

Abstract
Bell's palsy is hypothesized to result from virally mediated neural edema. Ischemia occurs as the nerve swells in its bony canal, blocking neural blood supply. Because viral infection is relatively common and Bell's palsy relatively uncommon, it is reasonable to hypothesize that there are anatomic differences in facial canal (FC) that predispose the development of paralysis. Measurements of facial nerve (FN) and FC as it follows its tortuous course through the temporal bone are difficult without a 3D view. In this study, 3D reconstruction was used to compare temporal bones of patients with and without history of Bell's palsy.
Methods
Twenty-two temporal bones (HTBs) were included in the study, 12 HTBs from patients with history of Bell's palsy and 10 healthy controls. Three-dimensional models were generated from HTB histopathologic slides with reconstruction software (Amira), diameters of the FC and FN were measured at the midpoint of each segment.
Results
The mean diameter of the FC and FN was significantly smaller in the tympanic and mastoid segments (p = 0.01) in the BP group than in the controls. The FN to FC diameter ratio (FN/FC) was significantly bigger in the mastoid segment of BP group, when compared with the controls. When comparing the BP and control groups, the narrowest part of FC was the labyrinthine segment in control group and the tympanic segment in the BP.
Conclusion
This study suggests an anatomic difference in the diameter of FC in the tympanic and mastoid segments but not in the labyrinthine segment in patients with Bell's palsy.
Keywords: Anatomy, Bells palsy, Facial nerve, Facial palsy, Histopathology, Three-dimensional, Temporal bone
Idiopathic acute facial paralysis, known as Bell's palsy, is hypothesized to occur when the inflammatory response to herpes simplex virus type 1 (HSV-1) infection induces edema within the facial nerve(1). As the facial nerve swells within the confines of the noncompliant bony facial canal, endoneural pressure increases and neural vasculature is compressed, leading to ischemia and axonal degeneration (2). Because HSV-1 viral infection is relatively common and Bell's palsy relatively is uncommon, it is reasonable to question whether there may be anatomic differences in the relative diameters of segments of the facial nerve and/or facial canal that explain why some patients develop paralysis and others do not.
The facial nerve's tortuous course through the temporal bone creates significant measurement challenges. Although the 2-dimensional anatomy of the facial canal in temporal bones of normal subjects has been well characterized (3–5), measurements are limited to the plane of sectioning that may be oblique rather than orthogonal to a given segment of the nerve. Computed tomography (CT) allows for measurement of the bony canal in the axial and coronal planes, but, unlike histopathologic sections, it does not permit separate measurement of the soft tissue of the nerve itself. In this study, 3-dimensional (3D) reconstructions of histopathologic sections of human temporal bones were created to compare both the facial nerve and facial canal diameters between patients with and without a history of Bell's palsy to determine if there may be an anatomic predisposition for this disease.
Materials and Methods
The specimens used for this study belong to the temporal bone collections of the Otopathology Laboratory of the University of Minnesota and the Massachusetts Eye and Ear Infirmary (MEEI). The human temporal bones (HTBs) were removed, decalcified, embedded in celloidin, sectioned at 20 μm, and every tenth section was stained with hematoxylin and eosin and mounted on glass slides. The slides were examined under a light microscope, and the ones with processing artifacts were excluded.
Inclusion and exclusion criteria were designed to identify all cases of idiopathic facial palsy (Bell's palsy) in the temporal bone collections. The inclusion criterion was the documented history of facial paralysis during the patient's lifetime. There were 78 HTBs meeting this inclusion criterion. The exclusion criteria were as follows: 1) central facial paralysis; 2) otologic surgery; and 3) facial palsy due to known causes, such as tumor, metastasis, iatrogenic injury, and polyneuropathies. There were 12 HTBs from 6 patients remaining after application of the exclusion criteria. Of the 6 patients, 5 had unilateral facial palsy, and 1 experienced sequential bilateral facial paralysis with an interval of 1 year in between the first and second sides. The ages ranged from 59 to 87 years, and there were 4 women. The group was divided into 2 subgroups: Bell's palsy side (BP), 7 temporal bones affected by the disease; and contralateral side (CLS), 5 temporal bones, not affected by the disease, from patients with unilateral facial palsy.
A control group was selected from the University of Minnesota collection. Control HTBs were from patients with no history of alterations of facial nerve function, otologic disease, or otologic surgeries. The control group consisted of 10 temporal bones from 10 patients who had the same age distribution as the group with facial paralysis (age range, 59–94 yr). One side from each patient was used as a control, randomly sampling 6 left and 4 right ears.
The histopathologic slides, containing every tenth section of the HTBs (200-μm interval), were scanned with a high-resolution slide scanner (PathScan Enabler IV, Meyer Instruments, Houston, TX, USA). The images were launched to the three-dimensional (3D) reconstruction software (AMIRA), aligned, and the facial nerve (FN) and facial canal (FC) were outlined and labeled as different materials (Fig. 1). For both FN and FC, the labeling started at the beginning of the Fallopian canal, covering the labyrinthine, tympanic, and mastoid portions. After the segmentation the 3D model was generated (Fig. 2A).
Figure 1.
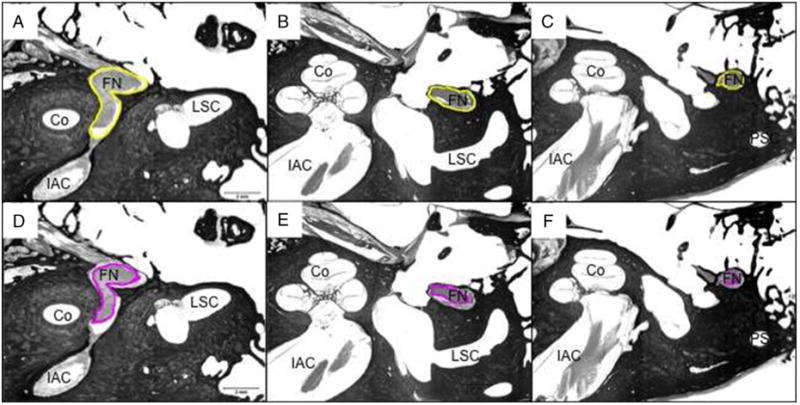
Segmentation of the facial canal (yellow) and facial nerve (pink) on the labyrinthine, tympanic, and mastoid segments. A and D, Labyrinthine segment and first genu. B and E, Tympanic segment. C and F, Mastoid segment. Co indicates cochlea; FN, facial nerve; IAC, internal auditory canal; LSC, lateral semicircular canal; PSC, posterior semicircular canal.
Figure 2.
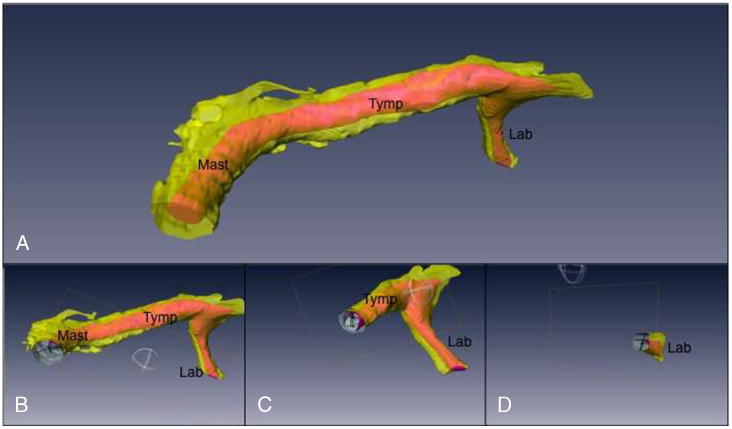
A, Three-dimensional model of the facial nerve (pink) and facial canal (yellow). B, Clipping plane on the mastoid segment, with the exclusion of the distal portion, for better visualization of the diameter measurement lines of the facial nerve and facial canal. C, Clipping plane on the tympanic segment. D, Clipping plane on the labyrinthine segment.
A clipping plane, perpendicular to each segment of the facial nerve, was created and the diameter of the FN and FC was measured at the midpoint (Fig. 2, B–D). For purposes of our measurements, the segments of facial nerve were defined as follows: 1) labyrinthine: from the fundus of the internal auditory canal to the beginning of the curve of the first genu; 2) tympanic: from the end of the curve of the first genu to the beginning of the curve of the second genu; and 3) mastoid: from the end of the second genu to the most inferior HTB section available. The most inferior slide available for each HTB contains the intratemporal facial nerve in proximity to the stylomastoid foramen, but the exact location of the stylomastoid foramen cannot be determined with certainty. The number of sections comprising the mastoid segment was similar between specimens. The midpoint was defined after the measurement of the length of each segment and was used to standardize the point of measurement in the curvilinear canal. The ratio between the diameters of the midpoint of the FC and FN in each segment was calculated by dividing the value, in μm, of the FN by the FC.
Comparisons of the mean diameters of the groups for each segment and the FC/FN ratio were made: 1) between the affected and nonaffected sides (BP and CLS) among patients with unilateral Bell's palsy, 2) between the controls and nonaffected side of patients with unilateral Bell's palsy (control and CLS groups), and 3) between the affected sides in all Bell's palsy patients (BP) and the controls.
For the statistical analysis, STATA version 11.2 (College Station, TX) was used. Because of the small sample size, a nonparametric test, Kruskall-Wallis, was used to compare the group means.
Results
Twenty-two temporal bones met criteria for inclusion in the study. Twelve were from 6 patients with history of Bell's palsy, divided into 2 subgroups: 1) affected temporal bones (BP, n = 7); and 2) unaffected contralateral sides (CLS, n = 5). The control group consisted of 10 temporal bones. The mean age was 70 (±10) years for the control group, and 78 (±9) for the Bell's palsy group (p > 0.05).
Facial Nerve and Facial Canal Results
The results of the FN and FC diameter are shown in Table 1.
Table 1. Group mean diameters of facial canal and facial nerve in each segment, in micrometersa.
| Bell's palsy | |||||
|---|---|---|---|---|---|
|
|
|||||
| Segment | Controls (n = 10) | BP (n = 7) | CLS (n = 5) | ||
| FC LAB | 1836.78 (±546) | 1673.27 (±663) | 1582.57 (±502) | ||
| FN LAB | 1217.05 (±367) | 1340.62 (±633) | 1131.28 (±393) | ||
| FC TYMP | 2428.72 (±393) | 1520.13 (±743) | p = 0.01 | 1368.88 (±809) | p = 0.04 |
| FN TYMP | 1689.62 (±333) | 1193.63 (±616) | p = 0.01 | 1093.18 (±573) | |
| FC MAST | 3397.54 (±457) | 1768.39 (±866) | p = 0.01 | 1986.78 (±821) | p = 0.02 |
| FN MAST | 1975.93 (±263) | 1201.57 (±626) | p = 0.01 | 1332.91 (±649) | |
FC indicates facial canal; FN, facial nerve; BP, bell's palsy side; CLS, contralateral unaffected side; LAB, labyrinthine segment; MAST, mastoid segment; TYMP, tympanic segment.
Plus-minus values are means ± SD.
Facial Canal Results
In the control group, the diameter of the midpoint of the facial canal increased along its course from the labyrinthine segment to the stylomastoid foramen. In the Bell's palsy group, the canal was narrower in the tympanic segment than the labyrinthine, and widest in the mastoid.
In the comparison to the control group, we found that the mean midpoint diameter of the facial canal is smaller in patients who had Bell's palsy (both BP and CLS groups), in all 3 segments, but is significantly different only in the tympanic and mastoid portions. There was no significant difference between the facial canal diameters between the 2 sides of patients with unilateral Bell's palsy (BP versus CLS).
Facial Nerve Results
The width of the facial nerve in the control group grew as it coursed distally following the observed pattern of the facial canal diameter. In both ears of patients affected with Bell's palsy, it was narrowest in the tympanic segment (BP and CLS).
As with the facial canal, although the facial nerve in both affected and unaffected sides of patients who had Bell's palsy was narrower in every segment, than in the control group, the difference was significant only in the tympanic and mastoid segments of the BP group, when compared with the control group. No significant differences were found between the unaffected CLS and control group or within the Bell's palsy subgroups (BP versus CLS).
Comparison of Facial Nerve to Facial Canal Ratios
The FN/FC ratios and comparisons for each segment are presented in Table 2. Given the variation observed within groups in absolute diameter measurements, the ratio of FN/FC diameter was calculated to provide a normalized measurement between groups. A larger ratio indicates that the facial nerve is occupying a greater proportion of the total area of the facial canal in a given segment of measurement, and thus, there is less space available for nerve edema. The FN/FC ratio in all segments was larger among the Bell's palsy temporal bones than the controls, but there was a statistically significant difference between BP and controls only in the mastoid segment and between CLS and controls only in the tympanic segment. There was no significant difference in the FN/FC ratio between the Bell's palsy subgroups (BP and CLS).
Table 2. Ratio between the diameters of the facial nerve and facial canal at the labyrinthine, tympanic and mastoid segmentsa.
| Control | Bell's palsy | ||||
|---|---|---|---|---|---|
|
|
|
||||
| Segment | (n = 10) | BP (n = 7) | CLS (n = 5) | ||
| FN/FC LAB | 0.68 (±0.15) | 0.79 (±0.05) | 0.71 (±0.03) | ||
| FN/FC TYMP | 0.70 (±0.10) | 0.79 (±0.09) | 0.82 (±0.05) | P = 0.02 | |
| FN/FC MAST | 0.59 (±0.08) | 0.68 (±0.07) | p = 0.04 | 0.66 (±0.07) | |
Plus-minus values are means ± SD.
Discussion
Inflammation of the facial nerve evidenced by lymphocytic infiltrates and edema has been established as a pathogenic mechanism of Bell's palsy(6). The edema leads to the nerve entrapment and consequent ischemia because of the blockage of the vasa nervorum. Despite the known pathogenesis, the cause of inflammation, segmental location of entrapment, and management of the disease remains controversial.
The search for anatomic differences in facial canal dimensions among Bell's palsy patients has been difficult because of the curvilinear course that the nerve takes through the temporal bone. Using temporal bone histopathologic slide sections, it is possible to follow the complex path of the facial nerve between the surrounding structures. However, as it curves along the way, it is impossible to consistently assess the dimensions of each segment of the facial nerve and facial canal with a purely 2D view because the sectioning plane inevitably crosses the nerve obliquely. Therefore, to study the anatomy of the facial nerve and the relationship of the nerve and the bony canal, it is imperative to have a 3D view. The microtomography resolution has been improved significantly; however, previous studies in human temporal bones did not show good resolution to carry out any descriptive study to evaluate any soft tissue structure in human temporal bones. Hence, several studies have been performed to find out the best way to do a 3-dimensional reconstruction of the temporal bone, using histologic sections of normal patients (7–9). In this study, we applied the same methods described by Wang et al. (7,8) to assess the facial nerve and facial canal diameters in the labyrinthine, tympanic, and mastoid segments in temporal bones of both normal and Bell's palsy's patients.
Our findings among the control subjects are similar to previous characterizations of normal human temporal bones. As in our study, Fisch (10), Saito et al. (11), and Nakashima et al. (3) have found that the labyrinthine segment was the narrowest portion of the facial canal, followed by the tym-panic segment. However, among the control group of our study, the ratio between the facial nerve and facial canal diameters did not differ between segments of the nerve, whereas Saito et al. and Nakashima et al. found that the ratio between facial nerve and facial canal in healthy subjects was significantly smaller in the mastoid portion compared to the other segments.
We found no significant difference in the diameter of the facial nerve or canal between the affected and unaffected sides in the subjects with unilateral Bell's palsy, suggesting that there is no anatomical predisposition favoring the development of compressive edema on one side versus the other. This finding differs from the one previously published study that compares affected and unaffected ears in Bell's palsy patients. Kefalidis et al. (12) measured the bony meatal foramen and the middle part of the labyrinthine segment in CT scans of 25 patients with a history of Bell's palsy The bony measurements at both sites were significantly smaller in the affected side.
Unlike previous studies, we also compared measurements in Bell's palsy patients to a control group. We observed that the mean diameter of the bony facial canal in the tympanic and mastoid segments on both sides (CLS and BP) of the Bell's palsy group was significantly smaller than the control group, and there was no significant difference between them in the labyrinthine segment. Overall, given that the absolute mean values of the tympanic and mastoid segment canal diameters were significantly narrower in Bell's palsy cases versus controls, but the absolute differences were relatively small; we propose that anatomic differences are unlikely to be the main predisposing factor in the development of Bell's palsy but may contribute to the risk.
We also observed that the ratio between the facial nerve and facial canal (FN/FC) was different between Bell's palsy and the control specimens only in the mastoid segment, suggesting that there would be more room for neural edema before the onset of ischemia in the mastoid segment in the controls versus affected patients. These findings, in conjunction with the observation of canal diameter differences between the groups in the tympanic and mastoid segments alone (and not labyrinthine) could corroborate the clinical improvement of patients with Bell's palsy that undergo the transmastoid surgery for facial nerve decompression (13–15).
The present study has several limitations related to the use of postmortem specimens. We identified every known case of facial paralysis catalogued in the Otopathology Research Collaboration Network (NIDCD, USA), which represents the largest active collection of human temporal bones. Although this is the largest series of Bell's palsy human temporal bone cases reported, given the low rate of donation of facial paralysis specimens, the sample size remains small.
Conclusion
This study demonstrated an anatomic difference in the diameter of the facial canal in the tympanic and mastoid segments but not in the labyrinthine in patients with Bell's palsy compared with the controls, which can be implicated in the pathophysiology of the disease and in the surgical approach.
Acknowledgments
This study was supported by the NIDCD 3U24 DC011968-01, R01 DC006452, 5M Lions International, the International Hearing Foundation, the Starkey Foundation, and CNPq - Brazil. The authors thank Ms. Monika Schachern for technical assistance.
Footnotes
The authors disclose no conflicts of interest.
References
- 1.Murakami S, Mizobuchi M, Nakashiro Y, et al. Bell palsy and herpes simplex virus: identification of viral DNA in endoneurial fluid and muscle. Ann Intern Med. 1996;124:27–30. doi: 10.7326/0003-4819-124-1_part_1-199601010-00005. [DOI] [PubMed] [Google Scholar]
- 2.Powell HC, Myers RR, Costello ML, et al. Endoneurial fluid pressure in Wallerian degeneration. Ann Neurol. 1979;5:550–7. doi: 10.1002/ana.410050610. [DOI] [PubMed] [Google Scholar]
- 3.Nakashima S, Sando I, Takahashi H, et al. Computer-aided 3-d reconstruction and measurement of the facial canal and facial-nerve .1. Cross-sectional area and diameter—preliminary-report. Laryngo-scope. 1993;103:1150–6. doi: 10.1288/00005537-199310000-00013. [DOI] [PubMed] [Google Scholar]
- 4.Fujita S, Nakashima S, Sando I, et al. Postnatal developmental-changes in facial-nerve morphology—computer-aided 3-D reconstruction and measurement. Eur Arch Otorhinolaryngol. 1994;251:434–8. doi: 10.1007/BF00181971. [DOI] [PubMed] [Google Scholar]
- 5.Tuccar E, Tekdemir I, Aslan A, et al. Radiological anatomy of the intratemporal course of facial nerve. Clin Anat. 2000;13:83–7. doi: 10.1002/(SICI)1098-2353(2000)13:2<83::AID-CA2>3.0.CO;2-Y. [DOI] [PubMed] [Google Scholar]
- 6.Liston SL, Kleid MS. Histopathology of Bell's palsy. Laryngoscope. 1989;99:23–6. doi: 10.1288/00005537-198901000-00006. [DOI] [PubMed] [Google Scholar]
- 7.Wang H, Northrop C, Burgess B, et al. Three-dimensional virtual model of the human temporal bone: a stand-alone, downloadable teaching tool. Otol Neurotol. 2006;27:452–7. doi: 10.1097/01.mao.0000188353.97795.c5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang H, Merchant SN, Sorensen MS. A downloadable three-dimensional virtual model of the visible ear. ORL J Otorhinolaryngol Relat Spec. 2007;69:63–7. doi: 10.1159/000097369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Green JD, Marion MS, Erickson BJ, et al. Three-dimensional reconstruction of the temporal bone. Laryngoscope. 1990;100:1–4. doi: 10.1288/00005537-199001000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Fisch U. Surgery for Bell's palsy. Arch Otolaryngol. 1981;107:1–11. doi: 10.1001/archotol.1981.00790370003001. [DOI] [PubMed] [Google Scholar]
- 11.Saito H, Takeda T, Kishimoto S. Facial nerve to facial canal cross-sectional area ratio in children. Laryngoscope. 1992;102:1172–6. doi: 10.1288/00005537-199210000-00013. [DOI] [PubMed] [Google Scholar]
- 12.Kefalidis G, Riga M, Argyropoulou P, et al. Is the width of the labyrinthine portion of the fallopian tube implicated in the pathophysiology of Bell's palsy? A prospective clinical study using computed tomography. Laryngoscope. 2010;120:1203–7. doi: 10.1002/lary.20896. [DOI] [PubMed] [Google Scholar]
- 13.Yanagihara N, Gyo K, Yumoto E, et al. Transmastoid decompression of the facial nerve in Bell's palsy. Arch Otolaryngol. 1979;105:530–4. doi: 10.1001/archotol.1979.00790210028006. [DOI] [PubMed] [Google Scholar]
- 14.Hagino K, Tsunoda A, Tsunoda R, et al. Measurement of the facial nerve caliber in facial palsy: implications for facial nerve decompression. Otol Neurotol. 2011;32:686–9. doi: 10.1097/MAO.0b013e318210b8e2. [DOI] [PubMed] [Google Scholar]
- 15.Bodénez C, Bernat I, Willer JC, et al. Facial nerve decompression for idiopathic Bell's palsy: report of 13 cases and literature review. J Laryngol Otol. 2010;124:272–8. doi: 10.1017/S0022215109991265. [DOI] [PubMed] [Google Scholar]