

Abstract
Objective.
To extend the empirical evidence regarding the predictors of older adults’ use of information and communications technology (ICT) and to further examine its relationship to depressive symptoms and well-being.
Method.
This cross-sectional study utilized a sample of community-dwelling older adults from the National Health and Aging Trends Study (N = 6,443). Structural equation modeling was used to estimate the effects of predictor variables on ICT use and the effects of use on depressive symptoms and well-being. Tests of moderation by demographic characteristics and level of ICT use were also performed.
Results.
Socioeconomic status (SES), age, and cognitive function accounted for approximately 60% of the variance in ICT use. SES was a stronger predictor for Blacks/African Americans, whereas cognitive function was a stronger predictor for Whites. ICT use was unrelated to depressive symptoms or well-being. However, it acted as a moderator, such that limitations in activities of daily living (ADLs) was a stronger predictor of depressive symptoms for high ICT users, whereas ill-health was a stronger predictor for non/limited users.
Discussion.
Findings do not support the claim that ICT use directly enhances mental health or well-being among older adults although it may protect against depressive symptoms for individuals coping with health conditions other than ADL impairments.
Key Words: Cognition, Depression, Health, ICT, Mental Health, Technology, Well-being.
Older adults’ use of information and communications technology (ICT), including computers, the Internet, and mobile communication devices (Selwyn, Gorard, Furlong, & Madden, 2003) has increased considerably over the past decade. For example, a recent survey estimated that 53% of adults aged 65 and older are Internet users (Zickuhr & Madden, 2012) compared with 22% in 2004 (Fox, 2004) although it is not clear to what extent such growth is due to the movement of higher use cohorts into this age demographic (i.e., cohort effects) versus growing use over time more generally (i.e., period effects). Cognizant of this trend, social scientists have sought to understand the specific purposes for which older adults use ICT, identify the factors that contribute to higher levels of use, and determine whether and how ICT use is related to mental health and well-being in this population.
Research examining the sociodemographic correlates of ICT use among older adults has indicated that the average user is younger and has more education and income than the average nonuser (Fazeli, Ross, Vance, & Ball, 2013; Spooner & Rainie, 2000; Wagner, Hassanein, & Head, 2010). Differences across racial/ethnic groups have also been observed, with Whites reporting greater Internet access and use than Blacks/African Americans and Hispanics/Latinos (Czaja et al., 2006; Livingston, Parker, & Fox, 2009; Spooner & Rainie, 2000), a gap that may reflect corresponding disparities in socioeconomic status (SES). In addition, men in this age group have typically reported greater computer experience and Internet use than women (Czaja et al., 2006; Fallows, 2005; Karavidas, Lim, & Katsikas, 2005). Although age and educational attainment have consistently predicted older adults’ ICT use (Wagner et al., 2010), effects of gender and income have been less robust (Carpenter & Buday, 2007; Werner, Carlson, Jordan-Marsh, & Clark, 2011).
In addition to sociodemographic characteristics, ICT use in this population has been related to attitudinal variables, including computer-specific anxiety, self-efficacy, and interest (Ellis & Allaire, 1999; Fazeli et al., 2013; Karavidas et al., 2005). Research has also supported a relationship between ICT use and cognitive function among older adults. Although score on a brief test of cognitive impairment was unrelated to the likelihood of computer use (Carpenter & Buday, 2007), multiple studies utilizing more extensive cognitive testing have shown that better performance is associated with greater computer use or experience (Fazeli et al., 2013; Tun & Lachman, 2010). In a longitudinal study (Freese, Rivas, & Hargittai, 2006), performance on a test of cognitive ability in high school predicted Internet use at age 65 although only for men. In contrast, results pertaining to associations with health and social network–related variables have been inconsistent (Carpenter & Buday, 2007; Gracia & Herrero, 2009; Werner et al., 2011). Furthermore, only one study to date has examined activities of daily living (ADLs), reporting a positive association between computer use and functional independence (Carpenter & Buday, 2007).
Given several preliminary or inconsistent results and that low statistical power may be responsible for certain null findings, further empirical investigation is needed to understand the factors that promote or support ICT use among older adults (Freese et al., 2006). Findings may have implications for the design of computer/Internet training programs and other efforts to narrow the “digital divide” facing older adults and racial/ethnic minorities in particular (Czaja et al., 2006). However, the broader importance of these findings is also linked to the question of whether ICT use contributes to mental health and well-being in this population. As theorized in the literature, there are several mechanisms by which various uses of ICT may be conducive to the social, mental, and emotional well-being of older adults (Slegers, Boxtell, & Jolles, 2008). E-mail is the most common computer-based activity among older adults although their use of text messaging and social networking sites is increasing (Carpenter & Buday, 2007; Karavidas et al., 2005; Smith, 2011; Zickuhr & Madden, 2012). The use of ICT for communication purposes may provide greater opportunity for supportive social interaction (Cody, Dunn, Hoppin, & Wendt, 1999; Slegers et al., 2008), a consistent predictor of health and well-being in older adulthood (Fiori, Antonucci, & Cortina, 2006; Pinquart & Sorensen, 2000). Similarly, ICT use may help to reduce loneliness, an important risk factor for depressive symptoms in older adults (Barg et al., 2006; Cacioppo, Hughes, Waite, Hawkley, & Thisted, 2006). ICT may also be used for leisure and entertainment, as well as for instrumental purposes (i.e., seeking heath information, banking, and shopping), potentially increasing quality of life and preserving a sense of autonomy (Selwyn et al., 2003; Slegers et al., 2008).
Despite the many hypothesized benefits of ICT use for older adults, the results of research examining its relationship to mental health and well-being in this population have been inconclusive. Studies have reported that computer and/or Internet use are related to greater perceived social support and connection (Cody et al., 1999), self-efficacy (Erickson & Johnson, 2011), life satisfaction (Karavidas et al., 2005; Shapira, Barak, & Gal, 2007), and psychological well-being (Chen & Persson, 2002; Koopman-Boyden & Reid, 2009; Shapira et al., 2007), as well as lower depression (Cotten, Ford, Ford, & Hale, 2012; McConatha, McConatha, & Dermigny, 1994; Shapira et al., 2007) and loneliness (Choi, Kong, & Jung, 2012). However, other observational and experimental studies with older adults have failed to find significant associations of ICT use with similar outcome variables (Billipp, 2001; Fazeli et al., 2013; Fokkema & Knipscheer, 2007; White et al., 2002). A randomized controlled study, for instance, found that learning to use a computer and the Internet over a 1-year period had no effect on measures of loneliness, mood, quality of life, and autonomy (Slegers et al., 2008). Dickinson and Gregor (2006) suggest that the inconsistent results in the extant literature are due to small and nonrepresentative study samples, misattributions of causality, and the confounding effect of social interactions in several intervention-based studies.
The objective of this study was twofold: to extend the empirical evidence concerning the predictors of older adults’ ICT use and to clarify the relationship of ICT use to mental health and well-being in this population. We sought to build upon the existing literature in several ways. First, we used data from the National Health and Aging Trends Study (NHATS), thereby employing several methodological features that address limitations of prior studies, including the increased statistical power and generalizability afforded by a large and demographically diverse sample, a multifaceted measure of ICT use, and a relatively comprehensive set of predictor variables. Second, previous studies have typically conducted regression analyses examining technology use as either an independent or dependent variable. In this study, we employed a structural equation modeling (SEM) approach to simultaneously estimate the effects of predictor variables on ICT use, and in turn, the effects of use on depressive symptoms and well-being. SEM has several advantages over multiple regression techniques, including iterative model fit solutions, exclusion of error variance, and incorporation of latent variables (Byrne, 2010; Kline, 2011). Third, although prior studies have considered only whether level of ICT use differs by age, gender, and race/ethnicity, we also conducted test of moderation to determine whether the relationships of ICT use to predictor and outcome variables differ across these demographic lines. Finally, we are not aware of any prior studies that have examined interactions of ICT use with other variables in predicting mental health or well-being. Therefore, we examined ICT use as a potential moderator of associations between predictor variables and depressive symptoms.
Method
Participants
We analyzed data from the first wave of the National Health and Aging Trends Study (NHATS), a longitudinal study in which a nationally representative sample of more than 8,000 Medicare beneficiaries aged 65 and older will be surveyed annually. Extensive face-to-face interviews, conducted in 2011, collected information pertaining to a broad array of topics, including home and facility environments; health conditions; physical, cognitive, and social functioning; and economic status. The study employed a stratified multistage sampling design, with selection probabilities designed to ensure sufficient sample sizes by age group and race/ethnicity (Montaquila, Freedman, Edwards, & Kasper, 2012). Non-Hispanic Blacks/African Americans and individuals in older age groups were oversampled. Consistent with previous studies, we selected a community sample and thus excluded participants who resided in nursing homes and other residential care facilities. We also excluded blind participants and those who reported a diagnosis of Alzheimer’s disease or another type of dementia. Because the analysis included several self-report and cognitive performance measures, we excluded cases in which data was collected from a proxy respondent. The resulting sample included 6,483 respondents. In addition, we excluded a small number of outliers in multivariate analyses, resulting in a final sample of 6,443 respondents.
Measures
ICT use.
From the set of technology-related survey items (Table 2), we derived two variables measuring different facets of ICT use.
Table 2.
Prevalence of Various Uses of Information and Communications Technology
| Percentagesa | ||
|---|---|---|
| Community sample, N = 6,483 | Full NHATS sample,b N = 7,609 | |
| Has a working telephone that is not a cellphone | 90.7% | 89.9% |
| Has a working cell phone | 80.8% | 75.9% |
| Has a working computer in place of residence (and knows how to use a computer) | 67.3% | 61.1% |
| No computer in residence but has used a computer somewhere else in the past month | 2.3% | 2.2% |
| Has sent messages by e-mail or text message within the past month | 44.2% | 40.2% |
| Rarely | 7.5% | 6.9% |
| Some days | 12.8% | 11.7% |
| Most days | 23.9% | 21.5% |
| Has gone on the Internet or online for any reason other than e-mail/texting in the past month | 46.9% | 42.7% |
| Has gone on the Internet or online to do the following: | ||
| Shop for groceries or personal items | 15.1% (32.3%) | 13.7% (32.0%) |
| Pay bills or do banking | 21.2% (45.2%) | 19.2% (44.9%) |
| Order or refill prescriptions | 8.5% (18.2%) | 7.7% (18.0%) |
| Contact any medical provider | 7.6% (16.2%) | 6.9% (16.1%) |
| Handle Medicare or other health insurance matters | 5.7% (12.2%) | 5.1% (12.0%) |
| Get information about health conditions | 17.1% (36.5%) | 15.7% (36.7%) |
Note. Numbers in parentheses refer to the percentage of respondents who have gone on the Internet or online for any reason other than e-mail/texting within the past month.
aWeighted.
bConsists of all respondents who completed the SP (subject person) questionnaire, including those who responded via proxy.
A communications technology variable was measured on a four-point ordinal scale (0 = had not e-mailed or texted within the past month; 1 = e-mailed or texted rarely; 2 = e-mailed or texted some days; 3 = e-mailed or texted most days). An information technology variable was also measured on a four-point scale (0 = did not have or use a computer; 1 = had or used a computer but had not gone on the Internet; 2 = had used the Internet but not for both shopping/banking and health-related purposes; 3 = used the Internet for at least one activity in each category).
SES.
SES variables included measures of education and income. Education was measured on a nine-point ordinal scale reflecting participants’ reported highest academic degree or level of schooling completed. Our measure of total household income utilized reported income data where available. Missing values were replaced with the median value across five income imputations provided in the NHATS data set, which were generated using a hot deck procedure (Montaquila, Freedman, & Kasper, 2012). This variable was extremely skewed and kurtotic due to a small number of high-income outliers. Therefore, we excluded cases with total incomes of $300,000 or greater, which represented less than 1% of the data points.
Cognitive function.
The NHATS survey battery included objective measures of functioning in multiple cognitive domains. A clock drawing test was conducted to assess executive function (Shulman, 2000). Verbal memory was assessed with immediate and delayed word recall tests similar to those used in the Health and Retirement Study (Ofstedal, Fisher, & Herzog, 2005). Participants are shown and read a list of 10 nouns and are asked to recall as many as possible, both immediately and again after a 5-min delay. Scores on these tests were averaged to derive a measure of memory function.
Ill-health.
Following Carpenter and Buday (2007), we attempted to represent both subjective and objective dimensions of physical health. Therefore, we included a self-rated overall health variable, measured on a five-point Likert scale (1 = excellent; 2 = very good; 3 = good; 4 = fair; 5 = poor). To represent the objective dimension, a composite measure of chronic disease burden was also constructed, with one point for each reported diagnosis, from a medical physician, of seven specific chronic conditions, including heart disease, high blood pressure, osteoporosis, arthritis, diabetes, lung disease, and cancer.
Limitations in ADLs.
The NHATS survey collects data on limitations in several key areas of daily functioning, including mobility, household activities, and self-care, focusing on respondents’ self-reported ability to perform these activities independently (with any assistive devices or aids, if used), and their level of difficulty when doing so. Dichotomous measures of requiring help or having difficulty on tasks in these domains were shown to have acceptable reliability in a separate validation study (Freedman et al., 2011). Activities subsumed under mobility included going outside, getting around inside, and getting out of bed; self-care activities included eating, dressing, bathing, and toileting; and household activities included laundry, shopping, making hot meals, and banking/paying bills. A measure of limitations was constructed for each domain, with a point allocated for each activity in which the respondent reported having difficulty or requiring assistance.
Social integration.
We included a measure of social integration similar to one utilized in another population-based study (Ertel, Glymour, & Berkman, 2008). Participants were asked whether or not they had, in the past month, ever engaged in several activities likely to involve social interaction, including visiting family or friends in person, attending religious services, participating in clubs, classes, or other organized activities, volunteering, providing care for another person, and going out for enjoyment. For reasons discussed in the following section, these items were grouped into two variables. A point was allocated for each endorsed activity, as well as for currently being married or living with a partner.
Depressive symptoms.
The Patient Health Questi onnaire-2 (PHQ-2; Kroenke, Spitzer, & Williams, 2003), a truncated version of the PHQ-9, is a two-item measure designed to screen for depression. It asks about depressed mood and anhedonia, at least one of which is required for a diagnosis of major depression in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). In the NHATS survey, respondents were asked to rate how often, over the past month, they have “had little interest or pleasure in doing things” and “felt down, depressed, or hopeless.” Both items are rated on a four-point Likert scale ranging from “not at all” to “nearly every day,” and continuous measures were utilized in analyses. Although a high score on the PHQ-2 is not a sufficient basis for a clinical diagnosis, the measure has been shown to have adequate construct validity, as well as sensitivity and specificity in identifying possible depression in older adult as well as primary care populations (Kroenke et al., 2003; Li, Friedman, Conwell, & Fiscella, 2007).
Well-being.
The NHATS survey included seven items (α = .59), asking respondents to rate, on a three-point Likert scale (1 = not at all; 2 = a little; 3 = a lot), their agreement with several statements reflecting aspects of well-being. These items are adapted from validated measures of psychological well-being (Ryff & Keyes, 1995) and sense of control (Lachman & Weaver, 1998) used in other population-based studies. Based on the results of exploratory factor analyses reported subsequently, we constructed three indicator variables to represent the underlying construct of well-being; these were labeled self-realization (“my life has meaning and purpose,” “I feel confident and good about myself”), perceived control/mastery (“I like my living situation very much,” “when I really want to do something, I usually find a way to do it,” “I have an easy time adjusting to change”), and resignation (“I gave up trying to improve my life a long time ago,” “other people determine most of what I can and cannot do”; both items reverse coded). For all three variables, higher scores were indicative of greater well-being.
Analytic Strategy
We utilized SEM to simultaneously estimate the effects of age, SES, cognitive function, ill-health, ADL limitations, and social integration on ICT use, and in turn, the effects of use on depressive symptoms and well-being, with a separate model for each outcome. The individual items and derived measures described in the previous section served as observed indicators of these latent variables in measurement and structural models. Item parceling was employed in the construction of two latent variables (Coffman & MacCallum, 2005). For the social integration variable, individual items were randomly allocated to one of two indicators. For the well-being variable, we drew upon the results of an exploratory factor analysis (EFA) in constructing three indicators, taking the average score across the individual survey items that loaded on a given factor (Coffman & MacCallum, 2005).
All SEM analyses were conducted using AMOS, version 21.0. Data were screened for missing values, outliers, and univariate and multivariate nonnormality. Variables that had missing values on more than 1% of data points included memory (1.6%), executive function (3.1%), and the three well-being indicators (1.4%–2.4%). Missing values were imputed using a full information maximum likelihood (ML) procedure. The literature in this area suggests that ML estimates are subject to the least bias resulting from any violations of missing-at-random assumptions (Little & Rubin, 1989; Muthen, Kaplan, & Hollis, 1987). As is common, the data were multivariate kurtotic. Therefore, we also conducted an alternative analysis using asymptotic distribution free (ADF) estimation, a technique that is free of normality assumptions. Due to the high statistical power afforded by the large sample size, the significance threshold for parameter estimates was set at an alpha level of .01.
Because most latent variables were measured with only two indicators, lack of model identification precluded performing a confirmatory factor analysis (CFA) on each latent variable separately. Therefore, overall measurement models including the set of latent variables were specified and tested using CFA. Because a validated scale measuring well-being was not available in the existing data set, we utilized a cross-validation strategy to model this latent outcome variable. Several goodness-of-fit measures were utilized to evaluate model fit. Although the chi-square statistic for the traditional Likelihood Ratio Test is reported, its sensitivity to sample size limits its practical utility in evaluating model fit with large sample sizes (Byrne, 2010; MacCallum, Browne, & Sugawara, 1996). Therefore, we selected other common goodness-of-fit measures, including the root mean square error of approximation (RMSEA), which is sensitive to model parsimony while correcting for sample size; the comparative fit index (CFI), which compares the hypothesized model with a baseline independence model; and the PCFI, a parsimony-adjusted fit index tied to the CFI (Byrne, 2010; Kline, 2011). Commonly used interpretive guidelines suggest that good model fit is indicated by RMSEA values smaller than .05 (Browne & Cudeck, 1993), CFI values greater than .95 (Hu & Bentler, 1999), and PCFI values greater than .50 (Mulaik et al., 1989).
Following assessment of the measurement models, we tested a structural model in which the exogenous latent variables of SES, memory, ill-health, ADL limitations, and social integration, along with the observed variable age, predict ICT use, which in turn predicts depressive symptoms (Model 1), as shown in Figure 1. Direct paths from the exogenous variables to depressive symptoms were also specified to control for these effects. We then tested the same model with well-being replacing depressive symptoms as the outcome variable (Model 2). Next, to investigate any moderation of the associations between ICT use and other variables by gender (Model 3), age (Model 4), and race/ethnicity (Model 5), we performed multigroup analyses testing for invariance of structural path (regression) coefficients across these demographic groups. Finally, we examined ICT use as a potential moderator of the associations between the predictor variables and depressive symptoms (Model 6). The model was thus respecified to remove the ICT use latent variable. For the sake of simplicity and given the greater reliability of a validated outcome measure (PHQ-2), this analysis was conducted only with depressive symptoms as the outcome variable. All analyses were weighted to adjust for oversampling as well as for design effects resulting from the complex sampling methodology employed in NHATS (Hahs-Vaughn & Lomax, 2006; Kaplan & Ferguson, 1999; Montaquila, Freedman, Spillman, & Kasper, 2012).
Figure 1.
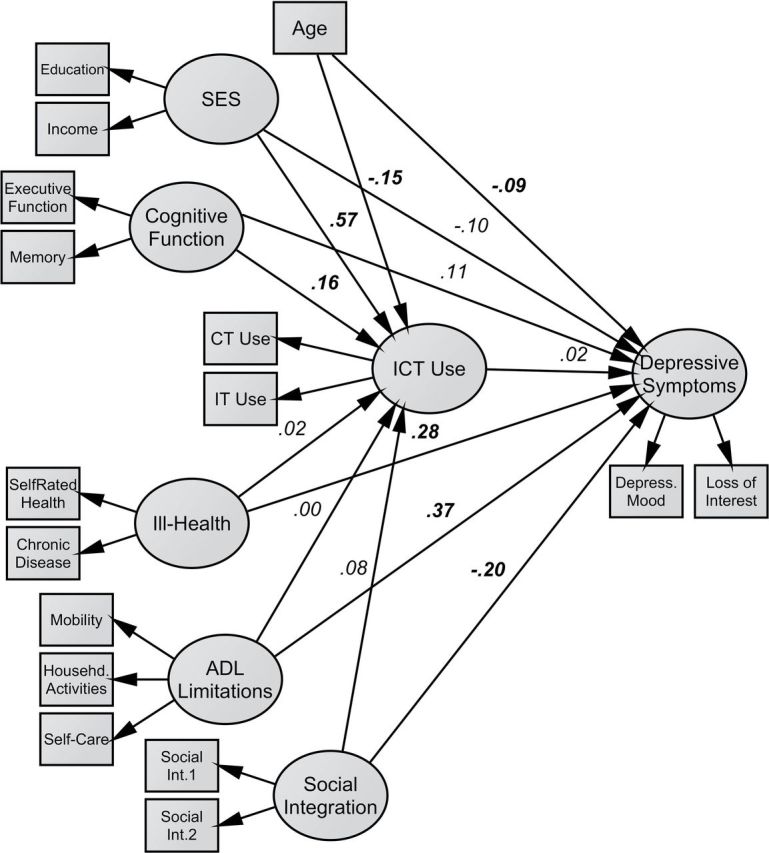
Full structural model predicting information and communications technology use and depressive symptoms (Model 1).
Results
Patterns of ICT Use
Characteristics of the community sample (N = 6,483), as well as scores on key variables, are presented in Table 1. The weighted percentages of both community and full samples that reported various technologies and related uses are presented in Table 2. Approximately 51.2% of the community sample and 47.0% of the full sample reported having e-mailed/texted or used the Internet for another reason within the past month, estimates that are in line with those reported in other recent studies (Tun & Lachman, 2010; Zickuhr & Madden, 2012). To examine differences in level of ICT use across demographic lines, we conducted a four-way ANOVA including age, education, gender, and race/ethnicity as independent variables. For the purpose of this analysis, the education variable was recoded to consist of only four categories (1 = did not complete high school; 2 = high school degree or equivalent; 3 = any postsecondary education including an associate’s degree; 4 = bachelor’s degree or higher). There were significant main effects of age, F(5, 4577) = 5.60, p < .001, and education, F(3, 4577) = 16.90, p < .001. In addition, there was a marginally significant main effect of race/ethnicity, F(2, 4577) = 3.73, p = .02. Consistent with the extant literature, ICT use was greater among younger individuals and those with more education. Bonferroni post hoc tests showed that ICT use decreased with each 5-year increment in age and increased with each additional level of educational attainment and that Whites reported greater use than Hispanics. In addition, there was a significant interaction between age and education, F(15, 4577) = 2.20, p = .005, as well as a marginally significant interaction between gender and education, F(3, 4577) = 3.33, p = .02. Visual inspection of plots indicated that differences in ICT use by educational status were greater in younger age groups and that levels of ICT use in men and women were similar at all but the highest level of education (bachelor’s degree and higher), at which men scored higher than women. Weighted intercorrelations between measures are shown in Table 3. For the purpose of calculating correlations, scores on individual items or derived variables were summed to obtain a total score for ADL limitations, ICT use, depressive symptoms (PHQ-2), and well-being.
Table 1.
Descriptive Statistics (N = 6,483)
| Demographic characteristics (frequency counts) | ||
|---|---|---|
| Unweighted | Weighted | |
| Age | ||
| 65–69 | 20.7% | 30.4% |
| 70–74 | 22.6% | 26.4% |
| 75–79 | 20.6% | 19.4% |
| 80–84 | 19.4% | 13.9% |
| 85–89 | 10.8% | 7.3% |
| 90+ | 5.9% | 2.7% |
| Female gender | 57.4% | 55.9% |
| Race/Ethnicity | ||
| Non-Hispanic White | 69.2% | 81.3% |
| Non-Hispanic Black/African American | 21.6% | 8.0% |
| Hispanic | 5.7% | 6.6% |
| Other | 3.6% | 4.0% |
| Scores on predictor and outcome measuresa | ||
| M | SD | |
| Education (1–9) | 5.34 | 2.22 |
| Household incomeb | 44,552 | 39,406 |
| Executive functioning (0–5) | 3.61 | 1.03 |
| Memory (0–10) | 4.31 | 1.66 |
| Self-rated health (1–5) | 3.33 | 1.10 |
| Chronic disease burden (0–7) | 2.17 | 1.36 |
| Limitations in activities of daily living (0–11) | 1.26 | 2.31 |
| Social integration (0–7) | 3.73 | 1.53 |
| Communications technology use (0–3) | 1.04 | 1.28 |
| Information technology use (0–3) | 1.29 | 1.08 |
| PHQ-2 (1–7) | 1.87 | 1.32 |
| Well-being (0–14) | 12.07 | 2.01 |
Note. aWeighted.
bThe household income variable was standardized.
Table 3.
Intercorrelations
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | — | ||||||||||
| 2. Education | −.14* | — | |||||||||
| 3. Income | −.19* | .49* | — | ||||||||
| 4. Executive Function | −.21* | .25* | .20* | — | |||||||
| 5. Memory | −.35* | .33* | .25* | .31* | — | ||||||
| 6. Self-rated health | −.12* | .32* | .28* | .18* | .25* | — | |||||
| 7. Chronic disease | .10* | −.10* | −.13* | −.05* | −.07* | −.44* | — | ||||
| 8. Activity of daily living limitations | .18* | −.17* | −.20* | −.17* | −.22* | −.45* | .31* | — | |||
| 9. Social integration | −.19* | .34* | .33* | .21* | .29* | .32* | −.11* | −.31* | — | ||
| 10. Information and communications technology use | −.33* | .52* | .43* | .28* | .39* | .31* | −.11* | −.23* | .37* | — | |
| 11. PHQ-2 | .02 | −.20* | −.18* | −.09* | −.14* | −.38* | .23* | .40* | −.25* | −.18* | — |
| 12. Well-being | −.12* | .22* | .19* | .15* | .20* | .35* | −.16* | −.34* | .29* | .25* | −.39* |
Note. *p < .01.
Evaluation of Measurement and Structural Models in Full-sample Analyses
A CFA using ML estimation indicated that the overall measurement model including depressive symptoms represented a good fit to the data, χ2(69) = 393.90, p < .001; CFI = .99, PCFI = .65, RMSEA = .03. To construct the latent well-being variable, an EFA of the set of well-being items using principal axis factoring and a promax rotation was conducted with a random subsample (n = 2,030). A three-factor solution provided the clearest extraction and accounted for approximately 60% of the variance. A CFA of this three-factor model of well-being, conducted with the remainder of the sample (n = 4,033), showed good fit to the data, χ2(1) = 0.83, p = .36; CFI = 1.0, RMSEA = .00, as did the overall measurement model including well-being, χ2(83) = 457.20, p < .001; CFI = .98, PCFI = .68, RMSEA = .04. All factor loadings were significant (p < .001), with standardized regression coefficients exceeding .40.
The overall structural model with depressive symptoms as the outcome variable (Model 1) exhibited good fit to the data, χ2(77) = 565.62, p < .001; CFI = .98, PCFI = .63, RMSEA = .04, as did the model with well-being (Model 2), χ2(92) = 571.30, p < .001; CFI = .97, PCFI = .66, RMSEA = .04. Path coefficients for Model 1 are displayed in Figure 1 and for both models in Table 4. SES was positively associated with ICT use (β = .57), as was cognitive function (β = .14). There was also a trend toward significance (p = .03) in which social integration was positively related to ICT use (β = .08). Conversely, age was negatively related to ICT use (β = −.14). ICT use in turn was not significantly associated with depressive symptoms. Depressive symptoms were positively associated with ADL limitations (β = .37) and ill-health (β = .28) and were negatively associated with social integration (β = −.21) and age (β = −.09). An alternative analysis using ADF estimation produced parameter estimates and standard errors that were not substantially different from ML estimates. Squared multiple correlation (R 2) statistics indicate that Model 1 explained 61.7% of the variance in ICT use and 46.1% of the variance in depressive symptoms. Similar results were obtained in Model 2, which explained 61.2% of the variance in ICT use and 37.4% of the variance in well-being. ICT use was not related to well-being, and its associations with other variables differed only trivially from the previous model although social integration reached significance as a predictor of ICT use (β = .12) in this model. As with depressive symptoms, well-being was predicted by ADL limitations (β = −.20), ill-health (β = −.19), and social integration (β = .38), though it was unrelated to age.
Table 4.
Standardized Regression Coefficients (β) in Full-Sample and Selected Multigroup Analyses
| Effect | Full-sample analyses | Selected multigroup analyses | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1: DepSx | Model 2: W.B. | Model 5: race/ethnicity | Model 6: level of ICT use | |||||
| White | Black | p Valuea | High ICT | Low ICT | p Valuea | |||
| ICT ← Age | −.15** | −.15** | −.15** | −.17** | ns | |||
| ICT ← SES | .57** | .55** | .52** | .77** | .002 | |||
| ICT ← Cog. | .16** | .14** | .19** | −.05 | .014 | |||
| ICT ← I.H. | .02 | .02 | .02 | .03 | ns | |||
| ICT ← ADL | .00 | .01 | −.01 | −.03 | ns | |||
| ICT ← Soc. | .08+ | .12* | .07 | −.01 | ns | |||
| DepSx ← ICT | .02 | .02 | −.05 | ns | ||||
| DepSx ← Age | −.09** | −.11** | −.21** | — | −.05 | −.11** | ns | |
| DepSx ← SES | −.10 | −.07 | .05 | — | −.09 | −.01 | ns | |
| DepSx ← Cog. | .11+ | .05 | −.02 | — | .00 | .14 | ns | |
| DepSx ← I.H. | .28** | .27** | .42** | — | .15** | .38** | <.001 | |
| DepSx ← ADL | .37** | .33** | .23** | — | .47** | .27** | <.001 | |
| DepSx ← Soc. | −.20** | −.20 | −.35 | — | −.10 | −.25** | ns | |
| W.B. ← ICT | −.01 | .00 | .08 | ns | ||||
| W.B. ← Age | .00 | |||||||
| W.B. ← SES | .00 | |||||||
| W.B. ← Cog. | −.04 | |||||||
| W.B. ← I.H. | −.21** | |||||||
| W.B. ← ADL | −.19** | |||||||
| W.B. ← Soc. | .38** | |||||||
Note. Results of Models 3 and 4 are not presented as there were no differences between groups by gender or age, respectively. Cog. = Cognitive function; I.H. = Ill-health; Soc. = Social integration; DepSx = Depressive symptoms; W.B. = Well-being. Dashes indicate that differences in coefficients were not tested for significance; ns = not significant.
aProbability value for critical ratio (z score) of difference between parameters across groups.
*p < .01. **p < .001.+ p < .05.
Tests of Moderation by Demographic Characteristics
Separate tests of moderation by demographic characteristics were conducted by splitting the sample into groups by gender (men, n = 2,744; women, n = 3,699), age (65–74, n = 2,787; 75–89, n = 3,656), and race/ethnicity (White, n = 4,460; Black/African American, n = 1,389). Model parameters for the Hispanic subsample could not be estimated separately due to larger standard errors resulting from the considerably smaller number of respondents. For each set of groups, we performed a nested model comparison, using a chi-square difference test to compare the fit of the equal model, in which the set of path coefficients was constrained equal, to the fit of the free model, in which these parameters were free to vary (Meyers, Gamst, & Guarino, 2006). An alpha level of .01 was retained, particularly given suggestions in the literature that the chi-square difference test is overly sensitive to noninvariance with large sample sizes (Cheung & Rensvold, 2002). In the model comparison across gender (Model 3), the chi-square test was not significant, χ2(13) = 22.55, p = .05, indicating that path coefficients were invariant (equivalent) across men and women. In testing age as a moderator (Model 4), age was removed from the model as an exogenous predictor. The chi-square test was again nonsignificant, χ2(11) = 12.10, p = .36. In the model comparison across racial/ethnic groups (Model 5), the chi-square test was significant, χ2(13) = 34.29, p = .001, suggesting that at least one path coefficient was not equivalent. To identify which coefficient(s) differed, we examined the critical ratios for differences between individual parameters in the free model. As shown in Table 4, SES had a significantly stronger effect on ICT use (p = .002) for Blacks/African Americans (β = .77) than for Whites (β = .52). Conversely, cognitive function was a considerably stronger predictor of use (p =.014) for Whites (β = .19) than for Blacks/African Americans, for whom it was not a significant predictor. We also found that as with depressive symptoms, none of the demographic characteristics moderated the association between well-being and ICT use, which was not significant in any subgroup.
Test of Moderation by Level of ICT Use
Finally, in order to test whether level of ICT use moderates the effects of the various exogenous variables on depressive symptoms (Model 6), we conducted a multigroup analysis comparing individuals who had both gone online and e-mailed/texted within the past month (high ICT users, n = 1,985) with those who had not (nonusers/limited users, n = 4,458). The chi-square test was significant, χ2(6) = 36.63, p < .001, suggesting noninvariance of at least one path coefficient across these groups. Examination of critical ratios for differences between individual parameters revealed that the positive association between ill-health and depressive symptoms was significantly weaker (p < .001) for high ICT users (β = .15) than for non/limited users (β = .38). Conversely, the positive association between ADL limitations and depressive symptoms was stronger (p < .001) for high ICT users (β = .47) than for non/limited users (β = .27).
Discussion
The objective of this study was to extend the empirical evidence concerning the predictors and outcomes of older adults’ use of ICT. We also sought to determine whether demographic characteristics moderate associations of these variables with ICT use and whether ICT use moderates the effects of certain predictor variables on depressive symptoms.
We found that age, SES, cognitive function, and social integration together accounted for more than half of the variance in ICT use. Age was negatively associated with ICT use, replicating a consistent finding in the literature. The effect of age was partly, but not fully, attenuated by controls for SES and cognitive function, which were negatively related to age and positively related to ICT use. These results are consistent with cohort effects involving higher education and income as well as greater exposure to technology among younger cohorts (Cutler, Hendricks, & Guyer, 2003; Fazeli et al., 2013) although decrements in cognitive function may also help explain the age gradient in ICT use. Furthermore, differences in level of ICT use across age cohorts were more pronounced among individuals with higher levels of education (particularly those with at least some postsecondary schooling), indicating that education-related disparities in ICT use have widened over time.
SES exhibited the strongest association with ICT use in this study. Although education and income variables were not tested as separate predictors in the structural models, their bivariate correlations with ICT use were similar in magnitude, suggesting a contribution of each to the prediction of ICT use. Although the cost of access to technology would seem to explain any relationship between income and ICT use, further research is needed to identify mechanisms by which greater educational attainment may lead to greater ICT use in older adults, potentially involving enhanced cognitive function or greater ICT-related knowledge, experience, or interest (Czaja et al., 2006; Ellis & Allaire, 1999; Karavidas et al., 2005). Furthermore, if exposure to ICT through one’ children is a common means of dissemination in older adulthood, the existence of ICT-related socioeconomic disparities in younger cohorts could further contribute to such disparities in older adults’ level of use.
The positive association between cognitive function and ICT use observed in this study adds to a growing body of literature linking these variables. In this study, cognitive function was measured by performance on tests of verbal memory and executive function. These capacities, which have been associated with older adults’ computer use/experience and performance (Fazeli et al., 2013; Ownby, Czaja, Loewenstein, & Rubert, 2008; Tun & Lachman, 2010), may influence the extent of ICT use by affecting the relative degree of ease or difficulty recalling and coordinating various operations. Additional research is needed to identify which cognitive domains are most strongly associated with ICT use and to determine the nature and direction of the underlying causal relationship. Social integration was marginally related to ICT use in this study. The strength of this association may vary depending on the particular social network measure used, perhaps accounting in part for the inconsistent findings in the literature (Carpenter & Buday, 2007; Werner et al., 2011). From a theoretical standpoint, the presence of more extensive social involvement may encourage greater use of e-mail/texting, as well as provide more opportunity for exposure to and guidance in the use of ICT more generally.
In this study, ICT use was not significantly related to ill-health or ADL limitations. Several studies have now reported a nonsignificant association with health (Carpenter & Buday, 2007; Gracia & Herrero, 2009). Results pertaining to ADL limitations are at odds with those of Carpenter and Buday (2007) although that study utilized a dichotomous measure of computer use. ICT use was unrelated to measures of depressive symptoms or well-being in this study. Given the size and demographic diversity of the sample, this result suggests that assertions as to the global benefits of ICT use for older adults’ mental health and well-being may be premature or overstated. This finding is consistent with a recent meta-analysis that found no effect of computer or Internet training on well-being in an older adult population although certain psychosocial outcomes, such as loneliness, may still be related to ICT use (Choi et al., 2012).
In this study, we found that after controlling for age and education, differences in level of ICT use across race/ethnicity and gender were limited. In multigroup analyses, we found no evidence of moderation by age or gender. However, there were noteworthy differences between racial/ethnic groups. Although SES was a robust predictor of ICT use for both Whites and racial/ethnic minorities, it was more strongly related to ICT use in the latter group. It is possible that within the context of occupational and social inequality experienced by Black/African American older adults, access to employment or other institutional settings that involved exposure to ICT was more strongly contingent upon educational attainment and financial means. We also found that cognitive function was more strongly related to ICT use among Whites than among Blacks/African Americans, for whom it was not a significant predictor. The results of this study suggest a need for further investigation of racial/ethnic differences in older adults’ life experiences related to ICT use. They also imply, however, that lower average levels of ICT use among racial/ethnic minorities should not be assumed to be a source of disadvantage with respect to mental health or well-being.
Finally, we investigated whether ICT use interacts with other variables in predicting depressive symptoms and found that level of ICT use (whether or not individuals had both gone online and e-mailed/texted within the past month) moderated the effects of two variables on depressive symptoms. Specifically, ill-health was a considerably weaker predictor of depressive symptoms for high ICT users than for non/limited users. Although speculative, it may be that certain uses of ICT, including going online to seek health information, represent forms of active coping in response to health challenges, perhaps imparting a greater sense of control or shaping more favorable expectancies. In addition, the use of e-mail or texting may provide individuals in poorer health with greater opportunity for social support. Alternatively, high ICT users may simply be more likely to possess active coping styles or an internal health locus of control (Werner et al., 2011). In contrast to the preceding result, we found that ADL limitations were more strongly related to depressive symptoms for high ICT users. These individuals appear to be more emotionally distressed by functional impairments, perhaps due to greater exposure to stigmatizing online media or information, or to the additional physical challenges of ICT use. Alternatively, this effect may be confounded by unknown psychological differences between high ICT users and non/limited users. Further investigation is needed to replicate these results and to explain the moderating role of ICT use.
Limitations
This study has various limitations. First, we excluded individuals who responded via proxy due to poor health, dementia, speech or hearing impediments, or language barriers, as well as individuals residing in nursing homes or other residential facilities. The extent of ICT use and its psychosocial consequences may be different for these segments of the population, an important area for future study. In addition, there are numerous ways in which ICT use may be operationalized. The measure used in this study simultaneously represented both frequency and breadth of use, as well as use for both communication and instrumental/informational purposes, thereby capturing more of the underlying population variability than would a dichotomous measure. Nevertheless, it by no means encompasses all uses of ICT reported by older adults (Carpenter & Buday, 2007; Selwyn et al., 2003). Furthermore, it remains possible that mental health and well-being outcomes are differentially related to specific ICT activities (Bessière, Pressman, Kiesler, & Kraut, 2010).
With respect to other variables, this study included brief screening measures of memory and executive function, as opposed to more extensive cognitive tests. Similarly, it utilized the PHQ-2, a brief depression screener that assesses a limited number of clinical symptoms. While demonstrating adequate construct and criterion validity with older adults (Li et al., 2007), it is not independently diagnostic of depression or indicative of mental health more broadly. The measure of well-being, while supported by factor analytic techniques and containing items similar to those included in validated scales, lacked a clear theoretical structure. In terms of the analytic method, we treated several variables measured on an ordinal scale as continuous although a large sample size should reduce any resulting bias to parameter estimates (Byrne, 2010). Lastly, the cross-sectional design of this study does not permit inferences regarding the causal relationship between variables. For example, although better memory and executive function may encourage greater ICT use among older adults, ICT use may help to preserve or bolster these or other cognitive capacities (Tun & Lachman, 2010). Longitudinal and experimental studies are needed to enable more reliable inferences concerning the direction of these associations.
REFERENCES
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author [Google Scholar]
- Barg F. K., Huss-Ashmore R., Wittink M. N., Murray G. F., Bogner H. R., Gallo J. J. (2006). A mixed-methods approach to understanding loneliness and depression in older adults. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 61, 329–339. 10.1093/geronb/61.6.S329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bessière K., Pressman S., Kiesler S., Kraut R. (2010). Effects of Internet use on health and depression: A longitudinal study. Journal of Medical Internet Research, 12, e6. 10.2196/jmir.1149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Billipp S. (2001). The psychosocial impact of interactive computer use within a vulnerable elderly population: A report on a randomized prospective trial in a home health care setting. Public Health Nursing, 18, 138–145. 10.1046/j.1525-1446.2001.00138.x [DOI] [PubMed] [Google Scholar]
- Browne M., Cudeck R. (1993). Alternative ways of assessing model fit. In Bollen K., Long J. (Eds.), Testing structural equation models (pp. 136–162). Newbury Park, CA: Sage Publications [Google Scholar]
- Byrne B. M. (2010). Structural equation modeling with AMOS: Basic concepts, applications, and programming (2nd ed.). New York, NY: Taylor and Francis Group [Google Scholar]
- Cacioppo J., Hughes M., Waite L., Hawkley L., Thisted R. (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychology and Aging, 21, 140–151. 10.1037/0882-7974.21.1.140 [DOI] [PubMed] [Google Scholar]
- Carpenter B. D., Buday S. (2007). Computer use among older adults in a naturally occurring retirement community. Computers in Human Behavior, 23, 3012–3024. 10.1016/j.chb.2006.08.015 [Google Scholar]
- Chen Y., Persson A. (2002). Internet use among young and older adults: Relation to psychological well-being. Educational Gerontology, 28, 731–744. 10.1080/03601270290099921 [Google Scholar]
- Cheung G. W., Rensvold R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9, 233–255. 10.1207/S15328007SEM0902_5 [Google Scholar]
- Choi M., Kong S., Jung D. (2012). Computer and Internet interventions for loneliness and depression in older adults: A meta-analysis. Healthcare Informatics Research, 18, 191–198. 10.4258/hir.2012.18.3.191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coffman D. L., MacCallum R. C. (2005). Using parcels to convert path analysis models into latent variable models. Multivariate Behavioral Research, 40, 235–259. 10.1207/s15327906mbr4002_4 [DOI] [PubMed] [Google Scholar]
- Cotten S. R., Ford G., Ford S., Hale T. M. (2012). Internet use and depression among older adults. Computers in Human Behavior, 28, 496–499. 10.1016/j.chb.2011.10.021 [Google Scholar]
- Cutler S. J., Hendricks J., Guyer A. (2003). Age differences in home computer availability and use. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 58, 271–280. 10.1093/geronb/58.5.S271 [DOI] [PubMed] [Google Scholar]
- Czaja S. J., Charness N., Fisk A. D., Hertzog C., Nair S. N., Rogers W. A., Sharit J. (2006). Factors predicting the use of technology: Findings from the center for research and education on aging and technology enhancement (CREATE). Psychology and Aging, 21, 333–352. 10.1037/0882-7974.21.2.333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dickinson A., Gregor P. (2006). Computer use has no demonstrated impact on the well-being of older adults. International Journal of Human-Computer Studies, 64, 744–753. 10.1016/j.ijhcs.2006.03.001 [Google Scholar]
- Ellis D., Allaire J. C. (1999). Modeling computer interest in older adults: The role of age, education, computer knowledge, and computer anxiety. Human Factors, 41, 345–55. 10.1518/001872099779610996 [DOI] [PubMed] [Google Scholar]
- Erickson J., Johnson G. M. (2011). Internet use and psychological wellness during late adulthood. Canadian Journal on Aging, 30, 197–209. 10.1017/S0714980811000109 [DOI] [PubMed] [Google Scholar]
- Ertel K. A., Glymour M. M., Berkman L. F. (2008). Effects of social integration on preserving memory function in a nationally representative US elderly population. American Journal of Public Health, 98, 1215–1220. 10.2105/AJPH.2007.113654 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fallows D. (2005). How men and women use the Internet Retrieved from http://www.pewinternet.org/Reports/2005/How-Women-and-Men-Use-the-Internet/01-Summary-of-Findings.aspx
- Fazeli P. L., Ross L. A., Vance D. E., Ball K. (2013). The relationship between computer experience and computerized cognitive test performance among older adults. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 68, 337–346. 10.1093/geronb/gbs071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiori K. L., Antonucci T. C., Cortina K. S. (2006). Social network typologies and mental health among older adults. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 61, 25–32. 10.1093/geronb/61.1.P25 [DOI] [PubMed] [Google Scholar]
- Fokkema T., Knipscheer K. (2007). Escape loneliness by going digital: A quantitative and qualitative evaluation of a Dutch experiment in using ECT to overcome loneliness among older adults. Aging & Mental Health, 11, 496–504. 10.1080/13607860701366129 [DOI] [PubMed] [Google Scholar]
- Fox S. (2004). Older Americans and the Internet. Retrieved from http://www.pewinternet.org/Reports/2004/Older-Americans-and-the-Internet/1-Summary-of-Findings.aspx [Google Scholar]
- Freedman V. A., Kasper J. D., Cornman J. C., Agree E. M., Bandeen-Roche K., Mor V, … Wolf D. A. (2011). Validation of new measures of disability and functioning in the National Health and Aging Trends Study. Journals of Gerontology, Series A: Biological Sciences and Medical Sciences, 66, 1013–1021. 10.1093/gerona/glr087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freese J., Rivas S., Hargittai E. (2006). Cognitive ability and Internet use among older adults. Poetics, 34(4–5), 236–249. 10.1016/j.poetic.2006.05.008 [Google Scholar]
- Gracia E., Herrero J. (2009). Internet use and self-rated health among older people: A national survey. Journal of Medical Internet Research, 11, e49. 10.2196/jmir.1311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hahs-Vaughn D. L., Lomax R. G. (2006). Utilization of sample weights in single-level structural equation modeling. The Journal of Experimental Education, 74, 163–190. 10.3200/JEXE.74.2.161-190 [Google Scholar]
- Hu L., Bentler P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. 10.1080/10705519909540118 [Google Scholar]
- Kaplan D., Ferguson A. J. (1999). On the utilization of sample weights in latent variable models. Structural Equation Modeling, 6, 305–321. 10.1080/10705519909540138 [Google Scholar]
- Karavidas M., Lim N., Katsikas S. (2005). The effects of computers on older adult users. Computers in Human Behavior, 21, 697–711. 10.1016/j.chb.2004.03.012 [Google Scholar]
- Kline R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York, NY: The Guilford Press [Google Scholar]
- Koopman-Boyden P. G., Reid S. L. (2009). Internet/E-mail usage and well-being among 65–84 year olds in New Zealand: Policy implications. Educational Gerontology, 35, 990–1007. 10.1080/03601270902917745 [Google Scholar]
- Kroenke K., Spitzer R. L., Williams J. B. W. (2003). The Patient Health Questionnaire-2: Validity of a two-item depression screener. Medical Care, 41, 1284–1292. 10.1097/01.MLR.0000093487.78664.3C [DOI] [PubMed] [Google Scholar]
- Lachman M. E., Weaver S. L. (1998). The sense of control as a moderator of social class differences in health and well-being. Journal of Personality and Social Psychology, 74, 763–773. 10.1037/0022-3514.74.3.763 [DOI] [PubMed] [Google Scholar]
- Li C., Friedman B., Conwell Y., Fiscella K. (2007). Validity of the Patient Health Questionnaire 2 (PHQ-2) in identifying major depression in older people. Journal of the American Geriatrics Society, 55, 596–602. 10.1111/j.1532-5415.2007.01103.x [DOI] [PubMed] [Google Scholar]
- Little R. J. A., Rubin D. B. (1989). The analysis of social-science data with missing values. Sociological Methods & Research, 18(2–3), 292–326. 10.1177/0049124189018002004 [Google Scholar]
- Livingston G., Parker K., Fox S. (2009). Latinos online, 2006–2008: Narrowing the gap. Retrieved from http://www.pewhispanic.org/2009/12/22/latinos-online-2006-2008-narrowing-the-gap/ [Google Scholar]
- MacCallum R. C., Browne M. W., Sugawara H. M. (1996). Power analysis and determination of sample size for covariance structure modeling. Psychological Methods, 1, 130–149. 10.1037/1082-989X.1.2.130 [Google Scholar]
- McConatha D., McConatha J., Dermigny R. (1994). The use of interactive computer services to enhance the quality-of-life for long-term-care residents. Gerontologist, 34, 553–556. 10.1093/geront/34.4.553 [DOI] [PubMed] [Google Scholar]
- Meyers L. S., Gamst G., Guarino A. (2006). Applied multivariate research: Design and interpretation. Thousand Oaks, CA: Sage Publishers [Google Scholar]
- Montaquila J., Freedman V. A., Edwards B., Kasper J. D. (2012). National Health and Aging Trends Study Round 1 Sample Design and Selection (NHATS Technical Paper No. 1). Retrieved from http://www.nhats.org/scripts/sampleDesign.htm [Google Scholar]
- Montaquila J., Freedman V. A., Kasper J. D. (2012). Round 1 income imputation (NHATS Technical Paper No. 3). Retrieved from http://www.nhats.org/scripts/TechnicalImputation.htm [Google Scholar]
- Montaquila J., Freedman V. A., Spillman B., Kasper J. D. (2012). Development of Round 1 Survey Weights (NHATS Technical Paper No. 2). Retrieved from http://www.nhats.org/scripts/TechnicalWeighting.htm [Google Scholar]
- Mulaik S. A., James L. R., Vanalstine J., Bennett N., Lind S., Stilwell C. D. (1989). Evaluation of goodness-of-fit indexes for structural equation models. Psychological Bulletin, 105, 430–455. 10.1037/0033-2909.105.3.430 [Google Scholar]
- Muthen B., Kaplan D., Hollis M. (1987). On structural equation modeling with data that are not missing completely at random. Psychometrika, 52, 431–462. 10.1007/BF02294365 [Google Scholar]
- Ofstedal M. B., Fisher G. G., Herzog A. R. (2005). Documentation of cognitive functioning measures in the Health and Retirement Study (HRS Documentation Report DR-006). Retrieved from http://hrsonline.isr.umich.edu/sitedocs/userg/dr-006.pdf [Google Scholar]
- Ownby R. L., Czaja S. J., Loewenstein D., Rubert M. (2008). Cognitive abilities that predict success in a computer-based training program. Gerontologist, 48, 170–180. 10.1093/geront/48.2.170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinquart M., Sorensen S. (2000). Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychology and Aging, 15, 187–224. 10.1037//0882-7974.15.2.187 [DOI] [PubMed] [Google Scholar]
- Ryff C. D., Keyes C. L. M. (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69, 719–727. 10.1037//0022-3514.69.4.719 [DOI] [PubMed] [Google Scholar]
- Selwyn N., Gorard S., Furlong J., Madden L. (2003). Older adults’ use of information and communications technology in everyday life. Ageing and Society, 23, 561–582. 10.1017/S0144686X03001302 [Google Scholar]
- Shapira N., Barak A., Gal I. (2007). Promoting older adults’ well-being through Internet training and use. Aging & Mental Health, 11, 477–484. 10.1080/13607860601086546 [DOI] [PubMed] [Google Scholar]
- Shulman K. I. (2000). Clock-drawing: Is it the ideal cognitive screening test? International Journal of Geriatric Psychiatry, 15, 548–561. 10.1002/1099–1166(200006)15:6<548::AID-GPS242>3.3.CO;2-L [DOI] [PubMed] [Google Scholar]
- Slegers K., van Boxtel M. P. J., Jolles J. (2008). Effects of computer training and Internet usage on the well-being and quality of life of older adults: A randomized, controlled study. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 63, 176–184. 10.1093/geronb/63.3.P176 [DOI] [PubMed] [Google Scholar]
- Smith A. (2011). Americans and their cell phones. Retrieved from http://pewinternet.org/Reports/2011/Cell-Phones.aspx [Google Scholar]
- Spooner T., Rainie L. (2000). African-Americans and the Internet. Retrieved from http://www.pewinternet.org/Reports/2000/AfricanAmericans-and-the-Internet/Summary.aspx [Google Scholar]
- Tun P. A., Lachman M. E. (2010). The association between computer use and cognition across adulthood: Use it so you won’t lose it? Psychology and Aging, 25, 560–568. 10.1037/a0019543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wagner N., Hassanein K., Head M. (2010). Computer use by older adults: A multi-disciplinary review. Computers in Human Behavior, 26, 870–882. 10.1016/j.chb.2010.03.029 [Google Scholar]
- Werner J. M., Carlson M., Jordan-Marsh M., Clark F. (2011). Predictors of computer use in community-dwelling, ethnically diverse older adults. Human Factors, 53, 431–447. 10.1177/0018720811420840 [DOI] [PMC free article] [PubMed] [Google Scholar]
- White H., McConnell E., Clipp E., Branch L. G., Sloane R., Pieper C., Box T. L. (2002). A randomized controlled trial of the psychosocial impact of providing Internet training and access to older adults. Aging & Mental Health, 6, 213–221. 10.1080/13607860220142422 [DOI] [PubMed] [Google Scholar]
- Zickuhr K., Madden M. (2012). Older adults and Internet use. Retrieved from http://www.pewinternet.org/Reports/2012/Older-adults-and-internet-use/Summary-of-findings.aspx [Google Scholar]