

Abstract
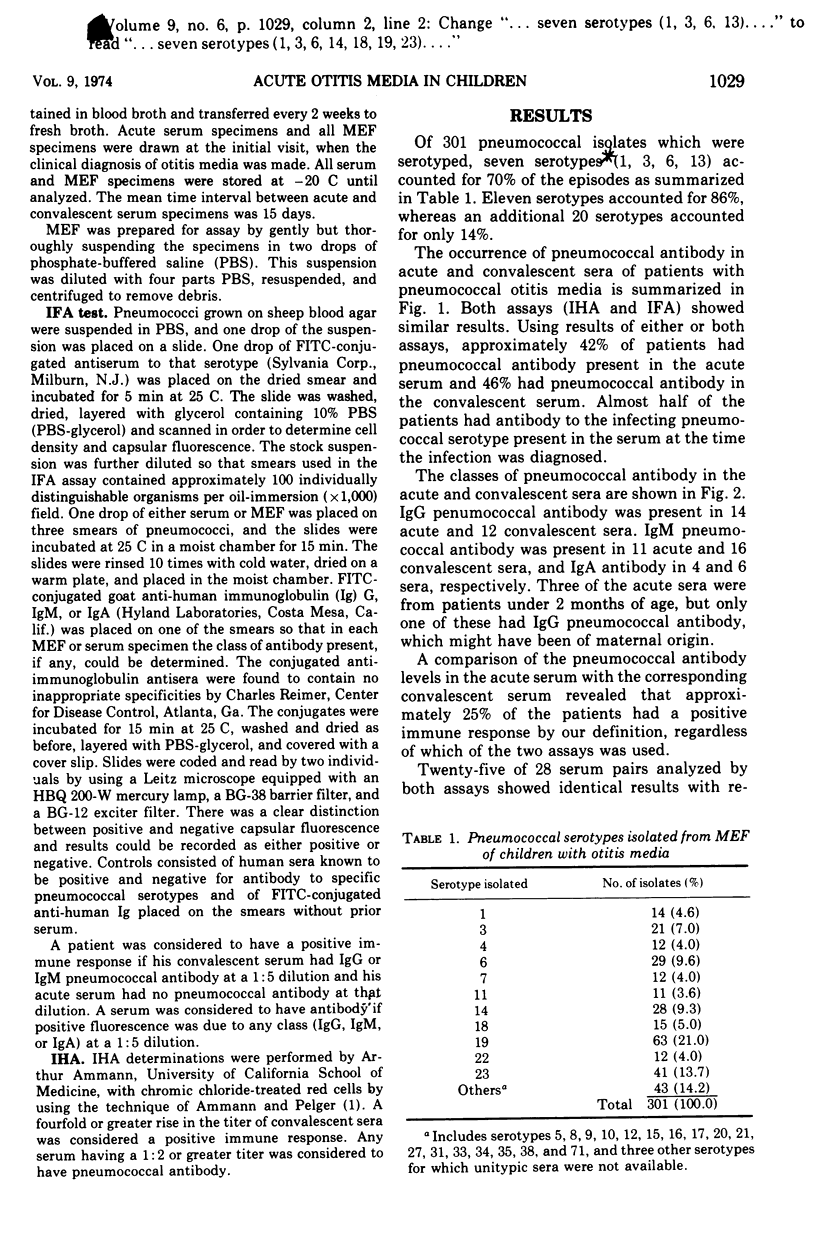
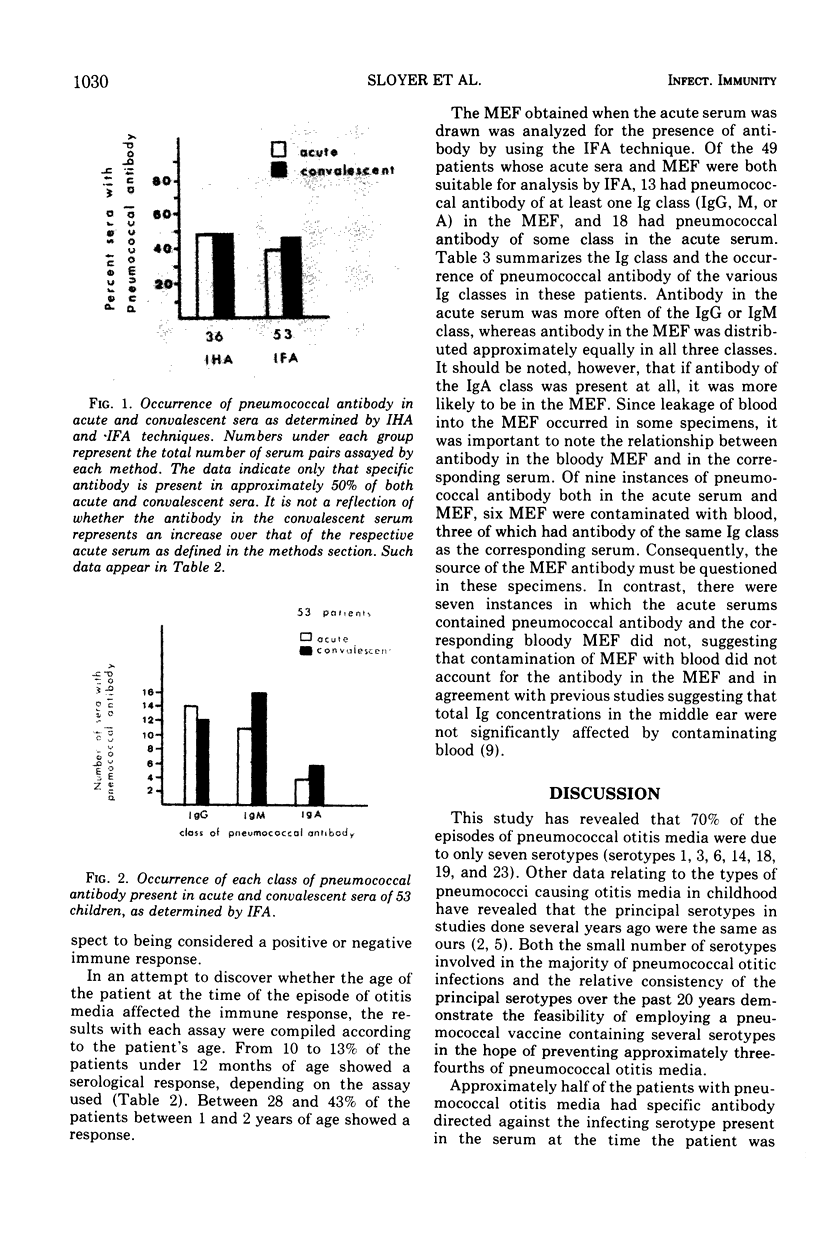
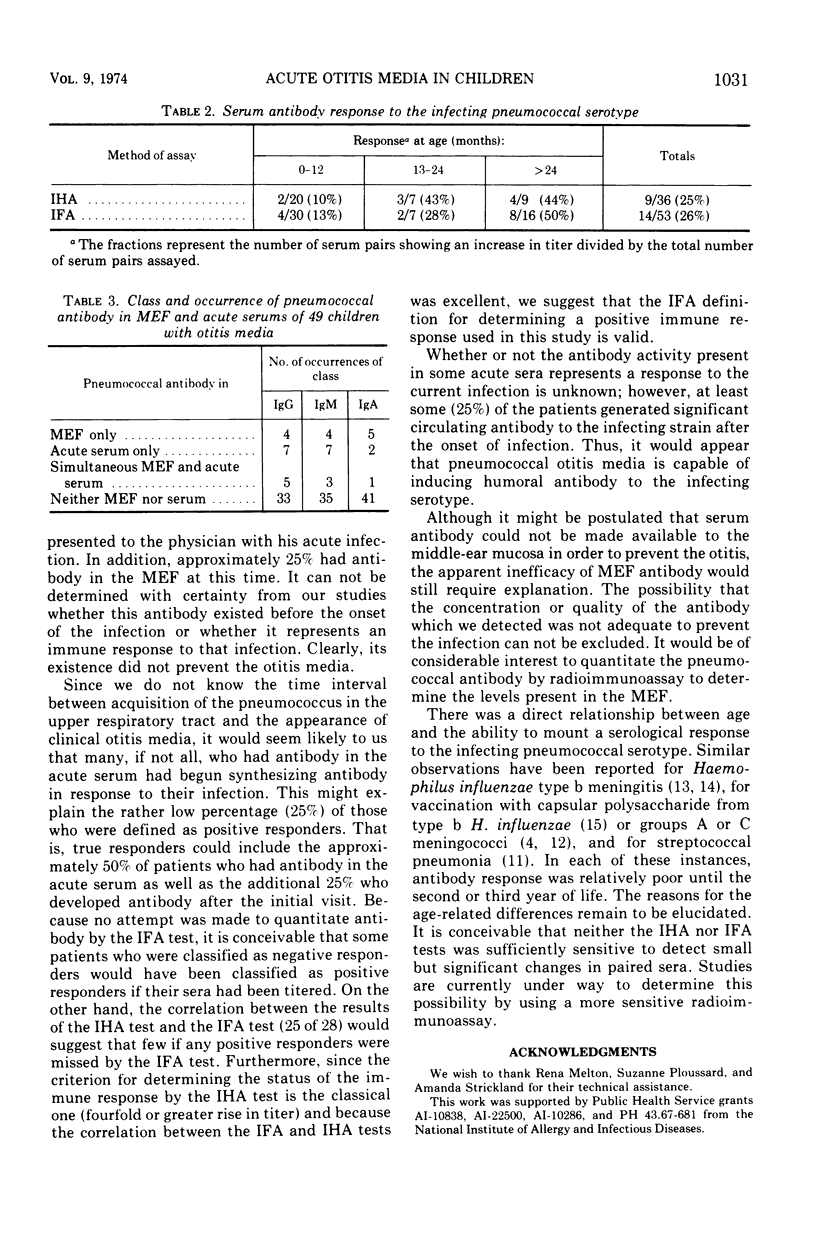
Seventy percent of pneumococci isolated from the middle-ear cavity of infants and children with acute otitis media were of one of the seven serotypes 1, 3, 6, 14, 18, 19, or 23. The immunological response in the serum and middle-ear fluid from otitis media caused by one of these serotypes was studied in 61 children by using either indirect hemagglutination or indirect fluorescent antibody tests, or both. Twenty-six of the patients had pneumococcal antibody present in the acute serum and 28 had it in the convalescent serum by at least one method. Thirteen of the 49 middle-ear fluids examined had antibody by the indirect fluorescent antibody technique. Serum pneumococcal antibody was found to reside predominantly in the immunoglobulin G or immunoglobulin M classes, whereas pneumococcal antibody with middle-ear fluid was found to be distributed equally among all three classes. Approximately 25% of the patients (16 of 61) had a positive immune response to their infection as evidenced by increased levels of pneumococcal antibody in the convalescent serum. The percentage of patients responding immunologically increased with age: 12% of infants less than 12 months showed a significant response, whereas 48% of children over 24 months responded.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ammann A. J., Pelger R. J. Determination of antibody to pneumococcal polysaccharides with chromic chloride-treated human red blood cells and indirect hemagglutination. Appl Microbiol. 1972 Nov;24(5):679–683. doi: 10.1128/am.24.5.679-683.1972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BJUGGREN G., TUNEVALL G. Otitis in childhood; a clinical and sero-bacteriological study with special reference to the significance of Haemophilus influenzae in relapses. Acta Otolaryngol. 1952 Aug-Oct;42(4-5):311–328. doi: 10.3109/00016485209120357. [DOI] [PubMed] [Google Scholar]
- Brownlee R. C., Jr, DeLoache W. R., Cowan C. C., Jr, Jackson H. P. Otitis media in children. Incidence, treatment, and prognosis in pediatric practice. J Pediatr. 1969 Oct;75(4):636–642. doi: 10.1016/s0022-3476(69)80460-9. [DOI] [PubMed] [Google Scholar]
- GROENROOS J. A., KORTEKANGAS A. E., OJALA L., VUORI M. THE AETIOLOGY OF ACUTE MIDDLE EAR INFECTION. Acta Otolaryngol. 1964 Aug-Sep;58:149–158. doi: 10.3109/00016486409121372. [DOI] [PubMed] [Google Scholar]
- Gotschlich E. C., Rey M., Triau R., Sparks K. J. Quantitative determination of the human immune response to immunization with meningococcal vaccines. J Clin Invest. 1972 Jan;51(1):89–96. doi: 10.1172/JCI106801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holm V. A., Kunze L. H. Effect of chronic otitis media on language and speech development. Pediatrics. 1969 May;43(5):833–839. [PubMed] [Google Scholar]
- Howie V. M., Ploussard J. H. Bacterial etiology and antimicrobial treatment of exudative otitis media: relation of antibiotic therapy to relapses. South Med J. 1971 Feb;64(2):233–239. doi: 10.1097/00007611-197102000-00022. [DOI] [PubMed] [Google Scholar]
- Howie V. M., Ploussard J. H., Sloyer J. L., Johnston R. B., Jr Immunoglobulins of the middle ear fluid in acute otitis media: relationship to serum immunoglobulin concentrations and bacterial cultures. Infect Immun. 1973 Apr;7(4):589–593. doi: 10.1128/iai.7.4.589-593.1973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howie V. M., Ploussard J. H. The "in vivo sensitivity test"--bacteriology of middle ear exudate, during antimicrobial therapy in otitis media. Pediatrics. 1969 Dec;44(6):940–944. [PubMed] [Google Scholar]
- KEVY S. V., LOWE B. A. Streptococcal pneumonia and empyema in childhood. N Engl J Med. 1961 Apr 13;264:738–743. doi: 10.1056/NEJM196104132641502. [DOI] [PubMed] [Google Scholar]
- Kaplan G. J., Fleshman J. K., Bender T. R., Baum C., Clark P. S. Long-term effects of otitis media: a ten-year cohort study of Alaskan Eskimo children. Pediatrics. 1973 Oct;52(4):577–585. [PubMed] [Google Scholar]
- Norden C. W., Melish M., Overall J. C., Jr, Baum J. Immunologic responses to Hemophilus influenzae meningitis. J Pediatr. 1972 Feb;80(2):209–214. doi: 10.1016/s0022-3476(72)80580-8. [DOI] [PubMed] [Google Scholar]
- Smith D. H., Peter G., Ingram D. L., Harding A. L., Anderson P. Responses of children immunized with the capsular polysaccharide of Hemophilus influenzae, type b. Pediatrics. 1973 Nov;52(5):637–644. [PubMed] [Google Scholar]