

Abstract
Abstract
These studies evaluated the 24-h forced expiratory volume in 1 sec (FEV1) profile of once-daily (QD) olodaterol compared to placebo and twice-daily (BID) formoterol in patients with moderate to very severe chronic obstructive pulmonary disease. In two replicate, randomized, double-blind, double-dummy, four-way crossover studies, patients received olodaterol 5 and 10 μg QD, formoterol 12 μg BID, or placebo for 6 weeks in addition to usual-care background maintenance therapy. Co-primary end points were FEV1 area under the curve from 0–12 h (AUC0–12) response (change from baseline) and FEV1 AUC from 12–24 h (AUC12–24) response after 6 weeks, with FEV1 AUC from 0–24 h response identified as a key secondary end point. Other secondary end points included FEV1 AUC from 0–3 h and trough FEV1 responses, as well as corresponding forced vital capacity responses. With both olodaterol doses, FEV1 increased to near-maximal 30 min post-morning dose, which was sustained over 24 h. FEV1 also increased within 30 min post-morning dose of formoterol and was sustained over 12 h; the second formoterol dose resulted in a further increase, sustained for an additional 12 h. FEV1 AUC0–12 and AUC12–24 responses with both QD olodaterol doses and BID formoterol were significantly greater than placebo at 6 weeks (P < .0001). Secondary end-point outcomes were consistent with those of the co-primary end points. These data, together with those from the wider phase III clinical program, provide evidence for the 24-h bronchodilator efficacy of olodaterol QD in this patient population.
Trial registry
ClinicalTrials.gov; NCT00931385 and NCT00932646.
Electronic supplementary material
The online version of this article (doi:10.1186/2193-1801-3-419) contains supplementary material, which is available to authorized users.
Introduction
Long-acting bronchodilators, such as long-acting β2-agonists (LABAs) and long-acting muscarinic antagonists, are the cornerstone of pharmacologic therapy for patients with chronic obstructive pulmonary disease (COPD) and are considered central to symptom management (Global Initiative for Chronic Obstructive Lung Disease 2013). The first long-acting bronchodilators available for maintenance treatment of COPD were the LABAs salmeterol and formoterol, which had a <24-h duration of action and so required twice-daily (BID) dosing (Global Initiative for Chronic Obstructive Lung Disease 2013). The development of newer LABAs, such as indacaterol, with a longer 24-h duration of action (Rodrigo & Neffen 2012) allows for a once-daily (QD) posology (Toy et al. 2011).
Olodaterol is a LABA (Bouyssou et al. 2010a) with high β2-receptor selectivity and a near full agonist response at the human β2-adrenoceptor (Bouyssou et al. 2010b). Effective 24-h bronchodilation with olodaterol in both asthma and COPD has been confirmed by single-dose studies (van Noord et al. 2011; O’Byrne et al. 2009) and studies over 4 weeks (Joos et al. 2012; O’Byrne et al. 2012; van Noord et al. 2009). The results of these phase II studies provided the rationale to further investigate 5 and 10 μg QD doses of olodaterol in a phase III clinical program.
The comprehensive olodaterol phase III clinical program was designed to evaluate multiple efficacy and safety end points in five sets of paired studies that between them assessed 48-week lung-function efficacy, symptomatic benefit, 24-h bronchodilator profile, and exercise capacity. All studies were conducted in replicate to independently authenticate outcomes (US Department of Health and Human Services et al. 1998).
The primary objective of the replicate studies presented here was to determine the 24-h forced expiratory volume in 1 sec (FEV1) profile of olodaterol 5 and 10 μg QD in comparison to placebo and formoterol 12 μg BID in patients with moderate to very severe (Global initiative for chronic Obstructive Lung Disease stage 2–4) COPD. Formoterol was chosen as the active comparator because QD LABAs were not available at the time these studies were conducted. These studies are complementary to two replicate pivotal studies that, as a secondary end point, measured FEV1 responses over 12 h in a subset of patients (NCT00782210 and NCT00782509) (Ferguson et al. 2013) and two replicate 6-week studies (NCT01040689 and NCT01040728) that assessed the 24-h profile of olodaterol QD vs tiotropium (Lange et al. 2013).
In the studies presented here, the study population was chosen to allow evaluation of the 24-h bronchodilation activity of olodaterol in patients closely representative of those in clinical practice, with specific attention given to disease severity, co-morbidities, and background therapies (European Medicines Agency 2012).
Methods
Study design
These were replicate, multicenter, randomized, double-blind, double-dummy, placebo-controlled, four-way crossover studies (registered with ClinicalTrials.gov: NCT00931385 [study 1222.24] and NCT00932646 [study 1222.25]) conducted in the US (Figure 1). Eligible patients who successfully completed a 2- to 6-week run-in period to ensure clinical stability received each of the following treatments in a random sequence: olodaterol 5 μg QD, olodaterol 10 μg QD, formoterol 12 μg BID, and placebo. Each administration of olodaterol comprised two actuations of the Respimat® inhaler QD, while formoterol was administered via Aerolizer® with each administration comprising one actuation BID. Each treatment period lasted for 6 weeks, with a 14-day washout in between. Patients were evaluated for 14 days following study completion. With the exception of LABAs, patients continued usual-care background COPD maintenance treatment, including short-acting muscarinic antagonists, long-acting muscarinic antagonists, inhaled corticosteroids, and xanthines, throughout the duration of these trials. Patients on LABAs were allowed to switch to short-acting muscarinic antagonists. Salbutamol (100 μg) was provided to all patients as rescue medication.
Figure 1.
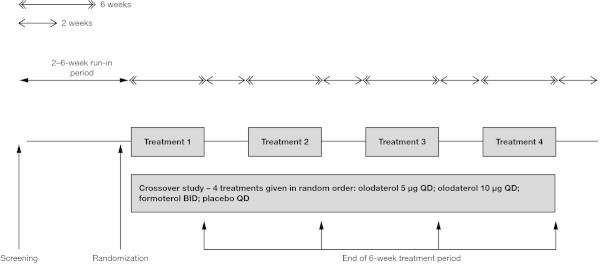
Study design. BID = twice daily; QD = once daily.
The study was approved by local ethics committees and carried out according to the Declaration of Helsinki and local regulations. Prior to study initiation, the protocol was approved by the local Institutional Review Board, Independent Ethics Committee, and the Competent Authority. All patients provided written, informed consent prior to the study commencing. Details of the local Institutional Review Boards are provided in Additional file 1: Table S1.
Patients
Patients were enrolled into the study if they met the following inclusion criteria: aged ≥40 years; current or ex-smokers with a smoking history of >10 pack-years; post-bronchodilator FEV1 < 80% of predicted normal; and post-bronchodilator FEV1/forced vital capacity (FVC) <70%. Key exclusion criteria were: significant disease other than COPD (defined by the investigator as a disease that may put the patient at risk by participating in the study, influence study outcomes, or cause concern with regards to the patient’s ability to participate in the study); history of asthma; history of myocardial infarction within 1 year of the screening visit; and unstable or life-threatening cardiac arrhythmia within the past year.
Study outcomes
The primary objective of the study was to determine if olodaterol 5 and 10 μg QD administered via the Respimat® inhaler provided superior 24-h bronchodilation vs placebo. A secondary objective was to compare the 24-h FEV1 time profile of QD olodaterol with that of BID formoterol. Co-primary end points were FEV1 area under the curve from 0 to 12 h (AUC0–12) response (defined as change from study baseline) and FEV1 AUC from 12 to 24 h (AUC12–24) response after 6 weeks of treatment. FEV1 AUC from 0 to 24 h (AUC0–24) response was identified as a key secondary end point. Other secondary efficacy variables included FEV1 measurements at individual time points over 24 h after 6 weeks of treatment, FEV1 AUC from 0 to 3 h (AUC0–3) response, peak FEV1 response, and trough FEV1 response. Corresponding FVC responses after 6 weeks were also measured. Safety end points included adverse events (AEs), vital signs, blood chemistry, and electrocardiogram.
Assessments
All qualifying pulmonary function tests (PFTs) (FEV1 and FVC) were conducted during the screening visit, and were started at approximately the same time of day for each patient (ie, between 7:00 AM and 9:00 AM; ±30 min maximal difference between the start of the tests on visit 2 and those conducted on subsequent test days). At the start of each treatment period, PFTs were conducted 60 min and 10 min before administration of the morning dose of study drug and at 30 min, 1, 2, and 3 h post-morning dose. Further PFTs were carried out at the end of each treatment period 30 min before administration of the morning dose and at 30 min, 1, 2, 3, 4, 6, 8, 10 h, 11 h 50 min, 12 h 30 min, and 13, 14, 22, 23 h, and 23 h 50 min post-morning dose of study drug (the evening dose of study drug was administered 12 h after the morning dose). Patients were required to stay overnight in the clinic or at a nearby hotel to ensure the quality and timing of PFTs at 22, 23 h, and 23 h 50 min post-dose on the second day of the 24-h PFT visit. All spirometric maneuvers were conducted in triplicate and performed according to American Thoracic Society/European Respiratory Society criteria (Miller et al. 2005). Daily trial medication and rescue medication use were recorded in paper diaries.
Safety end points were assessed in all patients who received at least one dose of study drug. All AEs, irrespective of causality, were monitored and recorded at each visit.
Statistical analysis
A sample size of 80 randomized patients provided 90% power to detect a treatment difference between olodaterol and placebo of 60 mL in FEV1 AUC0–12 and 51 mL in FEV1 AUC12–24, based on an estimated standard deviation of 0.160 and 0.140 L, respectively. The conservative randomized discontinuation was estimated to be 20%, resulting in 100 patients randomized.
The primary and secondary efficacy end points were based on the full analysis set, which included all patients with baseline data and evaluable post-dosing data for at least the first co-primary end point. Both primary and secondary end points were analyzed using a mixed-effects repeated measures model with terms for “center”, “patient within center”, “treatment”, and “period”. Analyses included the fixed categorical effects of “treatment”, “period”, and “random effect for patient”. Compound symmetry covariance structure was used to model within-patient variation. Analyses of AEs, laboratory data, and vital signs were descriptive in nature.
Results
Patient disposition and baseline characteristics
A total of 199 patients were randomized to treatment in both studies (Figure 2): 99 in study 1222.24 and 100 in study 1222.25. All patients were randomized between August 31 and September 15, 2009 (1222.24), and September 01 to 15, 2009 (1222.25) at different US sites involved in each study. All randomized patients received at least one dose of study drug and the majority (86%) completed all four treatment periods. There was a total of 24 occurrences of a patient discontinuing a treatment period (nine in study 1222.24 and 15 in study 1222.25), primarily due to AEs. Patients who discontinued from a treatment period were permitted to remain in the study and continue into the next treatment period. Patient demographics and baseline disease characteristics were well balanced across the studies (Table 1).
Figure 2.
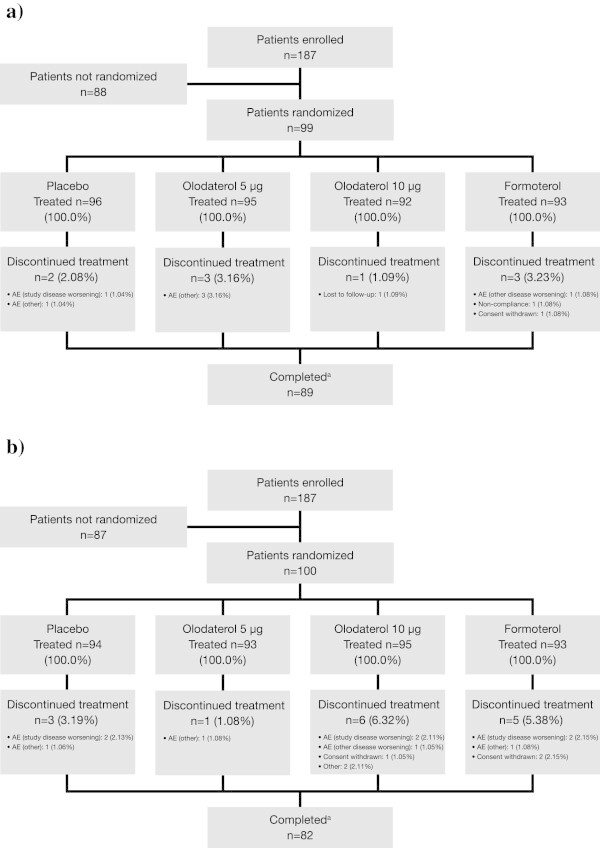
CONSORT diagram illustrating participant flow in (a) study 1222.24 and (b) study 1222.25. AE = adverse event. aAll patients who completed 4 treatment periods.
Table 1.
Baseline patient demographics and disease characteristics (treated set)
| Study 1222.24 | Study 1222.25 | |
|---|---|---|
| (n = 99) | (n = 100) | |
| Sex, n (%) | ||
| Male | 52 (52.5) | 54 (54.0) |
| Female | 47 (47.5) | 46 (46.0) |
| Age, mean (SD), years | 61.8 (8.9) | 63.5 (8.2) |
| COPD diagnosis, mean (SD), years | 7.4 (5.2) | 9.4 (7.9) |
| Pre-bronchodilator | ||
| Mean (SD) FEV1, L | 1.241 (0.451) | 1.242 (0.504) |
| Mean (SD) FEV1/FVC, % | 49.571 (11.562) | 48.673 (12.144) |
| Mean (SD) % of predicted normal FEV1 | 44.904 (13.908) | 46.010 (14.678) |
| Post-bronchodilator | ||
| Mean (SD) FEV1, L | 1.417 (0.494) | 1.439 (0.530) |
| Mean (SD) FEV1 change from | ||
| pre-bronchodilator, L | 0.177 (0.158) | 0.197 (0.158) |
| Mean (SD) FEV1/FVC, % | 50.224 (11.133) | 49.354 (11.460) |
| Mean (SD) % of predicted normal FEV1 | 51.368 (15.009) | 53.242 (14.706) |
| GOLD stage, n (%) | ||
| 2 | 51 (51.5) | 56 (56.0) |
| 3 | 39 (39.4) | 39 (39.0) |
| 4 | 9 (9.1) | 5 (5.0) |
| BMI, mean (SD), kg/m2 | 28.7 (7.7) | 27.8 (7.2) |
| Current smoker, n (%) | 60 (60.6) | 43 (43.0) |
| Smoking history, mean (SD), pack-years | 54.9 (24.8) | 51.2 (26.7) |
BMI = body mass index; COPD = chronic obstructive pulmonary disease; FEV1 = forced expiratory volume in 1 sec; FVC = forced vital capacity; GOLD = Global initiative for chronic Obstructive Lung Disease; SD = standard deviation.
Efficacy
The FEV1 time profiles for both doses of olodaterol were similar over 24 h (Figure 3). Mean FEV1 increased to near-maximal within 30 min and was sustained over the full 24-h post-dose evaluation period. Following the morning dose of formoterol, mean FEV1 also increased within 30 min and was comparable to both doses of olodaterol 0 to 3 h post-dose. The FEV1 time profile of formoterol intersected with the FEV1 time profile of both olodaterol doses at 4 h and was lower than the FEV1 responses observed with both doses of olodaterol 4 to 12 h post-dose. The evening dose of formoterol resulted in an additional increase in adjusted mean FEV1, which was sustained over the 12 to 24-h period (Figure 3).
Figure 3.
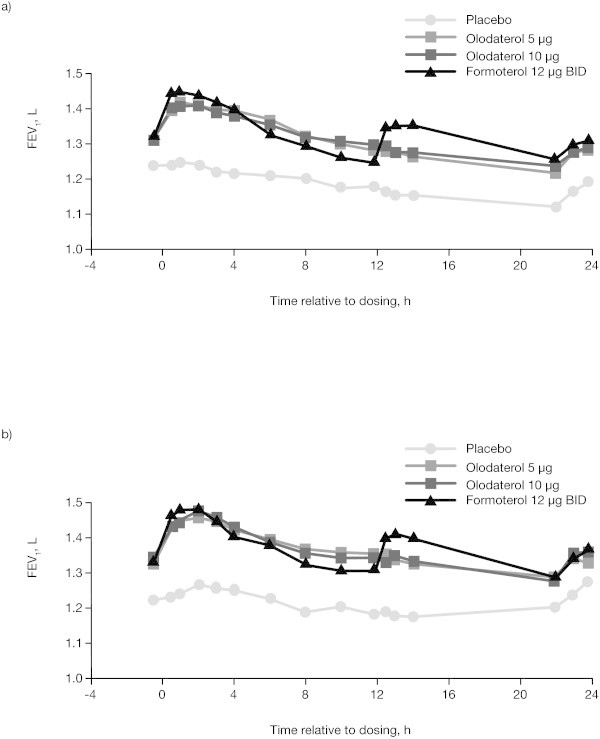
FEV 1 24-h profiles of olodaterol 5 and 10 μg and formoterol 12 μg BID compared to placebo at week 6 in (a) study 1222.24 and (b) study 1222.25. BID = twice daily; FEV1 = forced expiratory volume in 1 sec.
Primary and key secondary end points
In both studies, both primary end points of FEV1 AUC0–12 and AUC12–24 responses and the key secondary end point of FEV1 AUC0–24 response were significantly improved with olodaterol 5 μg QD, olodaterol 10 μg QD, and formoterol 12 μg BID compared to placebo (P < .0001) (Table 2). Pooled data showed no differences between olodaterol 5 and 10 μg QD compared to formoterol 12 μg BID for the FEV1 AUC0–12 response. However, the adjusted mean FEV1 AUC12–24 response for formoterol 12 μg BID was significantly greater than olodaterol 5 and 10 μg QD. For both FEV1 AUC0–12 and AUC12–24 responses, both doses of olodaterol were similar (Table 3). No statistically significant differences in FEV1 AUC0–24 responses were reported between all three active comparators (Table 3).
Table 2.
Adjusted mean FEV 1 AUC 0–12 , AUC 12–24 , and AUC 0–24 responses (L) compared to placebo after 6 weeks
| Treatment | Adjusted amean (95% CI) difference from placebo at 6 weeks | ||||
|---|---|---|---|---|---|
| FEV 1 AUC 0–12 | n | Adjusted mean (SE) | Mean (SE) | Pvalue | 95% CI |
| Study 1222.24 | |||||
| Placebo | 93 | −0.060 (0.020) | |||
| Olodaterol 5 μg QD | 92 | 0.088 (0.021) | 0.148 (0.018) | < .0001 | 0.113, 0.183 |
| Olodaterol 10 μg QD | 91 | 0.088 (0.021) | 0.148 (0.018) | < .0001 | 0.113, 0.183 |
| Formoterol 12 μg BID | 90 | 0.081 (0.021) | 0.141 (0.018) | < .0001 | 0.106, 0.177 |
| Study 1222.25 | |||||
| Placebo | 91 | −0.022 (0.024) | |||
| Olodaterol 5 μg QD | 92 | 0.150 (0.024) | 0.172 (0.017) | < .0001 | 0.139, 0.205 |
| Olodaterol 10 μg QD | 90 | 0.152 (0.024) | 0.174 (0.017) | < .0001 | 0.140, 0.208 |
| Formoterol 12 μg BID | 90 | 0.136 (0.024) | 0.158 (0.017) | < .0001 | 0.124, 0.191 |
| FEV 1 AUC 12–24 | |||||
| Study 1222.24 | |||||
| Placebo | 93 | −0.123 (0.021) | |||
| Olodaterol 5 μg QD | 92 | −0.014 (0.022) | 0.109 (0.019) | < .0001 | 0.073, 0.146 |
| Olodaterol 10 μg QD | 91 | 0.004 (0.022) | 0.127 (0.019) | < .0001 | 0.091, 0.164 |
| Formoterol 12 μg BID | 90 | 0.049 (0.022) | 0.172 (0.019) | < .0001 | 0.135, 0.209 |
| Study 1222.25 | |||||
| Placebo | 91 | −0.048 (0.025) | |||
| Olodaterol 5 μg QD | 92 | 0.069 (0.025) | 0.118 (0.018) | < .0001 | 0.082, 0.154 |
| Olodaterol 10 μg QD | 90 | 0.072 (0.025) | 0.120 (0.018) | < .0001 | 0.084, 0.157 |
| Formoterol 12 μg BID | 90 | 0.107 (0.025) | 0.155 (0.018) | < .0001 | 0.119, 0.191 |
| FEV 1 AUC 0–24 | |||||
| Study 1222.24 | |||||
| Placebo | 93 | −0.092 (0.020) | |||
| Olodaterol 5 μg QD | 92 | 0.037 (0.021) | 0.128 (0.017) | < .0001 | 0.094, 0.163 |
| Olodaterol 10 μg QD | 91 | 0.046 (0.021) | 0.137 (0.017) | < .0001 | 0.103, 0.172 |
| Formoterol 12 μg BID | 90 | 0.065 (0.021) | 0.156 (0.018) | < .0001 | 0.122, 0.191 |
| Study 1222.25 | |||||
| Placebo | 91 | −0.035 (0.024) | |||
| Olodaterol 5 μg QD | 92 | 0.110 (0.024) | 0.145 (0.016) | < .0001 | 0.114, 0.176 |
| Olodaterol 10 μg QD | 90 | 0.112 (0.024) | 0.147 (0.016) | < .0001 | 0.116, 0.179 |
| Formoterol 12 μg BID | 90 | 0.121 (0.024) | 0.156 (0.016) | < .0001 | 0.125, 0.187 |
AUC0–12 = area under the curve from 0 to 12 h; AUC0–24 = area under the curve from 0 to 24 h; AUC12–24 = area under the curve from 12 to 24 h; BID = twice daily; FEV1 = forced expiratory volume in 1 sec; SE = standard error.
aBased on a mixed effects repeated measures model. The model includes treatment and period as fixed effects and center and patient within center as random effects, along with compound symmetry as a covariance structure for within−patient variation.
Table 3.
Adjusted mean FEV 1 AUC 0–12 , FEV 1 AUC 12–24 , and FEV 1 AUC 0–24 responses (L); comparisons across active treatment arms after 6 weeks (pooled analysis)
| Treatment difference | ||||||
|---|---|---|---|---|---|---|
| FEV 1AUC 0–12 | Pvalue | FEV 1AUC 12–24 | Pvalue | FEV 1AUC 0–24 | Pvalue | |
| Mean (SE) | Mean (SE) | Mean (SE) | ||||
| Olodaterol 10 μg QD vs 5 μg QD | 0.001 (0.012) | .9527 | 0.010 (0.013) | .4423 | 0.005 (0.012) | .6474 |
| Olodaterol 10 μg QD vs formoterol 12 μg BID | 0.011 (0.012) | .3588 | −0.040 (0.013) | .0024 | −0.014 (0.012) | .2268 |
| Olodaterol 5 μg QD vs formoterol 12 μg BID | 0.011 (0.012) | .3876 | −0.050 (0.013) | .0001 | −0.020 (0.012) | .0944 |
AUC0–12 = area under the curve from 0 to 12 h; AUC0–24 = area under the curve from 0 to 24 h; AUC12–24 = area under the curve from 12 to 24 h; BID = twice daily; FEV1 = forced expiratory volume in 1 sec; QD = once daily; SE = standard error.
Secondary end points
There were statistically significant improvements in the peak FEV1 response for all active comparators compared to placebo (P < .0001) (Table 4). Pooled analysis demonstrated that there were no statistically significant differences in peak FEV1 responses between the two olodaterol doses; however, peak FEV1 response for both olodaterol 5 and 10 μg doses was significantly lower than formoterol (−0.036 and −0.034 L, respectively). Additionally, significant improvements in trough FEV1 and FEV1 AUC0–3 responses were observed with both doses of olodaterol and formoterol in comparison to placebo (Table 4).
Table 4.
Adjusted mean FEV 1 AUC 0–3 , peak FEV 1 , and trough FEV 1 responses (L) compared to placebo after 6 weeks
| Treatment | Adjusted amean (95% CI) difference from placebo at 6 weeks | ||||
|---|---|---|---|---|---|
| FEV 1 AUC 0–3 | n | Adjusted mean (SE) | Mean (SE) | Pvalue | 95% CI |
| Study 1222.24 | |||||
| Placebo | 93 | −0.030 (0.020) | |||
| Olodaterol 5 μg QD | 92 | 0.134 (0.021) | 0.164 (0.019) | < .0001 | 0.126, 0.201 |
| Olodaterol 10 μg QD | 91 | 0.135 (0.021) | 0.164 (0.019) | < .0001 | 0.127, 0.202 |
| Formoterol 12 μg BID | 90 | 0.168 (0.021) | 0.198 (0.019) | < .0001 | 0.160, 0.236 |
| Study 1222.25 | |||||
| Placebo | 91 | 0.004 (0.024) | |||
| Olodaterol 5 μg QD | 92 | 0.190 (0.025) | 0.186 (0.019) | < .0001 | 0.149, 0.223 |
| Olodaterol 10 μg QD | 90 | 0.202 (0.025) | 0.198 (0.019) | < .0001 | 0.162, 0.235 |
| Formoterol 12 μg BID | 90 | 0.217 (0.025) | 0.213 (0.019) | < .0001 | 0.176, 0.250 |
| Peak FEV 1 | |||||
| Study 1222.24 | |||||
| Placebo | 93 | 0.034 (0.022) | |||
| Olodaterol 5 μg QD | 92 | 0.208 (0.022) | 0.174 (0.020) | < .0001 | 0.135, 0.214 |
| Olodaterol 10 μg QD | 91 | 0.200 (0.022) | 0.166 (0.020) | < .0001 | 0.127, 0.206 |
| Formoterol 12 μg BID | 90 | 0.251 (0.022) | 0.218 (0.020) | < .0001 | 0.178, 0.257 |
| Study 1222.25 | |||||
| Placebo | 91 | 0.076 (0.026) | |||
| Olodaterol 5 μg QD | 92 | 0.268 (0.026) | 0.192 (0.019) | < .0001 | 0.154, 0.230 |
| Olodaterol 10 μg QD | 90 | 0.273 (0.026) | 0.197 (0.020) | < .0001 | 0.158, 0.235 |
| Formoterol 12 μg BID | 90 | 0.293 (0.026) | 0.217 (0.020) | < .0001 | 0.178, 0.255 |
| Trough FEV 1 | |||||
| Study 1222.24 | |||||
| Placebo | 93 | −0.093 (0.023) | |||
| Olodaterol 5 μg QD | 92 | 0.012 (0.024) | 0.106 (0.021) | < .0001 | 0.064, 0.147 |
| Olodaterol 10 μg QD | 91 | 0.020 (0.024) | 0.113 (0.021) | < .0001 | 0.072, 0.155 |
| Formoterol 12 μg BID | 90 | 0.040 (0.024) | 0.133 (0.021) | < .0001 | 0.092, 0.175 |
| Study 1222.25 | |||||
| Placebo | 91 | 0.012 (0.030) | |||
| Olodaterol 5 μg QD | 92 | 0.109 (0.030) | 0.097 (0.026) | .0003 | 0.045, 0.148 |
| Olodaterol 10 μg QD | 90 | 0.115 (0.030) | 0.103 (0.026) | .0001 | 0.051, 0.155 |
| Formoterol 12 μg BID | 90 | 0.093 (0.030) | 0.080 (0.026) | .0026 | 0.028, 0.132 |
AUC0–3 = area under the curve from 0 to 3 h; BID = twice daily; FEV1 = forced expiratory volume in 1 sec; QD = once daily; SE = standard error.
aBased on a mixed effects repeated measures model. The model includes treatment and period as fixed effects and center and patient within center as random effects, along with compound symmetry as a covariance structure for within−patient variation.
The corresponding FVC responses after 6 weeks’ treatment with olodaterol 5 and 10 μg QD and formoterol 12 μg BID were consistent with the FEV1 AUC responses and significantly improved vs placebo (Additional file 1: Tables S2–S4). In the pooled analysis, no statistically significant differences between olodaterol doses were observed for FVC AUC0–12, FVC AUC12–24, and FVC AUC0–24. Similar to FEV1 AUC12–24, the adjusted mean FVC AUC12–24 response for formoterol 12 μg BID was significantly greater than olodaterol 5 and 10 μg QD (−0.083 L [P = .0001] and −0.074 L [P = .0008], respectively, vs formoterol 12 μg BID). There were no other statistically significant differences in FVC AUC responses between the active treatment groups. FVC AUC0–12, AUC12–24, AUC0–24, and peak and trough FVC responses are shown in Additional file 1: Tables S2–S6, respectively.
Safety
Overall, 129 patients (64.8%) reported at least one AE during the studies. Incidence of AEs across active treatment groups was comparable. A total of 13 patients had AEs that were considered by the investigator to be related to study drug. The most frequently reported treatment-emergent AEs were COPD (17.6%) and upper respiratory tract infection (9.5%) (Table 5). Investigator-defined related AEs for each treatment group are shown in Additional file 1: Table S7. In total, 23 patients across both studies reported at least one serious AE, with the most frequently reported being COPD (three patients, study 1222.24; four patients, study 1222.25). Serious AEs in each treatment group are shown in Additional file 1: Table S7. One death in each study was reported: cardio-respiratory arrest (olodaterol 5 μg, study 1222.24) and respiratory failure (olodaterol 10 μg, study 1222.25). These were not considered by the investigator to be related to study treatment.
Table 5.
Frequency of AEs (pooled analysis)
| Pooled analysis | |||||
|---|---|---|---|---|---|
| Placebo | Olodaterol 5 μg | Olodaterol 10 μg | Formoterol 18 μg | Total | |
| (n = 190) | (n = 188) | (n = 187) | (n = 186) | (n = 199) | |
| Patients with any AE | 60 (31.6) | 61 (32.4) | 64 (34.2) | 49 (26.3) | 129 (64.8) |
| Patients with severe AEs | 11 (5.8) | 9 (4.8) | 6 (3.2) | 10 (5.4) | 28 (14.1) |
| Discontinuations due to AEs | 4 (2.1) | 4 (2.1) | 3 (1.6) | 3 (1.6) | 14 (7.0) |
| COPD | 12 (6.3) | 10 (5.3) | 9 (4.8) | 8 (4.3) | 35 (17.6) |
| Upper respiratory tract infection | 4 (2.1) | 5 (2.7) | 7 (3.7) | 7 (3.8) | 19 (9.5) |
| Bronchitis | 3 (1.6) | 7 (3.7) | 4 (2.1) | 4 (2.2) | 14 (7.0) |
| Cough | 1 (0.5) | 6 (3.2) | 1 (0.5) | 4 (2.2) | 12 (6.0) |
| Headache | 2 (1.1) | 2 (1.1) | 5 (2.7) | 2 (1.1) | 9 (4.5) |
| Sinusitis | 3 (1.6) | 1 (0.5) | 3 (1.6) | 3 (1.6) | 9 (4.5) |
| Urinary tract infection | 4 (2.1) | 0 | 4 (2.1) | 2 (1.1) | 9 (4.5) |
| Diarrhea | 1 (0.5) | 0 | 2 (1.1) | 2 (1.1) | 5 (2.5) |
| Nausea | 3 (1.6) | 1 (0.5) | 0 | 1 (0.5) | 5 (2.5) |
| Muscle spasms | 1 (0.5) | 1 (0.5) | 1 (0.5) | 2 (1.1) | 5 (2.5) |
| Chest pain | 2 (1.1) | 1 (0.5) | 2 (1.1) | 0 | 5 (2.5) |
| Pneumonia | 1 (0.5) | 0 | 2 (1.1) | 1 (0.5) | 4 (2.0) |
| Respiratory tract congestion | 3 (1.6) | 0 | 1 (0.5) | 0 | 4 (2.0) |
AE = adverse event; COPD = chronic obstructive pulmonary disease.
No changes indicative of an AE were observed for any laboratory parameters or vital signs with either dose of olodaterol, or formoterol.
Discussion
These replicate studies were designed to complement the evidence of long-term efficacy and safety provided by the pivotal 48-week studies in the olodaterol clinical trial program by evaluating the full 24-h FEV1 time profile of olodaterol 5 and 10 μg QD in comparison to placebo and formoterol 12 μg BID after chronic dosing.
FEV1 AUC0–12 and AUC12–24 were chosen as co-primary end points to allow a comparison between the different dosing regimens of olodaterol QD and formoterol BID. FEV1 AUC0–24 was included as a key secondary end point as it offered a comparison of the average 24-h FEV1 response between the active comparators.
This evaluation demonstrated that FEV1 AUC0–12, AUC12–24, and AUC0–24 responses were all significantly improved with both doses of olodaterol QD and formoterol BID vs placebo. There were distinct differences in the profiles of olodaterol and formoterol over the 24-h dosing interval, as might be expected given the different durations of action and consequent variations in dosing frequency; it should be noted that the methodology used likely overestimates the differences between active treatments. Nevertheless, FEV1 AUC0–24, a reflection of the mean bronchodilator effect over 24 h, was similar for both doses of olodaterol and formoterol. Similar differences in the 24-h FEV1 time profiles between QD and BID muscarinic antagonists have recently been observed in a trial comparing the 24-h bronchodilatory efficacy of aclidinium BID vs tiotropium QD in patients with moderate to severe COPD (Beier et al. 2013).
While these replicate studies measured lung function over a continuous 24-h dosing interval, there was a necessary pause in testing between 14 and 22 h post-dose to allow patients to have a relatively full night’s sleep. As such, it is to be noted that the calculation of FEV1 AUC12–24 in the study assumes a linear slope between 14 and 22 h post-dose for both olodaterol and formoterol. The FEV1 time profiles in Figure 3 clearly show a separation of formoterol and olodaterol as a result of the second peak for formoterol, 1 to 2 h after the evening dose. In contrast, between 22 and 24 h post-dose, the FEV1 time profiles for olodaterol and formoterol have converged. Due to the necessary pause in lung-function testing between 14 and 22 h post-dose, to allow patients to sleep, the precise time point at which this convergence occurred is not known.
The results for all other secondary outcomes supported those of the primary end points, with FVC responses mirroring FEV1 outcomes. The inclusion of peak FEV1 AUC0–3 and trough FEV1 measurements (at both ends of the daily dosing profile) provided further evidence to confirm the 24-h activity of olodaterol, with the ratio reflecting the degree of bronchodilation that is maintained at the end of the dosing interval in relation to the peak bronchodilation observed in the first hours after dosing. In addition, all FEV1 and FVC responses observed were in line with those expected for a patient population continuing with standard bronchodilation and corticosteroid maintenance therapy.
The outcomes from these replicate studies support those from earlier phase II trials employing similar end points, which demonstrated that single doses of olodaterol 5 and 10 μg QD provided effective and significant bronchodilation over a 24-h period (Joos et al. 2012; van Noord et al. 2009). Furthermore, the outcomes from these replicate studies add to the comprehensive set of evidence for the efficacy and safety of olodaterol QD in patients with COPD derived from the wider olodaterol phase III clinical program. A similar 12-h bronchodilation profile for olodaterol was observed in a subset of patients from two independent, 48-week, pivotal studies of olodaterol 5 and 10 μg QD in comparison with placebo (Ferguson et al. 2013). Additionally, outcomes from similar phase III, replicate, 6-week studies demonstrated that olodaterol 5 and 10 μg QD significantly improved FEV1 AUC0–12 and AUC12–24 responses compared to placebo, with a 24-h bronchodilator profile comparable to tiotropium (Lange et al. 2013).
A question that arises from the difference in the 24-h lung-function profiles of olodaterol QD and formoterol BID is whether the second evening peak in FEV1 with formoterol is associated with any improvements in night-time symptoms compared to olodaterol. This cannot be determined from our studies as no assessment of daytime and night-time symptoms was performed. However, two long-term, 48-week studies within the olodaterol phase III program were conducted using the BID comparator formoterol (Koch et al. 2013). Despite the second dose of formoterol being given in the evening, there were no differences between active treatments in night-time rescue medication usage at any time point in these studies (Boehringer Ingelheim, data on file). These data suggest that the evening peak in lung function with formoterol was not manifested in terms of advantages in night-time symptomatology.
Treatment with both doses of olodaterol and formoterol was well tolerated and incidence of AEs across treatment groups was comparable with the most commonly reported AEs: COPD and upper respiratory tract infection. In addition, safety outcomes in these studies were consistent with those reported in the pivotal studies.
Conclusions
These data, together with those from the wider phase III clinical program, provide evidence for the 24-h bronchodilator efficacy of olodaterol QD in patients with moderate to very severe COPD, with no differences in efficacy and tolerability observed between olodaterol 5 and 10 μg QD. Results from this study support the selection of the 5 μg dose for later use in clinical practice.
Electronic supplementary material
Additional file 1: Supplementary tables S1 to S7. (PDF 40 KB)
Acknowledgments
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. They take full responsibility for the scope, direction, content of, and editorial decisions relating to, the manuscript, were involved at all stages of development, and have approved the submitted manuscript. The authors received no compensation related to the development of the manuscript. This work was supported by Boehringer Ingelheim Pharma GmbH & Co. KG. Medical writing assistance was provided by Tanya Chaudry, PhD, of Complete HealthVizion, which was contracted and compensated by Boehringer Ingelheim Pharma GmbH & Co. KG.
Financial/Nonfinancial disclosures
The authors have reported the following conflicts of interest: Dr Feldman and Dr Bernstein have been Principal Investigators for pharmaceutical company studies. Dr Hamilton, Dr Nivens, and Mr Korducki are employees of Boehringer Ingelheim. Dr LaForce has no conflicts of interest.
Funding/Support
This work was supported by Boehringer Ingelheim Pharma GmbH & Co. KG.
Notation of prior abstract publication
European Respiratory Society Annual Congress, Barcelona, Spain, September 7–11, 2013.
Role of sponsors
These studies were funded by Boehringer Ingelheim. All data were interpreted by the authors.
Abbreviations
- AE
Adverse event
- AUC0–3
Area under the curve from 0 to 3 h
- AUC0–12
Area under the curve from 0 to 12 h
- AUC0–24
Area under the curve from 0 to 24 h
- AUC12–24
Area under the curve from 12 to 24 h
- BID
Twice daily
- COPD
Chronic obstructive pulmonary disease
- FEV1
Forced expiratory volume in 1 sec
- FVC
Forced vital capacity
- LABA
Long-acting β2-agonist
- QD
Once daily
- PFT
Pulmonary function test.
Footnotes
Competing interests
Dr Feldman: Principal Investigator for Boehringer Ingelheim. Dr Bernstein: Principal Investigator for Boehringer Ingelheim with funding provided to research center. Dr Hamilton, Dr Nivens and Mr Korducki: employees of Boehringer Ingelheim. Dr LaForce: no competing interest.
Authors’ contributions
Dr GJF: contributed to the study conception and design, provided oversight of the studies and analysis of the data, and was responsible for the drafting, review, and final approval of the manuscript. Dr JAB: served as Principal Investigator, participated in discussions regarding protocol design at investigator’s meeting, read and edited the manuscript. Dr AH: contributed to writing and implementing the protocol, overseeing the Principal Investigators, writing the clinical trial report, and approving the final manuscript. Dr MCN: contributed to writing and implementing the protocol, overseeing the Principal Investigators, writing the clinical trial report, and approving the final manuscript. Mr LK: contributed to the study conception and design, provided oversight of the studies and analysis of the data, and was responsible for the drafting, review, and final approval of the manuscript. Dr CLF: contributed to writing and implementing the protocol, overseeing the Principal Investigators, writing the clinical trial report, and approving the final manuscript. All authors read and approved the final manuscript.
Contributor Information
Gregory J Feldman, Email: gfeld3232@aol.com.
Jonathan A Bernstein, Email: BERNSTJA@UCMAIL.UC.EDU.
Alan Hamilton, Email: alan.hamilton@boehringer-ingelheim.com.
Michael C Nivens, Email: chad.nivens@boehringer-ingelheim.com.
Lawrence Korducki, Email: lawrence.korducki@boehringer-ingelheim.com.
Craig LaForce, Email: claforce@nccr.com.
References
- Beier J, Kirsten A-M, Mróz R, Segarra R, Chuecos F, Caracta C, Garcia Gil E. Efficacy and safety of aclidinium bromide compared with placebo and tiotropium in patients with moderate-to-severe chronic obstructive pulmonary disease: results from a 6-week, randomized, controlled Phase IIIb study. COPD. 2013;10:511–522. doi: 10.3109/15412555.2013.814626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bouyssou T, Casarosa P, Naline E, Pestel S, Konetzki I, Devillier P, Schnapp A. Pharmacological characterization of olodaterol, a novel inhaled β2-adrenoceptor agonist exerting a 24-hour-long duration of action in preclinical models. J Pharmacol Exp Ther. 2010;334:53–62. doi: 10.1124/jpet.110.167007. [DOI] [PubMed] [Google Scholar]
- Bouyssou T, Hoenke C, Rudolf K, Lustenberger P, Pestel S, Sieger P, Lotz R, Heine C, Büttner FH, Schnapp A, Konetzki I. Discovery of olodaterol, a novel inhaled β2-adrenoceptor agonist with a 24 h bronchodilatory efficacy. Bioorg Med Chem Lett. 2010;20:1410–1414. doi: 10.1016/j.bmcl.2009.12.087. [DOI] [PubMed] [Google Scholar]
- Guideline on clinical investigation of medicinal products in the treatment of chronic obstructive pulmonary disease (COPD) 2012. [Google Scholar]
- Ferguson G, Feldman G, Hofbauer P, Hamilton A, Allen L, Korducki L, Sachs P. Lung function efficacy of olodaterol QD delivered via Respimat in COPD patients: Results from two 48-week studies [abstract] Eur Respir J. 2013;42(Suppl 57):5s. [Google Scholar]
- Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2013. [Google Scholar]
- Joos G, Aumann JL, Coeck C, Korducki L, Hamilton AL, van Noord J. Comparison of 24-hour FEV1 profile for once-daily versus twice-daily treatment with olodaterol, a novel long-acting B2-agonist, in patients with COPD [abstract] Am J Respir Crit Care Med. 2012;185:abstract A2930. [Google Scholar]
- Koch A, Pizzichini E, Hamilton A, Hart L, Korducki L, De Salvo MC, Paggiaro P. Lung function efficacy of olodaterol QD delivered via Respimat versus placebo and formoterol BID in patients with COPD: two 48-week studies. Barcelona, Spain: Poster P764 presented at the European Respiratory Society Annual Congress; 2013. [Google Scholar]
- Lange P, Aumann J-L, Derom E, Hamilton A, Tetzlaff K, Ting N, van Noord JA. The 24-h FEV1 time profile of olodaterol QD delivered via Respimat® in COPD: Results from two 6-week studies [abstract] Eur Respir J. 2013;42(Suppl 57):982s. [Google Scholar]
- Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CPM, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J. Standardisation of spirometry. Eur Respir J. 2005;26:319–338. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- O’Byrne PM, van der Linde J, Cockcroft DW, Gauvreau GM, Brannan JD, FitzGerald M, Watson RM, Milot J, Davis B, O’Connor M, Hart L, Korducki L, Hamilton AL, Boulet L-P. Prolonged bronchoprotection against inhaled methacholine by inhaled BI 1744, a long-acting β2-agonist, in patients with mild asthma. J Allergy Clin Immunol. 2009;124:1217–1221. doi: 10.1016/j.jaci.2009.08.047. [DOI] [PubMed] [Google Scholar]
- O’Byrne PM, D’Urzo T, Gahlemann M, Hart L, Wang F, Beck E. Dose-finding study of once-daily treatment with olodaterol, a novel long-acting β2-agonist, in patients with asthma [abstract] Am J Respir Crit Care Med. 2012;185:abstract A3963. doi: 10.1186/s12931-015-0249-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodrigo GJ, Neffen H. Comparison of indacaterol with tiotropium or twice-daily long-acting β-agonists for stable COPD: a systematic review. Chest. 2012;142:1104–1110. doi: 10.1378/chest.11-2252. [DOI] [PubMed] [Google Scholar]
- Toy EL, Beaulieu NU, McHale JM, Welland TR, Plauschinat CA, Swensen A, Duh MS. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105:435–441. doi: 10.1016/j.rmed.2010.09.006. [DOI] [PubMed] [Google Scholar]
- Guidance for Industry: Providing Clinical Evidence of Effectiveness for Human Drug and Biological Products. 1998. [Google Scholar]
- van Noord JA, Korducki L, Hamilton A, Koker P. Four weeks once daily treatment with BI 1744 CL, a novel long-acting β2-agonist, is effective in COPD patients [abstract] Am J Respir Crit Care Med. 2009;179:abstract A6183. [Google Scholar]
- van Noord JA, Smeets JJ, Drenth BM, Rascher J, Pivovarova A, Hamilton AL, Cornelissen PJG. 24-hour bronchodilation following a single dose of the novel β2-agonist olodaterol in COPD. Pulm Pharmacol Ther. 2011;24:666–672. doi: 10.1016/j.pupt.2011.07.006. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Supplementary tables S1 to S7. (PDF 40 KB)