

Abstract
Purpose: To study contents of atherosclerotic plaques for the presence of fungi of the genus Candida; and an analysis of some immunological and biochemical indices in patients with acute coronary syndrome (ACS) that are positive for Candida albicans. Materials and methods: To test for the presence of fungi in an atherosclerotic plaque, we used a method developed by us (patent NO 531, a priority from 6/28/2010). A total of 47 atherosclerotic plaques were obtained during 20 autopsies. In addition, 80 individuals (58 male, 22 female; age range from 29 to 85) with acute coronary syndrome were subjected to a blood biochemical test, including quantification of TNF-α levels and IgG and IgM to Candida albicans was determined. Results: Fungi of the genus Candida were identified in 31.9% (15 out of 47) of atherosclerotic plaques. Particularly, Candida krusii and Candida grabrata were identified in overwhelming majority, although solitary colonies of Candida tropicalis and a single colony of Candida albicans were also detected. 80 (100%) patients were negative for IgM, but 30 (37.5%) were positive for IgG to Candida albicans. TNF-α was detected in a smaller quantity of IgG-negative patients (36.7%) relative to patients of IgG-positive group (70%), however its levels were considerably above in the first group (511.73±195.80 pg/ml) than in the second one (326.68±259.91 pg/ml, P < 0.05). Differences in the levels of ASAT and ALAT in patients positive to Candida albicans and negative for TNF-α were significantly higher than in the rest of patients. Conclusion: It is conceivable that fungi of the genus Candida are capable of inducing an inflammation of the vascular wall that in turn can lead to the development of atherosclerosis.
Keywords: Atherogenesis, fungi Candida, inflammation
Introduction
Atherosclerotic defeat of blood-vessels is present on the basis of many nosological units leading to early physical inability and mortality, which necessitates the studying of etiopathogenesis of atherosclerosis [1]. The inflammatory theory received a widesptread focus at the end of the last century according to which various infectious agents may serve as etiological factors of atherosclerosis [2-5].
A large set of methods are currently used for determination of interrelation of somatic disease with infectious agents such as epidemiological supervision, serological researches, detection of an antigen of bacteria and viruses, allocation of pure culture of a concrete microorganism from target organs, and also reproduction of some kinds of somatic pathology through infection of laboratory animals.
In addition to serological tests fluorescence microscopy is widely applied to the examination of contents of atherosclerotic plaques. Ch. pneumoniae, Cytomegalovirus and Herpes simplex were detected in atherosclerotic plaques by this method [6,7]. Currently, a relationship between cardiovascular diseases and infectious agents such as Chlamydia pneumoniae, Cytomegalovirus and Herpes simplex, Mycop-lasma infection, Helicobacter pilori are well-accepted [8-10]. These infection agents are characterized by endocellular vital activity used resources of cells-targets of the owner, ex-pressed immune suppressive properties and long persistency in an organism.
However, some fungi, in particular genus of Candida, also have properties similar to those discussed above. The fungi of genus Candida, which are present practically on all parts of the human body, are conditional-pathogen that can cause candidiasis when immunity is compromised. Studies of the most widespread fungus Candida albicans have revealed that it produces specific substances, such as adhesions and ligands, which suppress affixing of neutrophils to Candida, and reduce chemotaxis of leukocytes. Mann proteins found on the cell walls constitute external antigens of Candida albicans, and also play a dominant role in processes of colonization, adhesions and infection of fungi of genus Candida. A series of experiments have revealed that a culture of Candida is capable of producing a water-soluble high molecular weight fraction CAWS, also consisting of mannoproteins and β-glycan. Investigations of the biological activity of CAWS have allowed to reveal a number of features. It was found out that CAWS induces the production IFN-φ and IL-6 by splenocytes at a low dose (10 μg/ml), but inhibits proliferation of splenocytes induced by polysaccharides and T-cell mitogens at a high dose. In addition, CAWS blocks the production of trombodulin by endothelial cells and synergizes with TNFα, which in turn activates the curtailing system of blood [11].
Experiments introducing highly filtered solution of CAWS into mice a dose of 4 mg have revealed that animals develop arteritis and cardiomegaly, accompanied by increases in the levels of pro-inflammatory cytokines. Thus, the presence of the vital activity of fungi Candida in an organism contributes to damaging of the blood vessels both directly as well as through cytokines produced in response to them [12].
The purpose of this work is to study the contents of atherosclerotic plaques for the presence of fungi of the genus Candida, and analyses of some immunological and biochemical indicators in patients with acute coronary syndrome that are positive for Candida albicans.
Materials and methods
Detecting Candida
In order to reveal the fungi Candida albicans in contents of atherosclerotic plaques, we have worked out and used the method for detecting of microorganisms in atherosclerotic plaques, based on the method of cultural diagnostics (Patent number #531, priority date 28.06.2010). In order to determine the role of Candida albicans, we have developed and used a new method of identification of microorganisms in an atheromatous plaque (patent No 531, priority 28.06.2010 “Method for identification of a possible causative agent of atherosclerosis”). Our method is based on cultural diagnosis of microorganisms in a biological substance.
Cultural diagnosis is carried out in order to separate the microorganism from the tissue or other biological substance in order to determine the generic and specific assignment of the causative agent by separating a pure culture of the microorganism and study of its biological characteristics. Samples of the material to be studied are placed in a sterile dish and inoculated onto different culture media. Microorganisms are incubated at 36°C. In positive cases growth can be observed in 2-5 days. Identification of the microorganism is performed on the basis of microscopic data of pathological material, cultural characteristics, biochemical activity, etc.
Our task was to use the cultural diagnosis method to identify microorganisms in the content of an atheromatous plaque or its bottom.
For the purposes of the bacteriological study we used descending parts of the aorta, 3-5 cm x 3-5 cm in size, containing a minimum of 2 undamaged athromatous plaques at least 0.5 cm in size. Parts of the aorta were taken during autopsy provided no more than 24 hours elapsed from the time of death and death was either violent or non-violent provided there were no signs of chronic infectious diseases, oncological diseases and abscesses. After mechanical removal of blood clots with water and drying on a sterile rug, parts of the aorta were transported to the laboratory in a sterile dish (a disposable plastic cup with a Petri lid). In the laboratory bacteriological inoculation was carried out with all stages of work being photographed using digital camera. All undamaged plaques at least 0.5 cm in size were examined, which to some extent is an indication of the presence of atheromatous mass in the plaque. If the plaque is roughly 0.5 cm in diameter, a puncture of its operculum is carried out, where the sterile puncture needle is inserted into the plaque in parallel to the aorta on the lumens side, cut side up, having treated the site of injection with alcohol. Large-size plaques or calcareous plaques after treatment with alcohol are opened up with scissors. For which purpose, having purified the wire inoculating loop, tweezers and scissors/puncture needs over a burner flame, a plaque at least 0.5 cm in size is selected and holding it with tweezes on both sides the operculum is removed. If there is content (atheromatous mass) inside, carefully, without touching the sides, remove a part of the mass using the wire inoculating loop and inoculate onto different culture media - blood agar-agar, sugar broth, Sabouraud’s medium - culture medium No 2 GRM (ready medium for fungus identification). For the purposes of identification of the separated Candida type fungus, the mass was reinoculated onto HiCrome Candida Agar (HiCrome Candida differential Agar) - a chromogenic agar for Candida fungus is a selective and differential medium conductive to quick separation of the fungus from mixed cultures and enabling color and morphological differentiation of fungi colonies Candida albicans, Candida tropicalis, Candida krusei, Can-dida grabrata. If there is no atheromatous mass or its quantity is insufficient the bottom of the plaque is scraped and the content is inoculated onto the specified cultural media. The inoculated cultural medium is placed into a thermostat with a constant temperature of 30-32°C and incubated for 5-7 days. In positive cases small colonies can be observed on the medium on the second day: on Sabouraud’s medium there are small protruding colonies of white color, and on HiCrome Candida Agar the color of the colony depends of the type of fungi.
The proposed method of identification of microorganisms from atheromatous plaques is sufficiently effective, as it enables to screen out Candida type fungi, and in addition to this the use of HiCrome Candida Agar already enables the differentiation of colonies based on color. Frequency of separation of Candida type fungi from atheromatous plaques is approximately 30%.
Aortic sections
Aortic sections with at least 2 intact plaques were obtained during autopsies. None of the autopsy patients had violent death, symptoms of chronic infectious diseases, cancer formation or purulent process, and autopsies were carried out within 24 hours of death. Overall, 47 athesclerotic plaques were obtained from 20 autopsies.
Inoculation of atheromatous mass was carried out on Saburo medium for replanting them on HiCrome Candida Differential Agar (HIMEDIA, Russia-India).
Patients with ACS: 80 patients with acute coronary syndrome (58 male, 22 female, age range: 29-85, mean age is 60.14±10.78) were diagnosed on the basis of clinical and patient examination data and history.
Biochemical blood analyses, including determination of TNF-alpha levels, were conducted on all patients within the first two hours after hospital admission. In order to determine immunological markers of Candida albicans, the blood of patients was collected under conditions of basic metabolism.
Data processing was carried out in Microsoft Office Excel 2007.
The comparison of groups were performed using Student’s t-test, non-parametric data were compared using chi-square test.
Statistical significance threshold was set at P < 0.05.
Results
The presence of microorganisms in atheromatous plaques proves its connection to atherosclerosis. At present the method of fluorescent microscopy is widely used for this purpose. However this method requires expensive equipment and reagents, and an important role is played by the qualification of the expert carrying out the procedure.
An analysis of the contents of atherosclerotic plaques showed that 31.9% of plaques contained fungi of the genus Candida (Figure 1).
Figure 1.
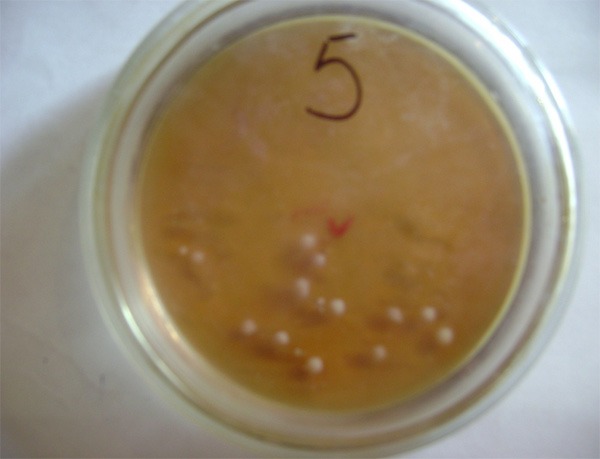
Candida colonies on Saburo medium after inoculation of contents of an atherosclerotic plaque (5th day).
Candida krusii and Candida grabrata were detected as the predominant species, although isolated colonies of Candida tropicalis and a single colony of Candida albicans were also detected (Figure 2).
Figure 2.
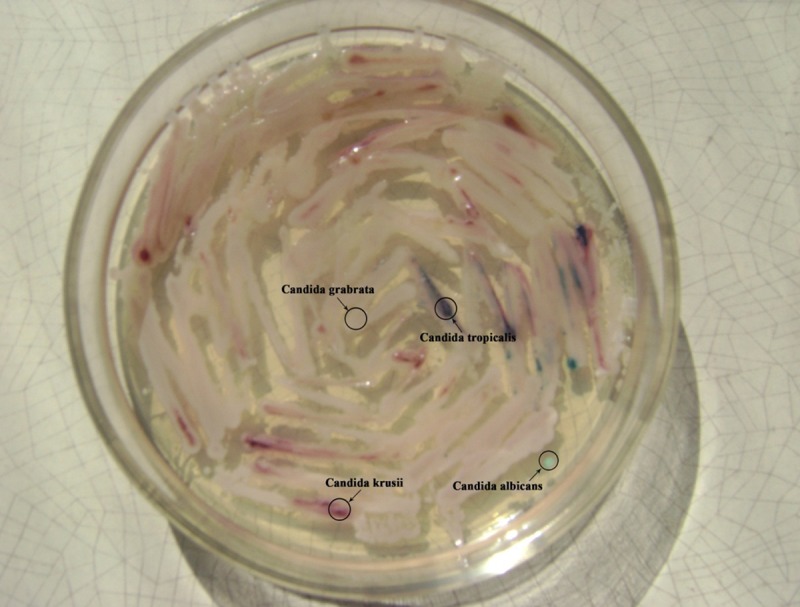
Candida colonies grown after replanting them on medium HiCrome Candida Agar (HiCrome Candida differential Agar) on 5th day.
Presence of antibodies against the causative agent shows first of all the presence of infection in the body, and to a certain extent the degree of sensibilization of the body to it.
ELISA results showed that none of 80 patients had antibodies of IgM class.
30 (37.5%) out of 80 patients were negative for antibodies of IgG class to Candida albicans.
Based on these data, patients were divided into 2 groups based on positivity to IgG Candida albicans (group I: negative, group II: positive). The level of anti-inflammatory cytokine TNF-α reflects the degree of inflammation, to which in accordance with the inflammatory theory of atherogenesis the destabilization of the plaque is connected, which is clinically manifested in an acute coronary syndrome.
It was found that in group I (30 patients), TNF-α was detected in 11 patients (36.7%), with an average level of 511.73±195.80 pg/ml. In group II, consisting of 50 patients, TNF-α was detected in 35 patients (70%), and the average level was 326.68±59.91 pg/ml. The calculation of nonparametric agreement criterion of chi-squared confirmed the difference in the frequency of TNF-α, depending on the presence of IgG antibodies to Candida albicans (Figure 3). The difference in the levels of TNF-α between the two groups is also statistically significant (test of Mann-Yitny, P < 0.05).
Figure 3.
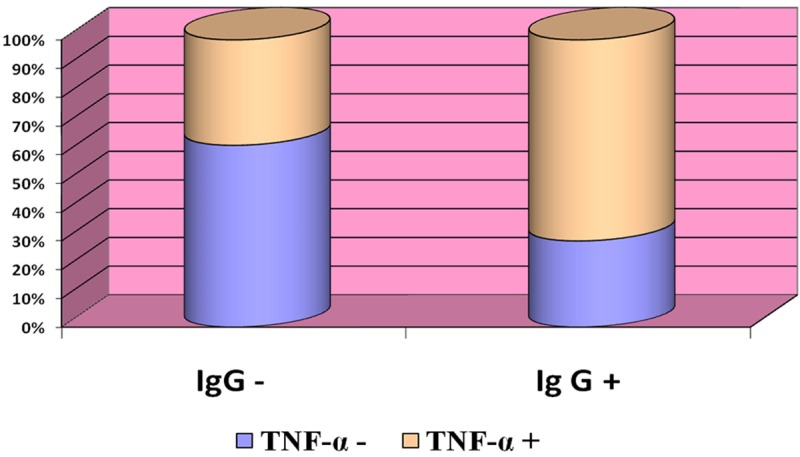
Frequency of TNF-α production in ACS patients that are negative or positive to antibodies of class IgG to Candida albicans
Then, we divided patients into more groups based on the presence of serum TNF-α, and additional tests of various biochemical parameters were conducted. Our work has revealed that in people who have class IgG Candida albicans acute coronary syndrome is observed more often than in people who do not have Candida albicans antibodies, and when such people do have acute coronary syndrome it is accompanied with a lower level inflammatory process (Table 1).
Table 1.
Laboratory representatives of blood of the patients positive and negative to Candida albicans, depending on presence or absence TNF-α (M±m)
| IgG negative | IgG positive | |||
|---|---|---|---|---|
|
|
||||
| TNF-α negative (n = 30) | TNF-α positive (n = 11) | TNF-α negative (n = 15) | TNF-α positive (n = 35) | |
| ASAT | 10.18±3.07* | 12.12±5.72* | 20.77±14.18* | 12.85±6.40* |
| ALAT | 13.78±4.35 | 15.57±8.34 | 27.69±24.11* | 16.30±8.18* |
| Urea | 6.93±1.71 | 6.12±1.35 | 6.31±2.26 | 6.49±2.56 |
| Total protein | 69.35±4.25 | 71.94±2.82 | 70.64±3.56 | 69.71±3.55 |
| Total bilirubin | 15.88±3.69 | 17.33±4.55 | 16.46±4.07 | 15.68±3.79 |
| Conjugated bilirubin | 4.05±1.39 | 4.62±1.78 | 4.22±1.67 | 4.14±1.0 |
| Total cholesterol | 5.15±1.71 | 5.07±1.05 | 5.73±1.63 | 5.21±1.33 |
| Cholesterol-high density lipoproteins | 1.00±0.31 | 0.97±0.38 | 0.94±0.26 | 1.02±0.25 |
| Cholesterol-low density lipoproteins | 3.66±1.52 | 3.29±0.84 | 3.79±1.41 | 3.54±0.99 |
| TG | 1.32±0.68 | 1.78±1.18 | 2.26±1.67 | 1.50±0.75 |
| TNF-α | - | 511.73±195.80* (36.7%) | - | 317.66±261.56* (70%) |
P < 0.05.
Based on Student’s T-test, show that differences of ASAT and ALAT in patients with IgG class antibodies to Candida albicans and the absence of TNF-α are significant.
Discussion
The results of our work do not reveal a relationship between destabilization of atherosclerotic process and acute candidiasis infection or an aggravation of the chronic candidiasis caused by Candida albicans. Nevertheless ACS authentically develops more often in the persons having antibodies of class IgG to Candida albicans, rather than in the persons who do not have antibodies to this infection and proceeds at less expressed inflammatory process. It is possible that this is related to the circulation of products of fungi in blood, which may lead to the damage of the vascular wall, causing an inflammatory process. High indices of transaminases in patients with presence of antibodies of IgG class to Candida albicans and absence TNF-α is consistent with the data on damaging action of the proteins of cellular membranes of Candida albicans to hepatocytes, which causes the parenchymal inflammation of the liver [7]. In turn, increased functional activity of the liver can lead to destabilization of atherosclerosis [14,15].
We have not observed a stark difference in blood lipids of patients based on the presence or absence of IgG class antibodies to Candida albicans and tumour necrosis factor in their blood.
Based on our results, it is possible to assume that fungi of genus Candida are capable of inducing an inflammation of the vascular wall, which in turn can lead to development of atherosclerosis. However based on our study, we cannot reliably assert that damage of the vascular wall by fungi is primary, because fungi are capable of existing and breeding in phagocytes and can get to the plaque together with a phagocyte at the moment of its migration into the vessel’s intima [16].
Virtual absence of Candida albicans among planted colonies in prevalence of Candida krusii and Candida grabrata is consistent with the data about reduced rate of candidiases caused by Candida albicans simultaneously with increasing rates of candidiases caused by Candida krusii and Candida grabrata [17,18]. Possibly, it is related with wide use of fluconazole - antifungal means of threeazol line to which Candida albicans has high-sensitivity, but Candida krusii and Candida grabrata possess natural resistance [17].
The data obtained by us are in line with the hypothesis put forward by P.S.R.K. Sastry [19], stating that the fungal infection can play a role in the development of atherosclerosis.
Disclosure of conflict of interest
None.
References
- 1.Akberov RF, Shafareyev AZ, Mihaylov MH. Progressing multifocal atherosclerosis: an etiology, clinical-radio diagnostics, modern aspects of treatment. Kazan: Ideal-Press publishing; 2008. [Google Scholar]
- 2.Alekperov EZ, Nadjarov RN. Modern concepts of the inflammation role in an atherosclerosis. Cardiology. 2010;6:88–91. [PubMed] [Google Scholar]
- 3.Vatutin NT, Chupina VA. Infection as the factor of development of the atherosclerosis and its complications. Cardiology. 2000;2:67–71. [Google Scholar]
- 4.Reshetnikov V, Malyutina SK, Nikitin YP. Frequency of the revealings of some infections in patients with an ischemic heart trouble. Clin Med. 2008;2:33–37. [Google Scholar]
- 5.Yulish YI, Nagornaya NV. Chronic endocellular infections and cardiovascular pathology. Clinical Lectures. 2007:2. [Google Scholar]
- 6.Muhlestein JB, Hammond EH, Carlquist JF, Radicke E, Thomson MJ, Karagounis LA, Woods ML, Anderson JL. Increased Indence of chlamydia species within the coronary arteries of patents with symptomatic atherosclerotic versus other forms of cardiovascular disease. J Am Coll Cardiol. 1996;7:1555–1561. doi: 10.1016/0735-1097(96)00055-1. [DOI] [PubMed] [Google Scholar]
- 7.Szkaradkiewich A, Bogaczy E, Ska-Staniewicz J, Torliński L, Wal M. Cytomegalovirus infection and atherosclerosis. Med Sci Monit. 2002;8:104–7. [PubMed] [Google Scholar]
- 8.Campbell LA, Yaraei K, Van Lenten B, Chait A, Blessing E, Kuo CC, Nosaka T, Ricks J, Rosenfeld ME. The acute phase reactant response to respiratory infection with Chlamydia pneumoniae: implication for the patogenesis of atherosclerosis. Microbes Infect. 2010;12:598–606. doi: 10.1016/j.micinf.2010.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Epstein SE, Zhou YF, Zhu J. Infection and atherosclerosis: emerging mechanistic paradigms. Circulation. 1999;100:e20–8. doi: 10.1161/01.cir.100.4.e20. [DOI] [PubMed] [Google Scholar]
- 10.Shiu B, Viira Y, Taker V, Fong I. Chlamidia pneumaniae (ChP), cytomegalovirus (C) and virus Herpes simplex (VHS) in an atherosclerosis of the carotid artery. Int Med Journal. 1998;2:136–138. [Google Scholar]
- 11.Kiyoshi K, Shingo Y, Miura NN, Horie S, Usui Y, Adachi Y, Yadomae T, Ohno N. Effect of CAWS, a mannoprotein-β-glican Complex of Candida albicans, on leukocyte, Endotelial Cell and Platelet Functions in vitro . Biol Pharm Bull. 2003;26:233–240. doi: 10.1248/bpb.26.233. [DOI] [PubMed] [Google Scholar]
- 12.Nagi-Miura N, Harada T, Shinohara H, Kurihara K, Adachi Y, Ishida-Okawara A, Oharaseki T, Takahashi K, Naoe S, Suzuki K, Ohno N. Lethal and severe coronary arteritis in DBA/2 mice induced by fungal pathogen, CAWS, Candida albicans water-soluble fraction. Atherosclerosis. 2006;186:310–320. doi: 10.1016/j.atherosclerosis.2005.08.014. [DOI] [PubMed] [Google Scholar]
- 13.Ivashkin VT. Cellular and molecular biology of the liver inflammation. Russ J Gastroenterol Hepatol Coloproctol. 1998;5:13–17. [Google Scholar]
- 14.Wang CC, Lin SK, Tseng YF, Hsu CS, Tseng TC, Lin HH, Wang LY, Kao JH. Elevator of serum aminotransferase activity increases risk of carotid atherosclerosis in patients with non-alcoholic fatty liver disease. J Gastroenterol Hepatol. 2009;24:1411–1416. doi: 10.1111/j.1440-1746.2009.05872.x. [DOI] [PubMed] [Google Scholar]
- 15.Marevichev MM, Jdanov VS, Galahanov IY. Atherosclerosis depending on alcohol intake in almost healthy men. Cardiovascular Therapy Prof. 2009;8(Suppl 1):226. [Google Scholar]
- 16.Bayramova GR. Modern view to the problem of chronic relapsing vulvovaginal candidiasis. Obstetrics Gynecology. 2008;4:52–56. [Google Scholar]
- 17.Bayramova GR. Chronic relapsing vulvovaginal candidiasis: the diagnostic principles and therapy possibilities. Obstetrics Gynecology. 2008;6:64–66. [Google Scholar]
- 18.Leroy O, Gangneux JP, Montravers P, Mira JP, Gouin F, Sollet JP, Carlet J, Reynes J, Rosenheim M, Regnier B, Lortholary O AmarCand Study Group. Epidemiology, Management and Risk Factor for Death of Invasive Candida Infections in Critical Care: A Multicenter, Prospective, Observational Study in Franse. Crit Care Med. 2009;37:1612–1618. doi: 10.1097/CCM.0b013e31819efac0. [DOI] [PubMed] [Google Scholar]
- 19.Sastry PS. Occult fungal infection is the underlying patogenic cause of atherogenesis. Med Hypotheses. 2004;63:671–674. doi: 10.1016/j.mehy.2003.12.050. [DOI] [PubMed] [Google Scholar]