

Abstract
Introduction:
This study aimed to assess average and peak craving intensity among nondaily intermittent smokers (ITS) in smoking episodes and when not smoking compared to that of daily smokers (DS).
Methods:
Two hundred and twelve ITS and 194 DS monitored their smoking and craving for 3 weeks using Ecological Momentary Assessment methods. Craving was assessed (0–100 scale) when subjects lit a cigarette and at random times when not smoking; 48,469 observations were analyzed using generalized estimating equations.
Results:
ITS experienced craving, including intense craving; their 95th percentile intensity averaged 77.7±22.5 out of 100 (higher among DS: 89.1±14.5). ITS reported lower craving than DS, both when smoking and when not smoking. In both groups, craving was less intense when not smoking (DS: 71.1±20.7 vs. 59.83±21.97; ITS: 59.91±23.03 vs. 26.63±19.87), but the difference was significantly greater among ITS. Among ITS, the probability of smoking rose continuously as craving increased over the full range of the scale. In contrast, among DS the probability of smoking rose until the midpoint of the scale, after which the relationship flattened. Findings were mostly similar for ITS with and without a history of past daily smoking.
Conclusions:
ITS do experience craving, including intense craving. The relationship between craving and smoking is stronger among ITS because DS experience moderate craving even between cigarettes. In contrast, ITS appear to experience craving in limited situations associated with smoking, suggesting that their craving and smoking may be driven by transient cues rather than endogenous needs.
INTRODUCTION
Nicotine dependence is considered the primary determinant of persistent cigarette smoking, with individuals typically smoking frequently throughout the day, every day. This is thought to be necessary in order to maintain nicotine levels high enough to avoid incipient withdrawal symptoms that would trigger an urge to smoke (Benowitz, 2010; Stolerman & Jarvis, 1995). Indeed, craving is sometimes conceptualized as the subjective experience of the drive to smoke when nicotine levels fall below this hypothetical threshold.
Recently, however, studies (Schane, Glantz, & Ling, 2009; Shiffman, 2009; Shiffman, Tindle et al., 2012) have begun to examine the increasingly prevalent phenomenon of nondaily smoking, which cannot be accounted for by this nicotine maintenance model. Nearly a third of adult U.S. smokers do not smoke daily (Centers for Disease Control and Prevention, 2008a, 2008b; Substance Abuse and Mental Health Services Administration, 2009). The length of time between cigarettes—often greater than 24 hr—means that nondaily or intermittent smokers (ITS) cannot maintain steady nicotine levels and may instead smoke for acute positive reinforcement, rather than for withdrawal avoidance.
Nondaily smoking is very common in the early stages of smoking (DiFranza et al., 2011; Rose, Dierker, & Donny, 2010) and might sometimes be regarded as a transient transitional stage en route to heavier and more addicted smoking. This is not necessarily the case among adult ITS. A recently reported sample of ITS (Shiffman, Tindle et al., 2012) had been smoking an average of 19 years, over which time they had consumed more than 40,000 cigarettes. These ITS reported smoking an average of only 4 days per week, consuming about 4 cigarettes/day on the days that they smoked, and abstaining voluntarily for periods averaging up to 5 consecutive days (Shiffman, Tindle et al., 2012). Despite their extended histories of smoking, however, ITS score very low on questionnaire measures of nicotine dependence, with many indicating no dependence at all (Shiffman, Ferguson, Dunbar, & Scholl, 2012).
A question then arises as to whether ITS experience craving to smoke and whether their smoking is associated with craving. On the one hand, craving is often regarded as pathognomonic of dependence (DiFranza et al., 2011; Drummond, 2001; Robinson & Berridge, 2000), in which case, ITS should show little or no craving. On the other hand, there are indications from pilot data that ITS may be cued to smoke in particular situations, such as when drinking or socializing (Shiffman, Kirchner, Ferguson, & Scharf, 2009), and cues may drive acute craving (Ferguson & Shiffman, 2009; Sayette & Tiffany, 2013; Shiffman et al., 2012). Therefore, ITS might be expected to report craving in situations where they smoke, but not otherwise. Accordingly, this study analyzes ITS craving both at moments of smoking and when not smoking and compares these levels to those reported by DS in the same settings.
Some accounts of craving (Kozlowski & Wilkinson, 1987; Sayette & Tiffany, 2013; Tiffany & Wray, 2012) have suggested that the experience of intense craving is qualitatively different from milder craving and that only more intense craving is unique to dependent smokers. Analyses by Tiffany and Wray (2012) suggested that different questionnaire items differing in “intensity” did not show such effects, but that higher ratings of craving did differentiate dependent and nondependent smokers. To assess whether ITS experience intense forms of craving, we analyzed peak reports of craving, as well as average craving.
This study used Ecological Momentary Assessment (EMA; Stone & Shiffman, 1994), which involves collecting real-time data in real-world settings, using palmtop computers as electronic diaries. Subjects completed craving ratings when lighting up a cigarette (event-contingent data on smoking occasions; see Shiffman et al., 2002). For comparison (Paty, Kassel, & Shiffman, 1992), the electronic diary also solicited craving ratings when subjects were not smoking, by “beeping” subjects at random between smoking episodes (signal-contingent assessment of a random sample of nonsmoking occasions; Shiffman et al., 2002). Craving data were collected from a sample of ITS and DS, examining mean levels, peak levels, and the relationship between craving intensity and smoking among ITS and DS.
While the contrast between DS and ITS is of particular interest, ITS themselves are heterogeneous. It has been estimated (Nguyen & Zhu, 2009; Tindle & Shiffman, 2011) that approximately half of ITS have never smoked daily (“native” ITS—NITS), while the rest were previously daily smokers (“converted” ITS—CITS). Comparing NITS and CITS, we found that CITS smoked on more days and smoked more cigarettes per day than NITS (Shiffman et al., 2012) and showed signs of greater dependence (Shiffman, Ferguson, et al., 2012). Thus, in this study, we collected detailed EMA data on smoking antecedents to characterize craving among ITS, to compare ITS to DS, and, within ITS, to contrast NITS and CITS.
Specifically, our research questions included: Do ITS experience craving? Do they experience intense cravings? Do they experience elevated craving when they are not smoking? What is the relationship between craving and smoking among ITS, compared to DS? And, finally, how do craving dynamics differ between CITS and NITS?
METHODS
Subjects
Subjects were 212 ITS (136 CITS, 68 NITS, and 8 of unknown status) and 194 DS recruited for this study via advertisement and promotion in Pittsburgh, PA between November 2007 and April 2010. This is the first report of EMA data from these samples; previous articles have reported on questionnaire and laboratory data from overlapping samples of subjects (Shiffman et al., 2013; Shiffman, Dunbar, Kirchner, Li, Tindle, Anderson et al., 2013; Shiffman, Dunbar, Scholl, & Tindle, 2012; Shiffman et al., 2012; Shiffman, Ferguson, et al., 2012). Subjects had to be at least 21 years old, report smoking for at least 3 years (both to avoid sampling people who were just learning to smoke) and smoking at their current rate for at least 3 months (allowing for recent converts), and not be planning to quit within the next month. DS had to report smoking every day, between 5–30 cigarettes/day. ITS had to report smoking 4–27 days per month, with no restrictions on number of cigarettes consumed on smoking days. Within ITS, converted ITS (CITS) were those who reported previously smoking daily for at least 6 months; the rest were native ITS (NITS). By design, we oversampled African American smokers, in order to have an adequate sample for subsequent analyses by race. Compared to their population proportions, African American smokers were over-represented among DS by a factor of 3.6 and among ITS by a factor of 1.8. Accordingly, data were weighted in these analyses (Kalton, 1983) to avoid distortion of findings due to this systematic and differential over-representation of African American smokers (Trinidad et al., 2009; unweighted analyses produced similar results). Table 1 shows the demographic and smoking characteristics of the samples.
Table 1.
Subject Demographics and Smoking Characteristicsa
| DS | ITS | CITS | NITS | |
|---|---|---|---|---|
| Age | 40.11 (11.68) | 35.36 (1.28) | 36.91 (1.55) | 33.01 (11.77) |
| Gender (% male) | 58.88 | 49.82 | 46.09 | 55.74 |
| Race (%) | ||||
| African American | 37.63 | 31.60 | 37.50 | 20.59 |
| Caucasian | 59.28 | 65.57 | 61.03 | 75.00 |
| Other | 3.09 | 2.83 | 1.47 | 4.41 |
| Education (% beyond high school) | 62.13 | 84.67 | 80.76 | 90.02 |
| Number of alcoholic drinks/week | 7.91 (10.26) | 9.41 (9.11) | 8.08 (8.69) | 10.92 (8.37) |
| Menthol smokers (%) | 55.19 | 46.56 | 51.55 | 37.74 |
| Cigarettes per smoking day | 15.93 (5.96) | 4.32 (2.94) | 4.90 (3.18) | 3.25 (1.84) |
| Smoking days per week | 6.99 (0.09) | 4.37 (1.67) | 4.65 (1.60) | 3.85 (1.71) |
| Smoking days per month | 29.94 (0.37) | 18.72 (7.15) | 19.95 (6.84) | 16.51 (7.31) |
| Fagerström Test for Nicotine Dependence | 5.21 (2.00) | 1.28 (1.62) | 1.55 (1.77) | 0.74 (1.08) |
Note. DS = daily smokers; ITS = intermittent smokers; CITS = converted ITS; NITS = native ITS.
Data are weighted by race, except for data on ethnicity itself.
aEntries are M (SD), unless % is specified.
Procedures
Subjects used a palmtop-computer-based Electronic Diary (ED; Palm Tungsten E2), running specialized software (invivodata) to monitor their smoking, after receiving hands-on individual training on the use of the computer, the EMA protocol, and all of the assessments. The duration of monitoring varied (range: 6–42 days), averaging 21.70 (SD = 4.08) days, close to the intended 21 days. The large majority of participants (88%) completed the study, with at least 20 days of monitoring; those whose education did not progress past high school were less likely to complete, completing an average of 2 fewer days of monitoring (20 vs. 22 days). There were no other demographic or smoking history differences characterizing those who did not complete the monitoring. Participants were compensated up to $120 for completion of 21 days of monitoring. Compensation was provided at the end of each week of monitoring, in progressively larger increments ($15, $30, and $75 at the end of first, second, and third weeks, respectively).
The EMA protocols and assessments were identical for DS and ITS, with the exception of algorithms for selecting cigarettes for assessment, as described later in this paragraph. Subjects were to record each cigarette as they lit it. Because completing an assessment on each smoking occasion would have been too burdensome, smoking occasions were sampled at random for assessment. For DS, 4–5 cigarettes/day were selected at random for assessment. To maintain this fixed target of cigarette assessments across variations in daily cigarette consumption, the sampling ratio on any given day was based on the prior days’ cigarette consumption (see Shiffman et al., 2002). For example, if a subject smoked 20 cigarettes on a particular day, a random 25% of cigarettes were sampled on the following day, in order to yield 5 cigarette assessments; if 10 cigarettes were smoked the prior day, 50% of cigarettes were assessed, and so on. For ITS, most days were expected to involve no more than four to five cigarettes. However, pilot work (Shiffman et al., 2009) indicated that ITS might sometimes engage in bouts of smoking multiple cigarettes in a short time, which could make assessment very burdensome. Therefore, the algorithm for assessing ITS’ cigarettes each day began by assessing all cigarettes until five assessments were completed. Once five cigarettes had been assessed, the algorithm switched to sampling 50% of smoking occasions, cutting that in half to 25% when a further cigarette was smoked within an hour of the last, to avoid burdening them with very frequent assessments during bouts of concentrated smoking. To account for the sampling scheme, cigarette assessments were weighted by the inverse probability of assessment (e.g., cigarettes whose probability of being assessed was 50% were weighted 2×, to represent their true frequency, and those with 25% probability were weighted 4×), so that any distortion caused by the sampling scheme (particularly the tendency for ITS’ cigarettes smoked later in the day—when they may have already completed five assessments—to have a lower likelihood of assessment) was balanced.
Additionally, ED used signal-based sampling to collect data on nonsmoking occasions, “beeping” subjects at random 3–4 times per day. No nonsmoking assessments could fall within 15min of a reported smoking occasion. Approximately, 3–4 prompts per day were issued, on average (M = 3.04, SD = 0.66). This protocol was active between the time subjects “woke up” ED until they “put ED to sleep” at bedtime, which suppressed beeping. The device was in the “active” mode, during which participants could interact with ED, for an average of 14.52 (SD = 2.45) hr each day.
Measurement
At each assessment, subjects rated the intensity of craving using a visual analog scale that was translated into a 0–100 rating. (The item text was “Cigarette craving?,” and subjects were presented with a horizontal line and could slide a pointer along the line on the touch-screen or simply touch the line at the point indicating their craving intensity. The ends of the line were labeled “NO!!” and “YES!!”, descriptors we have used previously; Shiffman et al., 2002). Tiffany and Wray (2012) have shown that a single-item rating of craving performs well. As an example, in a prior EMA study (Shiffman et al., 2002; Shiffman, Paty, Gnys, Kassel, & Hickcox, 1996), the correlation between ratings of two items—craving and urge—implied a single-item reliability of 0.85.
Dataset Construction
Review of ED data, along with participant reports, identified 113 segments of invalid data (i.e., spans of corrupt data in the ED datastream with discernible start and end points, which varied in time length from less than 30min to several days), due to factors such as software failure, battery exhaustion, or life circumstances that precluded participation (e.g., when incarcerated). These segments of data were deleted. A total of 17 individuals were dropped: 5 completed <50% of prompts, 3 did not adhere to cigarette entry protocol, 8 provided <5 days of data, and 1 ITS recorded no smoking occasions. The final dataset included 406 participants (212 ITS; 194 DS), 13,761 smoking and 11,640 nonsmoking assessments from DS, and 7,778 smoking and 15,290 nonsmoking assessments from ITS. Compliance was good, with participants completing 88% of prompts within the 2min allowed (DS: 87.6%; ITS: 88.2%).
Analysis
To assess the relationship between craving and smoking, generalized estimating equations (GEE; Zeger, Liang, & Albert, 1988) were computed, with smoking as the dependent variable and craving as the independent variable. The GEE models used the logit link and a first-order autoregressive correlation structure to account for the associations among the multiple observations provided by each respondent and examined quadratic as well as linear effects. The quadratic models were used to create model-based estimates of the probability of smoking over the range of craving values. For each subject, we also identified observations where craving intensity was rated above the scale midpoint of 50 and analyzed the craving rating at each subject’s 95th percentile of craving intensity. The percentages of subjects in each group who reached certain craving thresholds were compared using standard χ2 statistics.
RESULTS
As shown in Figure 1, craving was significantly associated with smoking in both groups, but the patterns were substantially different. In both groups, higher craving was associated with smoking, but the relationship was more than twice as strong among ITS (DS: OR = 1.22, 95% CI [1.17–1.27], p < .0001; ITS: OR = 1.46, 95% CI [1.38–1.55], p < .0001), resulting in a significant interaction (OR = 1.18, 95% CI [1.10–1.27], p < .0001). Notably, although ITS show higher mean craving when smoking than when not smoking (though lower than DS’ craving while smoking), their craving was dramatically lower (well below the scale midpoint) when they were not smoking. In contrast DS’ craving was still relatively high (above the scale midpoint) even when not smoking and was even higher when they were about to smoke.
Figure 1.
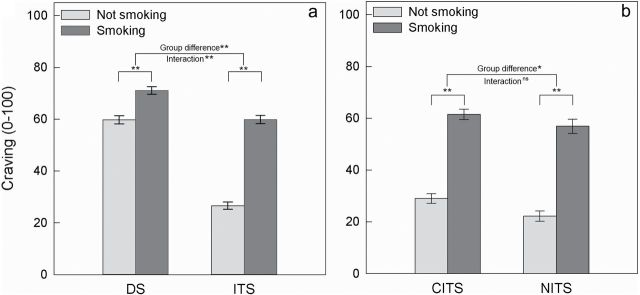
Mean craving levels reported when smoking and when not smoking for (a) daily smokers (DS) and nondaily intermittent smokers (ITS) and (b) converted ITS (CITS) and native ITS (NITS). Error bars are standard errors. ITS’ craving ratings are significantly lower than DS’ in both settings, and the smoker-group × setting interaction is significant. In contrast, CITS and NITS demonstrated similar contrasts of craving when smoking and not smoking, although CITS had significantly higher mean craving than NITS when not smoking.
*p < .005. **p < .0001. ns = not significant.
Further analyses examined the curvilinear (quadratic) relationship between craving and smoking. The analysis showed an interaction effect for quadratic trends (p < .0001), which is visible in Figure 2. (The figure shows model-based estimates of the probability of smoking at each level of craving. The probability of smoking is centered at each group’s mean, to correct for different probabilities of smoking in the sample of observations obtained from the two groups.) Among DS, the probability of smoking rose with increased craving until craving reached the midpoint of the scale, and then leveled off. In contrast, among ITS, the probability of smoking kept rising as craving rose, even at high levels of craving.
Figure 2.

Modeled associations between rated craving intensity and changes in the probability of smoking (vs. randomly selected nonsmoking occasions). Data are presented as changes relative to the group average probability of smoking, because the absolute probability is influenced by the sampling scheme for smoking and nonsmoking occasions, which differs between groups (i.e., the prompting algorithm aimed to gather the same number of randomly sampled nonsmoking occasions for each group, even though the number of smoking occasions was very different for the two groups). The value of 0, marked by a line, represents each group’s average probability of an observation representing smoking (vs. a nonsmoking observation) within the dataset and is not comparable between nondaily intermittent smokers, ITS, (0.31) and daily smokers, DS, 0.71.
The data indicate that both DS and ITS experience intense craving. Table 2 describes the intensity of craving reports across groups. Nearly all individuals reported craving intensity above the midpoint (50) of the of 100-point scale at some point during monitoring, though DS were more likely to do so. The within-subject 95th percentile of reported craving among DS was significantly higher than that of ITS, though the ITS value was greater than 75 on the 100-point scale. The most intense craving possible—rating at 99 or 100—was also more commonly reported by DS, though it was also observed in a substantial fraction of ITS.
Table 2.
High-Intensity Craving Reports Across Groups
| DS | ITS | CITS | NITS | |
|---|---|---|---|---|
| 95th percentile, mean (SD) | 89.12 (14.47) | 77.71 (22.52)a | 80.36 (21.54) | 73.06 (23.01)b |
| Percentage of observations above 50 | 75.02 | 40.75a | 44.95 | 32.70b |
| Percentage of individuals ever rating craving above 50 | 99.26 | 95.80a | 97.27 | 95.10 |
| Percentage of observations, 99–100 | 14.77 | 5.00a | 5.79 | 2.55b |
| Percentage of individuals ever rating craving, 99–100 | 66.37 | 42.43a | 46.30 | 35.37 |
Note. DS = daily smokers; ITS = intermittent smokers; CITS = converted ITS; NITS = native ITS.
Craving ratings obtained via a visual analog (0–100) scale.
aSignificantly lower than DS at p < .05.
bSignificantly lower than CITS at p < .05.
Analyses of CITS versus NITS showed that craving was elevated in smoking episodes versus randomly sampled nonsmoking episodes, similarly in both groups (Figure 1). Craving was linearly related to smoking in both groups, with no significant interactions or curvilinear effects. CITS and NITS differed slightly in extremes of craving intensity reported (Table 2). Among CITS, the 95th percentile of rated craving was significantly higher than that among NITS. The groups did not differ in the percentage of subjects who reported craving above the scale midpoint (i.e., >50) or near the scale maximum (i.e., 99–100).
DISCUSSION
Detailed EMA data collected on dozens of occasions per subject demonstrated that ITS do experience craving—even intense craving—but in a pattern that differed from DS’ craving experience. DS not only reported moderate-intensity craving on smoking occasions, but also reported relatively high levels of craving (well above the scale midpoint) even when they were between cigarettes, despite the fact that they were smoking ad libitum. This echoes the observation that dependence among DS is most correlated with background tonic craving experienced between smoking episodes, rather than the phasic craving experienced at the time of smoking (Shiffman, Waters, & Hickcox, 2004). ITS, in contrast, reported substantial craving intensity (though not as high as DS) in situations where they had elected to smoke; when not smoking, however, their craving was well below the scale midpoint. Similar patterns were seen in nondependent chippers (Shiffman & Paty, 2006), who often smoke daily, but at low levels. The observed pattern of craving is consistent with the idea that ITS smoke in certain situations, where the appropriate cues or circumstances are present, but do not otherwise have an “endogenous” drive to smoke, as expressed in low levels of background craving. Laboratory cue reactivity data from this same sample was consistent with this, in that ITS increased craving in response to cue exposures. However, ITS were no more responsive to cues than DS were (Shiffman, Dunbar, Kirchner, Li, Tindle, Anderson et al., 2013). Alternatively, it is possible that the peaks of craving reported by ITS do not arise from the effects of cues, but may arise occasionally for other reasons. DiFranza et al. (2011) have suggested that cravings arise at regular intervals, with the intervals varying for different smokers and at different levels of dependence.
The data also indicated that ITS can experience not only moderate craving, but intense craving as well, with average 95th percentile of craving intensity approaching 80 out of 100, and almost half of ITS reporting maximal craving of 99 or 100 at some point during the study. If intense craving is indeed a distinct experience, ITS experience it too.
Analysis of the functional shape of the relationship between craving and smoking shed further light on how craving influences smoking differently in ITS versus DS. Among DS, the probability of smoking rose steeply as craving increased from the low end of craving intensity to the scale midpoint. After that point, however, there was little further increase in the probability of smoking. In other words, DS had a low craving threshold for smoking; once this was exceeded, more craving did not further increase the probability of smoking. (The fact that this curve goes flat at the midpoint of the craving scale may be why some studies fail to find a relationship between craving and smoking [Wray, Gass, & Tiffany, 2013]; the relationship weakens once craving passess the scale midpoint.) In contrast, ITS do not appear to reach such an asymptotic point: their smoking behavior is sensitive to craving increases throughout the range of intensities. This suggests that ITS’ smoking is actually more driven by craving than DS’, even though they smoke less and experience milder craving.
The observed pattern of data is consistent with the notion that DS’ smoking is driven, at least in part, by an internal drive to smoke, which persists constantly throughout the day, while ITS’ smoking may be driven by specific exposures to cues that increase craving and prompt smoking in particular situations. Thus, relative to DS, ITS’ craving is more variable and spans a greater range. In addition, their smoking demonstrates greater variability (Shiffman et al., 2012), which corresponds with the observed variations in craving intensity. Whether ITS’ variable craving and smoking are tied to cues, or whether these fluctuate for other reasons, remains to be examined.
The study findings need to be interpreted in light of its limitations. Although the EMA methods used have advantages, they still rely on self-report; subjects could have deliberately or unintentionally misrepresented their state or behavior. The daily period during which smokers made themselves available for assessment may have not included all of their waking hours. Also, EMA monitoring might have caused reactivity—changes in behavior due to assessment. However, reactivity is greatest when subjects are trying to change their smoking (McFall, 1977), and these subjects were not. Previous analyses of smoking (Shiffman et al., 2002) and other behaviors (Collins et al., 1998; Hufford, Shields, Shiffman, Paty, & Balabanis, 2002) have also found at most modest reactivity to EMA. Craving was measured with a single item. It has been suggested that multiitem measures have advantages of including broader content (Sayette et al., 2000), but the single item is highly reliable and there is evidence that a single item is as valid as multiitem questionnaires (West & Ussher, 2010).
At the same time, the study had considerable strengths. The EMA method allowed for real-time assessment, which avoided problems of recall. The dataset analyzed was robust, with data from hundreds of smokers and over 40,000 momentary measurements of craving. The availability of data from nonsmoking moments allowed for use of a case-cross-over design, with true evaluation of the within-person association between craving and smoking (Paty et al., 1992). The sample of smokers included considerable diversity, covering a large range of smoking rates.
In summary, analyses of extensive EMA data reveal that ITS do experience craving, including occasionally intense craving, despite smoking very little and displaying low or no tobacco dependence. The findings are consistent with the notion that craving is not necessarily a unique feature of addiction and may simply represent an in-the-moment desire to smoke (or eat, drink, etc., Drummond, 2001; Kassel & Shiffman, 1992; Orford, 2001) that can rise from processes other than dependence.
FUNDING
This work was supported by the National Institutes of Health, National Institute on Drug Abuse (R01-DA020742 to SS), the National Science Foundation Graduate Research Fellowship (to MSD), the National Cancer Institute (R25-CA057703-15 to MSD and R01-CA141596-02 to HAT), and Cancer Council Tasmania (F0019238 to SGF).
DECLARATION OF INTERESTS
SS consults to and has an interest in eRT, which provides electronic diary services for clinical research.
ACKNOWLEDGMENTS
The authors are grateful to Thomas Kirchner and Deborah Scharf for help launching this study and for input on study design; to Anna Tsivina, Joe Stafura, Rachelle Gish, and Aileen Butera for their work conducting research sessions; to Neha Mehta and Laura Homonnay-Demilio for editorial assistance; and to Ellen Beckjord for providing useful comments on a draft of this article.
REFERENCES
- Benowitz N. L. (2010). Nicotine addiction. The New England Journal of Medicine, 362, 2295–2303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2008a). Behavioral risk factor surveillance system survey data. Atlanta, GA: Centers for Disease Control and Prevention; Retrieved from www.cdc.gov/chronicdisease/resources/publications/AAG/brfss.htm [Google Scholar]
- Centers for Disease Control and Prevention. (2008b). Cigarette smoking among adults—United States, 2007. Morbidity and Mortality Weekly Report, 57, 1221–1226 [PubMed] [Google Scholar]
- Collins R. L., Morsheimer E. T., Shiffman S., Paty J. A., Gnys M., Papandonatos G. D. (1998). Ecological momentary assessment in a behavioral drinking moderation training program. Experimental and Clinical Psychopharmacology, 6, 306–315. 10.1037/1064-1297.6.3.306 [DOI] [PubMed] [Google Scholar]
- DiFranza J. R., Wellman R. J., Mermelstein R., Pbert L., Klein J. D., Sargent J. D., … Winickoff J. P. (2011). The natural history and diagnosis of nicotine addiction. Current Reviews in Pediatrics, 72, 88–96 [Google Scholar]
- Drummond D. C. (2001). Theories of drug craving, ancient and modern. Addiction (Abingdon, England), 96, 33–46. 10.1046/j.1360-0443.2001.961333.x [DOI] [PubMed] [Google Scholar]
- Ferguson S. G., Shiffman S. (2009). The relevance and treatment of cue-induced cravings in tobacco dependence. Journal of Substance Abuse Treatment, 36, 235–243. 10.1016/j.jsat.2008.06.005 [DOI] [PubMed] [Google Scholar]
- Hufford M. R., Shields A. L., Shiffman S., Paty J., Balabanis M. (2002). Reactivity to ecological momentary assessment: An example using undergraduate problem drinkers. Psychology of Addictive Behaviors, 16, 205–211. 10.1037/0893-164X.16.3.205 [PubMed] [Google Scholar]
- Kalton G. (1983). Introduction to survey sampling. (SAGE University Paper series on Quantitative Applications in the Social Sciences, series no. 07-035). Beverly Hills and London: SAGE Publications, Inc [Google Scholar]
- Kassel J. D., Shiffman S. (1992). What can hunger teach us about drug craving? A comparative analysis of the two constructs. Advances in Behaviour Therapy and Research, 14, 141–167 [Google Scholar]
- Kozlowski L. T., Wilkinson D. A. (1987). Use and misuse of the concept of craving by alcohol, tobacco, and drug researchers. British Journal of Addiction, 82, 31–45 [DOI] [PubMed] [Google Scholar]
- McFall R. M. (1977). Parameters of self-monitoring. In Stuart R. B. (Ed.), Behavioral self-management: Strategies, techniques, and outcome (pp. 196–214). New York: Brunner/Mazel [Google Scholar]
- Nguyen Q. B., Zhu S. H. (2009). Intermittent smokers who used to smoke daily: A preliminary study on smoking situations. Nicotine & Tobacco Research, 11, 164–170. 10.1093/ntr/ntp012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orford J. (2001). Addiction as excessive appetite. Addiction (Abingdon, England), 96, 15–31. 10.1046/j.1360-0443.2001.961152.x [DOI] [PubMed] [Google Scholar]
- Paty J. A., Kassel J. D., Shiffman S. (1992). Assessing stimulus control of smoking: The importance of base rates. In de Vries H. (Ed.), The experience of psychopathology. Cambridge, U.K.: Cambridge University Press [Google Scholar]
- Robinson T. E., Berridge K. C. (2000). The psychology and neurobiology of addiction: an incentive-sensitization view. Addiction (Abingdon, England), 95 (Suppl 2), S91–S117. 10.1046/j.1360-0443.95.8s2.19.x [DOI] [PubMed] [Google Scholar]
- Rose J. S., Dierker L. C., Donny E. (2010). Nicotine dependence symptoms among recent onset adolescent smokers. Drug Alcohol Dependence, 106, 126–132. 10.1016/j.drugalcdep.2009.08.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sayette M. A., Shiffman S., Tiffany S. T., Niaura R. S., Martin C. S., Shadel W. G. (2000). The measurement of drug craving. Addiction (Abingdon, England), 95 (Suppl 2), S189–S210. 10.1046/j.1360-0443.95.8s2.8.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sayette M. A., Tiffany S. T. (2013). Peak provoked craving: An alternative to smoking cue-reactivity. Addiction (Abingdon, England), 108, 1019–1025. 10.1111/j.1360-0443.2012.04013.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schane R. E., Glantz S. A., Ling P. M. (2009). Nondaily and social smoking: An increasingly prevalent pattern. Archives of Internal Medicine, 169, 1742–1744. 10.1001/archinternmed.2009.315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S. (2009). Light and intermittent smokers: Background and perspective. Nicotine & Tobacco Research, 11, 122–125. 10.1093/ntr/ntn020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Dunbar M., Kirchner T., Li X., Tindle H., Anderson S., Scholl S. (2013). Smoker reactivity to cues: Effects on craving and on smoking behavior. Journal of Abnormal Psychology, 122, 264–280. 10.1037/a0028339 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Dunbar M. S., Kirchner T. R., Li X., Tindle H. A., Anderson S. J., … Ferguson S. G. (2013). Cue reactivity in non-daily smokers: Effects on craving and on smoking behavior. Psychopharmacology, 226, 321–333. 10.1007/s00213-012-2909-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Dunbar M. S., Scholl S. M., Tindle H. A. (2012). Smoking motives of daily and non-daily smokers: A profile analysis. Drug and Alcohol Dependence, 126, 362–368. 10.1016/j.drugalcdep.2012.05.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Ferguson S. G., Dunbar M. S., Scholl S. M. (2012). Tobacco dependence among intermittent smokers. Nicotine & Tobacco Research, 14, 1372–1381. 10.1093/ntr/nts097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Gwaltney C. J., Balabanis M. H., Liu K. S., Paty J. A., Kassel J. D., … Gnys M. (2002). Immediate antecedents of cigarette smoking: An analysis from ecological momentary assessment. Journal of Abnormal Psychology, 111, 531–545. 10.1037/0021-843X.111.4.531 [DOI] [PubMed] [Google Scholar]
- Shiffman S., Kirchner T. R., Ferguson S. G., Scharf D. M. (2009). Patterns of intermittent smoking: An analysis using Ecological Momentary Assessment. Addictive Behaviors, 34, 514–519. 10.1016/j.addbeh.2009.01.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Paty J. (2006). Smoking patterns and dependence: Contrasting chippers and heavy smokers. Journal of Abnormal Psychology, 115, 509–523. 10.1037/0021-843X.115.3.509 [DOI] [PubMed] [Google Scholar]
- Shiffman S., Paty J. A., Gnys M., Kassel J. D., Hickcox M. (1996). First lapses to smoking: Within-subjects analyses of real-time reports. Journal of Consulting and Clinical Psychology, 64, 366–379. 10.1037/0022-006X.64.2.366 [DOI] [PubMed] [Google Scholar]
- Shiffman S., Tindle H., Li X., Scholl S., Dunbar M., Mitchell-Miland C. (2012). Characteristics and smoking patterns of intermittent smokers. Experimental and Clinical Psychopharmacology, 20, 264–277. 10.1037/a0027546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S., Waters A., Hickcox M. (2004). The Nicotine Dependence Syndrome Scale: A multidimensional measure of nicotine dependence. Nicotine & Tobacco Research, 6, 327–348. 10.1080/1462220042000202481 [DOI] [PubMed] [Google Scholar]
- Stolerman I. P., Jarvis M. J. (1995). The scientific case that nicotine is addictive. Psychopharmacology (Berl), 117, 2–10. 10.1007/BF02245088 [DOI] [PubMed] [Google Scholar]
- Stone A. A., Shiffman S. (1994). Ecological momentary assessment (EMA) in behavioral medicine. Annals of Behavioral Medicine, 16, 199–202 [Google Scholar]
- Substance Abuse and Mental Health Services Administration. (2009). Results from the 2008 National Survey on Drug Use and Health: National findings. Rockville, MD: NSDUH Series Office of Applied Studies; Retrieved from http://store.samhsa.gov/product/Mental-Health-Findings-Results-from-the-2009-National-Survey-on-Drug-Use-and-Health-NSDUH-/SMA10-4609 [Google Scholar]
- Tiffany S. T., Wray J. M. (2012). The clinical significance of drug craving. Annals of the New York Academy of Sciences, 1248, 1–17. 10.1111/j.1749-6632.2011.06298.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tindle H. A., Shiffman S. (2011). Smoking cessation behavior among intermittent smokers versus daily smokers. American Journal of Public Health, 101, e1–e3. 10.2105/AJPH.2011.300186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trinidad D. R., Pérez-Stable E. J., Emery S. L., White M. M., Grana R. A., Messer K. S. (2009). Intermittent and light daily smoking across racial/ethnic groups in the United States. Nicotine & Tobacco Research, 11, 203–210. 10.1093/ntr/ntn018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- West R., Ussher M. (2010). Is the ten-item Questionnaire of Smoking Urges (QSU-brief) more sensitive to abstinence than shorter craving measures? Psychopharmacology, 208, 427–432. 10.1007/s00213-009-1742-x [DOI] [PubMed] [Google Scholar]
- Wray J. M., Gass J. C., Tiffany S. T. (2013). A systematic review of the relationships between craving and smoking cessation. Nicotine & Tobacco Research, 15, 1167–1182. 10.1093/ntr/nts268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeger S. L., Liang K. Y., Albert P. S. (1988). Models for longitudinal data: A generalized estimating equation approach. Biometrics, 44, 1049–1060 [PubMed] [Google Scholar]