

Abstract
Background:
The objectives of this study were to assess the total antioxidant levels, dental development, and oral health status in childhood obesity.
Materials and Methods:
A total of 120 children aged 6-12 years consisting of both genders from different school along Coastal Karnataka, India were part of the study and were categorized into obese/overweight, and normal children based on body mass index for age and sex. Total antioxidant capacity (TAC) levels determined by phosphomolybidic acid and spectrophotometric method were considered. Oral hygiene index-simplified, modified gingival index and dentition status index were used to analyze oral health status. Dental development was assessed using a clinical method and correlated with standard chronology of human dentition.
Results:
Levels of the total salivary antioxidants were increased in the study group which is very highly significant when compared with control group, oral health status in both the study group and control group was good. Number of children in study group showing accelerated dental development is relatively less when compared with control group, but is not statistically significant.
Conclusion:
Salivary TAC was significantly high in overweight and obese children than their normal counterparts. Prevalence of dental caries was high in obese/overweight children when compared to normal children.
Keywords: Body mass index, childhood obesity, oral health status
Introduction
Obesity has been defined as the excess fat deposition due to a chronic positive shift of the energy equation resulting from an increase in energy input, decrease in energy output or both.1
Obesity is chronic disease with global epidemic spread2 the prevalence of overweight and obesity in children is rapidly increasing in many countries around the world including India. The World Health Organization has compared this marked change in body weight to “Global epidemic disease.”3
According to WHO at least 50% of adults and 20% of children in U.K. and U.S.A. are currently overweight. Prevalence of overweight amongst Australian children has increased from 11% in 1985 to 20% in 1995. Childhood obesity has tripled in Canada in last 20 years. In a recent study, even in India more than 20-28% of adult males and 40-47% of adult females in urban Delhi were overweight and about 15-30% of children in urban areas were overweight by WHO standards.4
India’s economy growing at gross domestic product of 8% and part of emerging markets in the world along with China is said to become one of the global financial superpower by 2025, so India is undergoing rapid nutrition and lifestyle transition, rapid urbanization and mechanization, which has led to a reduction in energy expenditure along with an increase in energy intake due to increased purchasing power and availability of high fat, energy-dense fast foods.5 With changing diet children are devoid of antioxidants and phytonutrients which is important to neutralize free radicals produced from eating foods deficient in essential nutrients.6
Oxidative stress and low-grade silent inflammation caused due to high levels of free radicals in the body as a result of the unavailability of antioxidants is the underlying cause of chronic diseases such as diabetes, high blood pressure, heart disease, loss of energy, premature aging and even obesity.6
The global escalation of childhood obesity is a major concern, as excessive adiposity is the root cause of leading metabolic and cardiovascular diseases and related mortality. Widely prevalent in obese adults, these metabolic comorbidities are beginning to surface in obese children, and it will not be unreasonable to expect a dramatic increase in young adults afflicted with glucose intolerance, hypertension, dyslipidemia, non-alcoholic fatty liver disease, and ischemic heart disease in the near future. Substantial consequences to the physical and mental health must be anticipated when caring for these young obese patients, as many of these chronic diseases are now appearing in childhood rather than adulthood.7
Obesity is related to several aspects of oral health. An association between over-weight and oral health has been suggested in adults, whereas evidence supporting this association in children is controversial. Recent studies have shown a high level of dental caries and mild gingival inflammation associated with obese children.8 Children who were overweight or obese have shown to have accelerated dental development, even after adjusting for age and gender.9
However, the data provided in the literature is still scarce and sometimes unclear especially in the Indian scenario, hence, the present study was carried out to evaluate the total salivary anti-oxidant levels, dental development, and oral health status in childhood obesity.
Materials and Methods
The study included both males and female children aged 6-12 years, selected randomly from various private schools in the South Canara, Karnataka, India. Body weight was measured using a balanced beam scale and height was measured using a stadiometer. Children were measured wearing light clothing and without shoes. Body mass index (BMI) was calculated using the formula weight in kilograms divided by height in meter square. The BMI percentile for age and sex were plotted on the growth chart by Indian Academy of Pediatrics Growth Monitoring Guidelines for Children.10 Based on BMI for age, children were be categorized into two groups consisting of 60 subjects in each.
Study group
Sixty subjects belonging to overweight and obese category of BMI percentile for age and sex (>85th percentile) were part of study group.
Control group
Sixty subjects belonging to non-obese category of BMI percentile for age and sex (<85th percentile) were part of the control group.
Oral hygiene index-simplified (OHI-S) a WHO oral health assessment form was used to analyze oral health status.11 Gingival status was assessed using modified gingival index.12
Phosphomolybdate method using spectrophotometer13,14 was used to estimate salivary total anti-oxidants levels. Dental development was determined by assessing. Chronological age of the child as per the school records and last erupted tooth was noted on dental examination and correlated with Logan and Kronfeld’s chronology of human dentition.15
The data obtained were tabulated, mean and standard deviation calculated. Threshold of significance was set at when P < 0.05. Mann–Whitney U-test, Chi-square test, and unpaired t-test were done to compare and correlate the various parameters between the study and the control group.
Results
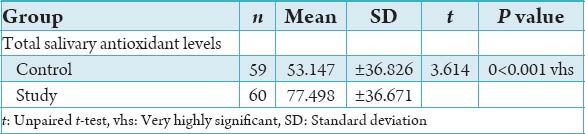
The total salivary antioxidant level in the control group showed a mean of 53.147 µg/dl whereas, that of Study group was 77.498 µg/dl. Levels of the total salivary anti-oxidants increased in the study group when compared with the control group, which was statistically significant (P < 0.0001) (Table 1).
Table 1.
Total salivary antioxidant levels in study group and control group.
n - Sample number
P - value - Probability value
P > 0.05 - Not significant (ns)
P < 0.05 - Significant (s)
P < 0.01 - Highly significant (hs)
P < 0.001 - Very highly significant (vhs)
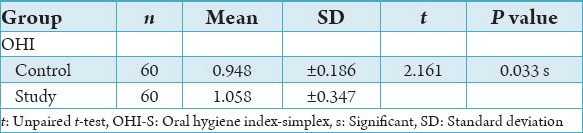
The mean scores for OHI-S in the control group showed 0.948 and, that of the study group was 1.058. The OHI-S scores were higher in study group when compared to the control group which was statistically significant (P - 0.033) (Table 2).
Table 2.
Oral hygiene of study group and control group using OHI-S.
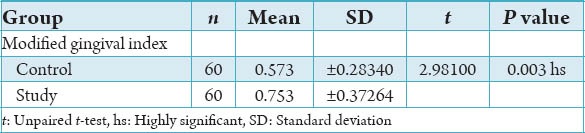
The gingival status score in the control group showed a mean of 0.573 and, that of the study group was 0.753.
The gingival index scores in study group were high when compared with the control group which was highly statistically significant (P - 0.003) (Table 3).
Table 3.
Gingival condition in study group and control group using gingival index.
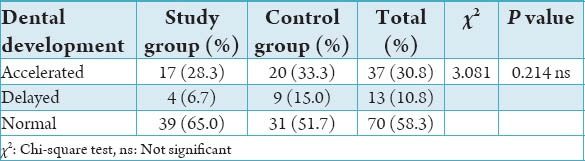
Dental development in 65.0% of children in study group and 51.7% in the control group had normal dental development and 6.7% of children in study group, and 15.0% of children in the control group showed delayed dental development. Whereas, 28.3% children in study group and 33.3% in the control group showed accelerated dental development.
Number of children in study group showing accelerated and delayed dental development was relatively less when compared to control group, but is not statistically significant (Table 4).
Table 4.
Dental development in study group and control group.
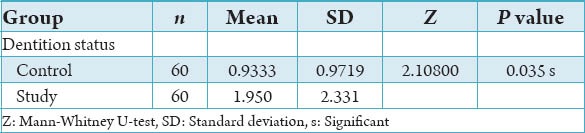
The mean scores of children in the study group who are affected by caries is 1.950 when compared to control group children with the mean scores of 0.9333. Caries experience in study group was high when compared to control group, which was statistically significant (Table 5).
Table 5.
Dental caries experience using dentition status.
Discussion
Childhood obesity is on the rise in the world and India is also catching up to it, and this study adds to very little data in the existing literature about association of childhood obesity an oral health and specifically in the Indian scenario.
Obesity is a state of excess storage of body fat resulting from a chronic imbalance between energy intake and energy expenditure.16 Obesity, in simple terms, may be defined as a state of imbalance between calories ingested versus calories expended which would lead to excessive or abnormal fat accumulation.
BMI is a measure of weight corrected for height and which reflects the total body fat and has been the most accepted parameter for defining over weight. Optimal BMI increases with age.
The oxidative damage can trigger a low-grade silent inflammation throughout the body that lingers for years or decades leading to the production of inflammatory hormones and chemicals, which turn on genes causing fat storage and disease and simultaneously turn off genes reducing inflammation and health risk.6 This weak immune response is the root cause of chronic degenerative disease such as diabetes, heart disease, and obesity.5
Obese individuals have a decrease in salivary and serum anti-oxidant levels which could also attribute to the pathogenesis of obesity.5 On the contrary, the present study has shown an increase in total salivary anti-oxidant levels in obese children when compared to nonobese children. The probable reason for the alteration in salivary total antioxidant capacity (TAC) could be because these children belong to a high socio economic stratum and are provided with a diet that is rich in phytonutrients and antioxidants.
The oral health status in both the study group and control group were good in the present study. This could be attributed to the good oral hygiene measures followed by these children. The parents of these children were well educated and from high socio-economic status. The children were also from private schools with both parents and teachers giving importance to personal and oral hygiene.
Good oral hygiene status has also reflected on good gingival health in the present study and is in accordance with other studies which has shown that obese adolescents were not at increased risk of chronic periodontitis.17
However, a significant number of studies have reported association between obesity and periodontal disease in adults, because multiple factors such as age, oxidative stress, general health, smoking, tobacco, the poor lifestyle play important role in the pathogenesis of periodontal disease.18
Therefore, good oral hygiene measures, lifestyle modification, oral and general health education during childhood of overweight and obese individuals establish a strong foundation for good periodontal and general health in the future.
Children who were overweight or obese had accelerated dental development, even after adjusting for age and gender,9 but in the present study, number of children in study group showing accelerated and delayed dental development was relatively less when compared to control group, that was not statistically significant.
This could be attributed to the small study group, and the methodology that was based on considering the clinically last erupted tooth that is acted upon by multiple factors.
Studies have also found that there is no significant accelerated skeletal maturity in overweight or obese children even after adjusting for age and sex.19
Dental caries is the most common infectious disease affecting humans. Recent studies have shown a high level of dental caries is associated with obese children,8,20,21 these in addition to food they eat. Dental caries could also be a source of oxidative stress in them.6
Even in the present study, the children from the study group had higher caries experience as compared to their control group. However, various studies show conflicting results (Table 6).22
Table 6.
Various studies on relationship between childhood obesity and dental caries.
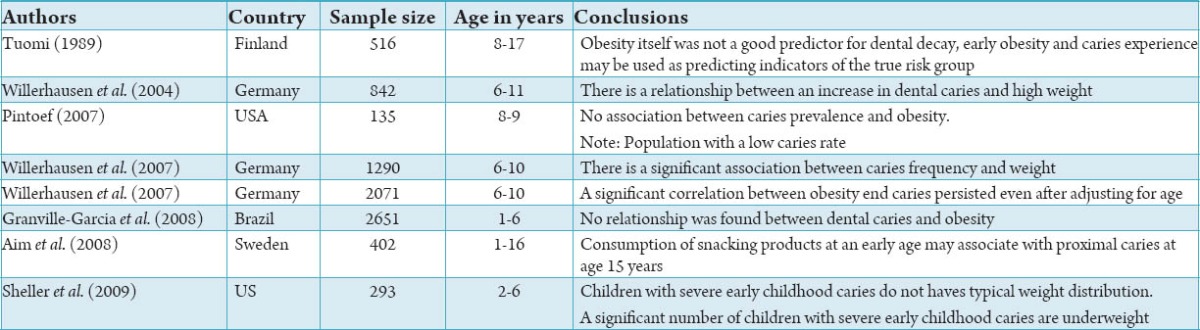
It is unclear if there is a correlation between caries and obesity or they just coexist since they have common etiologic factors such as diet and socioeconomic status. One could expect that as the result of diet habits, obese children will have a higher prevalence of caries when compared to children who are with a normal or lower than normal weight.22
While some of the etiologic factors of dental caries and obesity may interrelate, others may just be common to both diseases. Dental caries is a multi-factorial infectious disease which can be affected by oral hygiene, diet composition and frequency, socioeconomic status, salivary immune globulins, bacterial load, and fluoride intake. Obesity is a disease in which diet energy intake exceeds the body energy requirements resulting in excess in body fat. All these factors indicate a triangular association between “sugar-caries-obesity” which needs to further explored in the future.22
Environmental changes and lifestyle promoting increased energy intake and decreased energy output have a widespread impact on children causing the increase in the prevalence of overweight and obesity, this phenomenon having no age, gender or ethnic group limitations.
Thus, the pediatric dentist should be aware of the increasing challenge posed by the correlation between dental caries, obesity, oral and systemic disease. Furthermore, pediatric dentistry should team with other health professions for prevention and management of obese children.
Conclusion
Salivary TAC was significantly higher in overweight and obese children than their normal counterparts. Dental development is normal in obese/overweight children when compared to normal children. Prevalence of dental caries was high in obese/overweight children when compared to normal children.
Footnotes
Source of Support: Nil
Conflict of Interest: None
References
- 1.Martinez JA. Body-weight regulation: Causes of obesity. Proc Nutr Soc. 2000;59(3):337–45. doi: 10.1017/s0029665100000380. [DOI] [PubMed] [Google Scholar]
- 2.Mathus-Vliegen EM, Nikkel D, Brand HS. Oral aspects of obesity. Int Dent J. 2007;57(4):249–56. doi: 10.1111/j.1875-595x.2007.tb00128.x. [DOI] [PubMed] [Google Scholar]
- 3.Alm A, Fåhraeus C, Wendt LK, Koch G, Andersson-Gäre B, Birkhed D. Body adiposity status in teenagers and snacking habits in early childhood in relation to approximal caries at 15 years of age. Int J Paediatr Dent. 2008;18(3):189–96. doi: 10.1111/j.1365-263X.2007.00906.x. [DOI] [PubMed] [Google Scholar]
- 4.Bhave S, Bavdekar A, Otiv M. IAP National Task Force for Childhood Prevention of Adult Diseases: Childhood Obesity IAP National Task Force for Childhood Prevention of Adult Diseases: Childhood Obesity. Indian Pediatr. 2004;41(6):559–75. [PubMed] [Google Scholar]
- 5.Bhardwaj S, Misra A, Khurana L, Gulati S, Shah P, Vikram NK. Childhood obesity in Asian Indians: A burgeoning cause of insulin resistance, diabetes and sub-clinical inflammation. Asia Pac J Clin Nutr. 2008;17(Suppl 1):172–5. [PubMed] [Google Scholar]
- 6.Johnson BC. Lincoln, NE: iUniverse; 2007. New Priscription for Childhood Obesity. [Google Scholar]
- 7.Lee YS. Consequences of childhood obesity. Ann Acad Med Singapore. 2009;38(1):75–7. [PubMed] [Google Scholar]
- 8.Omar OM, Metwali NE, Elsedfy ZB, Abbas AH. Life-style and body mass index, implication for oral health in a group of Egyptian children. Cairo Dent J Part (II) 2007;183:192. [Google Scholar]
- 9.Hilgers KK, Akridge M, Scheetz JP, Kinane DE. Childhood obesity and dental development. Pediatr Dent. 2006;28(1):18–22. [PubMed] [Google Scholar]
- 10.Khadilkar VV, Khadilkar AV, Choudhury P, Agarwal KN, Ugra D, Shah NK. IAP growth monitoring guidelines for children from birth to 18 years. Indian Pediatr. 2007;44(3):187–97. [PubMed] [Google Scholar]
- 11.Willam EM. the Netherlands: Lea and Febiger; 1989. Clinical Practice of Dental Hygienist, Alphen aan den Rijn; pp. 269–73. [Google Scholar]
- 12.Erik PP. 4th ed. WHO Library Cataloguing in Publication Data; 1997. Oral Health Survey Basic methods; pp. 40–7. [Google Scholar]
- 13.Working Group 10 of the Commission on Oral Health, Research and Epidemiology (CORE) Saliva: Its role in health and disease. Int Dent J. 1992;42(4 Suppl 2):287–304. [PubMed] [Google Scholar]
- 14.Prieto P, Pineda M, Aguilar M. Spectrophotometric quantitation of antioxidant capacity through the formation of a phosphomolybdenum complex: Specific application to the determination of vitamin E. Anal Biochem. 1999;269(2):337–41. doi: 10.1006/abio.1999.4019. [DOI] [PubMed] [Google Scholar]
- 15.Logan WH, Kronfield R. Chronology of human dentition, slightly modified by McCall and Schour. J Am Dent Assoc. 1933;20:379. [Google Scholar]
- 16.Zhao LJ, Jiang H, Papasian CJ, Maulik D, Drees B, Hamilton J, et al. Correlation of obesity and osteoporosis: Effect of fat mass on the determination of osteoporosis. J Bone Miner Res. 2008;23(1):17–29. doi: 10.1359/JBMR.070813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Reeves AF, Rees JM, Schiff M, Hujoel P. Total body weight and waist circumference associated with chronic periodontitis among adolescents in the United States. Arch Pediatr Adolesc Med. 2006;160(9):894–9. doi: 10.1001/archpedi.160.9.894. [DOI] [PubMed] [Google Scholar]
- 18.Al-Zahrani MS, Bissada NF, Borawskit EA. Obesity and periodontal disease in young, middle-aged, and older adults. J Periodontol. 2003;74(5):610–5. doi: 10.1902/jop.2003.74.5.610. [DOI] [PubMed] [Google Scholar]
- 19.Akridge M, Hilgers KK, Silveira AM, Scarfe W, Scheetz JP, Kinane DF. Childhood obesity and skeletal maturation assessed with Fishman's hand-wrist analysis. Am J Orthod Dentofacial Orthop. 2007;132(2):185–90. doi: 10.1016/j.ajodo.2005.12.034. [DOI] [PubMed] [Google Scholar]
- 20.Willershausen B, Haas G, Krummenauer F, Hohenfellner K. Relationship between high weight and caries frequency in German elementary school children. Eur J Med Res. 2004;9(8):400–4. [PubMed] [Google Scholar]
- 21.Hilgers KK, Kinane DE, Scheetz JP. Association between childhood obesity and smooth-surface caries in posterior teeth: A preliminary study. Pediatr Dent. 2006;28(1):23–8. [PubMed] [Google Scholar]
- 22.Bimstein E, Katz J. Obesity in children: A challenge that pediatric dentistry should not ignore – Review of the literature. J Clin Pediatr Dent. 2009;34(2):103–6. doi: 10.17796/jcpd.34.2.65q424243n468452. [DOI] [PubMed] [Google Scholar]