

Abstract
It has been noted that benign paroxysmal positional vertigo (BPPV) may be associated with certain disorders and medical procedures. However, most studies to date were done in Europe, and epidemiological data on the United States (US) population are scarce. Gender-based information is even rarer. Furthermore, it is difficult to assess the relative prevalence of each type of association based solely on literature data, because different comorbidities were reported by various groups from different countries using different patient populations and possibly different inclusion/exclusion criteria. In this study, we surveyed and analyzed a large adult BPPV population (n = 1,360 surveyed, 227 completed, most of which were recurrent BPPV cases) from Omaha, NE, US, and its vicinity, all diagnosed at Boys Town National Research Hospital (BTNRH) over the past decade using established and consistent diagnostic criteria. In addition, we performed a retrospective analysis of patients’ diagnostic records (n = 1,377, with 1,360 adults and 17 children). The following comorbidities were found to be significantly more prevalent in the BPPV population when compared to the age- and gender-matched general population: ear/hearing problems, head injury, thyroid problems, allergies, high cholesterol, headaches, and numbness/paralysis. There were gender differences in the comorbidities. In addition, familial predisposition was fairly common among the participants. Thus, the data confirm some previously reported comorbidities, identify new ones (hearing loss, thyroid problems, high cholesterol, and numbness/paralysis), and suggest possible predisposing and triggering factors and events for BPPV.
Introduction
The peripheral vestibular organ consists of miniature inertial accelerometers: the semicircular canals (SCCs) specialized in detecting angular acceleration, and the otolithic organs in sensing linear acceleration including gravitational changes. In benign paroxysmal positional vertigo (BPPV), according to the accepted theory, utricular otoconia break apart from the mass and become dislocated into the semicircular canals. Thereby, the canals are sensitized to gravity and generate false information of angular acceleration in response to head position changes with respect to gravity.
BPPV is the most common cause of vertigo. In young people, one third to one half of BPPV cases can be attributed to some type of head trauma/injury [1]–[5]. A number of surgery-induced BPPV cases, especially inner ear and dental surgeries, have also been reported [6]–[10]. In the absence of head trauma or mechanical impact (e.g. surgical drilling) to cause otoconia dislocation, BPPV is categorized as unknown origin or idiopathic. In middle aged and older people, idiopathic BPPV cases are much more common. It is becoming increasingly evident that idiopathic BPPV cases can be associated with other illnesses such as migraine [9], [11]–[16], vestibular neuritis [17], [18], Meniere’s disease [9], [19]–[21], sudden hearing loss [19], [22]–[27], diabetes [28], [29], and autoimmune thyroiditis [31]. BPPV has also been linked with reduced bone mineral density [32]–[34], suggesting that the spontaneous release of otoconia may parallel bone demineralization (for review see [30]).
Unfortunately, the methods of the reported epidemiological studies were not standardized, and possibly used different diagnostic and inclusion/exclusion criteria. Sometimes there is disagreement between reports whether BPPV is associated with some diseases/conditions. For example, Warninghoff et al [35] did not detect an increased prevalence of diabetes mellitus, arterial hypertension, migraine, other headaches or obesity in the BPPV patients compared to the control population, likely due to a small sample size (n = 19 BPPV patients). Given some inconsistencies in the comorbidity findings and the scarcity of epidemiological studies in the US, we surveyed and reviewed the medical records of a large BPPV patient population diagnosed and treated at BTNRH in the current study, and identified predisposing and triggering factors and events. Our long-term goal is to use the information as a starting point to study the pathophysiology of BPPV, as well as help improve or modify treatment and prevention strategies.
Materials and Methods
Study design and subjects
Diagnostic records of BPPV patients at the BTNRH Vestibular Clinic between 2002–2011 (n = 1,377, with 1360 adults and 17 children) were analyzed after patients’ information was de-identified and anonymized. The quoted numbers of patients in this study excluded a small subset that also had other types of vertigo/dizziness in addition to BPPV. Then, adult patients (n = 1,360) were directly surveyed using an anonymous questionnaire. Only the participants who completed the questionnaire in its entirety with evaluable data were included. A positive diagnosis of BPPV was the presence of nystagmus elicited in either the Dix-Hallpike or roll maneuver. The current study did not differentiate or exclude sub-types of BPPV, such as subjective BPPV [36] or BPPV sub-typed by location (posterior, lateral or superior canal) [37]. Our purpose was to investigate comorbidities that predispose an individual to freeing otoconia and not location of otoconia displacement; sub-typing would result in very small numbers in some sub-groups for statistical analysis.
All aspects of the study, including the retrospective analysis, the content of the survey, the invitation letter and the survey procedures, were reviewed and approved by the Institutional Review Board at BTNRH in accordance with institutional, federal and international guidelines (approval number 11-11-X). As described above, patients’ information was de-identified and anonymized prior to analysis. Since the retrospective analysis and the adult-only survey were done anonymously, no consent was necessary.
Procedures
Initially, a retrospective review of the medical records of the stated BPPV patient population was conducted, which provided preliminary information on comorbidities of BPPV and the rate of BPPV recurrence.
Then, a survey was created and administered through Survey Monkey (www.surveymonkey.com). Most questions required the participant to select one answer from two to several choices, with additional lines to add other information or explanation by the participant. When applicable, the choices included “I am not sure”, “I cannot remember” or “Does not apply”. The survey was divided into the following sub-sections:
Demographic information, including age (in years), sex, race, ethnicity, and general area of residence (urban/suburban or rural).
BPPV recurrence, family history, season of onset. Recurrence was defined in the survey as experiencing an additional episode of BPPV after being symptom-free for at least 30 days.
Events/illnesses immediately preceding BPPV onset, medical history, medications and diet. A table (see Results) contained a list of events/illnesses and asked whether the participant experienced them prior to BPPV. The “prior to” was arbitrarily defined as “less than 6 months before”. With the exception of head trauma, we speculated that other events/illnesses would not immediately result in BPPV, so we were looking for associations in a more loose time-locked fashion. The survey questions were asked as listed in the tables in the Results, except that the phrase “Did you experience xxx prior to your first BPPV symptom (or during your BPPV symptoms)” was included in each line item for each condition/disease in the survey. In the table, this phrase is summarized in the legend to save space.
In the medical history section, participants were given a comprehensive list of medical conditions to select from and blank lines to fill in any other medical conditions. Participants were asked to list their current medications, and to indicate whether their medical conditions and medication taken co-occurred with BPPV onset. Some questions regarding events/illnesses immediately preceding BPPV onset somewhat overlapped questions in the medical history section, thus serving as confirmation.
Frequency of consumption of alcohol, tobacco, caffeine, tea or carbonated beverages, high fat/sugary/salty foods, fresh fruits/vegetables, and meat/fish was filed as never, less than once a week, 2–3 times a week, or more than 3 times a week for each stated item. Consumption of special diet (e.g. vegetarian) was also asked.
An invitation letter to participate in the study was mailed to 1,360 adult BPPV patients. Participants had the option of completing the survey online or on paper. Some surveys were also distributed to new patients at the time when BPPV was diagnosed at BTNRH. All responses were downloaded into Excel, which served as the database for review and analysis.
For comparison, age- and gender-matched prevalence data on the general US population were obtained from the Center for Disease Control (CDC), the National Institute of Health (NIH), and peer-reviewed published papers. With a few diseases, control data on the general US population stratified by age and gender were not available, so European gender-based data on similar age groups were used. Such cases are indicated in the tables in the Results section.
Statistical analysis
The total number of participants who answered each question and the subtotals who gave one type of answer were tallied. When calculating the percentage of each subtotal over the total, those who answered “I am not sure”, “I cannot remember” or “It does not apply” were not included in the total or subtotal. The control statistics usually consisted of thousands to hundreds of thousands of people. To provide an estimate of the statistical significance of the difference in the disease prevalence between BPPV patients and the general population, p values were calculated for each comorbid disease using Fisher’s exact test. To simplify the analysis and to provide a conservative estimate of statistical significance, the control population size was set at 1,000 for all comorbidities, and the mean values from meta-analysis (if available) or the highest prevalence data available were used in the analysis.
The ages of the survey participants (n = 227) and the entire adult BPPV population (n = 1,360) were compared using Student’s t-test, and statistical significance of the effects of comorbid conditions on BPPV recurrence was evaluated using Fisher’s exact test. Familial cases of BPPV (a 2nd, 3rd and more cases of BPPV in blood relatives in a family) were compared with the highest reported prevalence (life-time prevalence) of BPPV in the general population using Fisher’s exact test.
Results
Demographics
Of the 1,360 total adult patients, 227 (164∶63 or 2.6∶1 female to male) completed the survey in its entirety. Characteristics of the two groups are summarized in Table 1 . The survey participants had an age and gender distribution similar to the entire patient population under invitation ( Figure 1 ), except that the former had slightly fewer people above 70 years old.
Table 1. Demographics of the study population.
| BPPV adult patient population | BPPV survey participants | ||||||
| N | Age range(years) | Mean age(years) | N | Age range(years) | Mean age(years) | P | |
| Female | 923 | 18–94 | 58.3±16.0 | 164 | 19–84 | 56.1±13.0 | 0.04 |
| Male | 437 | 18–91 | 60.2±15.7 | 63 | 30–86 | 56.4±15.2 | 0.0007 |
| Gender mixed | 1,360 | 18–94 | 58.9±15.9 | 227 | 19–86 | 56.2±13.6 | 0.006 |
Figure 1. Age and gender distribution of BPPV survey participants (n = 227 total) (A), BPPV cases diagnosed at BTNRH in 2002–2011 (n = 1,377 total) (B), and Nebraska population in year 2010 (n = 1,826,341 total) [73] (C). Recurrent cases are counted only once (the first occurrence).
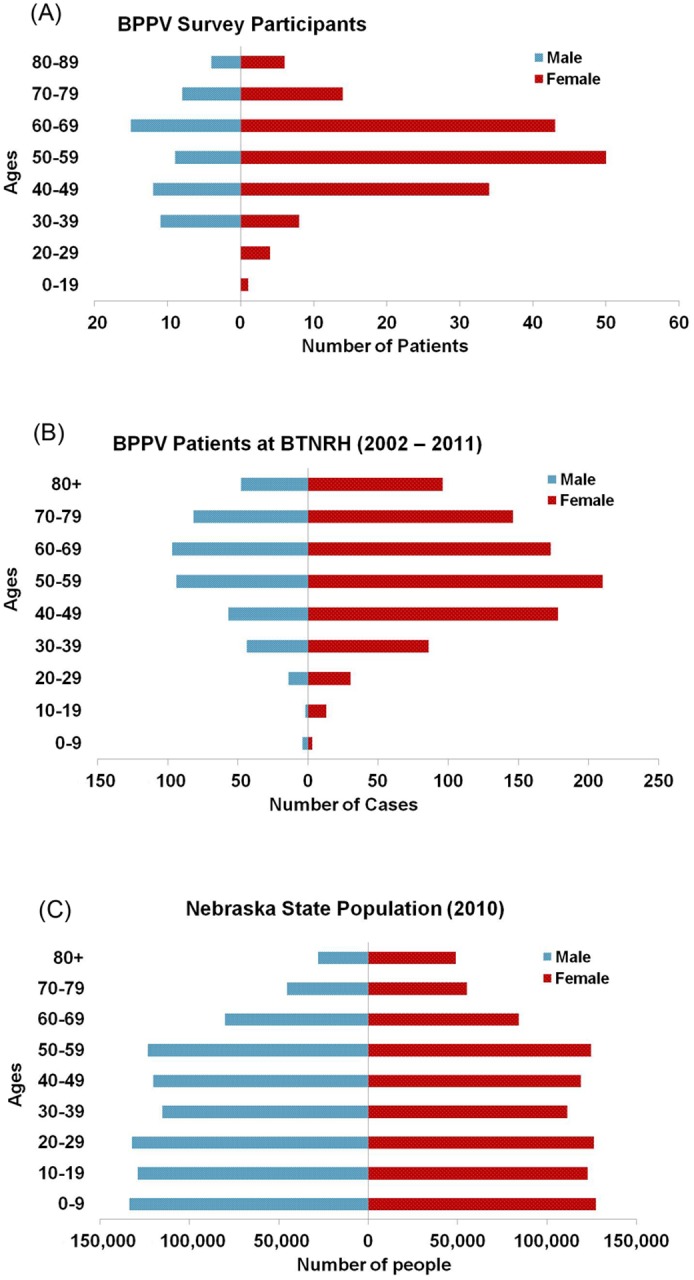
Among the survey participants, the ethnicity distribution was 80.9% “Not Hispanic or Not Latino”, and 19.1% “Hispanic or Latino”. The racial distribution was 95.8% White, 2.5% African American or Black, 1.3% Asian and 0.4% American Indian or Alaskan. Of the participants, 69.9% live in urban and suburban areas, 28.0% live in rural areas and 2.1% were not sure.
Recurrence of BPPV
In the BPPV survey population (n = 227), 174 participants (131 females and 43 males) reported recurrence of BPPV (53 non-recurrent cases), resulting in a recurrence rate of 76.3%. This is higher than the recurrence rates (27%–50%) reported by others [38], [39], [40], suggesting that recurrence may have been a strong motivation for participation.
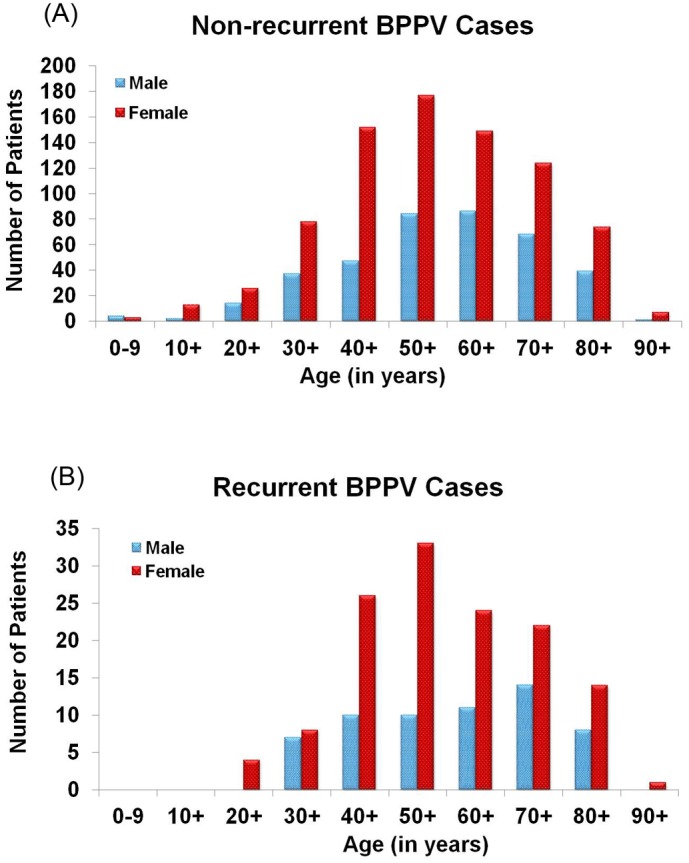
Among the entire BPPV population from 2002–2011 (n = 1,377), female recurrent and non-recurrent BPPV cases had a similar age distribution ( Figure 2 ), but male recurrent cases had an even greater age-related increase in the 70s group when compared to male non-recurrent cases. There were no recurrent female cases in the first 2 decades of life, and no recurrent male cases in the first 3 decades of life. In terms of recurrence, there was no significant difference between urban and rural dwellers, or in the frequencies of different types of diets or vitamin use. It could not be determined in the current study whether medication could have been a factor in BPPV occurrence or recurrence.
Figure 2. Age and gender distribution of non-recurrent (A, n = 1,185 total) and recurrent (B, 192 total) BPPV cases diagnosed at BTNRH from 2002–11.
Family history and other information
Among the survey participants, 23.8% (n = 54) reported having a known family member diagnosed with BPPV, 64.8% (n = 147) reported not having a family member with BPPV, and 11.4% (n = 26) did not know if any family member had BPPV. The affected family members were all blood-related except for 3 cases of non-genetic family members (spouses) who also had BPPV ( Table 2 ). The frequency of having a blood relative diagnosed with BPPV is significantly higher (p<0.0001) than the 2.4% life-time prevalence reported for the general population [41].
Table 2. Family history of BPPV.
| Family member | % of yes (n = 54 total) |
| Parents | 29.6% (n = 16) |
| Children | 14.8% (n = 9) |
| Siblings | 27.8% (n = 16) |
| Siblings and children | 1.9% (n = 1) |
| Parents & siblings | 11.1% (n = 6) |
| Grandparents/uncles/aunts/cousins | 7.4% (n = 4) |
| Spouse | 5.6% (n = 3) |
| No response | 1.9% (n = 1) |
Among the 68.4% (n = 227) of survey participants who remembered with certainty the season of BPPV onset, a higher percentage of participants had BPPV symptoms in the spring and fall: 28.2% in the spring, 18.0% in the summer, 28.9% in the fall, and 24.9% in the winter. Medical records showed that in the entire BPPV population, April and August had the highest number of cases at 11.0% and 10.7%, respectively. The higher incidences in the spring and fall implicate allergy in facilitating BPPV onset, which is supported by patients’ self-reported problems with allergy (see below).
Possible triggers and comorbidities of BPPV
When asked about incidents and conditions immediately preceding BPPV symptoms, most participants reported hearing loss ( Table 3 ). The next most common problem was headache associated with light and/or sound sensitivity and migraine, followed by infection. Most common infection was ear infection (28.6%, n = 10), sinus infection (28.6%, n = 10), and both (17.1%, n = 6).
Table 3. Incidents and conditions immediately preceding the first BPPV symptoms.
| Answers | Yes (n, %) | No (n, %) |
| Hearing loss | 93 (41.9%) | 129 (58.1%) |
| Any other ear problems | 14 (6.2%) | 211 (93.8%) |
| Current ear problems | 55 (24.3%) | 171 (75.7%) |
| Tinnitus | 6 (4.0%) | 144 (96.0%) |
| Headaches associated withincreased light/sound sensitivity | 47 (20.9%) | 178 (79.1%) |
| Migraine | 28 (12.4%) | 197 (87.6%) |
| Any infection | 37 (16.5%) | 187 (83.5%) |
| Any illness | 32 (14.3%) | 192 (85.7%) |
| Head injury | 27 (12.0%) | 198 (88.0%) |
| Other physical trauma | 13 (5.8%) | 212 (94.2%) |
| Any ear surgery | 13 (5.8%) | 212 (94.2%) |
| Any other surgery | 32 (14.3%) | 192 (85.7%) |
| Any other symptoms | 60 (27.0%) | 162 (73.0%) |
Only those who answered “yes” or “no” were included in the total or subtotal to obtain the percentages. Those who answered “does not apply” or “do not know/remember” were not included in the presented percentages.
In the Medical History section, the comprehensive list provided information on possible comorbidities and whether they co-occurred with BPPV, and confirmed those of the previous section in the survey ( Tables 4 & 5 ). Some differences in the answers may not be inconsistencies but may be the result of how the questions are phrased: one seeks information about the incidents/illnesses immediately preceding the first BPPV symptoms ( Table 3 ), while the second seeks information about their chronic situations that may or may not accompany the vertigo attacks ( Tables 4 & 5 ). Given the gender differences in comorbidities, male and female data were analyzed separately.
Table 4. Factors associated with BPPV in females.
| Comorbidities | Female BPPV patientsyes% (n out of 164 total) | General female population(set at n = 1,000) | P | References and notes for control data |
| Allergies | 50% (82) | 32.3%–35% (350) | 0.0003 | [56], [57] |
| Blood pressure | 38.4% (63) | 26.4–32.8% (328) | 0.18 | [58] |
| Ear/Hearing | 33.5% (55) | 12.7–14.4% (144) | <0.0001 | [58] Estimated based on gender ratio and data in 45–64 age group |
| Head injury | 8.5% (14) | 3.0% (30) | 0.003 | [59] Annual occurrence (0.3%) x 10 years |
| Headaches | 38.4% (63) | 17.0–38.0% (275) | 0.005 | [60], [61] Mean from meta-analysis; Chronic or repeated headaches were assumed |
| Heart | 17.7% (29) | 12.0% (120) | 0.058 | [58] Estimated from gender ratio |
| High cholesterol | 39.0% (64) | 31.0% (310) | 0.047 | [62] |
| Kidney/bladder | 10.4% (17) | 6.6% (66) | 0.10 | [58], [63] 1.8% chronic kidney diseases + 4.8% chronic bladder problems |
| Migraine | 26.2% (43) | 19.7% (197) | 0.06 | [64] |
| Numbness/Paralysis | 9.2% (15) | 5.6% (56) | 0.11 | [65], [66] Control on numbness (3.8%) only had stroke data (including mild stroke); on paralysis (1.8%) included injury cases |
| Thyroid | 21.3% (35) | 13.2% (132) | 0.008 | [67]–[69] Data on UK population |
The age- and gender-matched control statistics are on the general population in the size of thousands to hundreds of thousands. To simplify the analysis and to provide a conservative estimate of statistical significance, the control population size is set at 1,000 for all diseases for Fisher’s exact test in the table. If no mean prevalence data by meta-analysis are available, the highest prevalence data available for each disease in the control population is used to obtain the two-tailed p values. Significant (or nearly significant) comorbidities are bolded.
Table 5. Factors associated with BPPV in males.
| Comorbidities | Male BPPV patientsyes% (n out of 63 total) | General male population(set at n = 1,000 total) | P | References and notes for control data |
| Allergies | 38.1% (24) | 27.6% (276) | 0.08 | [57] Control are non-US population |
| Blood pressure | 44.4% (28) | 33.9% (339) | 0.10 | [58] |
| Cancer | 14.3% (9) | 9.5% (95) | 0.27 | [58] Estimated based on gender ratio and data in 45–64 age group |
| Ear/Hearing | 47.6% (30) | 23.4% (234) | <0.0001 | [58] Estimated based on gender ratio and data in 45–64 age group. |
| Head injury | 25.4% (16) | 4.0% (40) | <0.0001 | [59] Annual occurrence (0.4%) x 10 years |
| Headaches | 20.6% (13) | 12.5–31.0% (218) | 1.00 | [60] Mean from meta-analysis; Chronic or repeated headaches were assumed |
| High cholesterol | 50.8% (32) | 32.5% (325) | 0.004 | [62] |
| Kidney/bladder | 12.7% (8) | 6.8% (68) | 0.12 | [58], [63], [70], [71] 2.0% chronic kidney diseases + 4.8% chronic bladder problems |
| Migraine | 11.1% (7) | 7.0% (70) | 0.21 | [64] |
| Numbness/Paralysis | 14.3% (9) | 5.1% (51) | 0.007 | [65], [66] Control on numbness (3.0%) only had stroke data (including mild stroke); on paralysis (2.1%) included injury cases |
| Seizures | 4.8% (3) | 1.7% (17) | 0.11 | [72] |
| Thyroid | 11.1% (7) | 1.5% (15) | 0.0002 | [67]–[69] Data on UK population |
See Table 4 legend.
Among the 3 dozen listed categories of diseases and medical conditions, about a dozen had a different prevalence than that of the general population, with only some reaching significance ( Tables 4 & 5 ). Problems with the ear/hearing were again among the most common complaints in both genders. Incidences of headaches/migraine and head injury were also consistent with the previous question, and were common in females and males (especially young males), respectively. With male participants, the listed decades of life (1–9) had 0%, 0%, 0%, 45.5%, 23.1%, 36.4%, 21.4%, 0%, 25%, respectively, of head injury cases. With females, each decade had 0%, 0%, 1.7%, 20.0%, 6.0%, 5.4%, 15.8%, 0%, 0%, respectively, of head injury cases. When all age groups and genders were combined, the percentage of BPPV cases with head trauma was 12.4%, comparable to the reported range of 14%–18% in other BPPV populations [4], [29], [42], [43]. Because it has not been established that head and physical trauma in these patients were actually the cause of their BPPV (e.g. someone may have had head trauma and hearing loss at the same time), these participants were not excluded in the analysis of other comorbidities.
In both genders, problems with thyroid and high cholesterol were significantly more prevalent in the BPPV population ( Tables 4 & 5 ), although the comparison for thyroid diseases was made with control data from a large study conducted in the United Kingdom (UK) as age- and gender-matched data were not available on the US population.
In the BPPV female population, complaints of allergies and headaches were significantly more prevalent than in the control population. The former is consistent with above mentioned trend of BPPV occurring more frequently during allergy season. Musculoskeletal disorders (28.3%) were not more common in BPPV patients than the general population; however, it is unclear if the survey participants have had a bone scan, therefore, a negative answer to the question whether they had osteoporosis/osteopenia may not exclude the presence of the condition in some people.
Among the conditions that had a significantly higher prevalence in the BPPV population, some also appeared to increase disease recurrence ( Table 6 ); however, only numbness/paralysis reached statistical significance. Neither ear surgery nor head injury impacted BPPV recurrence significantly. Gender-separated analysis did not significantly improve the p values; it increased the p values with most of the comorbidities.
Table 6. Effects of comorbid conditions on BPPV recurrence.
| Comorbidities | RR | OR | P | N |
| Allergies | 0.94 | 0.77 | 0.43 | 76/27∶91/25 |
| Ear/Hearing problems | 1.12 | 1.64 | 0.15 | 74/17∶93/35 |
| High cholesterol | 1.10 | 1.54 | 0.20 | 75/18∶92/34 |
| Headaches | 0.98 | 0.93 | 0.87 | 55/18∶112/34 |
| Migraine | 1.08 | 1.41 | 0.44 | 38/9∶129/43 |
| Numbness/Paralysis | 1.29 | 7.34 | 0.03 | 21/1∶146/51 |
| Thyroid disease | 1.14 | 1.96 | 0.22 | 34/6∶133/46 |
| Physical trauma | 1.23 | 3.95 | 0.30 | 12/1∶155/51 |
The relative risk (RR) and odds ratio (OR) of BPPV recurrence in the presence vs. absence of a comorbid condition were calculated. The actual case numbers (N) are also presented in the order of recurrent/non-recurrent cases with and without the comorbid condition. Fisher’s exact test was used to obtain the two-tailed p values.
In the medical records of BPPV cases in 2002–2011 (n = 1,377), there were 67 cases of hearing loss (60 sensorineural hearing loss, 6 conductive, 1 unspecified sudden hearing loss), 20 hypoactive labyrinth, 10 migraine, 8 Meniere’s disease, 7 allergic rhinitis, 5 infective otitis externa, and 2 viral labyrinthitis. These comorbidities were reportedly co-occurring with BPPV at the time of the clinical visits, making them appear less prevalent than hearing loss reported in the survey. It is also possible that many patients did not mention their other medical conditions as vertigo was their primary concern during the clinical visits, or other diagnoses were not recorded.
Discussion
Due to the high prevalence and potentially incapacitating nature of BPPV, the present study examined factors that may predispose an individual to BPPV. We found a few significant comorbidities and familial predisposition for BPPV.
Notably, the number of cases with hearing loss is quite high among our BPPV patients, whereas previously reported numbers were quite low (less than 1%) [19], [44] except for incidences of sudden hearing loss. Sudden hearing loss has commonly been reported in BPPV patients, ranging from 9–51% [24]–[27], [45]; however, sudden hearing loss was rare among the BTNRH BPPV cases in the medical records (n = 1,377). Given that most of our BPPV patients are beyond middle age, we postulate that their hearing loss associated with BPPV is more likely caused by age-related degeneration, rather than by immune or inflammatory responses proposed as the cause of some cases of sudden hearing loss. This hypothesis would be in agreement with the observed effects of aging on BPPV in this population [46] and in other BPPV populations as well (for references see Introduction).
Nevertheless, our survey suggests that ear infection and inflammatory processes (infection and allergy) may also trigger BPPV. Increased incidences of sinus infections in other BPPV populations in the US have been noted [47]. Nasal allergies have also been associated with increased inner ear pathology [48]. The data suggest a possible association between allergies and BPPV onset, especially in women. Although our survey does not specify the type of allergies, nasal allergy is the most common type of allergies in the general population.
We also identified thyroid problems as a possible predisposing factor for BPPV occurrence. Thyroid problems disrupt the homeostasis of calcium and chloride [49], both of which affect otoconia in animal studies [50]–[52]. In addition, hypothyroidism delays the onset of inhibitory neurotransmission [49] during development. Although not yet examined in adults, if hypothyroidism also negatively affects inhibitory transmission in adulthood, it can lead to an imbalance of excitatory/inhibitory transmission. Indeed, autoimmune thyroiditis has been associated with BPPV [19], [30], [31].
Other previously unknown factors that we identified to be associated with BPPV include high cholesterol and numbness/paralysis. It is not clear how these and other factors in Tables 4 & 5 could be biologically linked to BPPV, but immobility may be a factor. For example, there are reports of BPPV possibly arising from bed-rest after surgeries which do not have mechanic impact on the ear or head [53].
In a concurrent study [46], we found that menopause is a major trigger of BPPV. Another common menopausal disease is osteoporosis and osteopenia. Although our data do not provide a definitive conclusion regarding the association of BPPV with osteoporosis or osteopenia, several other independent groups from different countries have reported significantly reduced bone mineral density and increased incidences of osteoporosis/osteopenia in BPPV patients [32]–[34]. Many other diseases can also be triggered or aggravated by menopause, such as allergies, high blood pressure, high cholesterol, headaches, migraine, heart diseases, and hearing loss [54], whether or not the condition shows a female preponderance in the overall prevalence. Most of these conditions showed a significantly higher prevalence in the BPPV patients than the age- and gender- matched controls (Table 4). Our survey data showed a possible association between migraine and BPPV when compared to the general population, and a strong association between generalized headache and BPPV. It is not clear if the higher migraine prevalence in BPPV patients reported by other investigators [16]; [12] reached statistics significance. Ishiyama et al. [12] noted a younger average age of onset and a higher recurrence rate of BPPV in patients with migraine than those without. Our migraine prevalence in BPPV patients may have been underestimated, because our survey invitation letter and an earlier part of the questionnaire emphasized a disease as “diagnosed”, so the participants likely only selected “yes” to migraine if they have been diagnosed. Also, BTNRH does not have a neurology specialty, and some patients with migraine may ignore their BPPV symptoms or not come to BTNRH clinics.
Our data confirm the previously noted familial predisposition in BPPV occurrence [55]. With the exception of 3 spousal cases, the affected family members are all genetic relatives. Anecdotally, vestibular clinicians have encountered twins who have lived apart but all have suffered BPPV (Janet O Helminski, personal communication). All these facts implicate a genetic contribution, not similar life styles or environment, in causing these familial BPPV incidences.
The survey response rate of 16% (18.5% when incomplete responses are counted) is reasonable because we had a long questionnaire, and the invitation letter was mailed on paper rather than emailed with a link (email is more convenient and could improve the response rate). As shown in Figure 1, the response is good representation of the entire BPPV population at BTNRH except for those above 70 years of age. Although comorbid diseases in very old patients may be missed, our findings may be more specific to BPPV rather than as a non-specific coincidence of aging. It should be noted that the majority of the participants were recurrent BPPV sufferers, therefore, the observed comorbidities may be somewhat biased toward BPPV recurrence even though most of the effects did not reach statistical significance (Table 6). Another potential bias of the study is that BTNRH is primarily an otolaryngology and pediatrics facility, and the patient data may over- or under-represent some comorbidities, such as hearing loss (possibly over), migraine (under), and high blood pressure (under). We anticipate such possibility to be small because these clinical visits at BTNRH were sought by patients for BPPV symptoms. Furthermore, certain conditions that showed a significantly higher prevalence in BPPV patients were also reported to occur shortly before the onset of BPPV (Table 3). When BPPV is consistently associated with certain diseases in studies done by independent groups using different patient populations, it would be important to conduct future studies to examine the biological mechanism and genetic predisposition to explain the link between these comorbidities and BPPV.
Conclusion
Our data show a significant effect of gender, familial predisposition, and certain conditions/diseases in BPPV etiology. Some of these associations (hearing loss, thyroid problems, high cholesterol, and numbness/paralysis) were previously unknown or are much higher than previously reported. When other investigators’ findings are also considered, it may be beneficial to the patients if clinicians diagnosing BPPV are alerted about potential comorbid conditions and consider screening these patients or checking their medical history for the following conditions: hearing loss, head injury, thyroid, lipid, allergies, headaches, diabetes, bone density, and family history.
Acknowledgments
We thank Kendra K. Schmid for statistical consultation, Walt Jesteadt for feedback on the manuscript, Susan J. Grennan and Hongyang Tan for help with some Excel analysis, and Rebecca Cash for help with the IRB application process.
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
Funding Statement
This work was supported by grants from the National Institutes of Health, R01DC008603, R01DC008603-S1, and P20GM103471 (formerly P20RR018788) pilot funding to YWL; postdoctoral training grant T32DC000013 to OAO; and P20GM103471 pilot funding to ESC. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Ahn SK, Jeon SY, Kim JP, Park JJ, Hur DG, et al. (2011) Clinical characteristics and treatment of benign paroxysmal positional vertigo after traumatic brain injury. J Trauma 70: 442–446. [DOI] [PubMed] [Google Scholar]
- 2. Blessing R, Strutz J, Beck C (1986) Epidemiology of benign paroxysmal positional vertigo. Laryngol Rhinol Otol (Stuttg) 65: 455–458. [PubMed] [Google Scholar]
- 3. Dispenza F, De SA, Mathur N, Croce A, Gallina S (2011) Benign paroxysmal positional vertigo following whiplash injury: a myth or a reality? Am J Otolaryngol 32: 376–380. [DOI] [PubMed] [Google Scholar]
- 4. Katsarkas A (1999) Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol 119: 745–749. [DOI] [PubMed] [Google Scholar]
- 5. Suarez H, Alonso R, Arocena M, Suarez A, Geisinger D (2011) Clinical characteristics of positional vertigo after mild head trauma. Acta Otolaryngol 131: 377–381. [DOI] [PubMed] [Google Scholar]
- 6. Viccaro M, Mancini P, La GR, De SE, Covelli E, et al. (2007) Positional vertigo and cochlear implantation. Otol Neurotol 28: 764–767. [DOI] [PubMed] [Google Scholar]
- 7. Andaz C, Whittet HB, Ludman H (1993) An unusual cause of benign paroxysmal positional vertigo. J Laryngol Otol 107: 1153–1154. [DOI] [PubMed] [Google Scholar]
- 8. Atacan E, Sennaroglu L, Genc A, Kaya S (2001) Benign paroxysmal positional vertigo after stapedectomy. Laryngoscope 111: 1257–1259. [DOI] [PubMed] [Google Scholar]
- 9. Hughes CA, Proctor L (1997) Benign paroxysmal positional vertigo. Laryngoscope 107: 607–613. [DOI] [PubMed] [Google Scholar]
- 10. Kaplan DM, Hehar SS, Tator C, Guha A, Laperriere N, et al. (2003) Hearing loss in acoustic neuromas following stereotactic radiotherapy. J Otolaryngol 32: 23–32. [DOI] [PubMed] [Google Scholar]
- 11. Lanzi G, Balottin U, Fazzi E, Tagliasacchi M, Manfrin M, et al. (1994) Benign paroxysmal vertigo of childhood: a long-term follow-up. Cephalalgia 14: 458–460. [DOI] [PubMed] [Google Scholar]
- 12. Ishiyama A, Jacobson KM, Baloh RW (2000) Migraine and benign positional vertigo. Ann Otol Rhinol Laryngol 109: 377–380. [DOI] [PubMed] [Google Scholar]
- 13. Thakar A, Anjaneyulu C, Deka RC (2001) Vertigo syndromes and mechanisms in migraine. J Laryngol Otol 115: 782–787. [DOI] [PubMed] [Google Scholar]
- 14. Uneri A (2004) Migraine and benign paroxysmal positional vertigo: an outcome study of 476 patients. Ear Nose Throat J 83: 814–815. [PubMed] [Google Scholar]
- 15. Marcelli V, Piazza F, Pisani F, Marciano E (2006) Neuro-otological features of benign paroxysmal vertigo and benign paroxysmal positioning vertigo in children: a follow-up study. Brain Dev 28: 80–84. [DOI] [PubMed] [Google Scholar]
- 16. Von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, et al. (2007) Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry 78: 710–715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Mandala M, Santoro GP, Awrey J, Nuti D (2010) Vestibular neuritis: recurrence and incidence of secondary benign paroxysmal positional vertigo. Acta Otolaryngol 130: 565–567. [DOI] [PubMed] [Google Scholar]
- 18. Parnes LS, Agrawal SK, Atlas J (2003) Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ 169: 681–693. [PMC free article] [PubMed] [Google Scholar]
- 19. Karlberg M, Hall K, Quickert N, Hinson J, Halmagyi GM (2000) What inner ear diseases cause benign paroxysmal positional vertigo? Acta Otolaryngol 120: 380–385. [DOI] [PubMed] [Google Scholar]
- 20. Wu ZM, Zhang SZ, Liu XJ, Chen X, Ji F, et al. (2007) Benign paroxysmal positioning vertigo related to inner ear disorders. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 42: 821–825. [PubMed] [Google Scholar]
- 21. Gross EM, Ress BD, Viirre ES, Nelson JR, Harris JP (2000) Intractable benign paroxysmal positional vertigo in patients with Meniere’s disease. Laryngoscope 110: 655–659. [DOI] [PubMed] [Google Scholar]
- 22. Rambold H, Heide W, Helmchen C (2004) Horizontal canal benign paroxysmal positioning vertigo with ipsilateral hearing loss. Eur J Neurol 11: 31–35. [DOI] [PubMed] [Google Scholar]
- 23.Mizukoshi K, Watanabe Y, Shojaku H, Okubo J, Watanabe I (1988) Epidemiological studies on benign paroxysmal positional vertigo in Japan. Acta Otolaryngol Suppl 447: 67–72. [DOI] [PubMed]
- 24.Park HM, Jung SW, Rhee CK (2001) Vestibular diagnosis as prognostic indicator in sudden hearing loss with vertigo. Acta Otolaryngol Suppl 545: 80–83. [PubMed]
- 25. Kim MB, Ban JH (2012) Benign paroxysmal positional vertigo accompanied by sudden sensorineural hearing loss: a comparative study with idiopathic benign paroxysmal positional vertigo. Laryngoscope 122: 2832–2836. [DOI] [PubMed] [Google Scholar]
- 26. Song JJ, Yoo YT, An YH, Yoo JC, Kim JS, et al. (2012) Comorbid benign paroxysmal positional vertigo in idiopathic sudden sensorineural hearing loss: an ominous sign for hearing recovery. Otol Neurotol 33: 137–141. [DOI] [PubMed] [Google Scholar]
- 27. Lee NH, Ban JH, Lee KC, Kim SM (2010) Benign paroxysmal positional vertigo secondary to inner ear disease. Otolaryngol Head Neck Surg 143: 413–417. [DOI] [PubMed] [Google Scholar]
- 28. Papi G, Guidetti G, Corsello SM, Di DC, Pontecorvi A (2010) The association between benign paroxysmal positional vertigo and autoimmune chronic thyroiditis is not related to thyroid status. Thyroid 20: 237–238. [DOI] [PubMed] [Google Scholar]
- 29. Cohen HS, Kimball KT, Stewart MG (2004) Benign paroxysmal positional vertigo and comorbid conditions. ORL J Otorhinolaryngol Relat Spec 66: 11–15. [DOI] [PubMed] [Google Scholar]
- 30. Lee SH, Kim JS (2010) Benign paroxysmal positional vertigo. J Clin Neurol 6: 51–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Modugno GC, Pirodda A, Ferri GG, Montana T, Rasciti L, et al. (2000) A relationship between autoimmune thyroiditis and benign paroxysmal positional vertigo? Med Hypotheses 54: 614–615. [DOI] [PubMed] [Google Scholar]
- 32. Vibert D, Kompis M, Hausler R (2003) Benign paroxysmal positional vertigo in older women may be related to osteoporosis and osteopenia. Ann Otol Rhinol Laryngol 112: 885–889. [DOI] [PubMed] [Google Scholar]
- 33. Jang YS, Kang MK (2009) Relationship between bone mineral density and clinical features in women with idiopathic benign paroxysmal positional vertigo. Otol Neurotol 30: 95–100. [DOI] [PubMed] [Google Scholar]
- 34. Jeong SH, Choi SH, Kim JY, Koo JW, Kim HJ, et al. (2009) Osteopenia and osteoporosis in idiopathic benign positional vertigo. Neurology 72: 1069–1076. [DOI] [PubMed] [Google Scholar]
- 35. Warninghoff JC, Bayer O, Ferrari U, Straube A (2009) Co-morbidities of vertiginous diseases. BMC Neurol 9: 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Buki B, Simon L, Garab S, Lundberg YW, Junger H, et al. (2011) Sitting-up vertigo and trunk retropulsion in patients with benign positional vertigo but without positional nystagmus. J Neurol Neurosurg Psychiatry 82: 98–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Cambi J, Astore S, Mandala M, Trabalzini F, Nuti D (2013) Natural course of positional down-beating nystagmus of peripheral origin. J Neurol 260: 1489–1496. [DOI] [PubMed] [Google Scholar]
- 38. Hain TC, Helminski JO, Reis IL, Uddin MK (2000) Vibration does not improve results of the canalith repositioning procedure. Arch Otolaryngol Head Neck Surg 126: 617–622. [DOI] [PubMed] [Google Scholar]
- 39. Nunez RA, Cass SP, Furman JM (2000) Short- and long-term outcomes of canalith repositioning for benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 122: 647–652. [DOI] [PubMed] [Google Scholar]
- 40. Perez P, Franco V, Cuesta P, Aldama P, Alvarez MJ, et al. (2012) Recurrence of benign paroxysmal positional vertigo. Otol Neurotol 33: 437–443. [DOI] [PubMed] [Google Scholar]
- 41. Fife TD (2009) Benign paroxysmal positional vertigo. Semin Neurol 29: 500–508. [DOI] [PubMed] [Google Scholar]
- 42. Baloh RW, Honrubia V, Jacobson K (1987) Benign positional vertigo: clinical and oculographic features in 240 cases. Neurology 37: 371–378. [DOI] [PubMed] [Google Scholar]
- 43. Froehling DA, Silverstein MD, Mohr DN, Beatty CW, Offord KP, et al. (1991) Benign positional vertigo: incidence and prognosis in a population-based study in Olmsted County, Minnesota. Mayo Clin Proc 66: 596–601. [DOI] [PubMed] [Google Scholar]
- 44. Celebisoy N, Polat F, Akyurekli O (2008) Clinical features of benign paroxysmal positional vertigo in Western Turkey. Eur Neurol 59: 315–319. [DOI] [PubMed] [Google Scholar]
- 45. Kim YH, Kim KS, Choi H, Choi JS, Han CD (2012) Benign Paroxysmal Positional Vertigo Is Not a Prognostic Factor in Sudden Sensorineural Hearing Loss. Otolaryngol Head Neck Surg 146: 279–82. [DOI] [PubMed] [Google Scholar]
- 46. Ogun OA, Buki B, Cohn ES, Janky KL, Lundberg YW (2014) Menopause and benign paroxysmal positional vertigo. Menopause 21: 886–889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Cohen HS, Stewart MG, Brissett AE, Olson KL, Takashima M, et al. (2010) Frequency of sinus disease in normal subjects and patients with benign paroxysmal positional vertigo. ORL J Otorhinolaryngol Relat Spec 72: 63–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Lasisi AO, Abdullahi M (2008) The inner ear in patients with nasal allergy. J Natl Med Assoc 100: 903–905. [DOI] [PubMed] [Google Scholar]
- 49. Friauf E, Wenz M, Oberhofer M, Nothwang HG, Balakrishnan V, et al. (2008) Hypothyroidism impairs chloride homeostasis and onset of inhibitory neurotransmission in developing auditory brainstem and hippocampal neurons. Eur J Neurosci 28: 2371–2380. [DOI] [PubMed] [Google Scholar]
- 50. Dror AA, Politi Y, Shahin H, Lenz DR, Dossena S, et al. (2010) Calcium oxalate stone formation in the inner ear as a result of an Slc26a4 mutation. J Biol Chem 285: 21724–21735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Everett LA, Belyantseva IA, Noben-Trauth K, Cantos R, Chen A, et al. (2001) Targeted disruption of mouse Pds provides insight about the inner-ear defects encountered in Pendred syndrome. Hum Mol Genet 10: 153–161. [DOI] [PubMed] [Google Scholar]
- 52. Kozel PJ, Friedman RA, Erway LC, Yamoah EN, Liu LH, et al. (1998) Balance and hearing deficits in mice with a null mutation in the gene encoding plasma membrane Ca2+-ATPase isoform 2. J Biol Chem 273: 18693–18696. [DOI] [PubMed] [Google Scholar]
- 53. Gyo K (1988) Benign paroxysmal positional vertigo as a complication of postoperative bedrest. Laryngoscope 98: 332–333. [DOI] [PubMed] [Google Scholar]
- 54. Hederstierna C, Hultcrantz M, Collins A, Rosenhall U (2007) Hearing in women at menopause. Prevalence of hearing loss, audiometric configuration and relation to hormone replacement therapy. Acta Otolaryngol 127: 149–155. [DOI] [PubMed] [Google Scholar]
- 55. Gizzi M, Ayyagari S, Khattar V (1998) The familial incidence of benign paroxysmal positional vertigo. Acta Otolaryngol 118: 774–777. [DOI] [PubMed] [Google Scholar]
- 56. Meggs WJ, Dunn KA, Bloch RM, Goodman PE, Davidoff AL (1996) Prevalence and nature of allergy and chemical sensitivity in a general population. Arch Environ Health 51: 275–282. [DOI] [PubMed] [Google Scholar]
- 57. Chen W, Mempel M, Schober W, Behrendt H, Ring J (2008) Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy 63: 1418–1427. [DOI] [PubMed] [Google Scholar]
- 58. Schiller JS, Lucas JW, Ward BW, Peregoy JA (2012) Summary health statistics for U.S. adults: National Health Interview Survey, 2010. National Center for Health Statistics. Vital Health Stat 10: 252. [PubMed] [Google Scholar]
- 59.Faul M, Xu L, Wald MM, Coronado VG (2010) Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Atlanta (GA): Center for Disease Control and Prevention, National Center for Injury prevention and Control.
- 60. MacGregor EA, Rosenberg JD, Kurth T (2011) Sex-related differences in epidemiological and clinic-based headache studies. Headache 51: 843–859. [DOI] [PubMed] [Google Scholar]
- 61. Scher AI, Stewart WF, Liberman J, Lipton RB (1998) Prevalence of frequent headache in a population sample. Headache 38: 497–506. [DOI] [PubMed] [Google Scholar]
- 62.CDC (2012) Cholesterol facts. Available: http://www.cdc.gov/cholesterol/facts.htm. Accessed 2013 February 6.
- 63.NIDDK (2012) National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC). Available: http://kidney.niddk.nih.gov/KUDiseases/pubs/kustats/index.aspx. Accessed 2013 February 6.
- 64. Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M (2001) Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 41: 646–657. [DOI] [PubMed] [Google Scholar]
- 65.Christopher and Dana Reeve Foundation (2013) One Degree of Separation: Paralysis and Spinal Cord Injury in the United States. Available: http://www.christopherreeve.org/site/c.ddJFKRNoFiG/b.5091685. Accessed 2013 February 6.
- 66.NHLBI (2012) Morbidity & Mortality: 2012 Chart Book on Cardiovascular, Lung, and Blood Diseases. Available: http://www.nhlbi.nih.gov/resources/docs/2012_ChartBook_508.pdf , NIH NHLBI. Accessed 2013 February 6.
- 67. Tunbridge WM, Evered DC, Hall R, Appleton D, Brewis M, et al. (1977) The spectrum of thyroid disease in a community: the Whickham survey. Clin Endocrinol (Oxf) 7: 481–493. [DOI] [PubMed] [Google Scholar]
- 68. Tunbridge WM, Evered DC, Hall R, Appleton D, Brewis M, et al. (1977) Lipid profiles and cardiovascular disease in the Whickham area with particular reference to thyroid failure. Clin Endocrinol (Oxf) 7: 495–508. [DOI] [PubMed] [Google Scholar]
- 69. Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, et al. (1995) The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf) 43: 55–68. [DOI] [PubMed] [Google Scholar]
- 70. Blackwell DL, Collins JG, Coles R (2002) Summary health statistics for U.S. adults: National Health Interview Survey, 1997. Vital Health Stat 10: 1–109. [PubMed] [Google Scholar]
- 71. Blackwell DL, Tonthat L (2002) Summary health statistics for the U.S. population: National Health Interview Survey, 1997. Vital Health Stat 10: 1–92. [PubMed] [Google Scholar]
- 72. Kobau R, Zahran H, Thurman DJ, Zack MM, Henry TR, et al. (2008) Epilepsy surveillance among adults–19 States, Behavioral Risk Factor Surveillance System, 2005. MMWR Surveill Summ 57: 1–20. [PubMed] [Google Scholar]
- 73.U.S.Census Bureau (2010) 2010 Demographic Profile Data - Nebraska. Available: http://quickfacts.census.gov/qfd/states/31000.html. Accessed 2013 February 8.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.