

Abstract
[Purpose] The purpose of this study was to show somatotype and physical characteristic differences between elite boxing athletes and non-athletes. [Methods] The somatotypes of 23 elite boxing athletes and 23 nonathletes were measured with the Heath-Carter method. The subjects were divided into four weight divisions as follows: lightweight, light middleweight, middleweight, and heavyweight class. [Results] The endomorphic component values of the boxing athletes were lower than those of the nonathletes. However, the mesomorphic component values of the boxing athletes were higher than those of the nonathletes. There was no significant difference in the ectomorphic component between the two groups. The higher weight divisions tended to have higher values of height, weight, and BMI than the lower weight divisions. The higher weight divisions also tended to have higher values for the endomorphic and mesomorphic components and a lower value for the ectomorphic component than the lower weight divisions. The group of nonathletes consisted of eight endomorphs, four mesomorphs, six ectomorphs, and five central types. Among the boxing athletes, there were 16 mesomorphic, four ectomorphic, and two central types and one endomorphic type. Subdividing the athletes into 13 somatotypes resulted in five balanced mesomorphs, five endomorphic mesomorphs, five mesomorph-ectomorphs, three mesomorph-endomorphs, two mesomorphic ectomorphs, two central types, and one ectomorphic mesomorph type. [Conclusion] The data from this study provides in part physical characteristics of elite boxing athletes that can be used to establish a reference for systemic study of sports physiotherapy.
Key words: Somatotype analysis, Elite boxing athletes, Specialized sports physiotherapy
INTRODUCTION
Boxing, which originated in ancient Egypt, has evolved over the course of 5,000 years1). Wearing gloves, both boxers attack and defend using their fists inside a ring2). A boxing match consists of three rounds of 3 min, with 1 min of rest between rounds3, 4). During each round, judges assess the scores of each boxers according to the number of clean punches made with the knuckle part of the glove against the target region of the opponent5). The target region is defined as any part of the front or sides of the head or body above the belt6). Weight categories in boxing are divided into 10 divisions ranging from ~48 to 90 kg or more7). The somatotype refers to the physical characteristics of the individual8). Hippocrates (400 BC) recognized two types of human somatotype: habitus phthisicus and habitus apoplecticus. Habitus phthisicus means “long and thin,” and habitus apoplecticus means “short and thick”. This was the origin of the somatotype9). However, it was impossible to define standardized somatotype characteristics, as there were differences according to lifestyles. The Heath-Carter method determines the somatotype according to the body’s size, bone width, and skin thickness10,11,12). It classifies individuals into 13 somatotypes based on the results of these measurements10,11,12). This classification suggests that acquired behavior and lifestyles could have an effect on body shape. Heath-Carter’s classification can be applied to elite boxing athletes and used to determine the effect of elite boxing on the somatotype. Studies have shown that the adaptation to physical effort as a result of training and the process of selection results in a decrease in somatotype diversity among athletes in similar sports or athletes using similar skills compared with nonathletes13,14,15). However, research on elite boxing athletes has rarely been done. Our study, therefore, provides the physical characteristics of elite boxing athletes to establish a reference for their training and rehabilitation.
SUBJECTS AND METHODS
This study consisted of 23 elite boxing athletes and 23 nonathletes. Measurements were taken in November 2013. Forty-six volunteers who had no physical or psychological conditions provided written informed consent to participate in this study. The participants were asked to complete a questionnaire administered by individual in-depth interviews that took 20–30 min per person16). The participants wore only shorts during the measurements, and the measurements were taken by a single person. Before the measurements, all the participants rested for 30 min. The weight categories were divided into four divisions: a lightweight class (~49 to ~56 kg), light middleweight class (~60 to ~64 kg), middleweight class (~69 to ~75 kg), and heavyweight class (~81 to 91 kg or more). The somatotypes were classified as ectomorphic, mesomorphic, endomorphic, and central types according to Heath-Carter’s modified somatotype method10,11,12). The girths of the upper arms and the thickest part of the calves were then determined with a tapeline. The breadths of the biepicondylar humerus and biepicondylar femur were measured with a large anthropometer. Finally, the triceps brachii, subscapular, suprailiac, and calf skinfold thicknesses were determined with a medical skinfold caliper (Jamar, Anaheim, CA, USA). Measurement results were then interpreted with the modified somatotype method10,11,12) (Fig. 3). The somatotypes were classified as endomorphic, mesomorphic, ectomorphic, and balanced types. They were further broken into 13 subcategories: balanced endomorph (Ben, the endomorphic component is dominant, and the values of the mesomorphic and ectomorphic components do not differ by more than 0.5), mesomorphic endomorph (Men, the endomorphic component is dominant, and the value of the mesomorphic component is higher than that of the ectomorphic component), mesomorph-endomorph (M-En, the values for the mesomorphic and endomorphic components do not differ by more than 0.5, and the value of the ectomorphic component is lower than the other values), endomorphic mesomorph (EnM, the mesomorphic component is dominant, and the endomorphic component is higher than the ectomorphic component), balanced mesomorph (BM, the mesomorphic component is dominant, and the values of the endomorphic and ectomorphic components do not differ by more than 0.5), ectomorphic mesomorph (EcM, the mesomorphic component is dominant, and the ectomorphic component is higher than the endomorphic component), mesomorph-ectomorph (M-Ec, the values of the mesomorphic and ectomorphic components do not differ by more than 0.5, and the value for the endomorphic component is lower than that of the other values), mesomorphic ectomorph (MEc, the ectomorphic component is dominant, and the mesomorphic component is higher than the endomorphic component), balanced ectomorph (BEc, the ectomorphic component is dominant, and the values for the endomorphic and mesomorphic components do not differ by more than 0.5), endomorphic ectomorph (EnEc, the ectomorphic component is dominant, and the endomorphic component is higher than the mesomorphic component), endomorph-ectomorph (En-Ec, the values for the endomorphic and ectomorphic components do not differ by more than 0.5, and the value for the mesomorphic component is lower than that of the other values), ectomorphic endomorph (EcEn, the endomorphic component is dominant, and the ectomorphic component is higher than the mesomorphic component), and central type (C, the values do not differ by 1 in any of the components)10,11,12, 17, 18) (Fig. 3). The formulas for the Heath-Carter method are as follows:
| Endomorphic component = −0.7182 + 0.1451 × ∑SF − 0.00068 × ∑SF2 + 0.0000014 × ∑SF3, |
where ∑SF = (sum of the triceps brachii, subscapular, and suprailiac skinfold thicknesses) × [170.18/height (cm)].
Fig. 3.

Schematic representation of the somatochart for sports physiotherapy. The somatochart was prepared as described in the Subjects and Methods (quoted and modified from Heath and Carter10,11,12).
Mesomorphic component = 0.858 × breadth of biepicondylar humerus + 0.601 × breadth of biepicondylar femur + 0.188 × modified girth of upper arm + 0.161 × modified girth of the calf − height × 0.131+4.5, where the modified value is [value − (1/10 of the skinfold thickness of the part)].
The ectomorphic component is calculated as the difference according to the value of the height weight ratio (HWR, HWR = height / 3√weight).
If HWR ≥ 40.75, then ectomorphic component = 0.732 × HWR − 28.58.
If 38.25 < HWR < 40.75, then ectomorphic component = 0.463 × HWR − 17.63.
If HWR ≤ 38.25, then ectomorphic component = 0.1.
The formulas marked on the somatotype chart are as follows:
X = ectomorphic component − endomorphic component
Y = 2 × mesomorphic component − (endomorphic component + ectomorphic component)
Statistical analyses were conducted using the SAS software (version 6.12) to calculate averages and standard deviations. The data are expressed as means ± standard error (SE) of the measurements. The significance level was set to α=0.05 when performing an independent t-test for group comparisons. The protocol for the study was approved by the Committee of Ethics in Research of the University of Yongin, in accordance with the terms of Resolution 5-1-20, December 2006. Furthermore, all volunteers provided informed consent for participation in the study.
RESULTS
Different physical characteristics were observed between the nonathletes and the elite boxing athletes (Table 1). The endomorphic component values of the boxing athletes were lower than those of the nonathletes. However, the mesomorphic component values in the boxing athletes were higher than in the nonathletes (Table 1). On the somatotype chart, the boxing athletes were more likely to be gathered in the central and upper parts (mesomorphic side) than the nonathletes (Fig. 1). There were also differences among the weight categories, with the higher weight divisions tending to have higher values of height, weight, and BMI than the lower weight divisions (Table 2). In addition, the higher weight divisions tended to have higher values for the endomorphic and mesomorphic components and a lower value for the ectomorphic component than the lower weight divisions (Table 2). The somatotype chart shows the classifications of the somatotypes, with points shifted left and up for the higher weight divisions (Fig. 2). The group of nonathletes consisted of eight endomorphs, four mesomorphs, six ectomorphs, and five central types. However, for the boxing athletes, there were 16 mesomorphic, four ectomorphic, and two central types and only one endomorphic type. Subdividing the athletes into 13 somatotypes resulted in five balanced mesomorphs, five endomorphic mesomorphs, five mesomorph-ectomorphs, three mesomorph-endomorphs, two mesomorphic ectomorphs, two central types, and one ectomorphic mesomorph type (Figs. 1 and 2, and Table 2).
Table 1. Characteristics of the nonathletes and elite boxing athletes.
| Variable | Nonathletes | Elite boxing athletes |
|---|---|---|
| Age (yr) | 22.6 ± 0.6 | 19.3 ± 0.3 |
| Gender | ||
| Male (%a/%b) | 23 (100.0/50.0) | 23 (100.0/50.0) |
| Female (%a/%b) | - | - |
| Height (cm) | 174.5 ± 0.8 | 173.2 ± 1.0 |
| Weight (kg) | 69.1 ± 1.4 | 70.2 ± 2.4 |
| BMI (kg/m²) | 22.7 ± 0.5 | 23.3 ± 0.6 |
| Career (yr) | - | 5.6 ± 0.5 |
| Training time | - | 5.1 ± 0.3 h/day |
| - | 30.1 ± 1.9 h/week | |
| Weight division | ||
| L (~49 to ~56 kg) (%a/%b) | - | 6 (26.1/13.0) |
| L-M (~60 to ~64 kg) (%a/%b) | - | 8 (34.8/17.4) |
| M (~69 to ~75 kg) (%a/%b) | - | 5 (21.7/10.9) |
| H (~81 to 91 kg or more) (%a/%b) | - | 4 (17.4/8.7) |
| Somatotype | ||
| Endomorphy (%a/%b) | 8 (34.8/17.4) | 1 (4.3/2.2) |
| Mesomorphy (%a/%b) | 4 (17.4/8.7) | 16 (69.6/34.8) |
| Ectomorphy (%a/%b) | 6 (26.1/13.0) | 4 (17.4/8.7) |
| Central (%a/%b) | 5 (21.7/10.9) | 2 (8.7/4.3) |
| Endo C. | 3.0 ± 0.2 | 2.3 ± 0.2* |
| Meso C. | 3.0 ± 0.2 | 3.7 ± 0.2* |
| Ecto C. | 2.6 ± 0.2 | 2.3 ± 0.2 |
Data are presented as means ± SE. aPercentage of athletes. bPercentage of all participants. BMI, body mass index; L, lightweight class; L-M, light middleweight class; M, middleweight class; H, heavyweight class; Endo C., endomorphic component; Meso C., mesomorphic component; Ecto C., ectomorphic component. * p < 0.05
Fig. 1.

Differences in somatochart between the nonathletes and elite boxing athletes. Somatotype analysis was performed, as described in the Subjects and Methods
Table 2. Differences in somatotype among the weight division of elite boxing athletes.
| Variable | Weight divisions of elite boxing athletes |
|||
|---|---|---|---|---|
| Lightweight (~49 to ~56 kg) |
Light middleweight (~60 to ~64 kg) |
Middleweight (~69 to ~75 kg) |
Heavyweight (~81 to 91 kg or more) |
|
| Number (%a/%b) | 6 (100.0/26.1) | 8 (100.0/34.8) | 5 (100.0/21.7) | 4 (100.0/17.4) |
| Height (cm) | 168.1±0.6 | 171.4±1.1* | 177.6±1.2*† | 179.0±1.3*† |
| Weight (kg) | 58.3±0.9 | 68.0±1.7* | 72.5±1.9* | 89.3±4.0*†# |
| BMI (kg/cm²) | 20.7±0.3 | 23.2±0.6* | 23.0±0.5* | 27.9±1.6*†# |
| 3 Somatotypes | ||||
| Endo (%a/%b) | - | - | - | 1 (25.0/4.3) |
| Meso (%a/%b) | 4 (66.7/17.4) | 6 (75.0/26.1) | 3 (60.0/13.0) | 3 (75.0/13.0) |
| Ecto (%a/%b) | 2 (33.3/8.7) | 1 (12.5/4.3) | 1 (20.0/4.3) | - |
| Central (%a/%b) | - | 1 (12.5/4.3) | 1 (20.0/4.3) | - |
| Endo C. | 1.8±0.2 | 2.3±0.3 | 2.1±0.3 | 3.5±0.6 |
| Meso C. | 3.2±0.2 | 3.7±0.2 | 3.5±0.5 | 4.5±0.4* |
| Ecto C. | 3.1±0.2 | 2.2±0.3* | 2.6±0.2 | 1.1±0.3*# |
| 13 Somatotypes | ||||
| Types (%a/%b) | M-Ec 3 (50.0/13.0) | BM 3 (37.5/13.0) | M-Ec 2 (40.0/8.7) | EnM 2 (50.0/8.7) |
| EcM 1 (16.7/4.3) | EnM 2 (25.0/8.7) | BM 1 (20.0/4.3) | ||
| BM 1(16.7/4.3) | M-En1 (12.5/4.3) | EnM 1 (20.0/4.3) | M-En 2 (50.0/8.7) | |
| MEc 1 (16.7/4.3) | MEc 1 (12.5/4.3) | Cen 1 (20.0/4.3) | ||
| Cen 1 (12.5/4.3) | ||||
Data are presented as means ± SE. aPercentage of athletes. bPercentage of all participants. BMI, body mass index; Endo C., endomorphic component; Meso C., mesomorphic component; Ecto C., ectomorphic component; M-Ec, mesomorph ectomorph; EcM, ectomorphic mesomorph; BM, balanced mesomorph; MEc, mesomorphic ectomorph; EnM, endomorphic mesomorph; M-En, mesomorph endomorph; Cen, central. *†# p < 0.05
Fig. 2.
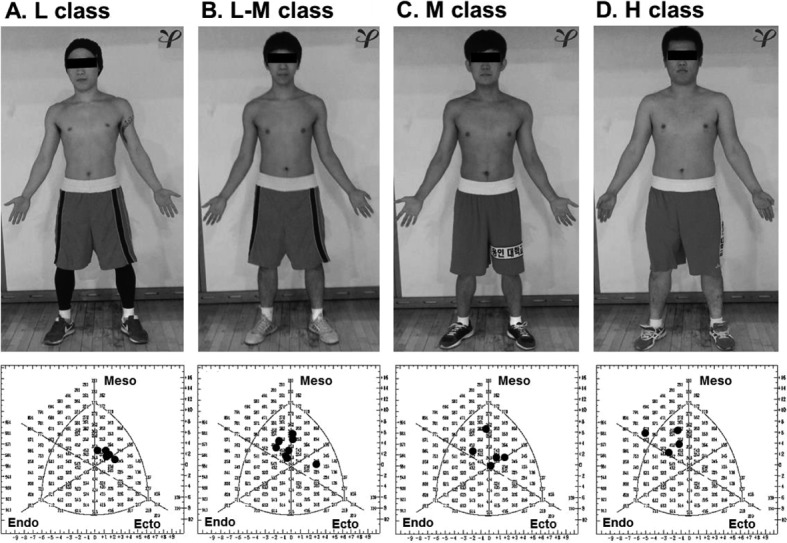
Differences in somatochart among the weight divisions of elite boxing athletes. The weight categories in the present study were divided into four divisions: the lightweight (A), light middleweight (B), middleweight (C), and heavyweight (D) classes. L class, lightweight class (~49 to ~56 kg); L-M class, light middleweight class (~60 to ~64 kg); M class, middleweight class (~69 to ~75 kg); H class, heavyweight class (~81 to 91 kg or more); Endo, endomorphy; Meso, mesomorphy; Ecto, ectomorph
DISCUSSION
In our study, although similar in weight, height, and BMI, the boxing athletes were more muscular than the nonathletes. The endomorphic component values of the boxing athletes were also lower than those of the nonathletes. However, the mesomorphic component values of the boxing athletes were higher than those of the nonathletes. The endomorphic and mesomorphic components of the nonathletes were not different, whereas the boxing athletes had higher mesomorphic component values and lower endomorphic component values. There was a much higher percentage of mesomorph types in the elite boxer group. This result was also seen in other studies, with athletes in other combat sports, such as judo, Korean wrestling also called ssireum, wrestling, and jujitsu, tending to have a mesomorphic somatotype17,18,19,20,21). Soccer players also showed a tendency toward a balanced mesomorphic somatotype22). However, the endomorphic component value of soccer players was lower than that in contact combat sports, such as judo and Korean wrestling17, 19). Boxers have to avoid attacks and powerful hits by their opponent and continue to move their entire body until the end of the match. As they require speed, power, and endurance, they have lower endomorphic component values and higher mesomorphic component values than athletes in other combat sports. Even in the same sports, physical characteristics differ according to the weight category. In a study of the somatotype of Korean wrestling players, higher weight divisions were shown to have higher values for height, weight, and BMI than lower weight divisions; there were also different somatotype components between the weight categories17, 19). The same result was found in the present study of elite boxers, with the higher weight divisions having higher values for height, weight, and BMI than the lower weight players. The heavyweight and lightweight classes had higher endomorphic and ectomorphic component values, respectively, than the other weight divisions. However, in each weight category, the mesomorphic component was more dominant than the other components. To summarize our data, boxing athletes have a higher mesomorphic component and a lower endomorphic component for their athletic performance. Therefore, we suggest that elite boxing athletes who are injured or training for a match need to be training for fat reduction and muscle power when returning from injury. However, further studies in the area of sports physiotherapy are needed to corroborate the pathologic mechanism of sports injury23,24,25).
REFERENCES
- 1.Smith MS: Physiological profile of senior and junior England international amateur boxers. J Sports Sci Med, 2006, 5: 74–89 [PMC free article] [PubMed] [Google Scholar]
- 2.El Ashker S: Technical performance effectiveness subsequent to complex motor skills training in young boxers. Eur J Sport Sci, 2012, 12: 475–484 [Google Scholar]
- 3.Thomson E, Lamb K, Nicholas C: The development of a reliable amateur boxing performance analysis template. J Sports Sci, 2013, 31: 516–528 [DOI] [PubMed] [Google Scholar]
- 4.International Boxing Association (AIBA). AIBA Openboxing Competition (Rule. 7) Aug 2013: 10.
- 5.El Ashker S: Technical and tactical aspects that differentiate winning and losing performances in boxing. Int J Perform Anal Sport, 2011, 11: 356–364 [Google Scholar]
- 6.Davis P, Wittekind A, Beneke R: Amateur boxing: activity profile of winners and losers. Int J Sports Physiol Perform, 2013, 8: 84–91 [DOI] [PubMed] [Google Scholar]
- 7.International Boxing Association (AIBA). AIBA Openboxing Competition (Rule.1) Aug 2013:5.
- 8.Walker RN, Tanner JM: Prediction of adult Sheldon somatotypes I and II from ratings and measurements at childhood ages. Ann Hum Biol, 1980, 7: 213–224 [DOI] [PubMed] [Google Scholar]
- 9.Carter JE: The somatotypes of athletes—a review. Hum Biol, 1970, 42: 535–569 [PubMed] [Google Scholar]
- 10.Heath BH, Carter JE: A comparison of somatotype methods. Am J Phys Anthropol, 1966, 24: 87–99 [DOI] [PubMed] [Google Scholar]
- 11.Heath BH, Carter JE: A modified somatotype method. Am J Phys Anthropol, 1967, 27: 57–74 [DOI] [PubMed] [Google Scholar]
- 12.Heath BH, Carter JE: Growth and somatotype patterns of Manus children, territory of Papua and New Guinea: application of a modified somatotype method to the study of growth patterns. Am J Phys Anthropol, 1971, 35: 49–67 [DOI] [PubMed] [Google Scholar]
- 13.Charzewski J, Glaz A, Kuzmicki S: Somatotype characteristics of elite European wrestlers. Biol Sport, 1991, 8: 213–221 [Google Scholar]
- 14.Krawczyk B, Sklad M, Jackiewicz A: Heath-carter somatotypes of athletes representing various sports. Biol Sport, 1997, 14: 243–250 [Google Scholar]
- 15.Lee WD, Lee LK, Kim B, et al. : Differences in body components and the significance of rehabilitation for taekwondo athletes compared to nonathletes. Toxicol Environ Health Sci, 2012, 4: 203–208 [Google Scholar]
- 16.Kim JH, Kim IH, Lee JU, et al. : Change of muscular activity and dynamic stability of the knee joint due to excessive and repetitive jumping or cutting by female athletes. J Phys Ther Sci, 2012, 24: 715–719 [Google Scholar]
- 17.Noh JW, Kim JH, Kim J: Somatotype analysis of Korean wrestling athletes compared with non-athletes for sports health sciences. Toxicol Environ Health Sci, 2013a, 5: 163–168 [Google Scholar]
- 18.Noh JW, Kim JH, Kim J: Somatotype analysis of elite taekwondo athletes compared to non-athletes for sports health sciences. Toxicol Environ Health Sci, 2013b, 5: 189–196 [Google Scholar]
- 19.Lewandowska J, Buśko K, Pastuszak A, et al. : Somatotype variables related to muscle torque and power in judoists. J Hum Kinet, 2011, 30: 21–28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sterkowicz-Przybycień KL, Sterkowicz S, Zarów RT: Somatotype, body composition and proportionality in polish top greco-roman wrestlers. J Hum Kinet, 2011, 28: 141–154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Andreato LV, Franchini E, Moraes SM, et al. : Morphological profile of Brazilian jiu-jitsu elite athletes. Rev Bras Med Esporte, 2012, 18: 46–50 [Google Scholar]
- 22.Nikolaidis PT, Vassilios Karydis N: Physique and body composition in soccer players across adolescence. Asian J Sports Med, 2011, 2: 75–82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kim IH, Kim JH, Lee JU, et al. : The effect of an early lumbar exercise program on trunk strength and the Oswestry disability index after herniated nucleus pulposus surgery. J Phys Ther Sci, 2012, 24: 165–168 [Google Scholar]
- 24.Yang SM, Lee WD, Kim JH, et al. : Differences in body components and electrical characteristics between youth soccer players and non-athletes. Health, 2013, 5: 1010–1015 [Google Scholar]
- 25.Lee LK, Kim JH, Kim MY, et al. : A review of signal transduction of endothelin-1- and mitogen-activated protein kinase-related pain for nanophysiotherapy. J Phys Ther Sci, 2014, 26: (in press). [DOI] [PMC free article] [PubMed] [Google Scholar]