

Abstract
Objective
To estimate the association between swimming lessons and the risk of drowning among children aged 1 to 19 years.
Design
Case-control study.
Setting
Cases were identified from medical examiners’/ coroners’ offices between mid-2003 and mid-2005. Jurisdictions included the states of Maryland and North Carolina, 14 districts (33 counties) in Florida, 3 counties in California, 1 county in Texas, and 1 county in New York.
Participants
Cases were children and adolescents aged 1 to 19 years who died of unintentional drowning. Interviews were conducted with 88 families of children who drowned and 213 matched controls.
Main Exposure
Swimming lessons.
Main Outcome Measure
Death due to unintentional drowning. Drownings that were intentional, of undetermined intent, or that occurred under conditions in which swimming ability was unlikely to impact risk (eg, in ice water or bathtubs) were excluded.
Results
Of the 61 cases in the 1- to 4-year age group, 2 (3%) had participated in formal swimming lessons vs 35 of 134 matched controls (26%) (adjusted odds ratio [OR], 0.12; 95% confidence interval [CI], 0.01–0.97). Among the 27 cases aged 5 to 19 years, 7 (27%) had ever taken formal swimming lessons vs 42 of 79 matched controls (53%) (adjusted OR, 0.36; 95% CI, 0.09–1.51). In adjusted analyses, there was no statistically significant association between informal instruction and drowning risk.
Conclusions
Participation in formal swimming lessons was associated with an 88% reduction in the risk of drowning in the 1- to 4-year-old children, although our estimates were imprecise and 95% CIs included risk reductions ranging from 3% to 99%.
During 2000 Through 2005, 6900 children younger than 20 years died of unintentional, non–boat-related drowning in the United States (rate, 1.42 per 100 000 person-years).1 Among children younger than 5 years, the rate was 2.68, and among those 1 to 2 years of age, it was 4.12. Interventions to prevent drowning are dependent on the age of the victim and the circumstances surrounding the event.2–4
For toddlers, mandatory pool fencing is one effective strategy for prevention of many drownings; however, it primarily addresses circumstances in which a child gains unauthorized access to the pool but does not address submersions that occur when a child is known to be in the pool area or around another body of water, eg, a lake or canal.5–8 The effectiveness of other potential prevention strategies is un-known.4 One such strategy is increased swimming ability through participation in swimming lessons. The American Academy of Pediatrics recommends that, after the age of 5 years, all children be taught to swim; however, because of the absence of data regarding effects of swimming lessons on drowning risk, the American Academy of Pediatrics does not recommend for or against swimming lessons as a preventive strategy among children younger than 5 years.9–11
This population-based case-control study estimated the association between participation in swimming lessons and risk of drowning. Our primary goal was to study the effects of swimming lessons in the 1- to 4-year age group, as this is the age group for which it has been most difficult to form appropriate recommendations. We also collected data about risk factors for drowning among older children because the surveillance and interview methods established for the younger children provided an opportunity to do so.
METHODS
OVERVIEW
Drowning deaths were identified through the offices of medical examiners or coroners (hereafter referred to as medical examiners). Jurisdictions targeted for participation were those with relatively large numbers of childhood drownings in the 1- to 4-year age group. To facilitate study procedures for initial contacts with families, we targeted jurisdictions in which investigation of drowning was routinely conducted by the medical examiner’s office. Study jurisdictions included the states of Maryland and North Carolina, 14 districts in Florida (covering a total of 33 counties), 3 counties in California, 1 county in Texas, and 1 county in New York. Information was obtained about drownings of children aged 1 through 19 years. Matched controls were identified through random-digit dialing as detailed later. This project was approved by the institutional review boards of the National Institute of Child Health and Human Development and Westat, the firm that conducted the data collection.
CASE DEFINITION, IDENTIFICATION, AND DATA COLLECTION
Cases were defined as deaths resulting from submersion in a liquid medium within a participating jurisdiction. A priori exclusion criteria included drownings that were intentional or of undetermined intent and submersions in bodies of water or under conditions in which swimming ability was unlikely to impact risk, such as ice water, bathtubs, and buckets.
Cases were identified through both active surveillance and passive reporting by participating medical examiner offices. Surveillance calls were made to participating offices on a weekly to monthly basis, depending on the historical frequency of drowning within that jurisdiction. In addition, study staff conducted newspaper searches in participating counties. Identification of a new case through a newspaper search triggered a call from study staff to the appropriate medical examiner office to verify eligibility and gather additional information about the incident. For most jurisdictions, surveillance began in spring 2003 and ended in September 2005, although some jurisdictions began later or ended earlier, generally because of administrative issues within the medical examiner office. For each identified eligible drowning, a standardized case abstract form was completed based on information from the routine investigation. The form included information about the decedent and details about the drowning scene (eg, site of submersion) and about the child’s past participation in formal swimming lessons.
Procedures for contacting case families have been previously published.12 Investigators from the medical examiner offices informed the next of kin about the study in person, by telephone, or, in one state, by mail. If the next of kin did not decline participation, they were sent a brochure and letter describing the study. The materials indicated that study staff would contact potential participants to schedule an in-depth telephone interview and included a telephone number to call if the participant did not want to be contacted. Next of kin who did not opt out were contacted to schedule the telephone interview.
During data collection, it became apparent that some families did not learn of the study through these procedures (eg, the investigator forgot to describe the study to the family). Procedures were thus modified, approximately 1 year following initiation of data collection, so that all families could be informed about and invited to participate in the study. In these instances, the medical examiner sent a letter and brochure describing the study and a short questionnaire regarding the child’s prior participation in swimming lessons. At the end of the questionnaire were 2 check boxes, one that gave permission for study staff to contact the family and another that indicated that the respondent did not wish to be contacted further about the study. Only those who returned the questionnaire and checked the box giving permission for further contact were contacted for a telephone interview.
IDENTIFICATION OF CONTROLS
Controls were sought only for those cases with information on swimming lessons from either the medical examiner investigation or the study interview (ie, if information on swimming lessons was not available from the medical examiner’s investigation and the case family had opted out of the study, we did not attempt to find matching controls). A minimum of 2 matched controls were sought for each case through random-digit dialing. Matching variables included age, sex, and county of residence. Additionally, in the 1- to 4-year age group, cases and controls were matched on the presence of a swimming pool at their home. For 1- to 4-year-olds, the date of birth for the control had to be within 6 months of the date of birth of the case and for 5- to 19-year-olds, cases and controls were matched by age group, 5 to 9, 10 to 14, and 15 to 19 years.
In each participating county, households were prescreened (ie, prior to identification of drowning events) to create a list of households with potentially eligible controls. The sampling frame used to screen households was the set of telephone exchanges that covered the jurisdiction.13,14 The number of households screened was dependent on the number of drownings expected in the 1- to 4-year age group based on data from prior years. The household screening enumerated the sex and year and month of birth for each household resident younger than 20 years. When date of birth was not available, age or age group was listed. When a drowning occurred, the 2 controls who most tightly matched the case were selected from this list.
In the more tightly matched 1- to 4-year age group, sometimes controls who met the earlier-listed criteria were not available in the prescreened list. In these instances, criteria were “loosened,” first to allow matched controls residing in adjacent counties, followed by extension of the age range to within 1 year of the case, and finally by including controls of the opposite sex. For cases who drowned within a participating jurisdiction but lived outside of that jurisdiction, a list of telephone numbers was generated based on the case’s telephone number. Lists were generated in a manner similar to that described earlier for prescreening, ie, with a sampling frame that was the set of telephone exchanges that covered the jurisdiction.13,14 All tightly matched controls identified in a group of numbers were interviewed in order to avoid bias that might occur if only the first identified households were enrolled. This alternate procedure was also used when the case resided in a participating county but no control was identified from the prescreened list.
CASE AND CONTROL INTERVIEWS
Study staff telephoned families of cases and controls, and those providing verbal consent underwent a computer-assisted telephone interview. Interviews included questions about exposure to water, swimming ability, participation in formal and informal swimming lessons, child development and temperament (1- to 4-year-olds), risk taking, medical conditions, and household characteristics. The case interview referred to the period prior to the drowning event, while the control interview obtained information for the period prior to the date on which the matched case drowned. Respondents were offered $25 to compensate for the time involved in completing the interview. Interviewers were aware of whether they were interviewing a case or control family but were not informed of the primary study objective.
The primary exposure was participation in formal swimming lessons, addressed by the question “Children sometimes receive formal swimming lessons that are paid for or that are received as part of another activity such as day care, school, or camp. Had [child’s name] ever taken formal swimming lessons?” Control families were read the same introduction and asked “Prior to [reference mm/yy], had [child’s name] ever taken formal swimming lessons?” Informal swimming instructions were assessed by asking if the child received informal instructions, pointers, or tips about swimming or water safety when he or she went swimming. In analyses, those receiving informal instruction most of the time or every time they went swimming were coded as receiving informal instruction. In study interviews, questions about formal swimming lessons were asked of all respondents; however, swimming ability and informal instruction were asked only of respondents whose children had ever been in a swimming pool, pond, or body of water other than a bathtub. Those who reported no exposure to water were coded as never having received pointers and as nonswimmers.
SAMPLE SIZE ESTIMATES
It was estimated that a sample size of 166 cases and 331 matched controls would be needed to detect an odds ratio (OR) of 0.5 (assumptions included a 28% prevalence of swimming lessons, type I error of 0.04 [to account for a planned interim analysis], and 80% power). A planned interim analysis was conducted after accrual of the first 65 cases with information on formal swimming lessons. Based on results of the interim analysis (OR, 0.17; P=.006), case accrual was terminated after approximately 30 months of data collection. Interviews with case and control families continued through January 2006.
POTENTIAL CONFOUNDERS
We considered a variable as a potential confounder if it was associated with drowning risk in prior studies or if we conceptualized the factor as being potentially associated with both swimming lessons and drowning risk but not a result of receipt of swimming lessons.15 We thus considered the following potential confounders: child’s age (coded as a continuous variable by month [ages 1–4 years] or year [ages 5–19 years]); sex; race; presence of other children younger than 6 years in the household; household income; respondent’s education; history of a seizure disorder; presence of other health problems (physician said that the child had a health problem expected to last 6 months or longer, including physical or mental impairments); respondent’s ranking of child’s general health; exposure to water in the summer months; exposure to water in the winter months; and risk taking (Injury Behavior Checklist16,17 [ages 1–9 years] and the Arnett Inventory of Sensation Seeking [ages 10–19 years]).18 In 1- to 4-year-olds, we also considered child motor development (specific motor skills) and temperament (Short Temperament Scale for Toddlers19,20). Variables that measured swimming ability or comfort in the water were not considered as confounders in multivariable models assessing the relation between swimming lessons and drowning, as these variables were thought to be impacted by swimming lessons.
STATISTICAL METHODS
Characteristics of cases with and without a study interview were compared using information from the medical examiner abstract form. Characteristics of cases and matched controls were then compared using conditional logistic regression, with confidence intervals (CIs) calculated from the standard errors of the regression coefficients and P values from the Wald statistic. In general, information for this comparison was obtained from the study interview. For one case, information about formal swimming lessons was missing from the study interview and was thus obtained from the medical examiner abstract form, which included an item about participation in formal swimming lessons, defined the same as in the study interview.
If a factor was associated with drowning death with a P value <.10, it was considered as a potential confounder of the association between swimming lessons and drowning death. Because of the small number of cases, a forward selection process was used to determine which variables to retain in the final model. As described by Greenland and Rothman,21 the initial model contained only a term for receipt of formal swimming lessons, and then each potential confounder was added individually to the initial model. The confounder that resulted in the largest change in the OR (of at least 10%) from the initial model was retained and, in conjunction with the term for swimming lessons, formed the model for the next step. The remaining potential confounders were each added individually, and the one resulting in the largest change in OR (of at least 10%) was retained. This continued until no additional variables changed the OR by at least 10%. The process was repeated with informal swimming lessons as the key exposure of interest. In the 1- to 4-year-old age group, both education and income were significantly associated with drowning risk and when added to a model with formal swimming instruction, each changed the OR by more than 10%. Since the 2 variables were highly correlated with one another (correlation coeffi-cient=0.51) and data were more complete for education, we chose to include education (rather then income) in adjusted models. In the analysis of informal lessons, income, but not education, changed the adjusted OR by more than 10% and was therefore included in the model. Results of adjusted models are reported as ORs with 95% CIs. All analyses were conducted using version 9 of SAS (SAS Institute Inc, Cary, North Carolina).
RESULTS
We identified 268 eligible cases. Four of these cases, identified through newspaper searches, had no accompanying data from the medical examiners’ office and thus were eliminated from analyses. Of the remaining 264 cases, investigators from the medical examiner offices introduced the study to 146 families, 55 of whom asked not to be contacted by study staff. Contact was initiated by study staff with the remaining 91 families. Of these, 75 were interviewed. An additional 43 families received study materials by mail, 13 of whom were interviewed by study staff. Comparable recruitment figures are presented by age group in the Figure.
Figure.
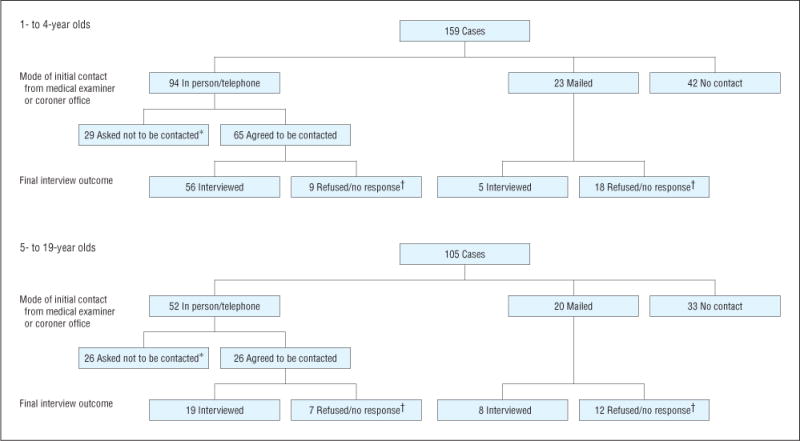
Case accrual by age group. *Respondents indicated through the medical examiner that they did not want study staff to contact them. †On contact from study staff, respondent refused participation in interview or study staff received no response to telephone calls.
Characteristics of children who drowned whose families were interviewed by study staff (study participants) were compared with those whose families were not interviewed but for whom there was information from medical examiners’ investigations (nonparticipants) (Table 1). Participants and nonparticipants were similar with respect to most characteristics. Information about participation in formal swimming lessons was missing from medical examiner reports more often for nonparticipants (49%) vs participants (25%). However, among those with this information, the percentage with swimming lessons was identical (6%) for participants and nonparticipants in the 1- to 4-year age group. Among 5- to 19-year-olds, medical examiner reports indicated that 37% of participants had formal swimming instruction vs 19% of nonparticipants.
Table 1.
Characteristics of Children Who Drowned With Study Interviews vs Those Without Interviews
| No. (%)b
|
||||
|---|---|---|---|---|
| 1- to 4-Year-Olds
|
5- to 19-Year-Olds
|
|||
| Characteristica | Participants (n=61) |
Nonparticipants (n=98) |
Participants (n=27) |
Nonparticipants (n=78) |
| Sex | ||||
| M | 36 (59) | 70 (71) | 23 (85) | 70 (90) |
| F | 25 (41) | 28 (29) | 4 (15) | 8 (10) |
| Race/ethnicity | ||||
| White | 36 (65) | 54 (55) | 11 (42) | 20 (27) |
| African American | 7 (13) | 17 (17) | 11 (42) | 34 (45) |
| Latino | 10 (18) | 16 (16) | 3 (12) | 12 (16) |
| Other | 2 (4) | 6 (11) | 1 (4) | 9 (12) |
| Site of drowning | ||||
| Pool/hot tub | 47 (77) | 75 (77) | 10 (37) | 35 (45) |
| Lake/pond | 10 (16) | 16 (16) | 5 (19) | 18 (23) |
| Other | 4 (6) | 7 (7) | 12 (44) | 25 (32) |
| Location of drowning | ||||
| Decedent’s home | 29 (48) | 60 (64) | 3 (12) | 8 (11) |
| Other home | 22 (36) | 22 (24) | 2 (8) | 9 (12) |
| Other | 10 (16) | 11 (12) | 20 (80) | 59 (78) |
| Participation in formal swimming lessons | ||||
| No | 47 (94) | 50 (94) | 10 (62) | 30 (81) |
| Yes | 3 (6) | 3 (6) | 6 (37) | 7 (19) |
Based on reports from medical examiners and coroners.
Totals vary slightly because of missing data; percentage of distribution based on a denominator of those with information.
To identify controls, we screened a total of 38 953 households. Of these, 12 224 households had at least 1 child aged 1 to 19 years. Nine hundred eighty-two households were selected for an extended interview. Of these, interviews were conducted with members of 556 households. Of the remaining selected households, 91 were found to be ineligible on contact (the most common reason being because the household did not include a child in the targeted age range), 236 were not successfully contacted, and 99 refused participation. The current analysis includes only controls matched with those cases with a completed study interview. A total of 213 controls are included in the current analyses (134 matched to cases aged 1–4 years and 79 matched to cases aged 5–19 years).
CHILDREN AGED 1 TO 4 YEARS
The mean age of cases was 2.62 years vs a mean age of 2.71 years for matched controls (P=.77). Cases were less likely to have participated in formal swimming lessons. Of the 61 interviewed cases, 2 (3%) had ever taken formal swimming lessons vs 35 of the 134 controls (26%) (P= .002). Cases were also reported to be less skilled swimmers. For example, only 5% of cases were reported as being able to float on the back for 10 seconds vs 18% of controls (P = .01).
Of the factors examined, race, income, education, risk taking, temperament, and presence of a medical condition were all associated with drowning risk, at a P value <.10 (Table 2). Education, risk taking, and race were retained as confounders in the final adjusted model examining the association between formal swimming lessons and drowning risk. In this model, participation in formal swimming lessons remained a significant predictor of drowning risk (adjusted OR, 0.12; 95% CI, 0.01–0.97). Variables retained as confounders in the model examining the association between informal swimming lessons and drowning risk included household income, temperament, and risk taking. After adjusting for these factors, there was no significant association between receipt of informal swimming instruction and drowning risk (adjusted OR, 0.54; 95% CI, 0.23–1.27).
Table 2.
Characteristics of Cases vs Matched Controls Aged 1 to 4 Years
| No. (%)b
|
|||
|---|---|---|---|
| Characteristica | Cases (n=61) |
Controls (n=134) |
P Valuec |
| Demographic | |||
| Age, y, mean (SD) | 2.62 (1.01) | 2.71 (1.03) | .77 |
| Sexd | .78 | ||
| F | 25 (41) | 56 (42) | |
| M | 36 (59) | 78 (58) | |
| Race | .04 | ||
| White | 35 (57) | 84 (72) | |
| Nonwhite | 26 (43) | 32 (28) | |
| Household income, $ | .03 | ||
| >50000 | 25 (48) | 83 (70) | |
| ≤50000 | 27 (52) | 36 (30) | |
| Education of respondente | .003 | ||
| >High school | 25 (44) | 84 (73) | |
| ≤High school | 32 (56) | 31 (27) | |
| Children <6yin household | .16 | ||
| No | 24 (42) | 63 (55) | |
| Yes | 33 (58) | 52 (46) | |
| Environmental | |||
| Exposure to water, May-Sep, time/mo | .15 | ||
| ≤1 | 22 (37) | 37 (28) | |
| >1 | 38 (63) | 97 (72) | |
| Exposure to water, Oct-Apr, time/mo | .12 | ||
| ≤1 | 46 (87) | 98 (80) | |
| >1 | 7 (13) | 24 (20) | |
| Of those with a pool | .68 | ||
| Four-sided fence | 10 (33) | 27 (44) | |
| Property fence | 7 (23) | 12 (19) | |
| No fence | 13 (43) | 23 (37) | |
| Health and development | |||
| Able to climb ladder | .30 | ||
| No | 18 (30) | 43 (38) | |
| Yes | 42 (70) | 70 (62) | |
| Able to open sliding door | .41 | ||
| No | 26 (50) | 66 (59) | |
| Yes | 26 (50) | 45 (41) | |
| Able to walk well | .30 | ||
| No | 0 | 5 (4) | |
| Yes | 61 (100) | 113 (96) | |
| Risk taking score, mean (SD) | 2.07 (0.48) | 1.90 (0.46) | .03 |
| Temperament score, mean (SD) | 2.74 (0.38) | 2.84 (0.32) | .06 |
| General health | .11 | ||
| Excellent/very good/good | 57 (93) | 114 (98) | |
| Fair/poor | 4 (7) | 2 (2) | |
| Seizure disorder | .79 | ||
| No | 60 (98) | 130 (98) | |
| Yes | 1 (2) | 3 (2) | |
| Other medical condition | .07 | ||
| No | 49 (80) | 120 (91) | |
| Yes | 12 (20) | 12 (9) | |
| Swimming lessons | |||
| Formal | .002 | ||
| No | 59 (97) | 99 (74) | |
| Yes | 2 (3) | 35 (26) | |
| Informal instructionf | .24 | ||
| Never/rarely/sometimes | 25 (42) | 42 (35) | |
| Every or most of the time | 35 (58) | 78 (65) | |
| Comfort in water | |||
| Liked the water | .65 | ||
| No | 14 (23) | 27 (20) | |
| Yes | 47 (77) | 106 (80) | |
| Comfortable in water | .71 | ||
| Uncomfortable/slightly uncomfortable | 12 (20) | 18 (15) | |
| Comfortable/very comfort | 49 (80) | 101 (85) | |
| Comfortable putting whole head in water | .36 | ||
| No | 38 (64) | 70 (59) | |
| Yes | 21 (36) | 49 (41) | |
| Swimming ability | |||
| Float on back for 10 s | .01 | ||
| No | 57 (95) | 110 (82) | |
| Yes | 3 (5) | 24 (18) | |
| Swim on stomach 15 ft | .07 | ||
| No | 59 (97) | 120 (90) | |
| Yes | 2 (3) | 14 (10) | |
| Jump in a pool/swim 5 ft/back to wall | .07 | ||
| No | 59 (97) | 106 (88) | |
| Yes | 2 (3) | 14 (12) | |
Characteristic of case or control, except where specified in headings.
Totals vary slightly because of missing data; percentage of distribution based on a denominator of those with information.
P value from the Wald statistic of a conditional logistic regression model containing only that variable.
Although cases and controls were matched by sex, we were not able to find sex-matched controls for all cases.
Asked only if the respondent lived with the child.
Assessed by asking how often the child received informal instructions, pointers, or tips about swimming or water safety when he or she went swimming.
CHILDREN AGED 5 TO 19 YEARS
The mean age of cases was 14.0 years vs a mean age of 13.7 years for matched controls (P=.06). Of the 26 cases with information on swimming lessons, 7 (27%) had ever taken formal swimming lessons vs 42 of the 79 matched controls (53%) (P=.02) (Table 3). Cases were also reported to be poorer swimmers. For example, 42% of cases were unable to swim continuously for at least a minute vs only 16% of matched controls (P=.01).
Table 3.
Characteristics of Cases vs Matched Controls Aged 5 to 19 Years
| No. (%)b
|
|||
|---|---|---|---|
| Characteristica | Cases (n=27) | Controls (n=79) | P Valuec |
| Demographic | |||
| Age, y, mean (SD) | 14.0 (5.2) | 13.7 (4.6) | .06 |
| Sexd | … | ||
| F | 4 (15) | 9 (11) | |
| M | 23 (85) | 70 (89) | |
| Race | .09 | ||
| White | 12 (48) | 47 (68) | |
| Nonwhite | 13 (52) | 22 (32) | |
| Household income, $ | .01 | ||
| >50000 | 5 (21) | 39 (57) | |
| ≤50000 | 19 (79) | 30 (43) | |
| Education of respondente | .11 | ||
| >High school | 10 (50) | 45 (65) | |
| ≤High school | 10 (50) | 24 (35) | |
| Children <6yin household | .88 | ||
| No | 19 (83) | 65 (82) | |
| Yes | 4 (17) | 14 (18) | |
| Environmental | |||
| Exposure to water, May–Sep, time/mo | .11 | ||
| ≤1 | 10 (38) | 18 (23) | |
| >1 | 16 (62) | 61 (77) | |
| Exposure to water, Oct–Apr, time/mo | .13 | ||
| ≤1 | 23 (88) | 60 (76) | |
| >1 | 3 (12) | 19 (24) | |
| Health and development | |||
| Risk taking score, ages 5–9 y, mean (SD) | 2.15 (0.80) | 1.87 (0.36) | .32 |
| Sensation seeking score, ages 10–19 y, mean (SD) | 2.30 (0.61) | 2.44 (0.40) | .44 |
| General health | … | ||
| Excellent/very good/good | 25 (100) | 69 (100) | |
| Fair/poor | 0 | 0 | |
| Seizure disorder | .005 | ||
| No | 20 (80) | 78 (100) | |
| Yes | 5 (20) | 0 | |
| Other medical condition | .38 | ||
| No | 17 (65) | 59 (76) | |
| Yes | 9 (35) | 19 (24) | |
| Swimming lessons | |||
| Formal | .02 | ||
| No | 19 (73) | 37 (47) | |
| Yes | 7 (27) | 42 (53) | |
| Informal instructionf | .45 | ||
| Never/rarely/sometimes | 9 (41) | 21 (30) | |
| Every or most of the time | 13 (59) | 49 (70) | |
| Comfort in water | |||
| Comfortable in water | .81 | ||
| Uncomfortable/slightly uncomfortable | 4 (17) | 11 (14) | |
| Comfortable/very comfortable | 20 (83) | 67 (86) | |
| Comfortable putting whole head in water | .32 | ||
| No | 7 (28) | 13 (19) | |
| Yes | 18 (72) | 56 (81) | |
| Comfortable in water to waist | .02 | ||
| No | 6 (24) | 4 (6) | |
| Yes | 19 (76) | 66 (94) | |
| Comfortable jumping into water over his/her head | .02 | ||
| No | 11 (44) | 15 (21) | |
| Yes | 14 (56) | 55 (79) | |
| Comfortable playing or swimming in water over his/her head | .007 | ||
| No | 12 (48) | 15 (22) | |
| Yes | 13 (52) | 54 (78) | |
| Swimming ability | |||
| Float on back for 10 s | .08 | ||
| No | 11 (42) | 20 (27) | |
| Yes | 15 (58) | 55 (73) | |
| Swim on stomach 15 ft | .003 | ||
| No | 14 (56) | 15 (19) | |
| Yes | 11 (44) | 62 (81) | |
| Jump in a pool/swim 5 ft/back to wall | .03 | ||
| No | 10 (40) | 15 (22) | |
| Yes | 15 (60) | 54 (78) | |
| Swim/take breath/continue | .03 | ||
| No | 10 (40) | 16 (21) | |
| Yes | 15 (60) | 61 (79) | |
| Swim 50 ft | .09 | ||
| No | 12 (52) | 23 (31) | |
| Yes | 11 (48) | 51 (69) | |
| Swim >1 min | .01 | ||
| No | 10 (42) | 12 (16) | |
| Yes | 14 (58) | 64 (84) | |
Characteristic of case or control, except where specified in headings.
Totals vary slightly because of missing data; percentage of distribution based on a denominator of those with information.
P value from the Wald statistic of a conditional logistic regression model containing only that variable.
All cases and controls in the 5- to 19-year age group were matched by sex; therefore, the P value is not applicable.
Asked only if the respondent lived with the child.
Assessed by asking how often the child received informal instructions, pointers, or tips about swimming or water safety when he or she went swimming.
Other factors associated with drowning risk (P < .10) included age of child, race, household income, and presence of a seizure disorder. (Because no controls were reported to have a seizure disorder, this variable was not included as a potential confounder in multivariable models.) Only income was retained as a confounder in the final adjusted model examining the association between formal swimming lessons and drowning risk. In this model, participation in formal swimming lessons was no longer a significant predictor of drowning risk (adjusted OR, 0.36; 95% CI, 0.09–1.51). No variables met our criteria for inclusion as a confounder in the model examining the association between informal swimming lessons and drowning risk. The unadjusted OR indicated no association between informal lessons and drowning risk (OR, 0.69; 95% CI, 0.27–1.77).
COMMENT
In this study, we found a protective association between past participation in formal swimming lessons and risk of drowning in children aged 1 to 4 years, with an adjusted OR of 0.12 and a 95% CI of 0.01 to 0.97. This can be interpreted as an 88% reduction in the risk of drowning among those with swimming lessons, with 95% confidence that a protective effect between 3% to 99% includes the true value. We found no statistically significant association between formal swimming lessons and drowning risk in older children or between informal swimming instruction and drowning risk at any age, although all of the estimated ORs were less than 1.
To our knowledge, this is the first study in the United States to examine the association between swimming lessons and drowning in children. However, a recent case-control study by Yang et al22 examined multiple potential risk factors for drowning in rural regions of China. In that study, cases, children aged 1 to 14 years who died of drowning between 2002–2004, were compared with age- and sex-matched controls, children selected from households in districts adjacent to that of the matched case. In adjusted analyses, Yang et al reported a protective effect of “proper” swimming lessons in the 1- to 4-year age group, with an OR of 0.6, indicating a 40% reduction in drowning risk. Similar to our study, the estimate was imprecise, with CIs that indicated that the true protective effect in that study could range from 10% to 80%. Also consistent with our findings, the study by Yang et al did not identify a significant association between participation in formal swimming lessons and drowning among older children. We identified no other studies that have examined effects of either formal lessons or informal lessons on drowning risk.
Limitations of our study include the relatively small sample size, particularly in the older age group. The wide CIs in our study were due largely to the small sample size and, in the 1- to 4-year age group, the small number of cases who had participated in formal swimming lessons. Further, we were able to interview next of kin for only 38% of identified drowning deaths in the 1- to 4-year age group and 26% in the 5- to 19-year age group. While there was no strong evidence that participants differed greatly from nonparticipants, we cannot rule out biases that this may have caused in our results.
Previous concerns have been raised about the potential for swimming lessons to increase the risk of drowning, either through increased exposure to water or through decreased parental vigilance as parents become more confident in their child’s swimming ability.23–26 In combination, the results of our study and the study by Yang et al provide reassurance that swimming lessons do not increase drowning risk. In the 1- to 4-year age group, lessons are likely to offer some protection, although the imprecision of estimates in both studies makes it difficult to draw conclusions about the true size of any effect.
Our study did not provide information about the mechanism through which swimming lessons exert their effect. While it seems reasonable to assume that at least part of the protective effect is through increased swimming skills, and studies have shown that these skills can be taught at a young age,26–28 swimming skills alone are insufficient to protect a child from drowning. In our study, many of the children who drowned, particularly in the older age group, were relatively skilled swimmers. For example, respondents reported that 48% of cases aged 5 to 19 years could swim 50 ft or more and 58% could swim continuously for at least a minute. Parents and caregivers who choose to enroll their children in swimming lessons should be cautioned that this alone will not prevent drowning and that even the most proficient swimmers can drown.
To enable researchers to replicate these findings, we recommend collection of information about swimming ability and past participation in formal swimming lessons as part of the routine investigation of all childhood drowning deaths. In the absence of uniform reporting of this information by all medical examiners and coroners, it will be difficult to collect this type of data on a larger sample. In combination with other prevention strategies, such as pool fencing, appropriate adult supervision, and training in cardiopulmonary resuscitation, swimming instruction can now be viewed as a potential component of a multi-faceted approach to prevention for younger children.
Acknowledgments
Funding Support: This work was supported by the National Institute of Child Health and Human Development under contract N01-HD-2-3341. Complete or partial salary support for Drs Brenner, Taneja, Haynie, Trumble, and Klebanoff was provided from National Institute of Child Health and Human Development intramural funds.
Footnotes
Author Contributions: Drs Brenner and Trumble and Mr Qian had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Brenner, Taneja, Haynie, and Klebanoff. Acquisition of data: Brenner, Taneja, and Klinger. Analysis and interpretation of data: Brenner, Taneja, Haynie, Trumble, Qian, and Klebanoff. Drafting of the manuscript: Brenner and Taneja. Critical revision of the manuscript for important intellectual content: Brenner, Taneja, Haynie, Trumble, Qian, Klinger, and Klebanoff. Statistical analysis: Trumble, Qian, and Klebanoff. Obtained funding: Brenner, Taneja, and Kle-banoff. Administrative, technical, and material support: Brenner, Taneja, and Klinger. Study supervision: Brenner and Taneja.
Financial Disclosure: None reported.
Additional Contributions: Wenyu Sun, MD, MPH, assisted with data analyses. We thank staff from the medical examiner and coroner offices for assisting in carrying out this important study. To compensate medical examiners’ offices and their staff for time and effort related to this study, each office was offered a one-time payment of $1500 and $25 for each reported case. This $25 per case payment was offered irrespective of case eligibility or whether the staff from the medical examiner office had contact with the case’s family. Offices and individuals we would like to acknowledge include Maryland Office of the Chief Medical Examiner; North Carolina Office of the Chief Medical Examiner; Sacramento County Coroner’s Office, California; San Diego County Medical Examiner’s Office, California; Riverside County Sheriff-Coroner’s Office, California; Harris County Medical Examiner’s Office, Texas (Luis A. Sanchez, MD, chief medical examiner; Stacey Mitchell, MSN, RN, deputy chief forensic nurse investigator); Suffolk County Office of the Medical Examiner, New York (Charles V. Wetli, MD, chief medical examiner, and Robert M. Golden, RPA, chief forensic investigator); and in Florida, medical examiners’ offices in District 1, Districts 3 and 4; District 5; District 6; Districts 7 and 24, District 9; District 10 (Stephen J. Nelson, MA, MD, chief medical examiner); District 11 (Shermaine Tyler-Luke, supervisor, Forensic Investigation Bureau, and Audrey Fagan, forensic investigator); District 12; District 13 (Vernard Adams, MD and JeanPierre Bihorel); District 15; District 17 (Joshua A. Per-per, MD, chief medical examiner Broward County); District 20; and District 21 (Sam Johnson, chief forensic investigator; Brett Harding, forensic investigator; and Rebecca A. Hamilton, chief medical examiner). We also extend our sincere appreciation to the families who participated in this study.
References
- 1.Centers for Disease Control and Prevention National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) www.cdc.gov/ncipc/wisqars. Accessed August 16, 2008.
- 2.Quan L, Cummings P. Characteristics of drowning by different age groups. Inj Prev. 2003;9(2):163–168. doi: 10.1136/ip.9.2.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brenner RA, Committee on Injury, Violence, and Poison Prevention Prevention of drowning in infants, children, and adolescents. Pediatrics. 2003;112(2):440–445. doi: 10.1542/peds.112.2.440. [DOI] [PubMed] [Google Scholar]
- 4.Rivara FP, Grossman DC, Cummings P. Injury prevention: second of two parts. N Engl J Med. 1997;337(9):613–618. doi: 10.1056/NEJM199708283370907. [DOI] [PubMed] [Google Scholar]
- 5.Fergusson DM, Horwood LJ. Risks of drowning in fenced and unfenced domestic swimming pools. N Z Med J. 1984;97(767):777–779. [PubMed] [Google Scholar]
- 6.Pitt WR, Balanda KP. Childhood drowning and near-drowning in Brisbane: the contribution of domestic pools. Med J Aust. 1991;154(10):661–665. doi: 10.5694/j.1326-5377.1991.tb121253.x. [DOI] [PubMed] [Google Scholar]
- 7.Thompson DC, Rivara FP. Pool fencing for preventing drowning in children. Coch-rane Database Syst Rev. 2000;(2):CD001047. doi: 10.1002/14651858.CD001047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Logan P, Branche CM, Sacks JJ, Ryan G, Peddicord J. Childhood drownings and fencing of outdoor pools in the United States, 1994. Pediatrics. 1998;101(6):E3. doi: 10.1542/peds.101.6.e3. http://pediatrics.aappublications.org/cgi/content/full/101/6/e3. Accessed December 5, 2008. [DOI] [PubMed] [Google Scholar]
- 9.Gardner HG, Committee on Injury, Violence, and Poison Prevention Office-based counseling for unintentional injury prevention. Pediatrics. 2007;119(1):202–206. doi: 10.1542/peds.2006-2899. [DOI] [PubMed] [Google Scholar]
- 10.Committee on Sports Medicine and Fitness and Committee on Injury and Poison Prevention. Swimming programs for infants and toddlers. Pediatrics. 2000;105(4, pt 1):868–870. [PubMed] [Google Scholar]
- 11.Committee on Injury, Violence, and Poison Prevention. Prevention of drowning in infants, children, and adolescents. Pediatrics. 2003;112(2):437–439. doi: 10.1542/peds.112.2.437. [DOI] [PubMed] [Google Scholar]
- 12.Taneja GS, Brenner RA, Klinger R, Trumble AC, Qian C, Klebanoff M. Participation of next of kin in research following sudden, unexpected death of a child. Arch Pediatr Adolesc Med. 2007;161(5):453–456. doi: 10.1001/archpedi.161.5.453. [DOI] [PubMed] [Google Scholar]
- 13.Ward EM, Kramer S, Meadows AT. The efficacy of random digit dialing in selecting matched controls for a case-control study of pediatric cancer. Am J Epidemiol. 1984;120(4):582–591. doi: 10.1093/oxfordjournals.aje.a113920. [DOI] [PubMed] [Google Scholar]
- 14.Olson SH, Kelsey JL, Pearson TA, Levin B. Evaluation of random digit dialing as method of control selection in case-control studies. Am J Epidemiol. 1992;135(2):210–222. doi: 10.1093/oxfordjournals.aje.a116273. [DOI] [PubMed] [Google Scholar]
- 15.Rothman KJ, Greenland S. Precision and validity in epidemiologic studies. In: Rothman KJ, Greenland S, editors. Modern Epidemiology. 2. Philadelphia, PA: Lippincott Williams and Wilkins-Raven; 1998. pp. 115–134. [Google Scholar]
- 16.Speltz ML, Gonzales N, Sulzbacher S, Quan L. Assessment of injury risk in young children: a preliminary study of the Injury Behavior Checklist. J Pediatr Psychol. 1990;15(3):373–383. doi: 10.1093/jpepsy/15.3.373. [DOI] [PubMed] [Google Scholar]
- 17.Potts R, Martinez IG, Dedmon A, Schwarz L, DiLillo D, Swisher L. Brief report: cross-validation of the Injury Behavior Checklist in a school-age sample. J Pe-diatr Psychol. 1997;22(4):533–540. doi: 10.1093/jpepsy/22.4.533. [DOI] [PubMed] [Google Scholar]
- 18.Arnett J. Sensation seeking: a new conceptualization and a new scale. Pers Individ Dif. 1994;16(2):289–296. [Google Scholar]
- 19.Fullard W, McDevitt SC, Carey WB. Assessing temperament in one- to three-year-old children. J Pediatr Psychol. 1984;9(2):205–217. doi: 10.1093/jpepsy/9.2.205. [DOI] [PubMed] [Google Scholar]
- 20.Sewell J, Oberklaid F, Prior M, Sanson A, Kyrios M. Temperament in Australian toddlers. Aust Paediatr J. 1988;24(6):343–345. doi: 10.1111/j.1440-1754.1988.tb01385.x. [DOI] [PubMed] [Google Scholar]
- 21.Greenland S, Rothman KJ. Introduction to stratified analysis. In: Rothman KJ, Greenland S, editors. Modern Epidemiology. 2. Philadelphia, PA: Lippincott Williams and Wilkins-Raven; 1998. pp. 253–279. [Google Scholar]
- 22.Yang L, Nong QQ, Li CL, Feng QM, Lo SK. Risk factors for childhood drowning in rural regions of a developing country: a case-control study. Inj Prev. 2007;13(3):178–182. doi: 10.1136/ip.2006.013409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Smith GS. Drowning prevention in children: the need for new strategies. Inj Prev. 1995;1(4):216–217. doi: 10.1136/ip.1.4.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Barss P. Cautionary notes on teaching water safety skills. Inj Prev. 1995;1(4):218–219. doi: 10.1136/ip.1.4.218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moran K, Stanley T. Parental perceptions of toddler water safety, swimming ability and swimming lessons. Int J Inj Contr Saf Promot. 2006;13(3):139–143. doi: 10.1080/17457300500373572. [DOI] [PubMed] [Google Scholar]
- 26.Asher KN, Rivara FP, Felix D, Vance L, Dunne R. Water safety training as a potential means of reducing risk of young children’s drowning. Inj Prev. 1995;1(4):228–233. doi: 10.1136/ip.1.4.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Parker HE, Blanksby BA. Starting age and aquatic skill learning in young children: mastery of prerequisite water confidence and basic aquatic locomotion skills. Aust J Sci Med Sport. 1997;29(3):83–87. [PubMed] [Google Scholar]
- 28.Erbaugh SJ. Effects of aquatic training on swimming skill development of preschool children. Percept Mot Skills. 1986;62(2):439–446. doi: 10.2466/pms.1986.62.2.439. [DOI] [PubMed] [Google Scholar]