

Abstract
Purpose
The present study aimed to examine the age and gender distributions among chronic cough patients referred to a tertiary cough clinic in Korea, and to investigate clinical factors related to the demographic findings.
Methods
Study participants were unselectively recruited from adult chronic cough patients who attended the cough clinic for the first time during one year. To validate their representativeness, their age and gender distributions were compared to the entire chronic cough population, or with those presenting with other chronic disease. Data from the baseline investigations were analyzed to identify clinical factors related to the demographic findings.
Results
A total of 272 chronic cough patients were included. They had a middle-aged female predominant feature (mean age: 52.8±15.7 years and female 69.1%). Their age and gender distributions were almost identical to the entire chronic cough population, but were distinct from patients with hypertension. Among clinical factors, the older female predominance was associated with enhanced capsaicin cough sensitivity, and also with the presence of 'cough by cold air' symptom. Allotussia and laryngeal paresthesia were highly common in chronic cough patients, affecting 94.8% and 86.8% of them, respectively.
Conclusions
The present study demonstrated older female predominance among adult chronic cough patients attending a referral cough clinic in Korea. The demographic features were significantly associated with the capsaicin cough responses and also potentially with allotussia (particularly cold air as the trigger). These findings suggest a role of cough reflex sensitization in the pathophysiology of chronic cough in adults.
Keywords: Cough, respiratory hypersensitivity
INTRODUCTION
Cough is a fundamental reflex defense mechanism and a common reason for patients to seek medical care. Chronic cough (>8 weeks duration) is a major health issue that affects 9%-33% of the population1 and severely impairs quality of life.2,3
Female predominance in western populations has been observed in chronic cough patients attending cough clinics.4,5,6,7,8,9,10 In the literature, several factors are related to the predominance of females such as a different likelihood of seeking medical attention,8 objective cough frequency,5 and cough reflex sensitivity.5,11,12,13,14,15,16 A major proportion of chronic cough patients are middle-aged or elderly females4,5,9,10,11; however, there is still no clear explanation on the demographic findings.
This study primarily examined the age and gender distributions of Korean adult chronic cough patients referred to a specialized clinic. In addition, we explored the clinical factors relevant to the demographic findings.
MATERIALS AND METHODS
Study participants
We examined the age and gender distributions of adult patients presented to a tertiary referral cough clinic with chronic cough (>8 weeks duration) from April 2012 to March 2013. Study participants were recruited randomly from chronic cough patients who attended a clinic for the first time during the study period. The criteria for the study were subjects aged ≥18 years old and without evidence of active pulmonary infection or malignancy. All participants provided written informed consent. The study protocol was approved by the institutional review board of Seoul National University Hospital.
Electronic medical record searches for demographic comparisons
An electronic medical record search was performed on outpatient visit records under the search term of 'chronic cough' as the primary diagnosis in order to validate study participants as representative of the entire chronic cough population attending a tertiary clinic. Age and gender parameters were retrieved from adult patients with chronic cough for the first time during the last 5 years (defined as Group A). Second, another search was conducted for the entire population who presented hypertension during one month (defined as Group B) to compare with other chronic diseases.
Clinical assessment
The clinical information analysis of study participants investigated clinical factors associated with demographic characteristics. Upon initial visit, they underwent investigation for differential diagnosis according to diagnostic protocols at the cough clinic such as chest X-rays, PNS views, methacholine challenge tests, induced sputum analyses, capsaicin cough sensitivity tests, rhinoscopy, and structured questionnaires.
Methacholine challenge tests assessed airway hyper-responsiveness (AHR) with a modified protocol based on Chai et al.17 A methacholine challenge test was prepared with diluted saline: 0.5, 1, 2, 4, 8, and 16 mg/mL delivered as an aerosol by a Rosenthal-French dosimeter (Laboratory for Applied Immunology, Baltimore, MD) and a nebulizer (DeVilbiss, Carlsbad, CA). Subjects were instructed to inhale 5 inspiratory capacity breaths while increasing the methacholine concentration from 0.5 to 16 mg/mL. A concentration of methacholine that caused a 20% decrease in forced expiratory volume in 1 second (FEV1) from the baseline was defined as PC20. AHR was defined positive if PC20 <16 mg/mL.18
Induced sputum was analyzed according to European Respiratory Society/American Thoracic Society working group report protocols.19 Sputum eosinophilia was defined as present if the subject had sputum eosinophils ≥3%. A total of 180 subjects completed induced sputum tests successfully (66.7%). No differences were found in age or gender distributions for subjects who underwent successful sputum induction and subjects that did not (n=90).
A capsaicin cough challenge test measured cough reflex sensitivity with a modified version20 of methods suggested by Fujimura et al.15 The subjects inhaled 0.5 to 64 µM of nebulized capsaicin. The process proceeded in a sequential order at 1-min intervals via a nebulizer attached to a breath-activated dosimeter delivering 8 µL. The number of induced coughs was counted and recorded. The test ended when a maximum concentration was reached. Capsaicin cough sensitivity was described as the lowest capsaicin concentration (C5) to provoke 5 consecutive coughs immediately after inhalation. C5 was arbitrarily defined as 128 µM for statistical analyses, if it was not produced in the test concentrations (≤64 µM). The imputation approach was adopted from methacholine challenge tests21; in addition, the total number of capsaicin-induced coughs was counted.
The presence of underlying rhinitis/rhinosinusitis was assessed by clinical history and supplemented by a PNS view or rhinoscopy. Rhinitis/rhinosinusitis was considered present if subjects had nasal symptoms (rhinorrhea and/or nasal obstruction) and/or positive radiologic or endoscopic findings (either nasal polyp, moderate amount of mucopurulent discharge, or more than moderate edema of the middle meatus).
Structured questionnaires included dichotomous yes/no items on 'allotussia' (cough triggered by non-harmful stimuli) and 'laryngeal paresthesia'. Allotussia was defined by a positive response to 'cough by cold air' or 'cough by singing/talking' asked by the question 'cough triggered when you inhale cold air' or 'cough triggered when you sing or talk', respectively. 'Laryngeal paresthesia' was defined by a positive response to 'abnormal throat sensation or tickle when not exposed to a cough trigger'.22
Statistical analysis
Descriptive statistics are presented as categorical variable percentages, means±standard deviations (or medians) and interquartile ranges for continuous variables. Chi-squared tests for categorical variables and unpaired t-tests, Mann-Whitney tests, or ANOVA for continuous variables assessed the group differences; in addition, a Spearman bivariate test analyzed the correlation of the variables. Cough reflex sensitivity (C5) were compared as log-transformed. Stata 12.0 software package (Stata Corporation, College Station, TX, USA) performed the statistical analyses. All tests were 2-sided and P values were significant at <0.05.
RESULTS
Age and gender distribution among chronic cough patients
We randomly recruited 273 chronic cough patients; subsequently, 272 subjects were included after the exclusion of one patient with pulmonary tuberculosis. Table 1 describes the baseline characteristics. The mean age was 52.8±15.7 years with a female predominance (69.1%). The age of onset for chronic cough was 49.2±16.2 years and disease duration before the initial visit was a 12 month median. Histograms in Fig. 1A and B present age, age of onset, and gender distributions.
Table 1.
Baseline characteristics of 272 chronic cough patients
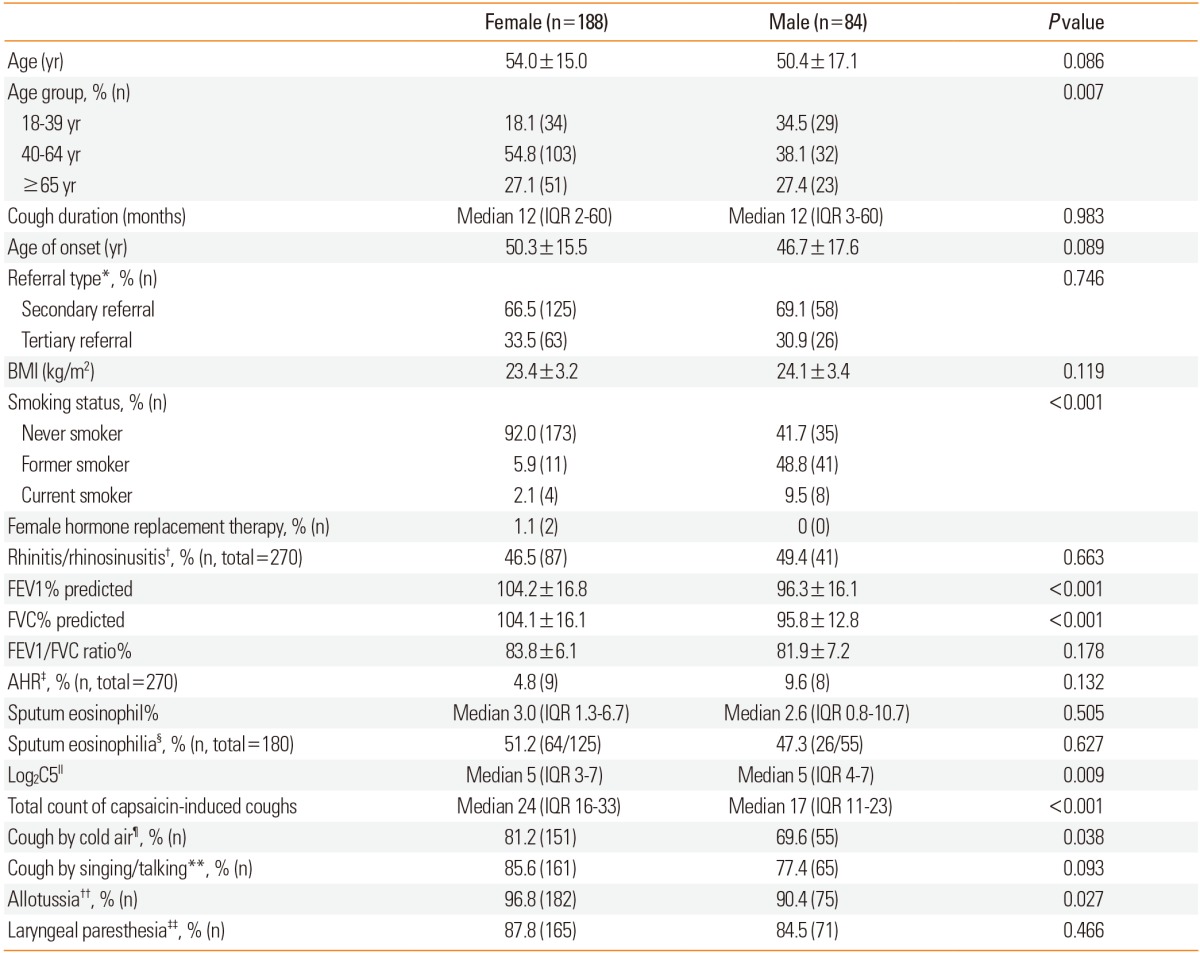
P values were determined by chi-squared tests, t-tests, or Mann-Whitney tests.
*Referral type defined as 'secondary referral' (if from primary physicians) or 'tertiary referral' (if from other specialists in secondary or tertiary hospitals); †Rhinitis/rhinosinusitis defined as positive if the subject had definite nasal symptoms (rhinorrhea and/or nasal obstruction) or positive nasal endoscopic findings (nasal polyp, mucopurulent discharge or edema in middle meatus); ‡AHR defined as positive if the subject had methacholine PC20 <16 mg/mL; §Sputum eosinophilia defined as positive if the subject had induced sputum eosinophil ≥3%; ∥C5 was defined by the lowest capsaicin concentration to provoke 5 consecutive coughs within one minute after inhalation; ¶Cough by cold air defined as positive if the subject answered yes to the questionnaire item 'cough triggered when you inhale cold air'; **Cough by singing/talking defined as positive if the subject answered yes to the questionnaire item 'cough triggered when you talk or sing'. ††Allotussia defined as positive if 'cough by cold air' or 'cough by singing/talking' was positive; ‡‡Laryngeal paresthesia defined as positive if the subject answered yes to the questionnaire item 'abnormal throat sensation or tickle when not exposed to a cough trigger'.
BMI, body mass index; IQR, interquartile range; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; AHR, airway hyper-responsiveness.
Fig. 1.
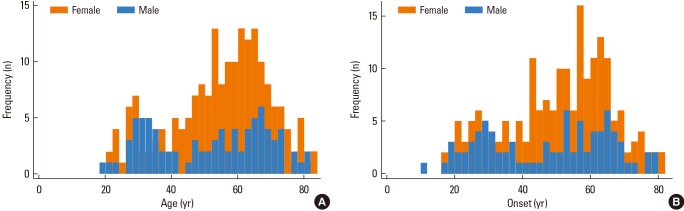
Histograms of age (A) and age of onset (B) distribution based on gender for study participants who presented chronic cough on the initial visit (n=272).
Age and gender distributions were compared with all chronic cough patients over the last 5 years (Group A, n=1,732) to validate representativeness. The study results indicated almost identical distributions in age and gender, compared with group A (age: 52.8±15.7 vs 51.8±16.2 years, P=0.670; and female: 69.3% vs 67.6%, P=0.573; Supplementary Figure E1A). In addition, study participants were compared to adult patients with hypertension (Group B, n=1,871) and indicated significant differences in age (52.8±15.7 vs 65.1±11.7 years, P<0.001) and gender (female: 69.3% vs 47.7%, P<0.001; Supplementary Figure E1B).
Clinical factors associated with demographic findings
Females were more prevalent than males with a ratio of 2:1 and the female predominance was evident after 40 years of age. We analyzed the association of clinical factors and demographic findings of 270 patients; excluded from the analysis were 2 patients (1 female and 1 male) that did not undergo a diagnostic investigation for their presumptive causes of cough (taking angiotensin converting enzyme inhibitors). No significant gender differences were indicated by cough duration, type of referral, BMI, rhinitis/rhinosinusitis, FEV1/FVC ratio, methacholine AHR and sputum eosinophilia. However, female cough patients had a significantly higher capsaicin cough sensitivity (lower log2C5 and higher total count of induced coughs) than males. Table 1 shows that female responses to the questionnaire item 'cough by cold air' or allotussia were significant.
Female predominance was more prominent after 40 years of age, and the subjects were arbitrarily categorized into 3 age groups (younger adult group 18-39 years, middle-aged group 40-64 years and elderly group ≥65 years) for subsequent analyses (Table 2). Subsequently, the rates of rhinitis/rhinosinusitis, AHR and sputum eosinophilia did not differ between gender for any age group. Among the clinical features of cough, 'cough by cold air' was more frequent in females than males for the elderly subgroup. 'Cough by singing/talking' was slightly more frequent in females than males for the middle-aged group. However, 'allotussia' or 'laryngeal paresthesia' was highly prevalent and affected 94.8% or 86.8% of chronic cough patients, respectively. The prevalence was similarly frequent (>80%) in every age/gender subgroup.
Table 2.
Age and gender differences for the clinical parameters of 270 chronic cough patients
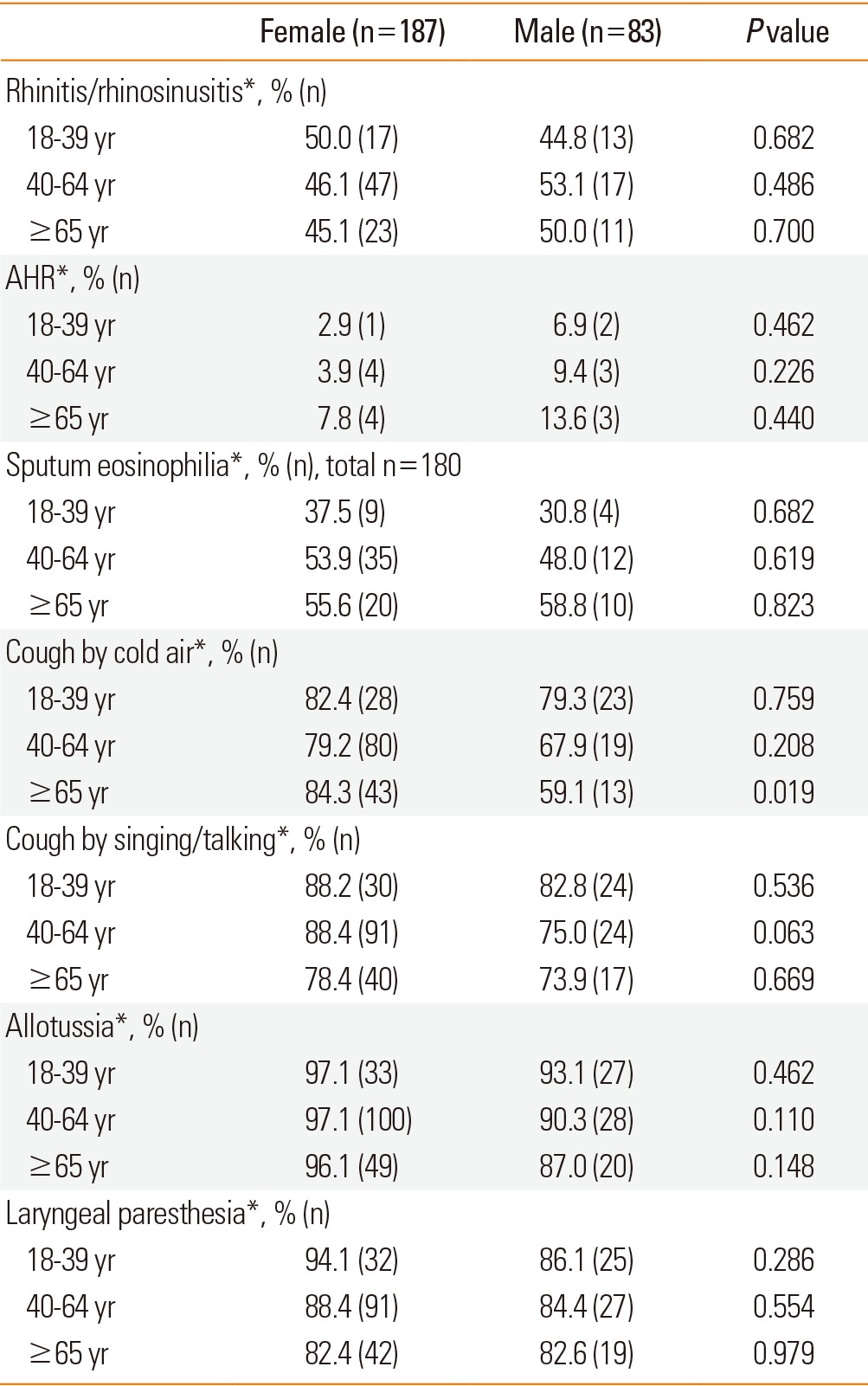
P values were determined by chi-squared test or one-way ANOVA test.
*See Table 1 for definitions.
AHR, airway hyper-responsiveness.
Capsaicin log2C5 was significantly lower in females than males (particularly in the elderly subgroup) and indicated a higher prevalence of capsaicin cough sensitivity for elderly females (Fig. 2). The total challenge test counts of capsaicin-induced coughs were significantly higher for females aged ≥40 years (Fig. 3). The capsaicin C5 (or total counts of induced cough) did not significantly relate to factors such as BMI, smoking status, presence of AHR, sputum eosinophilia, rhinitis/rhinosinusitis, 'cough by singing/talking' and laryngeal paresthesia. However, 'cough by cold air' was significantly associated with total counts of capsaicin-induced cough (years: median 22, IQR 15-32; vs no: median 18, IQR 11-28; P=0.008), and marginally with log2C5 (years: median 5, IQR 4-7; vs no: median 6, IQR 4-7; P=0.073).
Fig. 2.
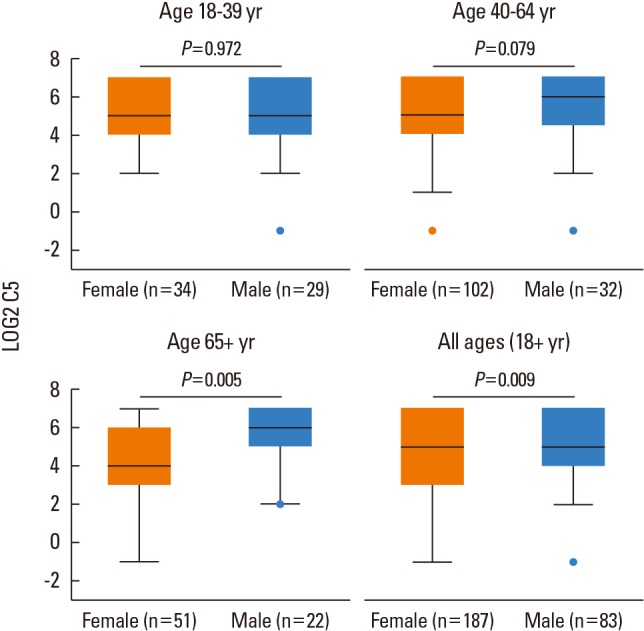
Box-and-whisker plots for capsaicin cough reflex sensitivity (C5) assessed in 270 chronic cough patients. Plots presented according to age groups. The box indicates the lower and upper quartile; central line, median value; and points at the end of the whiskers, upper extreme values. P values were determined by a Mann-Whitney test for a difference by gender.
Fig. 3.
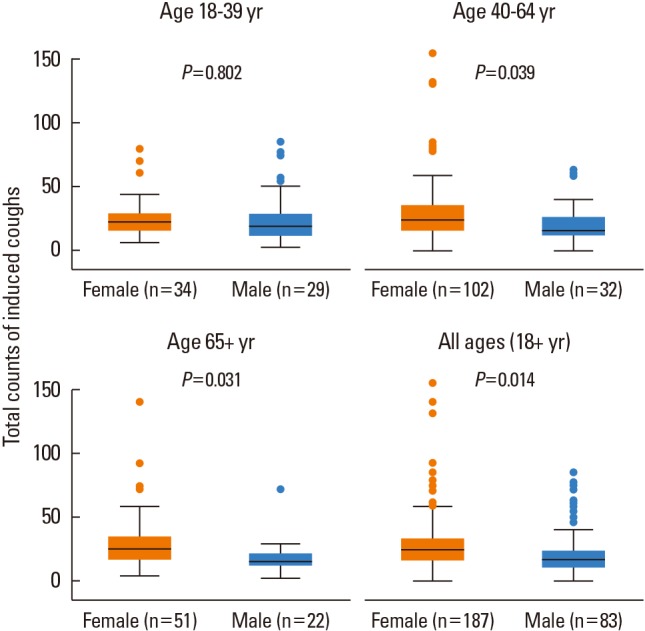
Box-and-whisker plots for total counts of capsaicin-induced coughs during the challenge. Plots presented according to age groups. Box indicates the lower and upper quartile; central line, median value; and points at the end of the whiskers, upper extreme values. P values were determined by a Mann-Whitney test for a difference by gender.
DISCUSSION
This study reports a middle-aged female predominance of adult chronic cough patients presented to a tertiary referral cough clinic in Korea. We found that capsaicin cough sensitivity was significantly related to the demographic features. In addition, allotussia or 'cough by cold air' was more frequent in older female patients.
The findings on age and gender distributions are consistent with previous results from European and American cough clinics.4,5,6,7,8,9,10 Epidemiologic data on community populations that encompass diverse age groups are limited; however, a recent Swedish community population survey supports the conclusions of cough clinics (subjects with cough; mean age 55.2 years and female 63.2%).23 The findings on age and gender distributions warrant further confirmation but the consistency in demographics has resulted in speculation by researchers on the presence of an intrinsic pathophysiology for chronic cough.
We found that female cough patients had a higher capsaicin cough sensitivity (in both of C5 and total counts of induced cough). The gender association for females and capsaicin response is a well-known finding in adults.5,11,12,13,14,15 Mechanistically, estrogen hormone is suggested as a link24 as it experimentally enhances the capsaicin sensing cough receptor, transient receptor potential vanilloid 1 (TRPV1).25,26 Capsaicin cough sensitivity is proven to be up-regulated among females after puberty.27 However, estrogen hypothesis could not explain the findings that chronic cough is prevalent among post-menopausal females. A large proportion of chronic idiopathic cough28 or ACE inhibitor cough29 were post-menopausal females.
Cough is a defensive reflex to clear harmful inhalational particles or prevent aspiration. The cough reflex is believed to be particularly developed in humans to prevent aspiration due to the evolutionary downward transition of the larynx to the esophageal opening for speech acquisition.30 It is speculated that pregnancy between the ages of 30 and 40 may promote the development of a cough reflex to prevent reflux and aspiration.31
The clinical relevance of enhanced capsaicin sensitivity is believed to be as follows. Airway TRPV1 is a channel predominantly located in the sensory nerves that can be activated by direct agonists such as heat, acid or capsaicin32; however, it is also activated and sensitized by indirect agonists such as endogenous bradykinins or prostaglandins.33 Local persistent inflammation (i.e., allergic airway inflammation) may result in the hypersensitization of TRPV1 receptors by an endogenous agonist release34; subsequently, any tussigen inhalation may cause an enhanced cough response (hypertussia) if the TRPV1 receptor is sensitized.35
With regards to capsaicin hypersensitivity, Japanese researchers have proposed a diagnostic term of 'atopic cough' for a subgroup of atopy patients and enhanced capsaicin cough sensitivity.36 It is uncertain if higher capsaicin sensitivity indicates the presence of 'atopic cough'37 in our study participants or rather represents an overall phenomenon of enhanced cough sensitivity for older females. Current literature is unclear on the presence of 'atopic cough'.37
Besides TRPV1, there are more sensory cough receptors functioning in the airways38 and the role of the transient receptor potential ankyrin 1 (TRPA1) channel has been highlighted in the pathogenesis of chronic cough.39,40 TRPA1 senses a variety of stimuli such as cold temperature, smoke, or irritants. In addition, nasal transient receptor potential menthol 8 channel is another recent finding on cough reflex modulation.38,41 Cough is a consequence of the interaction of various sensory afferent inputs known as 'cough plasticity'.38 Chronic cough is explained as a single disease entity with an intrinsic pathophysiology known as 'cough hypersensitivity syndrome'.4,42,43 It is a conceptual entity; however, the global consistency in demographic features (Alyn Morice et al. in submission) suggests the presence of an intrinsic pathophysiological mechanism. The findings on the significant correlation of capsaicin responses and demographic distributions suggested cough sensitivity for the pathogenesis of chronic cough. However, advances in cough reflex measuring methodology should further characterize the disease entity in regards to types of relevant sensory receptors.
The study questionnaire indicated that allotussia and laryngeal paresthesia were highly prevalent in chronic cough patients (more than 80%) and that allotussia was frequent in middle-aged or elderly female cough patients. The findings need careful interpretation as they were subjectively assessed by the presence of symptoms despite the prior utilization of definitions.22,44 However, the findings are of interest because sensory perception measurement outcomes could be considered as equally important to motor consequence (cough frequency) in cough research.45 The clinical relevance still needs further validation and some researchers suggest that capsaicin cough response (hypertussia) indicates a peripheral sensitization; however, allotussia or laryngeal paresthesia also reflects the central sensitization in the cough reflex.22,46 The findings on the high frequency of laryngeal paresthesia (86.8%) are in accordance to previous findings on refractory cough patients (94%)44 and suggest a potential role for central sensitization in chronic cough. The positive association between capsaicin cough responses and 'cough by cold air' can be explained by prior experimental findings that TRPA1 and TRPV1 are mostly co-expressed in sensory neurons.39
The present study has several limitations. It was a cross-sectional observational design and could not address causal relationships. The clinical relevance of enhanced capsaicin sensitivity among cough patients warrants longitudinal follow-up studies; in addition, it was conducted at a tertiary referral cough clinic and the external validity could be questioned. The lack of detailed information on socioeconomic factors is a limitation to the demographic findings.
Capsaicin sensitivity has a wide variability with overlaps between cough patients and healthy controls;47 subsequently, it may not have a discriminative power. However, a capsaicin test remains a valid tool for group level comparisons if the sample size is sufficient.5,11,12,13,14,15,31,35 Prior studies focused on relatively younger adult populations and none indicated a gender difference in the elderly7,13,14,15,16,17; subsequently, the present study is unique as we report on enhanced older female cough sensitivity. Studies by Kastelik et al.11 compared capsaicin cough sensitivity between pre-menopausal (<55 years, n=23) and post-menopausal women (≥55 years, n=37); however, their study had a small sample size and did not separately analyze the elderly group (≥65 years). Fujimura et al. reported a slightly higher capsaicin cough sensitivity in the post-menopausal than in the pre-menopausal healthy women (mean age: 50±7 years, total n=40); however, they did not include a sufficient elderly population.15
The validity of additional outcomes on the total number of induced coughs during capsaicin inhalation could be questionable. At present, the clinical value of C5 is now being challenged; subsequently, some researchers have tried modified outcomes in capsaicin cough testing such as 'total number of coughs after inhalation of specific concentration'35 or 'maximum cough response at specific concentration'.48 We exploratively measured the total count of induced coughs during inhalation as an additional outcome of the present study. We agree that further studies require additional validation. However, we believe that the definition has strength over C5 because it has no upper limit value (128 µM in the present study) and has less overlap between patient and control.
In conclusion, chronic cough patients referred to a cough clinic demonstrated a predominance of older females. Demographic features were significantly associated with an enhanced capsaicin cough response. Allotussia or 'cough induced by cold air' was also more frequent in female patients. Laryngeal paresthesia or allotussia was common and affected more than 80%-90% of chronic cough patients; subsequently, we suggest a role of cough reflex hypersensitivity in the pathophysiology of chronic cough in adults.
ACKNOWLEDGMENTS
This study was supported by a grant of Korea Healthcare technology R&D project, Ministry of Health & Welfare, Republic of Korea (A092076).
The authors would like to thank Professor Alyn Morice (University of Hull, Hull, UK) for his helpful suggestions and support. The authors also would like to thank Jung-Ah Lee, Jung-Eun Seo and Eun-Sook Koh (Seoul National University Hospital, Seoul, Korea) for their endless support in conducting the study.
Footnotes
There are no financial or other issues that might lead to conflict of interest.
Supplementary Material
Age and gender distribution in (A) the entire chronic cough adult population for the last 5 years (n=1,732) and (B) the entire hypertension adult patient population for 1 month (n=1,871).
References
- 1.Chung KF, Pavord ID. Prevalence, pathogenesis, and causes of chronic cough. Lancet. 2008;371:1364–1374. doi: 10.1016/S0140-6736(08)60595-4. [DOI] [PubMed] [Google Scholar]
- 2.Birring SS, Prudon B, Carr AJ, Singh SJ, Morgan MD, Pavord ID. Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ) Thorax. 2003;58:339–343. doi: 10.1136/thorax.58.4.339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.French CL, Irwin RS, Curley FJ, Krikorian CJ. Impact of chronic cough on quality of life. Arch Intern Med. 1998;158:1657–1661. doi: 10.1001/archinte.158.15.1657. [DOI] [PubMed] [Google Scholar]
- 4.Morice AH, Faruqi S, Wright CE, Thompson R, Bland JM. Cough hypersensitivity syndrome: a distinct clinical entity. Lung. 2011;189:73–79. doi: 10.1007/s00408-010-9272-1. [DOI] [PubMed] [Google Scholar]
- 5.Kelsall A, Decalmer S, McGuinness K, Woodcock A, Smith JA. Sex differences and predictors of objective cough frequency in chronic cough. Thorax. 2009;64:393–398. doi: 10.1136/thx.2008.106237. [DOI] [PubMed] [Google Scholar]
- 6.McGarvey LP, Heaney LG, Lawson JT, Johnston BT, Scally CM, Ennis M, Shepherd DR, MacMahon J. Evaluation and outcome of patients with chronic non-productive cough using a comprehensive diagnostic protocol. Thorax. 1998;53:738–743. doi: 10.1136/thx.53.9.738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mello CJ, Irwin RS, Curley FJ. Predictive values of the character, timing, and complications of chronic cough in diagnosing its cause. Arch Intern Med. 1996;156:997–1003. [PubMed] [Google Scholar]
- 8.French CT, Fletcher KE, Irwin RS. Gender differences in health-related quality of life in patients complaining of chronic cough. Chest. 2004;125:482–488. doi: 10.1378/chest.125.2.482. [DOI] [PubMed] [Google Scholar]
- 9.Kastelik JA, Aziz I, Ojoo JC, Thompson RH, Redington AE, Morice AH. Investigation and management of chronic cough using a probability-based algorithm. Eur Respir J. 2005;25:235–243. doi: 10.1183/09031936.05.00140803. [DOI] [PubMed] [Google Scholar]
- 10.Dicpinigaitis PV. Thoughts on one thousand chronic cough patients. Lung. 2012;190:593–596. doi: 10.1007/s00408-012-9420-x. [DOI] [PubMed] [Google Scholar]
- 11.Kastelik JA, Thompson RH, Aziz I, Ojoo JC, Redington AE, Morice AH. Sex-related differences in cough reflex sensitivity in patients with chronic cough. Am J Respir Crit Care Med. 2002;166:961–964. doi: 10.1164/rccm.2109061. [DOI] [PubMed] [Google Scholar]
- 12.Dicpinigaitis PV, Allusson VR, Baldanti A, Nalamati JR. Ethnic and gender differences in cough reflex sensitivity. Respiration. 2001;68:480–482. doi: 10.1159/000050554. [DOI] [PubMed] [Google Scholar]
- 13.Dicpinigaitis PV, Rauf K. The influence of gender on cough reflex sensitivity. Chest. 1998;113:1319–1321. doi: 10.1378/chest.113.5.1319. [DOI] [PubMed] [Google Scholar]
- 14.Nieto L, de Diego A, Perpiñá M, Compte L, Garrigues V, Martinez E, Ponce J. Cough reflex testing with inhaled capsaicin in the study of chronic cough. Respir Med. 2003;97:393–400. doi: 10.1053/rmed.2002.1460. [DOI] [PubMed] [Google Scholar]
- 15.Fujimura M, Kasahara K, Kamio Y, Naruse M, Hashimoto T, Matsuda T. Female gender as a determinant of cough threshold to inhaled capsaicin. Eur Respir J. 1996;9:1624–1626. doi: 10.1183/09031936.96.09081624. [DOI] [PubMed] [Google Scholar]
- 16.Fujimura M, Sakamoto S, Kamio Y, Matsuda T. Sex difference in the inhaled tartaric acid cough threshold in non-atopic healthy subjects. Thorax. 1990;45:633–634. doi: 10.1136/thx.45.8.633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chai H, Farr RS, Froehlich LA, Mathison DA, McLean JA, Rosenthal RR, Sheffer AL, Spector SL, Townley RG. Standardization of bronchial inhalation challenge procedures. J Allergy Clin Immunol. 1975;56:323–327. doi: 10.1016/0091-6749(75)90107-4. [DOI] [PubMed] [Google Scholar]
- 18.Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, MacIntyre NR, McKay RT, Wanger JS, Anderson SD, Cockcroft DW, Fish JE, Sterk PJ. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000;161:309–329. doi: 10.1164/ajrccm.161.1.ats11-99. [DOI] [PubMed] [Google Scholar]
- 19.Paggiaro PL, Chanez P, Holz O, Ind PW, Djukanović R, Maestrelli P, Sterk PJ. Sputum induction. Eur Respir J Suppl. 2002;37:3s–8s. doi: 10.1183/09031936.02.00000302. [DOI] [PubMed] [Google Scholar]
- 20.Park HW, Kim SH, Chang YS, Lee BJ, Min KU, Kim YY, Cho SH. Complementary roles of capsaicin cough sensitivity test and induced sputum test to methacholine bronchial provocation test in predicting response to inhaled corticosteroids in patients with chronic non-productive cough. Ann Allergy Asthma Immunol. 2007;98:533–539. doi: 10.1016/S1081-1206(10)60731-4. [DOI] [PubMed] [Google Scholar]
- 21.Mauger EA, Mauger DT, Fish JE, Chinchilli VM, Israel E Asthma Clinical Trials Network. Summarizing methacholine challenges in clinical research. Control Clin Trials. 2001;22:244S–251S. doi: 10.1016/s0197-2456(01)00159-3. [DOI] [PubMed] [Google Scholar]
- 22.Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet. 2012;380:1583–1589. doi: 10.1016/S0140-6736(12)60776-4. [DOI] [PubMed] [Google Scholar]
- 23.Bende M, Millqvist E. Prevalence of chronic cough in relation to upper and lower airway symptoms; the Skovde population-based study. Front Physiol. 2012;3:251. doi: 10.3389/fphys.2012.00251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patberg KW. The female preponderance to cough hypersensitivity syndrome: another clue pointing to the role of TRPV1 in cough. Lung. 2011;189:257–258. doi: 10.1007/s00408-011-9295-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yan T, Liu B, Du D, Eisenach JC, Tong C. Estrogen amplifies pain responses to uterine cervical distension in rats by altering transient receptor potential-1 function. Anesth Analg. 2007;104:1246–1250. doi: 10.1213/01.ane.0000263270.39480.a2. [DOI] [PubMed] [Google Scholar]
- 26.Peng HY, Huang PC, Liao JM, Tung KC, Lee SD, Cheng CL, Shyu JC, Lai CY, Chen GD, Lin TB. Estrous cycle variation of TRPV1-mediated cross-organ sensitization between uterus and NMDA-dependent pelvic-urethra reflex activity. Am J Physiol Endocrinol Metab. 2008;295:E559–E568. doi: 10.1152/ajpendo.90289.2008. [DOI] [PubMed] [Google Scholar]
- 27.Varechova S, Plevkova J, Hanacek J, Tatar M. Role of gender and pubertal stage on cough sensitivity in childhood and adolescence. J Physiol Pharmacol. 2008;59:719–726. [PubMed] [Google Scholar]
- 28.McGarvey LP. Does idiopathic cough exist? Lung. 2008;186(Suppl 1):S78–S81. doi: 10.1007/s00408-007-9048-4. [DOI] [PubMed] [Google Scholar]
- 29.Gibson GR. Enalapril-induced cough. Arch Intern Med. 1989;149:2701–2703. [PubMed] [Google Scholar]
- 30.Brooks SM. Perspective on the human cough reflex. Cough. 2011;7:10. doi: 10.1186/1745-9974-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Morice AH. Chronic cough hypersensitivity syndrome. Cough. 2013;9:14. doi: 10.1186/1745-9974-9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Adcock JJ. TRPV1 receptors in sensitisation of cough and pain reflexes. Pulm Pharmacol Ther. 2009;22:65–70. doi: 10.1016/j.pupt.2008.12.014. [DOI] [PubMed] [Google Scholar]
- 33.Belvisi MG, Barnes PJ. TRPV1 in the airways. In: Malmberg AB, Bley KR, editors. Turning up the heat on pain: TRPV1 receptors in pain and inflammation. Boston (MA): Springer; 2005. pp. 167–187. [Google Scholar]
- 34.Grace MS, Dubuis E, Birrell MA, Belvisi MG. Pre-clinical studies in cough research: Role of Transient Receptor Potential (TRP) channels. Pulm Pharmacol Ther. 2013;26:498–507. doi: 10.1016/j.pupt.2013.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ternesten-Hasseus E, Larsson C, Larsson S, Millqvist E. Capsaicin sensitivity in patients with chronic cough- results from a cross-sectional study. Cough. 2013;9:5. doi: 10.1186/1745-9974-9-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Fujimura M, Ogawa H, Nishizawa Y, Nishi K. Comparison of atopic cough with cough variant asthma: is atopic cough a precursor of asthma? Thorax. 2003;58:14–18. doi: 10.1136/thorax.58.1.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.McGarvey L, Morice AH. Atopic cough: little evidence to support a new clinical entity. Thorax. 2003;58:736–737. doi: 10.1136/thorax.58.8.736-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Plevkova J, Song WJ. Chronic cough in subjects with upper airway diseases - analysis of mechanisms and clinical applications. Asia Pac Allergy. 2013;3:127–135. doi: 10.5415/apallergy.2013.3.2.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Belvisi MG, Dubuis E, Birrell MA. Transient receptor potential A1 channels: insights into cough and airway inflammatory disease. Chest. 2011;140:1040–1047. doi: 10.1378/chest.10-3327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Birrell MA, Belvisi MG, Grace M, Sadofsky L, Faruqi S, Hele DJ, Maher SA, Freund-Michel V, Morice AH. TRPA1 agonists evoke coughing in guinea pig and human volunteers. Am J Respir Crit Care Med. 2009;180:1042–1047. doi: 10.1164/rccm.200905-0665OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Buday T, Brozmanova M, Biringerova Z, Gavliakova S, Poliacek I, Calkovsky V, Shetthalli MV, Plevkova J. Modulation of cough response by sensory inputs from the nose - role of trigeminal TRPA1 versus TRPM8 channels. Cough. 2012;8:11. doi: 10.1186/1745-9974-8-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Chung KF. Chronic 'cough hypersensitivity syndrome': a more precise label for chronic cough. Pulm Pharmacol Ther. 2011;24:267–271. doi: 10.1016/j.pupt.2011.01.012. [DOI] [PubMed] [Google Scholar]
- 43.Birring SS. Controversies in the evaluation and management of chronic cough. Am J Respir Crit Care Med. 2011;183:708–715. doi: 10.1164/rccm.201007-1017CI. [DOI] [PubMed] [Google Scholar]
- 44.Vertigan AE, Gibson PG. Chronic refractory cough as a sensory neuropathy: evidence from a reinterpretation of cough triggers. J Voice. 2011;25:596–601. doi: 10.1016/j.jvoice.2010.07.009. [DOI] [PubMed] [Google Scholar]
- 45.Chung KF, McGarvey L, Mazzone SB. Chronic cough as a neuropathic disorder. Lancet Respir Med. 2013;1:414–422. doi: 10.1016/S2213-2600(13)70043-2. [DOI] [PubMed] [Google Scholar]
- 46.O'Neill J, McMahon SB, Undem BJ. Chronic cough and pain: Janus faces in sensory neurobiology? Pulm Pharmacol Ther. 2013;26:476–485. doi: 10.1016/j.pupt.2013.06.010. [DOI] [PubMed] [Google Scholar]
- 47.Morice AH, Fontana GA, Belvisi MG, Birring SS, Chung KF, Dicpinigaitis PV, Kastelik JA, McGarvey LP, Smith JA, Tatar M, Widdicombe J European Respiratory Society (ERS) ERS guidelines on the assessment of cough. Eur Respir J. 2007;29:1256–1276. doi: 10.1183/09031936.00101006. [DOI] [PubMed] [Google Scholar]
- 48.Hilton EC, Baverel PG, Woodcock A, Van Der Graaf PH, Smith JA. Pharmacodynamic modeling of cough responses to capsaicin inhalation calls into question the utility of the C5 end point. J Allergy Clin Immunol. 2013;132:847–855.e1-5. doi: 10.1016/j.jaci.2013.04.042. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Age and gender distribution in (A) the entire chronic cough adult population for the last 5 years (n=1,732) and (B) the entire hypertension adult patient population for 1 month (n=1,871).