

Abstract
Video laryngoscope (VL) provides excellent laryngeal exposure in patients when anaesthesiologists encounter difficulty with direct laryngoscopy. Videolaryngoscopy, like flexible fibreoptic laryngoscopy demands a certain level of training by practitioners to become dexterous at successful intubation with a given instrument. Due to their cost factors, VLs are not easily available for training purposes to all the students, paramedics and emergency medical services providers in developing countries. We tried to develop a cost-effective instrument, which can work analogous to various available VLs. An inexpensive and easily available instrument was used to create an Airtraq Model for VL guided intubation training on manikin. Using this technique, successful intubation of manikin could be achieved. The Airtraq Model mimics the Airtraq Avant® and may be used for VL guided intubation training for students as well as paramedics, and decrease the time and shorten the learning curve for Airtraq® as well as various other VLs.
Keywords: Airtraq®, learning curve, optical stylets, video laryngoscope
INTRODUCTION
Wide range of rigid video laryngoscope (VL) are available in the Indian market today like McGrath 5®, Glidescope®, Airtraq®, Kingsvision®, Truview EVO2®, CMAC®, Pentax®, VT-A100® and so on. The rigid VLs are expensive compared with traditional laryngoscopes. The higher price, coupled with the high economic recession is leading to slower adoption of the more expensive rigid VL across the globe. The use of VLs may, however, be of benefit in a teaching situation where novice practitioners can visualise the technique of a supervisor and vice versa.[1] However, as with conventional laryngoscopy and with other airway devices, successful use of the VL requires skill and multiple uses to become proficient.[2,3] Each VL offers different features such as video and still recordings, disposable or reusable blades, different battery types, ruggedness, different sizes of scopes and monitors. For the students to get accustomed with various VLs, it is necessary to get oriented to various types of VL blades and the images which are seen on either the monitor or through the eyepiece of the respective laryngoscope being used. The best way to determine which VL is preeminent for novice is to try in his own hands from the various available VLs and start using it on manikins, and then move to the cadaver lab and patients. These devices are effective in providing visualisation of difficult airways, but they have a long and difficult learning curve, with desertion by many prospective operators before they acquire competence.[4,5,6] Unfortunately, the use of VL is associated with longer time to tracheal intubation compared with the traditional techniques which can be explained with the variable learning curves of practitioners.[7] It is a known fact that visualisation of larynx is easy with all VLs but negotiating the endotracheal tube through it into the larynx is difficult.[8] The foremost thing to remember about these new ranges of laryngoscopes is that there is a definite learning curve with each instrument before one can master the art of intubation with that particular instrument.
Despite the growing number of practitioners attempting to use VL in their everyday practices, only few training tools exist. The biggest limitation to the day to day use for VL in operation theatre is their cost factor and the most affordable VL available in a developing country such as India, is Airtraq®. Single use Airtraq® with disposable blades has to be used after adequate training, otherwise it won’t be cost effective.[9] For the institutional teaching purpose Airtraq® has demo blades which can be used innumerable times. However, to make all the novices and practitioners learn the technique of intubation and to reach plateau of their learning curve quickly in VL, we have developed a cheap model of VL which is both cost effective and can also mimic various available VLs/optical stylets in market.
METHODS
The training kit is prepared as below: First of all, a sheath of Airtraq Avant® (regular size) is separated out [Figure 1]. The eyepiece portion is removed. (One can also remove the square plastic portion of distal tip to avoid glare from endoscope's light-emitting diode (LED) as shown by arrow in Figure 1).
Figure 1.

Airtraq Avant Sheath®
Next we need to purchase a simple cheap flexible borescope (industrial/snake endoscope, Figure 2). The camera portion of borescope is introduced into the sheath of Airtraq Avant® on the same side where its ideal fibreoptics rests [Figure 3]. Borescope/snake endoscope may have a universal serial bus (USB) cable (available up to 20 feet in length) which is plugged into a laptop and that gives power to the LED and the camera. The borescope is then switched on and this whole assembly is introduced into the airway of the manikin, and various intraoral images can be seen and appreciated on its monitor/laptop. As we advance the model and visualise the larynx we need to stabilize the image of larynx on monitor's centre and then try to intubate through the side channel of Airtraq sheath® as shown in Figure 4. This whole VL model can be used as many times to train students repeatedly.
Figure 2.

Borescopes/snake endoscopes
Figure 3.

Snake endoscope passed through Airtraq Avant Sheath®
Figure 4.
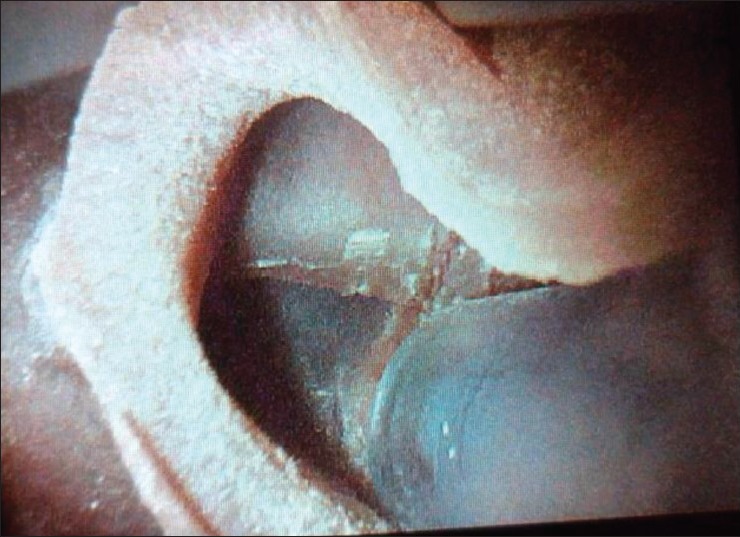
Endotrachial tube negotiating through the vocal cords as seen on screen
DISCUSSION
A borescope is an optical tool used to view areas that would otherwise not be visible. A videoscope or video borescope typically utilises a charge-coupled device or complementary metal–oxide–semiconductor camera sensor, located at the tip of the borescope, to produce an image that is relayed to an external viewing device such as a liquid crystal display monitor. Similarly all the VLs available in market today utilise video camera technology to visualise airway structures and facilitate endotracheal intubation. Thus, we can use the video technology of a borescope/videoscope for making a cheap model of VL.
The purpose of this report is to describe an inexpensive model, which is similar in some extent to but not inspired by VividTrac VT-A100®. Its use can further be extended to mimic not only various VLs but also newer optical stylets and so on. This whole VL model will cost around 5000-10,000 INR and can be used multiple times.
The borescope/USB endoscope can be tried in the sheath of Glidoscope®, CoPilotVL® and Pentax® VL and used similarly. The flexible borescope alone can be used to mimic other simpler instruments like stylet view (Vustik)®, Trachview®, MS201 Video Laryngoscope® and Disposcopes® which could be tried upon the manikin directly without the aid of any laryngoscopes or their sheaths. This may prove to be of great benefit to the novice who would like to master their intubation skills in different types of VL and thereby attain plateau of learning curve for various available VLs.
This model of Airtraq® can be inexpensive, easily created and qualitatively consistent with the original Airtraq Avant®. The system described is a working proof of a concept model. It utilises off the shelf, current materials and items. A word of caution - the USB endoscope/borescope is not medically licensed as a clinical device for endoscopy. What has been demonstrated is for experimental and research development only and not for clinical use. The author here describes this model only for practice purpose on manikin and in cadaver labs and does not support in any way the use of this model on patients.
Nowadays various VL manufacturing companies have come up with the idea of replacing the bulb from the Macintosh® and Miller® blades with similar USB endoscopes. This type of video USB laryngoscopes will have the added advantage over the newer VL in that they would both be cheap and will require no extra learning curve. Different types of cheap flexible snake endoscopes, which can be attached to the USB port of our Android smart phones are available as shown in Figure 5 and can be used as VL model on manikin for training purposes.
Figure 5.

Wifi borescopes
Airtraq® has now come up with monitor supporting Bluetooth connectivity whereby the image can be transferred to i-phones®, i-pad® and personal computers. Hope that in near future some of the VL manufacturing companies will come up with similar idea and manufacture optical blades with blue tooth connectivity and the smart phones in our pockets can be used as monitors for them - a concept that can be called WiFi videolaryngoscopy!
SUMMARY
Cheap models of different types of VL or optical stylets can be designed from simple and easily available borescope or video endoscope and can be utilised for attaining basic training for use of actual VLs or optical stylets.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Channa AB. Video laryngoscopes. Saudi J Anaesth. 2011;5:357–9. doi: 10.4103/1658-354X.87262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cooper RM. Use of a new videolaryngoscope (GlideScope) in the management of a difficult airway. Can J Anaesth. 2003;50:611–3. doi: 10.1007/BF03018651. [DOI] [PubMed] [Google Scholar]
- 3.Konrad C, Schüpfer G, Wietlisbach M, Gerber H. Learning manual skills in anesthesiology: Is there a recommended number of cases for anesthetic procedures? Anesth Analg. 1998;86:635–9. doi: 10.1097/00000539-199803000-00037. [DOI] [PubMed] [Google Scholar]
- 4.Cooper RM, Pacey JA, Bishop MJ, McCluskey SA. Early clinical experience with a new videolaryngoscope (GlideScope) in 728 patients. Can J Anaesth. 2005;52:191–8. doi: 10.1007/BF03027728. [DOI] [PubMed] [Google Scholar]
- 5.Jenkins K, Wong DT, Correa R. Management choices for the difficult airway by anesthesiologists in Canada. Can J Anaesth. 2002;49:850–6. doi: 10.1007/BF03017419. [DOI] [PubMed] [Google Scholar]
- 6.Boedeker BH, Murray WB, Nicholas TA. Intubation using the video laryngoscope. Am Med J. 2012;3:67–74. [Google Scholar]
- 7.Butchart AG, Young P. The learning curve for videolaryngoscopy. Anaesthesia. 2010;65:1145–6. doi: 10.1111/j.1365-2044.2010.06522.x. [DOI] [PubMed] [Google Scholar]
- 8.Durga P, Kaur J, Ahmed SY, Kaniti G, Ramachandran G. Comparison of tracheal intubation using the Airtraq(®) and Mc Coy laryngoscope in the presence of rigid cervical collar simulating cervical immobilisation for traumatic cervical spine injury. Indian J Anaesth. 2012;56:529–34. doi: 10.4103/0019-5049.104568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baciarello M, Zasa M, Manferdini ME, Tosi M, Berti M, Fanelli G. The learning curve for laryngoscopy: Airtraq versus Macintosh laryngoscopes. J Anesth. 2012;26:516–24. doi: 10.1007/s00540-012-1351-4. [DOI] [PubMed] [Google Scholar]