

Abstract
Mandibular first molar commonly has two roots, the mesial and the distal root. Surprisingly in some mandibular first molar has an unusual extra third root in between mesial and distal root. This extra root is the most commonly seen in lingual side and is called as radix entomolaris. If this extra root is seen on the buccal side, it is termed as radix paramolaris (RP), which is a very rare phenomenon. Recently, various case report studies has shown the presence of third canal in the mesial and distal roots of mandibular molars. They are named as middle mesial and middle distal canal, respectively. Here, we present a case report of mandibular second molar showing three canals in the mesial root and a RP.
KEY WORDS: Middle mesial canal, radix entomolaris, radix paramolaris
The primary objective of the endodontic treatment relies on identification and complete cleaning of the root canal system. Root canal morphology possesses anatomical variations that might contribute to endodontic failures. Thus, the success of endodontic treatment relies on thorough knowledge of the root canal anatomy.[1,2,3] Vertucci and William described the presence of independent three canals in mesial root of mandibular first molar. Since then, the unusual middle mesial and middle distal canals associated with mandibular first molar has been reported in many clinical studies and case reports. Similarly, the number of roots and root canals also varies. The extra third root in the mandibular molar was mentioned first in the literature by Carabelli[4] is called as radix entomolaris (RE).[5] This supernumerary root located distolingually in mandibular molars (mainly in first molars). Therefore, the additional root if located in the mesiobuccal side is called as radix paramolaris (RP). Here, a case report describes the root canal treatment in a mandibular second molar with three independent mesial canal orifices exiting in three foramen and a RP.
Case Report
The case we present here is about a 22-year-old female patient referred to the Department of conservative dentistry and endodontics with the chief complaint of pain in the left lower back tooth for the past 2 days. The pain is of mild, intermittent, and throbbing nature. Her medical history was noncontributory and she gave a dental history of root canal treatment was done in that tooth before 2 months in a dental clinic. On clinical examination, it was found access opening was done in a grossly decayed left mandibular second molar. The tooth was tender on vertical percussion. On palpation in buccal and lingual vestibule, there was no tender on palpation. Tooth mobility and periodontal probing around the tooth were within normal limits. 2% lignocaine in 1:100000 adrenaline local anesthesia was given as inferior alveolar nerve block. The treatment was continued by complete caries excauation and canal exploration after rubber dam isolation. On microscopic exploration of the floor of the pulp chamber a canal was found present between mesial and distal roots on buccal side. On radiographically, the file placed in it was found as extra root like RE. RE is an extra third root in mandibular molars present on the lingual side, which is shorter in length than other two roots. However, here, it is seen on buccal side called as RP. On careful exploration on mesial root, presence of three canals was suspected and the middle mesial canal was identified. The distal root had single canal. After working length estimation done [Figure 1], all the canals were enlarged until 20 size K file and biomechanical preparation was completed by protaper rotary systems. All three mesial canals were enlarged until F1, distal canal until F3 and the extra third root on buccal side until F2 with copious irrigation of saline simultaneously. Then the master cones checkup were done as shown in Figure 2. Then the final irrigation was done with 17% ethylenediaminetetraacetic acid, 3% sodium hypochlorite and by saline. Canals were dried with paper points and obturated with Gutta-percha cones of respective sizes with kerr sealer. Then the access was closed with zinc oxide eugenol cement [Figure 3]. Figure 4 shows the post obturation magnified view of floor of the pulp chamber showing the five canals with RP in middle.
Figure 1.
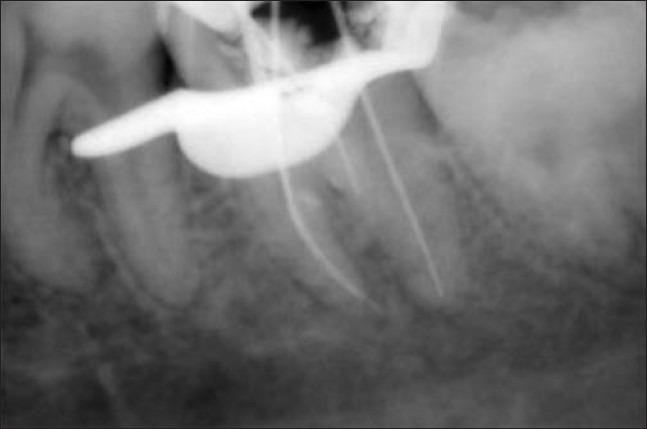
Working length determination
Figure 2.

Master cone check up
Figure 3.

Post obturation radiograph
Figure 4.
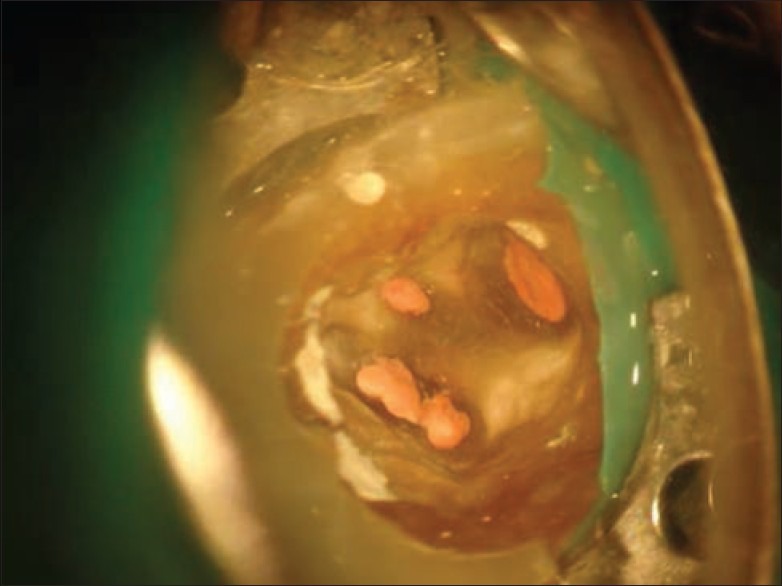
Microscopic image of floor of pulp chamber showing type B RP
Discussion
The mandibular molars usually have two roots with two canals in mesial roots and one canal in distal root. It is more common that mandibular molars having four canals with two in mesial and distal root viz. the first molar. However, recent studies shows there are more chance for a 3rd canal in mesial and distal root as middle mesial and middle distal, respectively. This presence in second molar is very rare but, recently few studies of Ryan et al. and Jain reported with cases of five or six canals in mandibular first molars only.[6,7] The isthmus connecting the mesiobuccal and lingual or distobuccal and lingual is debrided and left uninstrumented in most of the cases. However, on careful exploration of this isthmus a third canal with a separate path of exit can be seen in many of the cases as reported by Deepalakshmi et al. in their four cases.[8]
Here, in this case of 37 with three mesial canals, all three files and Gp points went until full working length independently without any fusion at the apex to exit as one. It seems that in all three canals, there will be isthmus communicating them in between laterally as it travel, these lateral connections were debrided completely with 3% sodium hypochlorite and sealed by the root canal sealer. RE is an extra third root in mandibular molar, which is shorter than the mesial and distal roots; seen in distolingual corner like a distolingual canal in the floor of the chamber.[9,10] However, in this case, the extra root is seen in buccal version. The buccal version of the extra third root was commonly term as RP.[10] The RP occurrence rate is about 0%, 2%, and 5% in mandibular first, second and third molars respectively.[10] Carlsen and Alexandersen described two different types of RP: Type A: RP in which the cervical part is located on the mesial root complex; Type B: RP in which the cervical part is located centrally, between the mesial and distal root complexes, an additional cusp was present on the buccal side.[11] This present case belongs to Type B of RP.
Conclusion
The complex root canal anatomy stresses the operator to observe the canal morphology with care without underestimating it and missing the extra root and roots canals, which can occur in any cases as a rare finding. Thus, the success of endodontics lies in the careful exploration of the canals and debridement of it. “Expect the unexpectations though it is rare.”
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Hess W. Part 1. New York: William Wood and Co; 1925. The Anatomy of the Root-Canals of the Teeth of the Permanent Dentition. [Google Scholar]
- 2.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 3.Vertucci JF, Haddix EJ, Britto RL. Tooth morphology and access cavity preparation. In: Cohen S, Hargreaves MK, editors. Pathways of Pulp. 9th ed. St. Louis, Mo, USA: Mosby Elsevier; 2006. pp. 203–4. [Google Scholar]
- 4.Carabelli G. 2nd ed. Vienna: Braumullerund Seidel; 1844. Systemic handbook of Dentistry: Historical overview of dentistry; p. 114. [Google Scholar]
- 5.Bolk L. Bemerkungen of root-variations on the human lower molar. Zeiting for morphology and anthropology. 1915;17:605–10. [Google Scholar]
- 6.Ryan JL, Bowles WR, Baisden MK, McClanahan SB. Mandibular first molar with six separate canals. J Endod. 2011;37:878–80. doi: 10.1016/j.joen.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 7.Jain S. Mandibular first molar with three distal canals. J Conserv Dent. 2011;14:438–9. doi: 10.4103/0972-0707.87223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Deepalakshmi M, Karumaran CS, Miglani R, Indira R. Independent and confluent middle mesial root canals in mandibular first molars: A report of four cases. Case Rep Dent 2012. 2012:103125. doi: 10.1155/2012/103125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: An endodontic challenge. Int Endod J. 2004;37:789–99. doi: 10.1111/j.1365-2591.2004.00870.x. [DOI] [PubMed] [Google Scholar]
- 10.Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: Clinical approach in endodontics. J Endod. 2007;33:58–63. doi: 10.1016/j.joen.2006.05.007. [DOI] [PubMed] [Google Scholar]
- 11.Carlsen O, Alexandersen V. Radix entomolaris: Identification and morphology. Scand J Dent Res. 1990;98:363–73. doi: 10.1111/j.1600-0722.1990.tb00986.x. [DOI] [PubMed] [Google Scholar]