

Abstract
Background:
Since there is no disease-specific instrument for measuring quality-of-life (QOL) in Ostomy patients in Persian language.
Aim:
This study was designed to translate and evaluate the validity and reliability of City of Hope-quality of life-Ostomy questionnaire (COH-QOL-Ostomy questionnaire).
Subjects and Methods:
This study was designed as cross-sectional study. Reliability of the subscales and the summary scores were demonstrated by intra-class correlation coefficients. Pearson's correlations of an item with its own scale and other scales were calculated to evaluated convergent and discriminant validity. Clinical validity was also evaluated by known-group comparisons.
Results:
Cronbach's alpha coefficient for all subscales was about 0.70 or higher. Results of interscale correlation were satisfactory and each subscale only measured a single and specified trait. All subscales met the standards of convergent and discriminant validity. Known group comparison analysis showed significant differences in social and spiritual well-being.
Conclusion:
The findings confirmed the reliability and validity of Persian version of COH-QOL-Ostomy questionnaire. The instrument was also well received by the Iranian patients. It can be considered as a valuable instrument to assess the different aspects of health related quality-of-life in Ostomy patients and used in clinical research in the future.
Keywords: City of Hope-quality of life questionnaire-Ostomy questionnaire, Ostomy, Quality-of-life, Reliability, Validity
Introduction
Ostomy is a surgical procedure to treat several gastrointestinal diseases, including trauma, colon and rectum cancer, Crohn's disease, bowel obstruction, congenital malformations, and complications of diverticulitis.[1,2] The ostomas may be temporary and can be removed at a later date.[1]
Ostomy is known to impact negatively on a patient's physical activity, psychological performance and social function. Patients with Ostomy suffer from rectal discharge, inability to control gas, difficulties and adjustments of returning to work, decreased sexual activity, and difficulties in travel and leisure activities.[3] They are involved with consequences of this therapeutic method for a long time.[3,4] These problems will reduce quality-of-life (QOL) in Ostomy patients. Thus, assessment of QOL of stoma patients is necessary and can be useful for decisions made in order to control disease, complications, treatment and improve QOL.[1,4,5]
Different reasons for assessing QOL have led to the development and use of different generic and disease-specific instruments.[6] Several instruments have been developed to measure health related quality-of-life (HRQOL) among Ostomy patients. They include quality from the patient's perspective, stoma care QOL index, City of Hope-quality of life-Ostomy questionnaire (COH-QOL-Ostomy questionnaire), Ostomy adjustment scale, Ostomy adjustment inventory-23, coping strategies inventory, QOL index, survey of pre-operative factors of Ostomy adjustment and stoma-QOL.[7] However, the instruments used in most studies have not been validated specifically for stoma patients.[8,9,10,11,12]
One of disease-specific tools is COH-QOL-Ostomy questionnaire. This questionnaire has been derived from a research on QOL conducted in 1983 by the investigators in Nursing Research at the COH National Medical Center, Duarte, CA and revised and validated by Grant et al., in 2004.[4]
Until now, there has not been a suitable tool for measuring QOL in Ostomy patients in Iran. Due to the increased prevalence of colorectal cancer and other conditions leading to ostoma construction in Iran,[13,14,15] standardization of the instrument for evaluating the QOL in these patients seems necessary. The aim of the present study is to translate and evaluate the reliability and validity of the COH-QOL-Ostomy questionnaire when applied to an Iranian sample of patients with Ostomy.
Subjects and Methods
Patients
This survey was a cross-sectional study conducted from March to October 2011 on a random sample of 103 stoma patients who were referred to the Iranian Ostomy Society. Any patient, with adequate physical and mental ability, who had an Ostomy in place for at least 3 months, was eligible to enter the study.
The exclusion criteria were the presence of a psychologic disorder and chronic diseases affecting the QOL such as diabetes mellitus, heart and respiratory diseases, cirrhosis and physical disability. The individuals were informed that participation in the study was not compulsory. Informed consent for enrolment was obtained and patient's anonymity was preserved. The research protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences.
Questionnaire
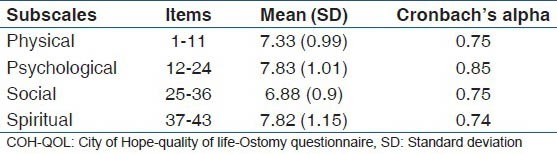
The COH-QOL-Ostomy questionnaire is multidimensional and made up of 43 items, which are categorized into four subscales including physical (Item: 1-11), psychological (Item: 12-24), social (Item: 25-36) and spiritual (Item: 37-43) well-being. Each question is answered with a Likert graded response in the range of 0-10, in which zero reflects the worst outcome and 10 the best. Subscale scores are calculated by adding all the scores of each subscale and dividing their sum by the number of items in that subscale. A total QOL score is calculated by adding the scores on all 10-point items and dividing by the total number of items.[3,4,16,17]
The standard “forward-backward” procedure was applied to translate the questionnaire from English into Persian. First, questionnaire was translated by one Coloproctologist. Then, an official bilingual translator did the back translation into English. Then the back-translation was compared with the original questionnaire with a reasonable match. The final version was approved by the COH National Medical Center. In the next step, a pilot testing was performed for determining of conceptual and perceptual problems of Persian version of the questionnaire. We asked 10 patients about difficulty, confusing, difficult word and upsetting of each item of questionnaire.
Standardization procedures
To test the reliability, the internal consistency of the questionnaire was measured using Cronbach's alpha coefficient. Cronbach's alpha coefficient above 0.7 is considered as a desirable reliability estimate.[6]
The face validity indicates the ability of an instrument to cover all relevant aspects of the phenomena of interest based on medical experts’ opinions.[18] In this study, the face validity was examined by four physicians (two Gastroenterologists and two Psychologists).
Construct validity is composed of two components, convergent validity and discriminant validity. Convergent validity refers to a moderately high correlation between an item and its own subscale. Correlation coefficient of 0.4 or higher is considered as evidence of satisfactory convergent validity.[6,19] Discriminant validity indicates a low correlation between an item and any of the other subscales. Each items should be correlated with own subscales significantly equal or higher than two standard errors than correlations with other subscales. Since the standard error value is heavily influenced by sample size and given the relatively small sample size in the present study, one standard error was used as a criterion for assessment of discriminant validity.[20] Pearson's correlation coefficient was estimated in order to evaluate the convergent and discriminant validity.
Interscale correlations indicate that each subscale only measures a single trait. Correlation coefficients between different subscales should be lower than the internal consistency estimates of each subscale separately.
Clinical validity has been estimated by known-groups comparison. In order to evaluate the extent to which the COH-QOL-Ostomy questionnaire had been able to discriminate between sub-groups of patients with different clinical status, the underlying cause of the disease leading to Ostomy was taken into consideration as a variable. For analyzing the comparison made between known groups, t-test was used. All tests were two-sided and P < 0.05 were considered as statistically significant. Calculations were performed using SPSS v. 13 software (Chicago, IL, USA).
Results
In total, 103 patients were included in the study. The mean (SD) age was 53.5 (12.28) (range: 21-75 years). 56.3% (58/103) of patients were male.
Most patients (67%, 69/200) had a colostomy, 22 patients (21%) had an ileostomy, 9% had a urostomy (9/102), 2% had both colostomy (2/102) and urostomy and 1 patient (1%) had both colostomy and ileostomy. Cancer had been the most common condition leading to Ostomy surgery (n = 79, 77%). Other diseases were inflammatory bowel disease (n = 11, 10.5%) and other conditions including polyp, trauma, peritonitis, obstruction and fistula (n = 13, 12.5%).
In pilot testing, all patients stated that they have not had any difficulty in understanding the questions. Rate of missing data was less than 5%. Cronbach's alpha coefficient for all subscales was about 0.70 or higher, indicating satisfactory internal consistency. The physical well-being subscale had the lowest reliability (0.74). Reliability outcomes are shown in Table 1.
Table 1.
Cronbach's alpha for COH-QOL-Ostomy questionnaire subscales
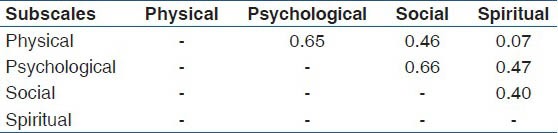
All interscale correlations were in the expected direction. The correlation estimate between the subscales was lower than the internal consistency of each of them. It means that each subscale of COH-QOL-Ostomy questionnaire had an ability to measure only a single concept [Table 2].
Table 2.
Interscale correlation coefficients
The face validity of the Persian version of COH-QOL-Ostomy questionnaire was approved by the experts. According to Multitrait scaling analysis of the COH-QOL-Ostomy Questionnaire, all item-scale correlations were above 0.40 indicating satisfactory convergent validity of the items. However, Item 9 showed a lower correlation with physical well-being subscale. The results of the assessment of convergent validity are shown in Table 3.
Table 3.
Convergent and discriminant validity for subscales of COH-QOL-Ostomy questionnaire
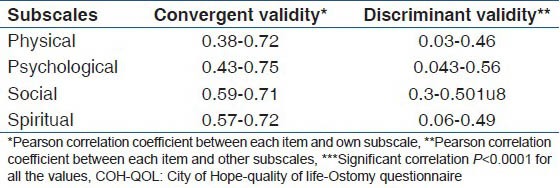
Given the sample size in the current study and standard error of 0.1, correlation coefficient of each subscale with its own items had to be at least one SD larger than its correlation with items of other subscales. In this study, all items, except Item 8 and Item 39, represented adequate discriminant validity [Table 3] (Item 8 on physical-being an Item 39 on spiritual well-being had high correlation with other subscales and did not have adequate discriminant validity).
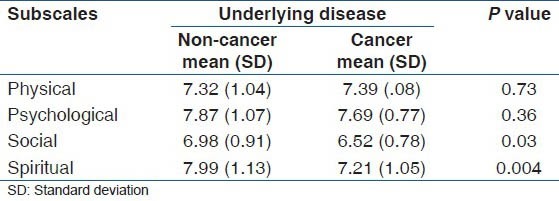
Known group comparison analysis showed significant differences in social and spiritual well-being, and the cancer patients with Ostomy had the worst well-being in the mentioned subscales [Table 4].
Table 4.
Comparison group analysis based on underlying disease
Discussion
The results of this study suggest that the Persian version of COH-QOL-Ostomy questionnaire is a valid and reliable tool for assessing QOL in patients with Ostomy in Iran, and it can be used in clinical researches. Minimum rate of incomplete questions and missing items indicate that this instrument is acceptable and intelligible for patients.
Although, the original COH-QOL-Ostomy questionnaire has been shown to be valid and reliable in the English language;[4] no article has been published about validation of this questionnaire in other languages. Our findings showed that this questionnaire has the potential to be used as a cross-culturally valid instrument to measure the health-related QOL in multicultural research settings.
The present study proved that the Persian version of COH-QOL-Ostomy questionnaire has good convergent validity, marginal discriminatory power, internal consistency and reliability. The results of the reliability analysis were satisfactory. The internal consistency reliability coefficient was high for all subscales. Internal consistency coefficient greater than 0.7 is considered as optimal;[6] therefore, these results suggest that the COH-QOL-Ostomy questionnaire has a good internal consistency.
Interscale correlation analysis showed that all subscales of COH-QOL-Ostomy questionnaire had a low to moderate correlation with the other subscales, indicating that these areas are related but represent various aspects of QOL.
Findings showed that all item-scale correlation coefficients met the standards of convergent and discriminant validity. The convergent validity was acceptable and correlation between items within each subscale was high. The correlation of each item with its constitutive dimension was higher than with the others that indicates to good discriminative ability of COH-QOL-Ostomy questionnaire.
To test the discriminatory power of COH-QOL Ostomy in separating different subgroups of people with different clinical status, the subscale scores of patients were compared according to their underlying diseases. According to the analysis, social and spiritual subscales were able to differentiate between patients with different underlying diseases, but physical and psychological subscales did not have such a significant discriminatory power. However, this could be due to use of inappropriate variable for known group comparison analysis. In other words, it is possible that the underlying disease leading to Ostomy surgery has had no impact on current physical and psychological well-being of patients.
The current study is the first study of its type in Iran focusing on standardizing a specific instrument to measure QOL in patients with Ostomy. However, the interpretation of results is limited due to using exclusively Ostomy patients of Iranian Ostomy Association. Multicentric studies are needed to confirm these results and their generalizability.
Conclusion
The findings supported the reliability and validity of Persian version of COH-QOL-Ostomy Questionnaire. This questionnaire is the only disease-specific QOL questionnaire available for patients with Ostomy in Iran. The instrument was also found to be acceptable to Iranian patients. It will be considered as a valuable instrument to assess the different aspects of HRQOL in Ostomy patients and recommended for use in clinical research.
Acknowledgments
We would like to express our appreciation to Mrs. Minai (the ET nurse of IOS), Mrs. Rostamzadegan and Mrs. Choopani (the secretariats of IOS) for their assistance in data collection.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Dabirian A, Yaghmaei F, Rassouli M, Tafreshi MZ. Quality of life in ostomy patients: A qualitative study. Patient Prefer Adherence. 2010;5:1–5. doi: 10.2147/PPA.S14508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Prieto L, Thorsen H, Juul K. Development and validation of a quality of life questionnaire for patients with colostomy or ileostomy. Health Qual Life Outcomes. 2005;3:62. doi: 10.1186/1477-7525-3-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Krouse R, Grant M, Ferrell B, Dean G, Nelson R, Chu D. Quality of life outcomes in 599 cancer and non-cancer patients with colostomies. J Surg Res. 2007;138:79–87. doi: 10.1016/j.jss.2006.04.033. [DOI] [PubMed] [Google Scholar]
- 4.Grant M, Ferrell B, Dean G, Uman G, Chu D, Krouse R. Revision and psychometric testing of the city of Hope quality of life-Ostomy questionnaire. Qual Life Res. 2004;13:1445–57. doi: 10.1023/B:QURE.0000040784.65830.9f. [DOI] [PubMed] [Google Scholar]
- 5.Marquis P, Marrel A, Jambon B. Quality of life in patients with stomas: The Montreux study. Ostomy Wound Manage. 2003;49:48–55. [PubMed] [Google Scholar]
- 6.Safaee A, Moghim Dehkordi B. Validation study of a quality of life (QOL) questionnaire for use in Iran. Asian Pac J Cancer Prev. 2007;8:543–6. [PubMed] [Google Scholar]
- 7.Aronovitch SA, Sharp R, Harduar-Morano L. Quality of life for patients living with ostomies: Influence of contact with an ostomy nurse. J Wound Ostomy Continence Nurs. 2010;37:649–53. doi: 10.1097/WON.0b013e3181f90d16. [DOI] [PubMed] [Google Scholar]
- 8.Carlsson E, Berndtsson I, Hallén AM, Lindholm E, Persson E. Concerns and quality of life before surgery and during the recovery period in patients with rectal cancer and an ostomy. J Wound Ostomy Continence Nurs. 2010;37:654–61. doi: 10.1097/WON.0b013e3181f90f0c. [DOI] [PubMed] [Google Scholar]
- 9.Colquhoun P, Kaiser R, Jr, Efron J, Weiss EG, Nogueras JJ, Vernava AM, 3rd, et al. Is the quality of life better in patients with colostomy than patients with fecal incontience? World J Surg. 2006;30:1925–8. doi: 10.1007/s00268-006-0531-5. [DOI] [PubMed] [Google Scholar]
- 10.Ito N, Tanaka M, Kazuma K. Health-related quality of life among persons living in Japan with a permanent colostomy. J Wound Ostomy Continence Nurs. 2005;32:178–83. doi: 10.1097/00152192-200505000-00006. [DOI] [PubMed] [Google Scholar]
- 11.Norton C, Burch J, Kamm MA. Patients’ views of a colostomy for fecal incontinence. Dis Colon Rectum. 2005;48:1062–9. doi: 10.1007/s10350-004-0868-5. [DOI] [PubMed] [Google Scholar]
- 12.Wilson TR, Alexander DJ. Clinical and non-clinical factors influencing postoperative health-related quality of life in patients with colorectal cancer. Br J Surg. 2008;95:1408–15. doi: 10.1002/bjs.6376. [DOI] [PubMed] [Google Scholar]
- 13.Azadeh S, Moghimi-Dehkordi B, Fatem SR, Pourhoseingholi MA, Ghiasi S, Zali MR. Colorectal cancer in Iran: An epidemiological study. Asian Pac J Cancer Prev. 2008;9:123–6. [PubMed] [Google Scholar]
- 14.Kolahdoozan S, Sadjadi A, Radmard AR, Khademi H. Five common cancers in Iran. Arch Iran Med. 2010;13:143–6. [PubMed] [Google Scholar]
- 15.Derakhshan F, Khojeini EV, Balaii H, Naderi N, Firouzi F, Farnood A, et al. Epidemiology of inflammatory bowel disease in Iran: A review of 803 cases. Gastroenterol Hepatol Bed Bench. 2008;1:19–24. [Google Scholar]
- 16.Gemmill R, Sun V, Ferrell B, Krouse RS, Grant M. Going with the flow: Quality-of-life outcomes of cancer survivors with urinary diversion. J Wound Ostomy Continence Nurs. 2010;37:65–72. doi: 10.1097/WON.0b013e3181c68e8f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gao W, Yuan C, Wang J, Du J, Wu H, Qian X, et al. A Chinese version of the city of Hope quality of life-Ostomy questionnaire: Validity and reliability assessment. Cancer Nurs. 2013;36:41–51. doi: 10.1097/NCC.0b013e3182479c59. [DOI] [PubMed] [Google Scholar]
- 18.Häuser W, Dietz N, Grandt D, Steder-Neukamm U, Janke KH, Stein U, et al. Validation of the inflammatory bowel disease questionnaire IBDQ-D, German version, for patients with ileal pouch anal anastomosis for ulcerative colitis. Z Gastroenterol. 2004;42:131–9. doi: 10.1055/s-2004-812835. [DOI] [PubMed] [Google Scholar]
- 19.Beitz J, Gerlach M, Ginsburg P, Ho M, McCann E, Schafer V, et al. Content validation of a standardized algorithm for ostomy care. Ostomy Wound Manage. 2010;56:22–38. [PubMed] [Google Scholar]
- 20.Ware JE, Harris WJ, Gandek B, Rogers BW, Reese PR. Boston, MA: Health Assessment Lab; 1997. MAP-R for Windows: Multitrait Multi-Item Analysis Program – Revised User's Guide. [Google Scholar]