

Abstract
Excessive gingival display, commonly referred to as ‘gummy smile’ is a major hurdle in overall personality of an individual. Gummy smile, secondary to altered passive eruption and tooth mal-positioning, can be predictably treated with Surgery and orthodontic therapy. In patients with jaw deformities, orthognathic surgery can be performed. However, this requires hospitalization and entails significant discomfort. Lip repositioning is a simple surgical procedure to treat ‘gummy smile’. The procedure restricts the muscle pull of the elevator lip muscles thereby reducing the gingival display while smiling. This procedure is safe and predictable with minimal risk or side effects. This case report describes the successful treatment of excessive gingival display using surgical lip repositioning procedure which can be used as an alternative treatment modality for treatment of excessive gingival display.
Keywords: Excessive gingival display, gummy smile, lip repositioning
INTRODUCTION
The harmony of the smile is determined not only by the shape, the position, and the colour of teeth but also by the gingival tissues. Excessive gingival display (EGD), which is commonly described as ‘gummy smile’ adversely affects smile aesthetics and therefore undesirable. It is one of the several developmental or acquired deformities and conditions that manifest in the periodontium.[1] It is an aesthetic concern that can affect a large portion of the population, with a reported prevalence between 10.5% and 29%.[2,3] In the recent years, EGD has received an increased emphasis in dental literature and various treatment options are now available for correction of gummy smile.
The various causes of gummy smile include vertical maxillary excess, anterior dentoalveolar extrusion, altered passive eruption, short or hyperactive upper lip, or combinations thereof.[4,5]
Treatment of EGD by esthetic crown lengthening with or without osseous resection is well documented.[6,7] Dentoalveolar extrusion can be treated successfully by orthodontic therapy.[8] EGD, due to vertical maxillary excess, can be successfully treated by orthognathic surgery.[9] However, this surgery is associated with significant morbidity and requires hospitalization. Therefore, lip repositioning is recommended as an alternative treatment for EGD.
The objective of lip repositioning is to limit the retraction of elevator smile muscles. Lip repositioning results in shallow vestibule restricting the muscle pull thereby limiting the gingival display during smiling.
CASE REPORT
A 22-year-old female patient undergoing orthodontic treatment, presented with the complaint of gummy smile following retraction of maxillary anterior teeth [Figure 1].
Figure 1.
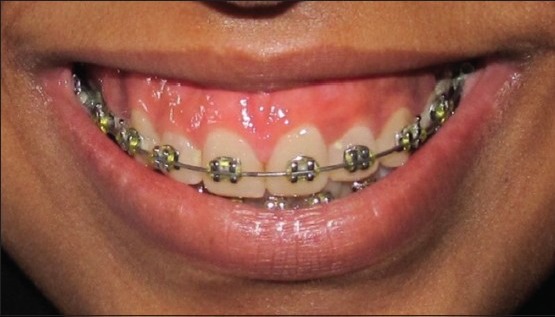
Preoperative smile
The patient's medical history was noncontributory with no contraindication for surgery. Clinical examination revealed moderate amount of maxillary gingival display. With full smile, patient's teeth were visible from maxillary right first molar to maxillary left first molar with 5-6 mm of gingival display. Maxillary anterior teeth had normal crown height and width/length ratio. A diagnosis of moderate vertical maxillary excess was made. Orthognathic surgery as a treatment option was discussed with the patient. However, patient preferred less invasive lip repositioning procedure over orthognathic surgery. Informed consent was obtained prior to the procedure.
Surgical procedure
Adequate local anesthetic (lignocaine 2% with epinephrine 1:100,000) was administered in vestibular mucosa and lip from maxillary right first molar to maxillary left first molar. The surgical site was marked with an indelible pencil. A partial thickness flap was raised from mesial line angle of left maxillary first molar to the mesial line angle of right maxillary first molar at the mucogingival junction [Figure 2]. A second incision 10–12 mm above the first incision was made in the labial mucosa. The two incisions were joined on either side and a strip of partial thickness flap was removed, exposing the underlying connective tissue [Figure 3]. The two incisions were then approximated using continuous interlocking sutures [Figure 4].
Figure 2.
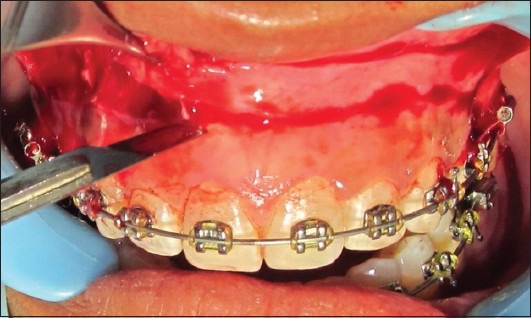
Removal of split thickness flap
Figure 3.

Exposed underlying connective tissue
Figure 4.

Margins approximated by sutures
Patient was prescribed nonsteroidal anti-inflammatory drugs (diclofenac sodium 50 mg three times daily for 3 days) and oral antibiotics (amoxicillin 500 mg three times daily for 5 days). Patient was instructed to apply ice pack post operatively and minimize lip movement for 1 week. Sutures were removed 2 weeks post operatively. Patient reported mild pain and tension while smiling during the first week after surgery.
Sutures were removed 2 weeks postoperatively. Suture line healed in the form of a scar which was covered by labial mucosa and therefore not visible on smiling [Figure 5].
Figure 5.

Scar tissue as seen 6 month postoperatively
RESULT
Gingival display at baseline was 5-6 mm which changed drastically at 3 and 6 months postoperatively [Figure 6]. At 3 month and at 6 months gingival display was 3 mm. There was no difference in gingival display between 3 and 6 months. However, the lip reverted back to its original position with almost complete relapse after 12 months [Figure 7].
Figure 6.

Postoperative smile after 6 months
Figure 7.

Postoperative smile after 1 year
DISCUSSION
This report aimed to document lip repositioning technique to decrease the amount of gingival display in patients with gummy smile. The results showed esthetic satisfaction up to 6 months postoperatively after which lip slowly reverted back towards its original position with almost complete relapse at the end of 1 year.
Studies have shown that minimal gingival display during smile is considered esthetically acceptable.[10,11,12] However, aesthetic perception varies depending on social environment, personal experience and culture.[13,14] Dental professionals are usually more critical than laypersons regarding gingival display.[15,16] The amount of gingival display that is considered attractive varies from 1-3 mm.[17,18]
The results showed that the employed surgical procedure successfully reduced the gingival display with low morbidity. The procedure is safe and has minimum side effects.[19] Reports in the literature have shown minimal post operative bruising, discomfort and swelling. Mucocele formation has been the most severe reported complication.[20,21]
Lip repositioning procedure began as a plastic surgical treatment and ever since variations have been reported.[20] The original technique did not include severing the muscle attachment after flap reflection.[19,22] However, some authors suggested performing myectomies to detach smile muscle attachment to prevent relapse.[23,24,25] Another method to prevent reattachment of smile elevator muscles is the placement of spacer between elevator muscles of lip and anterior nasal spine thereby preventing superior displacement of repositioned lip.[26]
Contraindications for lip repositioning surgery include inadequate width of attached gingiva in maxillary anterior sextent. Insufficient amount of tissue poses difficulty in flap reflection, stabilization and suturing. Patients with severe vertical maxillary excess cases are also not the ideal candidates for lip repositioning and should be treated with orthognathic surgery.[20]
Silva et al. in 2012 reported successful management of excessive gingival display in a study wherein thirteen patients with excessive gingival display were treated with a modified lip repositioning technique. Treatment consisted of the removal of two strips of mucosa, bilaterally to the maxillary labial frenum and coronal repositioning of the new mucosal margin. The baseline gingival display of 5.8 ± 2.1 mm significantly decreased to 1.4 ± 1.0 mm at 3 months and was maintained until 6 months (1.3 ± 1.6 mm). Subjects were satisfied with their smile after surgery and would likely choose to undergo the procedure again (92%).[27]
Similar results were obtained in other case reports by Rosenbaltt,[20] Simon,[21] and Humayun et al.[28] who achieved approximately 4 mm of reduction in gummy smile.
Jacobs et al. in 2013 reported a case series where seven patients were successfully managed with trial, and then definitive, lip repositioning wherein a mean reduction in gingival display of 6.4 ± 1.5 mm was achieved.[29]
Vital et al. in 2013 presented case report of two patients treated with modified lip repositioning technique and obtained significant improvement in the amount of gingival exposure and esthetic satisfaction after a 6 month follow up.[30]
The literature shows only clinical case reports for gummy smile treatment.[30] Several authors have presented case reports of single patients successfully treated with lip repositioning surgery with a follow up period of 6 months.[29]
This case report shows that although the results of lip repositioning surgery appear stable for up to 6 months postoperatively, its utility as a long term treatment option remains questionable. More studies with larger sample size and long term follow-up are necessary to establish the level of scientific evidence of this procedure.
CONCLUSION
Lip repositioning procedure is an effective way of reducing the EGD. However, long-term stability of the results needs to be seen. None the less, this procedure appears to be a promising alternative treatment option for excessive gingival display.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Armitage GC. Development of a classification system for periodontal disease and conditions. Ann Periodontol. 1999;4:1–6. doi: 10.1902/annals.1999.4.1.1. [DOI] [PubMed] [Google Scholar]
- 2.Tjan AH, Miller GD. The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51:24–8. doi: 10.1016/s0022-3913(84)80097-9. [DOI] [PubMed] [Google Scholar]
- 3.Dong JK, Jin TH, Cho HW, Oh SC. The esthetics of the smile: A review of some recent studies. Int Prosthodont. 1999;12:9–19. [PubMed] [Google Scholar]
- 4.Garber DA, Salama MA. The aestheticsmile: Diagnosis and treatment. Periodontol 2000. 1996;11:18–28. doi: 10.1111/j.1600-0757.1996.tb00179.x. [DOI] [PubMed] [Google Scholar]
- 5.Silberberg N, Goldstein M, Smidt A. Excessive gingival display – etiology, diagnosis, and treatment modalities. Quintessence Int. 2009;40:809–18. [PubMed] [Google Scholar]
- 6.Lee EA. Aesthetic crown lengthening: Classification, biologic rationale, and treatment planning considerations. Pract Proced Aesthet Dent. 2004;16:769–78. [PubMed] [Google Scholar]
- 7.Chu SJ, Karabin S, Mistry S. Short tooth syndrome: Diagnosis, etiology and treatment management. J Calif Dent Assoc. 2004;32:143–52. [PubMed] [Google Scholar]
- 8.Kokich VG. Esthetics: The orthodontic periodontic restorative connection. Semin Orthod. 1996;2:21–30. doi: 10.1016/s1073-8746(96)80036-3. [DOI] [PubMed] [Google Scholar]
- 9.Ezquerra F, Berrazueta MJ, Ruiz-Capillas A, Arregui JS. New approach to the gummy smile. Plast Reconstr Surg. 1999;104:1143–50. [PubMed] [Google Scholar]
- 10.Arnett GW, Bergman RT. Facial keys to orthodontic diagnosis and treatment planning. Part I. Am J Orthod Dentofacial Orthop. 1993;103:299–312. doi: 10.1016/0889-5406(93)70010-L. [DOI] [PubMed] [Google Scholar]
- 11.Fowler P. Orthodontics and orthognatic surgery in the combined treatment of an excessive gummy smile. N Z Dent J. 1999;95:53–4. [PubMed] [Google Scholar]
- 12.Zachrisson BU. Esthetic factors involved in anterior tooth display and smile: Vertical dimension. J Clin Orthod. 1998;32:432–45. [Google Scholar]
- 13.Oumeish OY. The cultural and philosophical concepts of cosmetics in beauty and art through the medical history of mankind. Clin Dermatol. 2001;19:375–86. doi: 10.1016/s0738-081x(01)00194-8. [DOI] [PubMed] [Google Scholar]
- 14.Flores-Mir C, Silva E, Barriga MI, Lagravere MO, Major PW. Layperson's perception of smile aesthetics in dental and facial views. J Orthod. 2004;31:204–9. doi: 10.1179/146531204225022416. [DOI] [PubMed] [Google Scholar]
- 15.Roden-Johnson D, Gallerano R, English J. The effects of buccal corridor spaces and arch form on smile esthetics. Am J Orthod Dentofac Orthop. 2005;127:343–50. doi: 10.1016/j.ajodo.2004.02.013. [DOI] [PubMed] [Google Scholar]
- 16.Pinho S, Ciriaco C, Faber J, Lenza MA. Impact of dental asymmetries on theperception of smile esthetics. Am J Orthod Dentofacial Orthop. 2007;132:748–3. doi: 10.1016/j.ajodo.2006.01.039. [DOI] [PubMed] [Google Scholar]
- 17.Geron S, Atalia W. Influence of sex onthe perception of oral and smile esthetics withdifferent gingival display and incisal plane inclination. Angle Orthod. 2005;75:778–84. doi: 10.1043/0003-3219(2005)75[778:IOSOTP]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Kokich VO, Kokich VG, Kiyak HA. Perceptions of dental professionals and laypersons to altered dental esthetics: A symmetric and symmetric situations. Am J Orthod Dentofacial Orthop. 2006;130:141–51. doi: 10.1016/j.ajodo.2006.04.017. [DOI] [PubMed] [Google Scholar]
- 19.Kamer FM. “How do I do it”- Plastic surgery, practical suggestions on facial plastic surgery, smile surgery. Laryngoscope. 1979;89:1528–32. doi: 10.1002/lary.5540890917. [DOI] [PubMed] [Google Scholar]
- 20.Rosenblatt A, Simon Z. Lip repositioningfor reduction of excessive gingival display: A clinical report. Int J Periodontics Restorative Dent. 2006;26:433–7. [PubMed] [Google Scholar]
- 21.Simon Z, Rosemblatt A, Dorfmann W. Eliminating a gummy smile with surgicallip repositioning. J Cosmetic Dent. 2007;23:100–8. [Google Scholar]
- 22.Rubinstein AM, Kostianovsky AS. Cirugiaestetica de la malformacion de la sonrisa. Pren Med Argent. 1973;60:952. [Google Scholar]
- 23.Cachay-Velasquez H. Rhinoplasty and facial expression. Ann Plast Surg. 1992;28:427–33. doi: 10.1097/00000637-199205000-00006. [DOI] [PubMed] [Google Scholar]
- 24.Miskinyar SA. A new method for correction of gummy smile. Plast Reconstr Surg. 1983;72:397–400. doi: 10.1097/00006534-198309000-00027. [DOI] [PubMed] [Google Scholar]
- 25.Litton C, Fournier P. Simple surgical correction of gummy smile. Plast Reconstr Surg. 1979;63:372–3. doi: 10.1097/00006534-197903000-00014. [DOI] [PubMed] [Google Scholar]
- 26.Ellenbogen R, Swara N. The improvement of gummy smile using the implant spacer technique. Ann Plast Surg. 1984;12:16–24. doi: 10.1097/00000637-198401000-00004. [DOI] [PubMed] [Google Scholar]
- 27.Silva CO, Ribeiro-Junior NV, Campos TV, Rodrigues JG, Tatakis DN. Excessive gingival display: Treatment by a modified lip repositioning technique. J Clin Periodontol. 2012;40:260–5. doi: 10.1111/jcpe.12046. [DOI] [PubMed] [Google Scholar]
- 28.Humayun N, Kolhatkar S, Souiyas J, Bhola M. Mucosal coronally positioned flap for the management of excessive gingival display in the presence of hyper mobility of the upper lip and vertical maxillary excess: A case report. J Periodontol. 2010;81:1858–63. doi: 10.1902/jop.2010.100292. [DOI] [PubMed] [Google Scholar]
- 29.Jacobs PJ, Jacobs BP. Lip repositioning with reversible trial for the management of excessive gingival display. Int J Periodontics Restorative Dent. 2013;33:169–75. doi: 10.11607/prd.1483. [DOI] [PubMed] [Google Scholar]
- 30.Ribeiro-Júnior NV, Campos TV, Rodrigues JG, Martins TM, Silva CO. Treatment of excessive gingival display using a modified lip repositioning technique. Int J Periodontics Restorative Dent. 2013;33:309–14. doi: 10.11607/prd.1325. [DOI] [PubMed] [Google Scholar]