

Abstract
Background
Prostatic abscesses are an uncommon disease usually caused by enterobacteria. They mostly occur in immunodeficient patients. It is thus extremely rare to have a Staphylococcal prostatic abscess in a young immunocompetent patient.
Case presentation
A 20-year-old patient was treated with ofloxacin for a suspicion of prostatitis. An ultrasonography was performed because of persisting symptoms and showed acute urinary retention and prostatic abscesses. So the empirical antibiotic therapy was modified with ceftriaxone/amikacin. The disease worsened to severe sepsis and the patient was admitted in ICU. CT-scan and MRI confirmed three abscesses with perirectal infiltration and the bacteriological samples (abscesses and blood cultures) were positive to methicillin-susceptible Staphylococcus aureus producing Panton-Valentine leukocidine. The treatment was changed with fosfomycin/ofloxacin which resulted in a general improvement and the regression of the abscesses.
Conclusion
Staphyloccocus aureus producing Panton-Valentine leukocidin are most commonly responsible for skin and soft tissue infections. To this day, no other case of prostatic abscess due to this strain but susceptible to methicillin has been described.
Electronic supplementary material
The online version of this article (doi:10.1186/1471-2334-14-466) contains supplementary material, which is available to authorized users.
Keywords: Prostatic abscess, Staphylococcus aureus, Panton-valentine leukocidin, Severe sepsis
Background
Prostatic abscesses have become uncommon and their incidence has dropped since the introduction of antibiotics [1]. They are mostly due to enterobacteria, especially Escherichia coli. Sometimes Staphylococcus aureus is involved [2] and most of the cases are due to methicillin-resistant strains in patients with immunodeficiency risk factors. These patients generally present with chronic or subacute infections which rarely progress into severe sepsis or septic shock. Some Staphylococcus aureus strains can produce Panton-Valentine leukocidin (PVL), this toxin being a virulence factor. We present here a case of prostatic abscesses due to methicillin-susceptible Staphylococcus aureus (MSSA) producing PVL in an immunocompetent patient.
Case presentation
A 20-year-old patient was admitted in the hospital because of dysuria and burning during micturition. His medical history was unremarkable except for allergic asthma and recurrent furuncles for a year and a half with a negative HIV serology. Urine culture performed 1 day after symptoms appearance, showed a leukocyturia without bacteriuria so it did not require any treatment. Two days later, as the symptoms persisted, laboratory tests disclosed an inflammatory syndrome including a hyperleukocytosis (25,060 white blood cells/mm3) with a majority of neutrophilic leukocytes, a thrombocytosis and an increased level of C-Reactive protein (CRP) at 109 mg/L. Bladder ultrasound revealed a full bladder which resulted in the insertion of a suprapubic catheter and the initiation of oral ofloxacin. The patient was discharged home but presented again two days later with abdominal and pelvic pain. New laboratory tests showed persisting inflammatory syndrome and coagulation disorders (PT at 48%). The antibiotic therapy was replaced by ceftriaxone and amikacin. The prostate ultrasound revealed two abscesses and a transrectal needle aspiration collected 15 ml of purulent fluid with Gram positive cocci at gram stain.Six days later, condition worsened moving to severe sepsis with hyperthermia, chills and hypotension. The laboratory tests showed a worsening of the inflammatory syndrome (hyperleukocytosis = 43,000 white blood cells/mm3) and of the coagulation disorders (PT at 31%) and a hyperlactatemia at 2.90 mmol/l. Persistent perirectal abscesses were evidenced on the pelvic magnetic resonance imaging (MRI) (Figure 1). Ciprofloxacin was then added and the patient was transferred in the intensive care unit (ICU).
Figure 1.
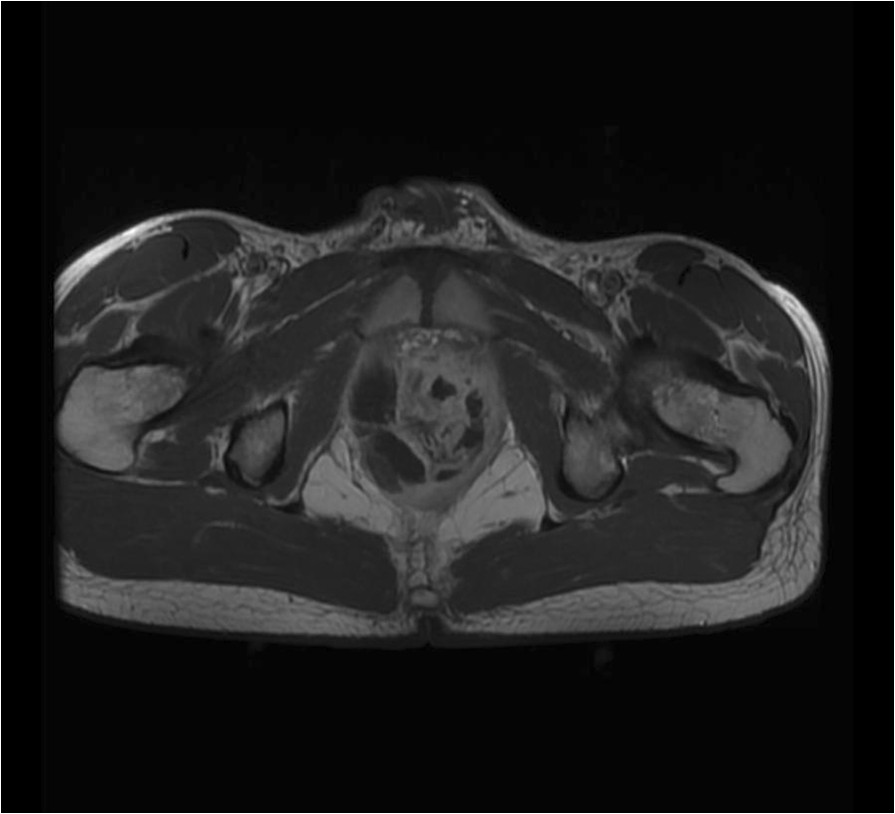
Pelvic MRI at D0. Pelvic MRI at D0 showing multiple intra-prostatic abscesses: the biggest ones are situated in the right lobe.
At admission, the patient was hemodynamically unstable with a blood pressure at 98/52 mmHg requiring fluid resuscitation. The abdomen was painful. A CT-scan evidenced a clear prostatic hypertrophy with several abscesses (20 × 15 × 33 mm; 64 × 21 × 26 mm and 38 × 10 × 30 mm), a perianal infiltration and retroperitoneal, lateral-aortic and presacral enlarged nodes (Figure 2). Microbiological samples from prostatic abscesses and blood cultures were positive for MSSA producing PVL. Antimicrobial susceptibility tests showed that the strain was multisusceptible except for penicillin G, tetracycline and trimethoprim-sulfamethoxazole. Due to the atypical clinical presentation including multiple abscesses, we investigated by PCR the presence of genes encoding PVL [3] that was positive. Molecular characterization, performed by the French National Reference Centre for Staphylococci, using DNA microarray (Alere StaphyType DNA microarray; Alere Technologies GmbH, Jena, Germany), highlighted that the strain has an agr allele type 4, and was assigned to clonal complex CC121 [4] (MLST ST 121). Data confirmed that the strain harboured PVL genes but also genes encoding enterotoxins B, K and Q and the egc cluster. Treatment with fosfomycin and ofloxacin was started at admission (D0) without need for surgery.Apyrexia was obtained within 48 hours and the inflammatory syndrome improved. An echocardiography ruled out endocarditis. The antibiotic therapy lasted six weeks and was changed at D16 for oral rifampicin and ofloxacin. On the same day, control MRI showed a decline of the perirectal infiltration and a disappearance of the collection in the left side of the prostate (Figure 3). The suprapubic catheter was retrieved at D10 and patient’s micturition was normal again.
Figure 2.
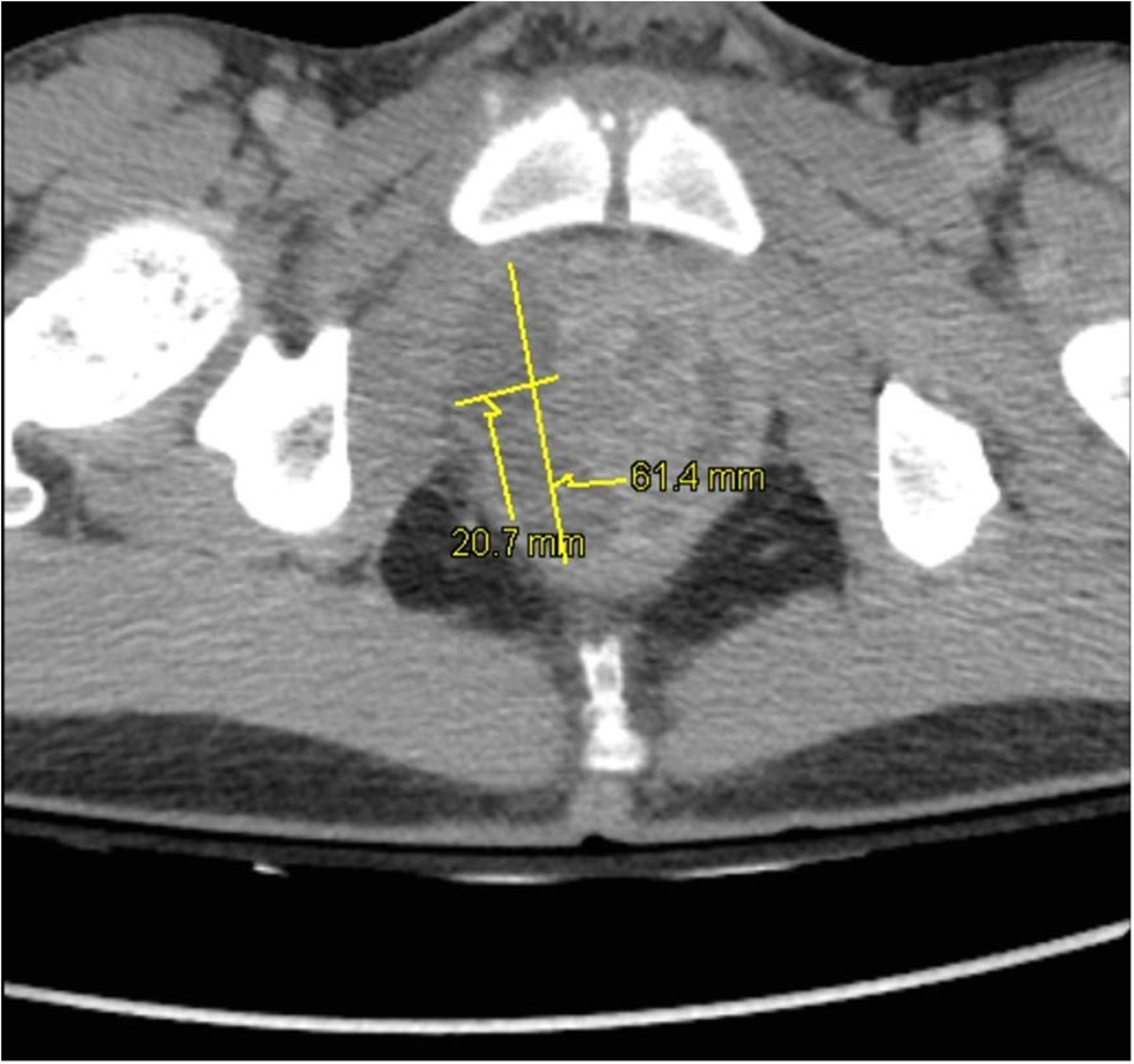
Pelvic CT-scan. Pelvic CT-scan showing prostatic hypertrophy and intra-prostatic abscesses: 20 × 15 × 33 mm and 64 × 21 × 26 mm in the right lobe and 38 × 10 × 30 mm in the left lobe.
Figure 3.
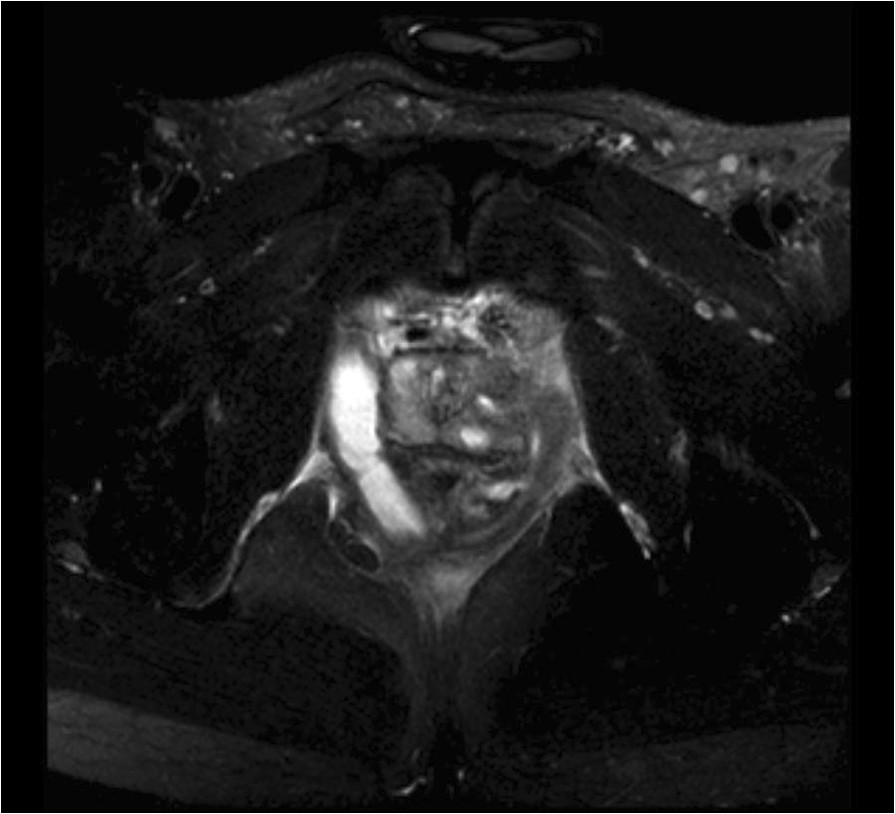
Pelvic MRI at D16. Control pelvic MRI at D16 showing regression of the abscesses in the left lobe and persistence in the right lobe.
Evaluation for an oropharyngeal and nasal Staphylococcus aureus carriage realised by swab on day 17 was negative.
Discussion and conclusions
Prostatic abscesses have become rare since the onset of antibiotics and are found in 0.5 to 2.5% of patients with a prostate inflammation [1]. They mostly occur in patients with local risk factors (urine retention, indwelling urethral catheter, chronic prostatitis…) or immunodeficiency risk factors [5].
The gold-standard for prostatic abscesses diagnostic is still transrectal ultrasonography [5, 6]. It allows a needle aspiration which is used to confirm the diagnostic and identify the microorganism involved [7]. CT-scan and MRI are useful to assess extension around the prostate or to look for remote focuses [8].
The most common etiologic agent is Escherichia coli but Staphylococcus aureus is often associated with prostatic abscesses [2]. Several cases of prostatic abscesses due to community-acquired methicillin-resistant Staphylococcus aureus (MRSA) have been reported in the literature [9–12]. In our case, the etiologic agent was MSSA producing PVL. Prevalence of Staphylococcus aureus producing PVL seems to have increased for several years: in 1995, Prevost et al. study reported 5% of strains in Western Europe [13] whereas in 2012, 36% of strains producing PVL were reported in the United-States [14]. This statement is particularly true for the USA. In Europe, it is unclear whether the prevalence has truly increased or if it is due to increased ascertainement. Moreover, in Europe, there is clonal heterogeneity [15]. In the USA, there is a strong association between strains producing PVL and MRSA [14]. In Europe, Australia and Africa, there is a high proportion of MSSA producing PVL [16–19]. In our case the strain producing PVL was susceptible to methicillin. MSSA strains producing PVL are often from the clonal complex CC121, ST 121 [20, 21].
The PVL is a synergohymenotropic toxin that acts through the association of two components F and S. It destroys cells by creating pores in the membrane [22] and is responsible for leukocyte and macrophage destruction and tissue necrosis. Its role in the pathogenesis and the spreading of infections is still unclear [23]. Strains producing PVL are usually linked with skin infections such as furuncles and abscesses, with necrotising pneumonia [23] and with bone and joint infections [24] that mostly occur in healthy children and young adults.
PVL may contribute to the infection severity and be a virulence factor. This could explain that our patient presented with severe sepsis. Studies conducted in animals showed that PVL led to the persistence of infection and made its local extension easier [25]. Other studies highlighted a higher frequency of hemoptysis, general signs (tachycardia, low blood pressure, polypnea and cyanosis) and deaths in pneumonia caused by Staphylococcus aureus producing PVL, which illustrates the virulence of the toxin [22]. In 2013, Shallcross et al. showed in a meta-analysis that infections were most likely to recur and surgery performed more often in skin and soft tissue infections caused by strains producing PVL [26]. Of note, the patient had a history of repetitive furuncles for a year and a half which could be linked with recurrence. To our knowledge, this is the first case of prostatic abscess due to Staphylococcus aureus producing PVL with the toxin possibly responsible for the severe sepsis.
Prostatic abscesses treatment usually includes an antibiotic therapy adapted to the microorganism and drainage of the abscess. Ultrasound-guided transrectal needle aspiration must be preferred to surgical drainage or transurethral prostatic resection as the needle path is shorter and the tolerance rate higher [27]. The antibiotic treatment aims at eradicating Staphylococcus aureus but it must also decrease the toxin effects. In 2008, a study evidenced the ability of linezolid, clindamycin and rifampicin to inhibit PVL production [28].
Prostatic abscesses must be searched for in all patients presenting with prostatitis symptoms associated with abdominal pain. A Staphylococcus aureus origin must be suspected if the disease worsens and develops to severe sepsis despite an adapted antibiotic therapy, especially in a young subject. Moreover, if this pathogen producing PVL is discovered, an antibiotic therapy including toxin inhibition must be started.
Consent
Written informed consent was obtained from the patient for publication of this case report and of the images associated. A copy of the written consent is available for review by the Editor of this journal.
Acknowledgments
We thank Sarah Demai who provided medical writing services.
Abbreviations
- CRP
C-Reactive protein
- HIV
Human immunodeficiency virus
- ICU
Intensive care unit
- MRI
Magnetic resonance imaging
- MRSA
Methicillin-resistant Staphylococcus aureus
- MSSA
Methicillin-susceptible Staphylococcus aureus
- PCR
Polymerase chain reaction
- PVL
Panton-Valentine leukocidin
- PT
Prothrombin time.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Footnotes
Competing interests
The authors declare that they have no competing interest.
Authors’ contribution
MD, BF 1) acquisition and interpretation of data 2) article drafting 3) approved version. OB, ALF, FF, FL, YB, AC 1) acquisition of data 2) article revision 3) approved version. All authors read and approved the final manuscript.
Contributor Information
Maria Dubos, Email: dubos.maria@gmail.com.
Olivier Barraud, Email: olivier.barraud@chu-limoges.fr.
Anne-Laure Fedou, Email: anne-laure.fedou@chu-limoges.fr.
Fabien Fredon, Email: fabien.fredon@chu-limoges.fr.
Frédéric Laurent, Email: frederic.laurent@chu-lyon.fr.
Yannis Brakbi, Email: yannisbra@yahoo.fr.
Anne Cypierre, Email: anne.cypierre@chu-limoges.fr.
Bruno François, Email: b.francois@unilim.fr.
References
- 1.Langer JE, Cornud F. Inflammatory disorders of the prostate and the distal genital tract. Radiol Clin North Am. 2006;44(5):665–677. doi: 10.1016/j.rcl.2006.07.004. [DOI] [PubMed] [Google Scholar]
- 2.Weinberger M, Cytron S, Servadio C, Block C, Rosenfeld JB, Pitlik SD. Prostatic abscess in the antibiotic era. Rev Infect Dis. 1988;10(2):239–249. doi: 10.1093/clinids/10.2.239. [DOI] [PubMed] [Google Scholar]
- 3.Lina G, Piémont Y, Godail-Gamot F, Bes M, Peter MO, Gauduchon V, Vandenesch F, Etienne J. Involvement of panton-valentine leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis. 1999;29(5):1128–1132. doi: 10.1086/313461. [DOI] [PubMed] [Google Scholar]
- 4.Monecke S, Coombs G, Shore AC, Coleman DC, Akpaka P, Borg M, Chow H, Ip M, Jatzwauk L, Jonas D, Kadlec K, Kearns A, Laurent F, O’Brien FG, Pearson J, Ruppelt A, Schwarz S, Scicluna E, Slickers P, Tan HL, Weber S, Ehricht R. A field guide to pandemic, epidemic and sporadic clones of methicillin-resistant staphylococcus aureus. PLoS One. 2011;6(4):e17936. doi: 10.1371/journal.pone.0017936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Granados EA, Riley G, Salvador J, Vincente J. Prostatic abscess: diagnosis and treatment. J Urol. 1992;148(1):80–82. doi: 10.1016/s0022-5347(17)36516-3. [DOI] [PubMed] [Google Scholar]
- 6.Barozzi L, Pavlica P, Menchi I, De Matteis M, Canepari M. Prostatic abscess: diagnosis and treatment. AJR Am J Roentgenol. 1998;170(3):753–757. doi: 10.2214/ajr.170.3.9490969. [DOI] [PubMed] [Google Scholar]
- 7.Cytron S, Weinberger M, Pitlik SD, Servadio C. Value of transrectal ultrasonography for diagnosis and treatment of prostatic abscess. Urology. 1988;32(5):454–458. doi: 10.1016/0090-4295(88)90427-X. [DOI] [PubMed] [Google Scholar]
- 8.Ludwig M, Schroeder-Printzen I, Schiefer HG, Weidner W. Diagnosis and therapeutic management of 18 patients with prostatic abscess. Urology. 1999;53(2):340–345. doi: 10.1016/S0090-4295(98)00503-2. [DOI] [PubMed] [Google Scholar]
- 9.Beckman TJ, Edson RS. Methicillin-resistant staphylococcus aureus prostatitis. Urology. 2007;69(4):779.e1–779.e3. doi: 10.1016/j.urology.2007.02.018. [DOI] [PubMed] [Google Scholar]
- 10.Fraser TG, Smith ND, Noskin GA. Persistent methicillin-resistant staphylococcus aureus bacteremia due to a prostatic abscess. Scand J Infect Dis. 2003;35(4):273–274. doi: 10.1080/00365540310004045. [DOI] [PubMed] [Google Scholar]
- 11.Baker SD, Horger DC, Keane TE. Community-acquired methicillin-resistant staphylococcus aureus prostatic abscess. Urology. 2004;64(4):808–810. doi: 10.1016/j.urology.2004.05.009. [DOI] [PubMed] [Google Scholar]
- 12.Park SC, Lee JW, Rim JS. Prostatic abscess caused by community-acquired methicillin-resistant staphylococcus aureus. Int J Urol. 2011;18(7):536–538. doi: 10.1111/j.1442-2042.2011.02774.x. [DOI] [PubMed] [Google Scholar]
- 13.Prevost G, Couppie P, Prevost P, Gayet S, Petiau P, Cribier B, Monteil H, Piemont Y. Epidemiological data on staphylococcus aureus strains producing synergohymenotropic toxins. J Med Microbiol. 1995;42(4):237–245. doi: 10.1099/00222615-42-4-237. [DOI] [PubMed] [Google Scholar]
- 14.Brown ML, O’Hara FP, Close NM, Mera RM, Miller LA, Suaya JA, Amrine-Madsen H. Prevalence and sequence variation of panton-valentine leukocidin in methicillin-resistant and methicillin-susceptible staphylococcus aureus strains in the United States. J Clin Microbiol. 2012;50(1):86–90. doi: 10.1128/JCM.05564-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Otter JA, French GL. Molecular epidemiology of community-associated maticillin-resistant staphylococcus aureus in Europe. Lancet Infect Dis. 2010;10(4):227–239. doi: 10.1016/S1473-3099(10)70053-0. [DOI] [PubMed] [Google Scholar]
- 16.Bennett CM, Coombs GW, Wood GM, Howden BP, Johnson LE, White D, Johnson PD. Community-onset staphylococcus aureus infections presenting to general practices in South-eastern Australia. Epidemiol Infect. 2014;142(3):501–511. doi: 10.1017/S0950268813001581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Oosthuysen WF, Orth H, Lombard CJ, Sinha B, Wasserman E. Population structure analyses of Staphylococcus aureus at Tygerberg Hospital, South Africa, reveals a diverse population, a high prevalence of Panton-Valentine leukocidin genes, and unique local methicillin-resistant S. aureus clones. Clin Microbiol Infect. 2013;20(7):652–659. doi: 10.1111/1469-0691.12452. [DOI] [PubMed] [Google Scholar]
- 18.Shallcross LJ, Williams K, Hopkins S, Aldridge RW, Johnson AM, Hayward AC. Panton-Valentine leukocidin associated staphylococcal disease: a cross-sectional study at a London hospital, England. Clin Microbiol Infect. 2010;16(11):1644–1648. doi: 10.1111/j.1469-0691.2010.03153.x. [DOI] [PubMed] [Google Scholar]
- 19.Vorobieva V, Bazhukova T, Hanssen AM, Caugant DA, Semenova N, Haldorsen BC, Simonsen GS, Sundsfjord A. Clinical isolates of Staphylococcus aureus from the Arkhangelsk region, Russia: antimicrobial susceptibility, molecular epidemiology, and distribution of Panton-Valentine leukocidin genes. APMIS. 2008;116(10):877–887. doi: 10.1111/j.1600-0463.2008.01092.x. [DOI] [PubMed] [Google Scholar]
- 20.Monecke S, Müller E, Dorneanu OS, Vremeră T, Ehricht R. Molecular typing of MRSA and of clinical Staphylococcus aureus isolates from Iaşi, Romania. PLoS One. 2014;9(5):e97833. doi: 10.1371/journal.pone.0097833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rasigade J-P, Laurent F, Lina G, Meugnier H, Bes M, Vandenesch F, Etienne J, Tristan A. Global distribution and evolution of panton-valentine leukocidin-positive methicillin-susceptible Staphylococcus aureus, 1981–2007. J Infect Dis. 2010;201(10):1589–1597. doi: 10.1086/652008. [DOI] [PubMed] [Google Scholar]
- 22.Gillet Y, Issartel B, Vanhems P, Fournet JC, Lina G, Bes M, Vandenesch F, Piémont Y, Brousse N, Floret D, Etienne J. Association between staphylococcus aureus strains carrying gene for panton-valentine leukocidin and highly lethal necrotising pneumonia in young immunocompetent patients. Lancet. 2002;359(9308):753–759. doi: 10.1016/S0140-6736(02)07877-7. [DOI] [PubMed] [Google Scholar]
- 23.Voyich JM, Otto M, Mathema B, Braughton KR, Whitney AR, Welty D, Long RD, Dorward DW, Gardner DJ, Lina G, Kreiswirth BN, DeLeo FR. Is panton-valentine leukocidin the major virulence determinant in community-associated methicillin-resistant staphylococcus aureus disease? J Infect Dis. 2006;194(12):1761–1770. doi: 10.1086/509506. [DOI] [PubMed] [Google Scholar]
- 24.Dohin B, Gillet Y, Kohler R, Lina G, Vandenesch F, Vanhems P, Floret D, Etienne J. Pediatric bone and joint infections caused by panton-valentine leukocidin-positive staphylococcus aureus. Pediatr Infect Dis J. 2007;26(11):1042–1048. doi: 10.1097/INF.0b013e318133a85e. [DOI] [PubMed] [Google Scholar]
- 25.Crémieux A-C, Dumitrescu O, Lina G, Vallee C, Côté JF, Muffat-Joly M, Lilin T, Etienne J, Vandenesch F, Saleh-Mghir A. Panton–valentine leukocidin enhances the severity of community-associated methicillin-resistant staphylococcus aureus rabbit osteomyelitis. PLoS One. 2009;4(9):e7204. doi: 10.1371/journal.pone.0007204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shallcross LJ, Fragaszy E, Johnson AM, Hayward AC. The role of the panton-valentine leucocidin toxin in staphylococcal disease: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13(1):43–54. doi: 10.1016/S1473-3099(12)70238-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Collado A, Palou J, García-Penit J, Salvador J, de la Torre P, Vicente J. Ultrasound-guided needle aspiration in prostatic abscess. Urology. 1999;53(3):548–552. doi: 10.1016/S0090-4295(98)00570-6. [DOI] [PubMed] [Google Scholar]
- 28.Dumitrescu O, Badiou C, Bes M, Reverdy M-E, Vandenesch F, Etienne J, Lina G. Effect of antibiotics, alone and in combination, on panton–valentine leukocidin production by a staphylococcus aureus reference strain. Clin Microbiol Infect. 2008;14(4):384–388. doi: 10.1111/j.1469-0691.2007.01947.x. [DOI] [PubMed] [Google Scholar]
Pre-publication history
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/14/466/prepub