

Abstract
A 65-year-old man was referred to the respiratory clinic with recurrent chest infections on a background of stage 3 chronic obstructive pulmonary disease. On examination, there was wheeze bilaterally more marked on the left lower lobe. Subsequent imaging revealed an obstruction of the left main bronchus that was concerning for malignancy. Initially, on flexible bronchoscopy, a hard mass was found and multiple biopsies were positive for actinomycosis. Subsequent rigid bronchoscopy was undertaken and a set of dentures were removed from the airway.
Background
This is a case of a 65-year-old man who was treated for recurrent infective exacerbation of his chronic obstructive pulmonary disease (COPD) for a year. On chest X-ray and CT thorax, he had an obstructive lesion that was suspicious for lung cancer. Biopsies at flexible bronchoscopy showed actinomycosis. This case brings together respiratory, microbiology and cardiothoracic surgery.
Case presentation
A 65-year-old man was referred to the respiratory clinic with a 12-month history of recurrent chest infections, worsening dyspnoea and wheeze. He had been treated with multiple courses of antibiotics and steroids, but failed to improve. He had a background of COPD GOLD stage 3, (forced expiratory volume in 1 s 1.3 L, 43% predicted) and myocardial infarction with angioplasty 3 years previously. He was an ex-smoker with a 40 pack-year history. Clinical examination revealed no clubbing or lymphadenopathy; however, he did have bilateral wheeze more marked on the left lower lobe. Oxygen saturations were normal on room air.
Investigations
Chest X-ray showed left lower lobe consolidation (figure 1). A CT of the thorax revealed obstruction of the left main bronchus with distal air bronchograms, concerning for central malignancy (figure 2). Initial bronchoscopy demonstrated a mass occluding the distal left main bronchus 1.5 cm distal to the carina with prominent granulation tissue. Endobronchial sampling revealed actinomycosis with no malignant cells. He was referred to our hospital for a bronchoscopy with a view to endobronchial debulking via argon plasma coagulation. At bronchoscopy, proximal granulation tissue was removed to reveal a hard immobile foreign biopsy (figure 3). Actinomycosis was again cultured.
Figure 1.
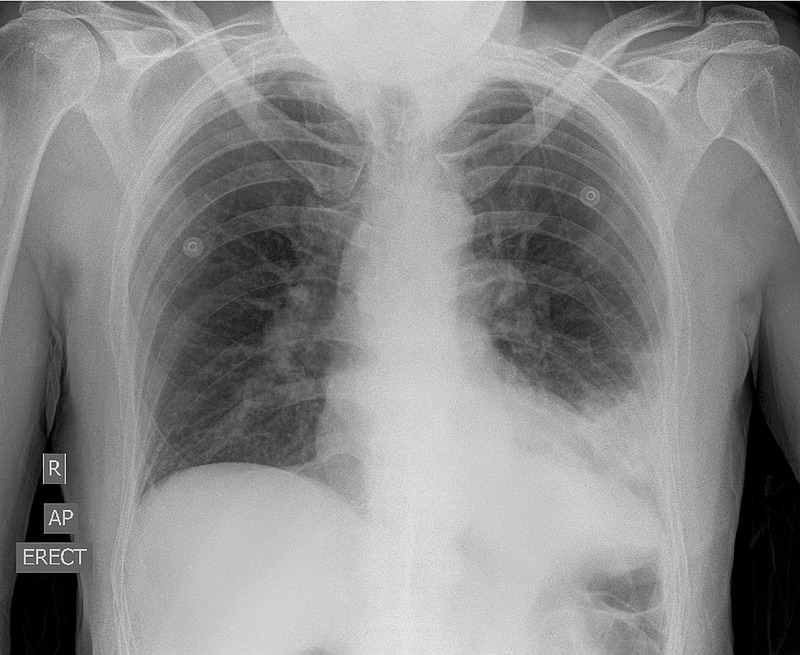
Chest X-ray: consolidation of the left lower lobe.
Figure 2.
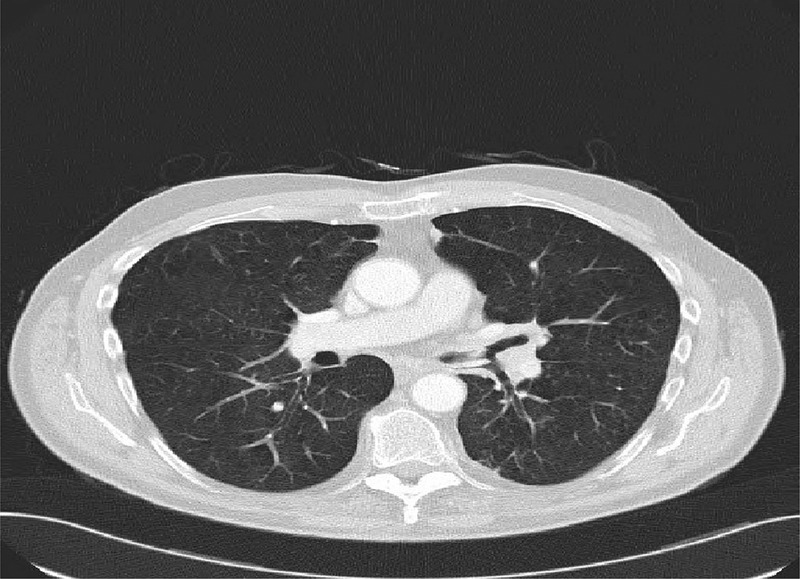
CT thorax: early emphysematous change with consolidation in the left lung and air bronchograms; however, a mass lesion could not be excluded.
Figure 3 .

Dentures visible on flexible bronchoscopy obstructing the left main bronchus 1.5 cm distal to the carina.
Differential diagnosis
Actinomycosis is a chronic suppurative anaerobic infection usually residing in the oropharynx or gastrointestinal tract. Endobronchial actinomycosis is rare and uncommon but when found it is generally in association with foreign body aspiration or necrotising pneumonias. It is usually acquired through inhalation, aspiration or haematogenous spread. Classic presentations are thoracic mass lesions, rib destruction and empyema. However, it can masquerade behind presumed bronchogenic malignancy and tuberculosis.
Treatment
On questioning he did admit that he had ‘mislaid’ his dentures 1 year previously. He was referred for rigid bronchoscopy where a set of dentures (figure 4) were removed.
Figure 4.

Partial dentures retrieved after rigid bronchoscopy.
Outcome and follow-up
His symptoms rapidly improved with clearance of his X-ray and reduced dyspnoea.
Discussion
In adults, foreign body aspiration is much less common than with children and it often is due to intoxication, general anaesthesia, neurological condition or sedation, and is often tolerated for much longer than it is in children.1 There is a diagnostic challenge when trying to take a history from a patient who may have aspirated or inhaled their dentures. Many patients may not recall that they have aspirated them and the denture plate and teeth are radiolucent making the identification on imaging much more difficult.2 Patients may have coexistent disease and this may delay in further investigating.
Learning points.
This case highlights the need to investigate patients with persistent and ongoing dyspnoea and recurrent infections despite having advanced chronic obstructive pulmonary disease.
Unilateral clinical and radiological signs should always be investigated.
A clinical and radiological diagnosis of malignancy should always be confirmed, if possible.
Aspiration in adults is not common and detection of aspirated dentures can be difficult as they are not radiopaque.3
An interesting aspect of this case was the detection of actinomycosis. This anaerobic bacteria can grow around a foreign body in an airway and mimic bronchogenic carcinoma.4 5 We suggest that the presence of this organism in the airway should prompt a thorough evaluation for foreign body.
Acknowledgments
Mr Ronan Ryan, Department of Cardiothoracic Surgery, St James’ Hospital, Dublin 8.
Footnotes
Contributors: MM and SJL were involved in conception of design and acquisition of data. MM was involved in analysis of data and drafting of the article. MPR, RKM and SJL were involved in critical revision of the article. SJL was involved in final approval of the article to be published.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Baharloo F, Veyckemans F, Francis C, et al. Tracheobronchial foreign bodies: presentation and management in children and adults. Chest 1999;115:1357–62 [DOI] [PubMed] [Google Scholar]
- 2.Hashmi S, Walter J, Smith W, et al. Swallowed partial dentures. J R Soc Med 2004;97:72–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chadwell JB, Mitchell JR, Donnino M, et al. Aspiration of radiolucent dentures in facial trauma: case report. Ear Nose Throat J 2010;89:E1. [DOI] [PubMed] [Google Scholar]
- 4.Yidiz O, Doganay M. Actinomycosis and nocardia pulmonary infections. Curr Opin Pulm Med 2006;12:228–34 [DOI] [PubMed] [Google Scholar]
- 5.Chouabe S, Perdu D, Deslee G, et al. Endobronchial actinomycosis associated with foreign body: four cases and a review of the literature. Chest 2002;121:2069–72 [DOI] [PubMed] [Google Scholar]