

Abstract
Hair and scalp disorders commonly seen in the African female have been associated with hair care practices. Distal trichorrhexis nodosa (TN) has been commonly reported with various forms of trauma to the hair from hair grooming practices. We report the case of recurrent generalized hair loss resulting from proximal TN in a 28-year-old Nigerian female with atopy. The use of chemical relaxers precipitated each episode of hair loss. Generalized proximal TN has been reported in those of afro Caribbean descent. The acute nature and extent of the hair loss suggest there may be some underlying structural defect in such individuals.
Keywords: Hear care practices, recurrent hair loss, trichorrhexis nodosa
INTRODUCTION
Hair loss in the African female is multifactorial in origin. It is dry, kinky and prone to fractures in its natural state.[1] Various hair grooming practices attempting to improve its appearance have also been implicated in hair loss.[2,3,4] Hair loss may result from scalp or hair shaft abnormalities induced by physical or chemical trauma. Trichorrhexis nodosa (TN) is a hair shaft abnormality precipitated by trauma. Although the distal type is commonly reported in those of African descent, we document the first case of recurrent generalized proximal TN in a Nigerian female with underlying atopy.
CASE REPORT
Report
A 28-year-old Nigerian female was seen in the clinic with three episodes of universal hair loss starting at the age of seven. Each episode was associated with the use of different chemical hair straighteners. Her hair grew back slowly to its usual length in between the episodes. Occasionally, she had some scaling of the scalp and gave a history of underlying atopy. There was no similar family history, no prior history of pruritus or involvement of other hair bearing areas. No associated history of deafness or routine drug use.
Examination showed a young lady with short and curly (natural) hair. There was reduced hair density in the occipital area. On performing a hair pull test a significant number of hairs broke easily. She had dry skin, hyperlinearity of her palms and normal nails.
Light microscopy of a few hairs randomly picked showed nodular thickening along some hair shafts and splitting of the hair shaft into fibers, trichoptilosis [Figure 1] mainly in the proximal part. Brush tip edges from fractures, trichoclasis [Figure 2] was also seen. A diagnosis of generalized proximal TN was made with underlying atopy.
Figure 1.
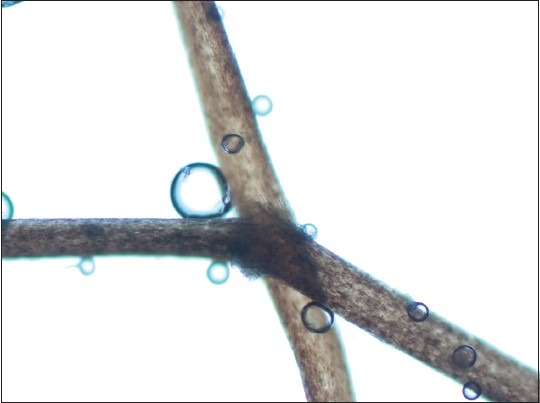
Hair shaft with fracture and nodular appearance at site of fracture
Figure 2.

Showing brush tip appearance of fractured proximal hair shaft
DISCUSSION
Trichorrhexis nodosa is a hair shaft defect due to increased fragility.[5] Commonly affects the hair on the scalp although there are reports of pubic, beard, and moustache involvement. It is commoner in those of Afro Caribbean descent possibly because of the hairstyling techniques.[6] The nodes represent areas of frayed cortical fibers that bulge out through a ruptured cuticle. It is associated with fractures and splitting of the hair shaft into many small fibers giving a brush tip appearance. Commonly, the disruption is distal resulting from weathering of the hair, as a result, of chemical, physical and thermal injury while grooming. TN has been reported in association with Netherthon's syndrome (atopic dermatitis, icthyosis, deafness), but there is no known association with atopic dermatitis alone. She was told to avoid the use of harsh grooming habits. There is a need to determine contributing, possible genetic factors to hair fragility in women who develop recurrent generalized proximal TA. The association of TA and atopy needs to be further investigated. This report emphasizes the need to examine the hair shafts of patients presenting with hair loss in our environment.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Steggerda M, Seiber HC. Size and shape of head hairs from six racial groups. Heredity. 1942;32:315–8. [Google Scholar]
- 2.Mirmirani P. Ceramic flat irons: Improper use leading to acquired trichorrhexis nodosa. J Am Acad Dermatol. 2010;62:145–7. doi: 10.1016/j.jaad.2009.01.048. [DOI] [PubMed] [Google Scholar]
- 3.Scott DA. Disorders of the hair and scalp in blacks. Dermatol Clin. 1988;6:387–95. [PubMed] [Google Scholar]
- 4.Papa CM, Mills OH, Jr, Hanshaw W. Seasonal trichorrhexis nodosa. Role of cumulative damage in frayed hair. Arch Dermatol. 1972;106:888–92. doi: 10.1001/archderm.106.6.888. [DOI] [PubMed] [Google Scholar]
- 5.Whiting DA, Dy LC. Office diagnosis of hair shaft defects. Semin Cutan Med Surg. 2006;25:24–34. doi: 10.1016/j.sder.2006.01.004. [DOI] [PubMed] [Google Scholar]
- 6.Sperling LC. Scarring alopecia and the dermatopathologist. J Cutan Pathol. 2001;28:333–42. doi: 10.1034/j.1600-0560.2001.280701.x. [DOI] [PubMed] [Google Scholar]