

Abstract
Objective:
To find the prevalence of keratin metaplasia and its relation with clinico-pathological profile of the odontogenic cyst.
Materials and Methods:
Odontogenic cysts were studied histologically with special stains to identify the presence of keratin and compared with various parameters such as underlying connective tissue inflammation, average epithelial thickness, and site of the cyst, type of the cyst, age and the sex of the patient.
Results:
Of 71 cases of various odontogenic cysts, 26 (36.6%) cases exhibited keratinization in the epithelial lining. In cysts with severe inflammation there is absence of keratinization.
Conclusions:
This study reveals higher prevalence of keratin metaplasia in the odontogenic cysts. Furthermore, inflammation is found to be one of factor influencing keratin metaplasia.
KEY WORDS: Cyst, dentigerous radicular and residual cyst, keratin metaplasia, odontogenic cyst
The odontogenic cysts are derived from epithelium associated with the development of the dental apparatus.[1] The commonly reported metaplastic changes in the literature of the odontogenic epithelium are keratinization,[2] mucous cell,[3,4,5] and ciliated cell[6,7,8,9] as an adaptive change to various environmental pressures. This study was carried out to find the prevalence of keratin metaplasia in epithelial lining of odontogenic cyst and to compare the metaplastic changes with various parameters such as underlying connective tissue inflammation, average epithelial thickness, and site of the cyst, type of the cyst, age and the sex of the patient.
Materials and Methods
Histopathologically confirmed, 71 cases of odontogenic cysts were retrieved from the archives, which included 24 dentigerous cysts, 38 radicular cysts and 9 residual cysts. Two sections of 6 μm thickness were prepared from each of the 71 cysts, out of which one section was stained with the hematoxylin and eosin stain[10] for general appraisal, and the other was stained with modified Papanicolaou technique[11] for detecting keratinization. Along with the histopathological findings, respective age and sex of the patients, and site of the cyst was recorded. Apart from this, the grade of inflammation and average epithelial thickness was assessed. The underlying connective tissue inflammation was recorded arbitrarily as mild/moderate/severe based on the severity of the inflammatory features. Average epithelial thickness was calculated by counting the number of cells in full thickness cross-sections of the epithelium at three random points on the each cystic epithelial lining.
Results
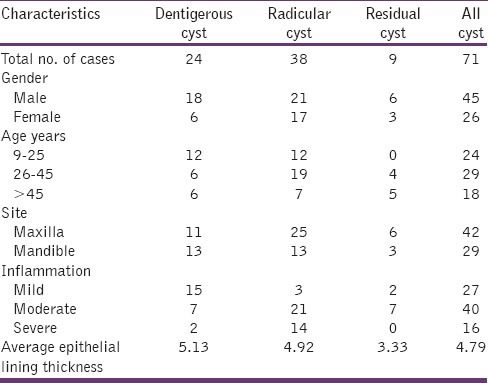
The clinico-pathological profile of the 71 cases of odontogenic cyst is shown in Table 1. The age of the patient ranged from 9 to 68 years with a mean age of 32.8 years. For statistical analysis the age of the patient and average epithelial thickness of the cystic lining was arbitrarily divided into three groups in order to analyze any association with change in the value of these parameters, as shown in Table 1.
Table 1.
Clinico-pathologic profile odontogenic cysts
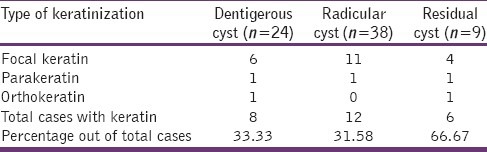
Of the total 71 cases, 26 cases (36.6%) exhibited some form of keratinization. According to cyst type various form of keratinization seen are shown Table 2. It is to be noted that out of 26 cases only 5 cases shown widespread keratinization (3 parakeratin and 2 orthokeratin), whereas rest of the 21 cases shown keratinization of group of epithelial cells, especially in the superficial layer of epithelial lining of odontogenic cyst.
Table 2.
Distribution of keratinization according to the type of cyst
Discussion
It is known that the term keratin metaplasia was used for the presence of keratinized epithelial cells in the lining of radicular and dentigerous cysts.[2,12,13] In our study also, the keratinization was considered as a metaplastic change, because of the fact that the lining epithelium of the odontogenic cyst is derived from the remnants of odontogenic epithelium. If this keratinization has occurred in the lining epithelium of odontogenic cyst, it is to be considered as an adaptive change to environmental causes existing within the cyst.
According to the type of the cyst, it was found that, eight out of 24 (33.3%) dentigerous cysts, 12 out of 26 (31.6%) radicular cyst and six out of 9 (66.7%) residual cyst exhibited keratinization. Our result did not confer with that of Browne,[2] who reported that the keratin was present only in 2.5% of the dentigerous cysts and 2% of the dental cysts. High and Hirschmann[3] studied age changes in 33 residual cysts and found (0%) no evidence of keratin formation in any of the cysts.
In our opinion, the vast difference between the prevalence of keratin formation is probably due to the application of special stain, modified Papanicolaou technique[11] in this study, which is a more sensitive stain for the presence of keratin. It was inferred that the previous studies relied upon hematoxylin and eosin stain for the evaluation of presence of keratin. The reason for keratin formation in the odontogenic cyst was described as metaplasia but, the factors responsible are poorly understood. Elsewhere, genetic factors, location, mechanical stress, radiation,[14] inflammation, the nature of lamina propria,[15] vitamin A deficiency,[16] lack of oxygen and nourishment[17] were ascribed as the factors affecting keratinization.
In our study, we found that there is an increased prevalence of keratin metaplasia in the residual cyst type, especially in the older age group (>45 years) and in cases with more than five layers of epithelial thickness, but not to the level of statistical significance. Interestingly, when compared to cases with mild inflammation, there was a greater amount of keratinization in cases with moderate inflammation, but total absence in case of severe inflammation. This influence of inflammation on the keratinization is highly significant in statistical analysis. In our study, this may be explained that the presence of mild to moderate inflammation may be responsible for the increase in average epithelial thickness (mild hyperplasia) leading to active event of keratinization as a differentiation process. However, severe inflammation may prove lethal to epithelial cells; thus, there is a break in further progression to the level of keratinization. Furthermore, it has been reported that there is a decreased level of keratinization wherever there is increased inflammation in gingiva.[15] In our study, we found no correlation between keratin formation and the sex of the patient or the site of the cyst.
Though more evidence of keratin metaplasia occurring in the cystic lining is inferred from the our study results, carcinoma arising from the cystic lining is known to be a very rare phenomenon.[18,19,20,21] In addition, malignant transformation in the odontogenic cyst is also reported in the absence of keratin metaplasia.[22,23] Therefore, there is no justification in regarding an odontogenic cyst with keratin metaplasia as a precancerous lesion.[13] Hence, the clinical significance of odontogenic cyst showing keratin metaplasia is still unknown.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Cohen B. The enigma of vestigial tissues. Ann R Coll Surg Engl. 1976;58:104–14. [PMC free article] [PubMed] [Google Scholar]
- 2.Browne RM. Metaplasia and degeneration in odontogenic cysts in man. J Oral Pathol. 1972;1:145–58. doi: 10.1111/j.1600-0714.1972.tb01655.x. [DOI] [PubMed] [Google Scholar]
- 3.High AS, Hirschmann PN. Age changes in residual radicular cysts. J Oral Pathol. 1986;15:524–8. doi: 10.1111/j.1600-0714.1986.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 4.Hodson JJ. Muco-epidermoid odontogenic cysts of the jaws with special reference to those in the mandible. Proc R Soc Med. 1956;49:637–9. [PMC free article] [PubMed] [Google Scholar]
- 5.Slabbert H, Shear M, Altini M. Vacuolated cells and mucous metaplasia in the epithelial linings of radicular and residual cysts. J Oral Pathol Med. 1995;24:309–12. doi: 10.1111/j.1600-0714.1995.tb01190.x. [DOI] [PubMed] [Google Scholar]
- 6.Gorlin RJ. Potentialities of oral epithelium namifest by mandibular dentigerous cysts. Oral Surg Oral Med Oral Pathol. 1957;10:271–84. doi: 10.1016/0030-4220(57)90092-0. [DOI] [PubMed] [Google Scholar]
- 7.Marsland EA, Browne RM. Two odontogenic cysts, partially lined with ciliated epithelium. Oral Surg Oral Med Oral Pathol. 1965;19:502–7. doi: 10.1016/0030-4220(65)90013-7. [DOI] [PubMed] [Google Scholar]
- 8.Takeda Y, Oikawa Y, Furuya I, Satoh M, Yamamoto H. Mucous and ciliated cell metaplasia in epithelial linings of odontogenic inflammatory and developmental cysts. J Oral Sci. 2005;47:77–81. doi: 10.2334/josnusd.47.77. [DOI] [PubMed] [Google Scholar]
- 9.Yamazaki M, Cheng J, Nomura T, Saito C, Hayashi T, Saku T. Maxillary odontogenic keratocyst with respiratory epithelium: A case report. J Oral Pathol Med. 2003;32:496–8. doi: 10.1034/j.1600-0714.2003.00149.x. [DOI] [PubMed] [Google Scholar]
- 10.Bancroft JD, Gamble M. London: Churchill Livingstone; 2002. Theory and Practice of Histological Techniques. [Google Scholar]
- 11.Elzay RP. A modification of the Papanicolaou exfoliative cytology stain to demonstrate keratin in paraffin-block tissue sections. Oral Surg Oral Med Oral Pathol. 1983;56:51–3. doi: 10.1016/0030-4220(83)90055-5. [DOI] [PubMed] [Google Scholar]
- 12.Browne RM, Gough NG. Mlignnt chnge in the epithelium lining odontogenic cysts. Cancer. 1972;29:1199–207. doi: 10.1002/1097-0142(197205)29:5<1199::aid-cncr2820290511>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 13.Shear M, Speight P. Oxford: Blackwell Munksgaard; 2007. Cysts of the Oral and Maxillofacial Regions. [Google Scholar]
- 14.Adams D. Keratinization of the oral epithelium. Ann R Coll Surg Engl. 1976;58:351–8. [PMC free article] [PubMed] [Google Scholar]
- 15.Kumar GS, editor. New Delhi: Elsevier; 2008. Orbans's Oral Histology and Embroyology. [Google Scholar]
- 16.Kumar V, Abbas AK, Fausto N. New Delhi: WB Saunders Company; 2004. Robbins and Cotron Pathologic Basis of Disease. [Google Scholar]
- 17.Fischer A. The differentiation and keratinization of epithelium in vitro. J Exp Med. 1924;39:585–8. doi: 10.1084/jem.39.4.585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Scheer M, Koch AM, Drebber U, Kübler AC. Primary intraosseous carcinoma of the jaws arising from an odontogenic cyst – A case report. J Craniomaxillofac Surg. 2004;32:166–9. doi: 10.1016/j.jcms.2003.12.005. [DOI] [PubMed] [Google Scholar]
- 19.Swinson BD, Jerjes W, Thomas GJ. Squamous cell carcinoma arising in a residual odontogenic cyst: Case report. J Oral Maxillofac Surg. 2005;63:1231–3. doi: 10.1016/j.joms.2005.04.016. [DOI] [PubMed] [Google Scholar]
- 20.Yasuoka T, Yonemoto K, Kato Y, Tatematsu N. Squamous cell carcinoma arising in a dentigerous cyst. J Oral Maxillofac Surg. 2000;58:900–5. doi: 10.1053/joms.2000.8219. [DOI] [PubMed] [Google Scholar]
- 21.Yoshida H, Onizawa K, Yusa H. Squamous cell carcinoma arising in association with an orthokeratinized odontogenic keratocyst. Report of a case. J Oral Maxillofac Surg. 1996;54:647–51. doi: 10.1016/s0278-2391(96)90653-9. [DOI] [PubMed] [Google Scholar]
- 22.Fanibunda K, Soames JV. Malignant and premalignant change in odontogenic cysts. J Oral Maxillofac Surg. 1995;53:1469–72. doi: 10.1016/0278-2391(95)90680-0. [DOI] [PubMed] [Google Scholar]
- 23.Kramer HS, Scribner JH. Squamous-cell carcinoma arising in a dentigerous cyst. report of a case. Oral Surg Oral Med Oral Pathol. 1965;19:555–61. doi: 10.1016/0030-4220(65)90019-8. [DOI] [PubMed] [Google Scholar]