Children (MISIC) Manual. [Google Scholar]
- 11.Peter S. 3rd ed. New Delhi: Arya Publishing House; 2006. Essential of Preventive and Community Dentistry; pp. 148–9. (177-85). [Google Scholar]
- 12. [Last accessed on 2013 Dec 10]. Available from: http://www.who.int/bulletin/volumes/83/9/petersen0905abstract/en/
- 13.Satpathy M. Psychological tests developed for children in India: A review of recent trends in research, practice and application. In: Shyam R, Khan A, editors. Clinical Child Psychology. 1st ed. New Delhi: Kalpaz Publication; 2009. pp. 275–92. [Google Scholar]
- 14.Shanker B, Tewari A, Jain RL, Verma SK. A study of prevalence and severity of dental caries in children of different intelligence quotient levels. J Indian Dent Assoc. 1983;55(10):413–7. [PubMed] [Google Scholar]
- 15.Furnham A. Thinking about intelligence. Psychologist. 2000;13(10):510–4. [Google Scholar]
- 16.Ding Y, YanhuiGao, Sun H, Han H, Wang W, Ji X, et al. The relationships between low levels of urine fluoride on children's intelligence, dental fluorosis in endemic fluorosis areas in Hulunbuir, Inner Mongolia, China. J Hazard Mater. 2011;186(2-3):1942–6. doi: 10.1016/j.jhazmat.2010.12.097. [DOI] [PubMed] [Google Scholar]
- 17.Shivaprakash PK, Ohri K, Noorani H. Relation between dental fluorosis and intelligence quotient in school children of Bagalkot district. J Indian Soc Pedod Prev Dent. 2011;29(2):117–20. doi: 10.4103/0970-4388.84683. [DOI] [PubMed] [Google Scholar]
- 18.Lingam R, Jongmans MJ, Ellis M, Hunt LP, Golding J, Emond A. Mental health difficulties in children with developmental coordination disorder. Pediatrics. 2012;129(4):e882–91. doi: 10.1542/peds.2011-1556. [DOI] [PubMed] [Google Scholar]
- 19.Ramsden S, Richardson FM, Josse G, Thomas MS, Ellis C, Shakeshaft C, et al. Verbal and non-verbal intelligence changes in the teenage brain. Nature. 2011;479(7371):113–6. doi: 10.1038/nature10514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jensen AR, Reynolds CR. Sex differences on the WISC-R. Pers Individ Dif. 1983;4(2):223–6. [Google Scholar]
- 21.Jain M, Mathur A, Sawla L, Choudhary G, Kabra K, Duraiswamy P, et al. Oral health status of mentally disabled subjects in India. J Oral Sci. 2009;51(3):333–40. doi: 10.2334/josnusd.51.333. [DOI] [PubMed] [Google Scholar]
- 22.Ulseth JO, Hestnes A, Stovner LJ, Storhaug K. Dental caries and periodontitis in persons with Down syndrome. Spec Care Dentist. 1991;11(2):71–3. doi: 10.1111/j.1754-4505.1991.tb00819.x. [DOI] [PubMed] [Google Scholar]
- 23.Palin T, Hausen H, Alvesalo L, Heinonen OP. Dental health of 9--10-year-old mentally retarded children in eastern Finland. Community Dent Oral Epidemiol. 1982;10(2):86–90. doi: 10.1111/j.1600-0528.1982.tb00369.x. [DOI] [PubMed] [Google Scholar]
- 24.Butts JE. Dental status of mentally retarded children. II. A survey of the prevalence of certain dental conditions in mentally retarded children of Georgia. J Public Health Dent. 1967;27(4):195–211. doi: 10.1111/j.1752-7325.1967.tb03914.x. [DOI] [PubMed] [Google Scholar]
- 25.Denloye OO. Periodontal status and treatment needs of 12-15 year old institutionalized mentally handicapped school children in Ibadan, Nigeria. Odontostomatol Trop. 1999;22(86):38–40. [PubMed] [Google Scholar]
- 26.Vigild M. Periodontal conditions in mentally retarded children. Community Dent Oral Epidemiol. 1985;13(3):180–2. doi: 10.1111/j.1600-0528.1985.tb00440.x. [DOI] [PubMed] [Google Scholar]