

Abstract
Objective:
This investigation examined patterns of heavy drinking among Black and White young adults from a person-centered perspective and linked family and individual factors in adolescence to young adult drinking patterns.
Method:
The analysis focuses on 331 10th-grade students (168 Whites, 163 Blacks; 51% males) who were followed into young adulthood (ages 20 and 22). Cluster analyses using heavy episodic drinking, drunkenness, and alcohol problems in young adulthood resulted in groups of drinkers with different patterns. Groups were examined across and within race. Associations between young adult drinking groups and adolescent family and individual factors were tested.
Results:
Groups followed well-established race differences, with Whites clustering into frequent drinking groups more than Blacks, and Blacks clustering into non–heavy drinking groups more than Whites. Further, Black heavy drinkers reported fewer alcohol problems than White counterparts. Parental monitoring, consistent discipline, ethnic identity, and delinquency were associated with adult heavy episodic drinking groups for both races. Monitoring and delinquency, along with parental norms, were associated with drunkenness groups for both races. However, race differences were observed for drunkenness clusters such that attachment was predictive for White clusters, and parental guidelines and discipline were predictive for Black clusters.
Conclusions:
Large race differences in heavy drinking at young adulthood were confirmed. Family dynamics in 10th grade were identified as important for the development of different drinking patterns in the early 20s, when many individuals have left home, which suggests a key target for substance use prevention programs.
Alcohol use, abuse, and dependence pose serious social, health, and economic consequences for individuals and communities (e.g., Rehm et al., 2009; World Health Organization, 2011). In particular, heavy episodic drinking (HED) can lead to negative outcomes such as risky behavior, poor health, and negative social sequelae (Courtney and Polich, 2009; Oesterle et al., 2004; Voas et al., 2012). HED is the consumption of at least four or five alcoholic beverages (depending on sex) on a single occasion, often with the intent of becoming intoxicated (Kandel, 1980; White, 1987).
In the United States, the use of alcohol is highest during young adulthood (ages 18–25; Chen et al., 2004; Substance Abuse and Mental Health Services Administration [SAMHSA] 2012a). Of note, nationally representative studies have consistently shown race differences in alcohol use in adolescence and young adulthood, with more Whites reporting HED than Blacks. For example, in 2012, the rate of high school seniors who reported heavy drinking was twice as high for White as Black students (25.7% vs. 11.3%; Johnston et al., 2013). In young adulthood, 46.1% of Whites reported HED compared with 26.9% of Blacks (SAMHSA, 2012b).
Given these large race differences, it is possible that young Blacks and Whites differ not only in prevalence rates but also in other aspects of their drinking, such as levels of negative consequences. Individual consequences can occur in various domains, including physical (e.g., withdrawal, blacking out), interpersonal (e.g., fights, avoidance by family), and social roles (e.g., missing work or school; White and Labouvie, 1989), and are only moderately correlated with drinking amounts (Larimer et al., 2004; Turner et al., 2000). Research on college populations has shown that Blacks incur fewer or the same alcohol-related consequences as Whites (e.g., Beckett et al., 2006; Clarke et al., 2013; Presley, 1996); however, it is unclear if this pattern is generalizable to non–college-attending youth.
Another aspect of drinking in young adulthood is one’s judgment of drunkenness. HED is a behavioral construct typically operationalized as consuming a specific number of drinks during a defined period. In contrast, reporting on one’s drunkenness requires judgments about the physiological and psychological experiences that typify “being drunk.” Although the two concepts are strongly associated, they do not perfectly overlap (Midanik, 1999), and given the paucity of studies examining race differences in perceptions of drunkenness (Humphrey et al., 1983), understanding this dimension of drinking may offer additional insights about race differences. If reports of drunkenness are informed by cultural norms (Midanik, 1999), and if norms against heavy drinking are stronger in Black than White communities (Wallace, 1998), it is possible that race differences in young adults’ subjective evaluations of drunkenness will be even greater than HED differences. However, stricter norms could lead to more reports of drunkenness because relatively mild indications of intoxication may be viewed as deviant.
The current analysis approaches the understanding of drinking from a person-centered perspective. Such an approach identifies qualitatively different groups of individuals who are distinguished by specific patterns of drinking-related behaviors. By identifying groups that display particularly problematic behavior (i.e., excessive drunkenness, consistent HED, alcohol problems), this approach can point to intervention targets and enhance prevention efforts.
We were interested in understanding whether there are groups of young adults with qualitatively different patterns of drinking behaviors and whether there are race differences in group membership that reflect more than simple differences in HED prevalence rates. That is, by including drunkenness and alcohol problems, we hope to shed light on additional similarities or differences in Black and White drinking patterns. Last, we examined whether early (i.e., adolescent) family and individual characteristics are associated with different patterns of drinking in young adulthood. We focused on factors that previous research has suggested may demonstrate race differences in mean levels or in their relationship to young adult drinking behavior.
Family factors
Parental supervision and monitoring (i.e., knowing where the child is, with whom, doing what) in adolescence has been shown to reduce young adult heavy drinking (Aquilino and Supple, 2001; Arria et al., 2008; Barnes et al., 2006; Guo et al., 2001; White et al., 2006). Likewise, the relationship between parental alcohol consumption and increased young adult problem use is robust (Alati et al., 2005; Chassin et al., 2002, 2004; King and Chassin, 2007; Merline et al., 2008). The research on other family factors in adolescence—such as norms for substance use, closeness or bonding with parents, and consistent discipline—is mixed (Aquilino and Supple, 2001; Barnes et al., 2006; Guo et al., 2001; Locke and Newcomb, 2004; Maggs et al., 1997; Roche et al., 2008; Varvil-Weld et al., 2012). Some studies have found that these factors decrease young adults’ drinking, and others did not find any effect. Of interest, studies have found that Black more than White families display many factors associated with lower substance use in youth, including parental guidelines for substance use, monitoring, norms against substance use, strict discipline, and lower parental alcohol use (Catalano et al., 1992; Gillmore et al., 1990; Giordano et al., 1993; Peterson et al., 1994; Wallace and Muroff, 2002). It is also possible that Black adolescents are more attached to their parents than are Whites (Giordano et al., 1993; although Catalano et al., 1992, found no race difference).
Individual factors
Several individual characteristics may differentially predict drinking patterns in Blacks and Whites. For example, adolescent religiosity is related to less alcohol consumption (Rostosky et al., 2007; White et al., 2006; Windle et al., 2005). Black youth generally report greater religiosity and are more likely to belong to conservative Protestant denominations than Whites (Wallace et al., 2003a). Exposure to strong anti-alcohol values and norms may translate into a more central role of religion for Blacks’ drinking patterns versus Whites’. Similarly, ethnic identity, the exploration and affirmation of one’s belonging to an ethnic group, in adolescence is related to lower substance use in young adulthood (Brook and Pahl, 2005; Brook et al., 1998). Given that identification with being African American is likely related to adoption of cultural norms that include less frequent drinking at young ages (Wallace, 1998) and less acceptance of drunkenness (Greenfield and Room, 1997), ethnic identity may serve as a more important predictor of drinking patterns for Blacks than Whites. Last, delinquency is a predictor of more substance use (Harford and Muthén, 2000; Mason et al., 2010; Wiesner et al., 2005; Zucker, 2008), but among Blacks the connection may not be very strong given low rates of alcohol use and equal or higher rates of delinquency (Hawkins et al., 2000). Given the relative paucity of literature on drinking patterns among Black and White young adults, we view this study as exploratory in nature and have not put forth specific hypotheses for drinking groups or associations with family (parental monitoring, attachment, norms and guidelines about alcohol use, and consistent discipline) or individual factors (religious conservatism, ethnic identity exploration and affirmation, and delinquent behavior).
Method
Sample
Participants were part of an experimental test of the prevention program Staying Connected to Your Teen, delivered in the eighth grade (for program details, see Haggerty et al., 2007). The current analysis includes participants from both the treatment and control groups approximately 7 and 9 years after treatment. Black and White eighth-grade students and their parents were recruited from the Seattle Public Schools, and 46% consented to participate with their parents (55% Black, 40% White). After we stratified the adolescent sample by race and gender, participants were randomized into treatment groups. Assessments used here were conducted in the 10th grade and at ages 20 and 22. All study protocols were approved by the University of Washington Institutional Review Board.
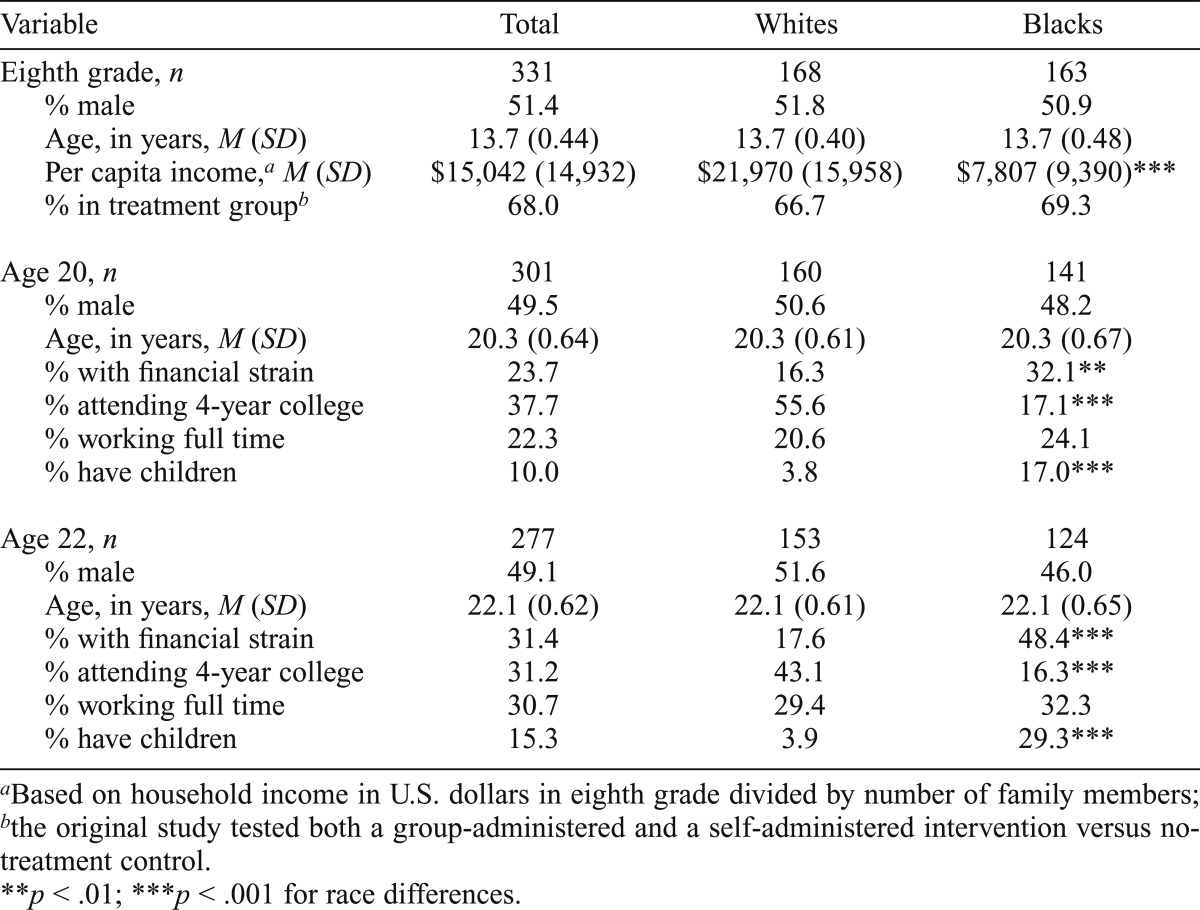
Table 1 provides demographic information for the 163 Black and 168 White participants. Consistent with their respective populations in Seattle, large race differences in socioeconomic variables, such as income, t(324) = 12.04, p < .001, were found. In young adulthood, Blacks continued to experience greater financial strain, age 20: χ2(1, 300) = 10.44, p = .001, age 22: χ2(1, 277) = 30.04, p < .001; were more likely to have children, age 20: χ2(1, 300) = 14.57, p < .001, age 22: χ2(1, 275) = 30.04, p < .001; and were less likely to attend a 4-year college than Whites, age 20: χ2(1, 300) = 47.09, p < .001, age 22: χ2(1, 276) = 22.96, p < .001. Because this sample consists of two thirds nonstudents, the findings generalize to more than college populations, which have been the focus of the literature to date. Furthermore, this sample, which contains both Black and White students and nonstudents, allows us to examine whether higher rates of college attendance among Whites may account for race differences in drinking behavior. College attendance is associated with heavy drinking (White et al., 2006), presumably because of greater access to alcohol and social acceptability of drinking (White et al., 2008).
Table 1.
Sample characteristics by race
| Variable | Total | Whites | Blacks |
| Eighth grade, n | 331 | 168 | 163 |
| % male | 51.4 | 51.8 | 50.9 |
| Age, in years, M (SD) | 13.7 (0.44) | 13.7 (0.40) | 13.7 (0.48) |
| Per capita income,a M (SD) | $15,042 (14,932) | $21,970 (15,958) | $7,807 (9,390)*** |
| % in treatment groupb | 68.0 | 66.7 | 69.3 |
| Age 20, n | 301 | 160 | 141 |
| % male | 49.5 | 50.6 | 48.2 |
| Age, in years, M (SD) | 20.3 (0.64) | 20.3 (0.61) | 20.3 (0.67) |
| % with financial strain | 23.7 | 16.3 | 32.1** |
| % attending 4-year college | 37.7 | 55.6 | 17.1*** |
| % working full time | 22.3 | 20.6 | 24.1 |
| % have children | 10.0 | 3.8 | 17.0*** |
| Age 22, n | 277 | 153 | 124 |
| % male | 49.1 | 51.6 | 46.0 |
| Age, in years, M (SD) | 22.1 (0.62) | 22.1 (0.61) | 22.1 (0.65) |
| % with financial strain | 31.4 | 17.6 | 48.4*** |
| % attending 4-year college | 31.2 | 43.1 | 16.3*** |
| % working full time | 30.7 | 29.4 | 32.3 |
| % have children | 15.3 | 3.9 | 29.3*** |
Based on household income in U.S. dollars in eighth grade divided by number of family members;
the original study tested both a group-administered and a self-administered intervention versus no-treatment control.
p < .01;
p < .001 for race differences.
Although overall attrition during various assessment periods was relatively low, the losses were not equivalent by race: age 20 loss for Whites 5% versus Blacks 13%, χ2(1, 301) = 7.66, p < .01; age 22 Whites 9% versus Blacks 24%, χ2(l, 277) = 13.63, p < .001. Furthermore, attrition was more likely among males, at age 20, χ2(1, 331) = 4.59, p < .05, and those with lower per capita incomes, age 20: t(324) = -2.84, p < .01; age 22: t(324) = -3.78, p < .001. To reduce bias because of attrition, we used instrumental variables (earlier measures of drinking, deviant behavior) in a multiple imputation model (Graham, 2012), imputing 100 data sets.
Measures
Race of participants was determined based on parental identification of the student’s race for school enrollment. College attendance was coded as dichotomous based on participants’ reports of current attendance in a 4-year institution at ages 20 and 22.
Heavy episodic drinking (ages 20 and 22) was defined as consuming at least four (females) or five (males) drinks in one occasion during the past 2 weeks (Wechsler et al., 1995). Participants who self-reported any HED during the past 2 weeks were considered heavy episodic drinkers.
Alcohol-related problems or consequences (ages 20 and 22) were measured using the Rutgers Alcohol Problem Index (White and Labouvie, 1989), which assesses physical (e.g., withdrawal symptoms), interpersonal (e.g., hurt relationships with friends and family), and social role (e.g., avoided responsibilities) consequences of heavy drinking on a 5-point scale (from never to more than 10 times in the past year). The final score, based on the sum of 14 items (age 20, α = .87; age 22, α = .89), reflects both the frequency (repetition) and diversity (different types) of consequences.
Drunkenness (ages 20 and 22) was based on one self-report item measuring the frequency of “getting drunk.” Responses were on a 7-point scale from never to once a day, with higher scores representing more frequent drunkenness.
Family variables (10th grade; mean age = 16.1 years).
Parental monitoring was calculated as the mean of seven items (α = .81) reflecting adolescents’ perceptions of general parental supervision and knowledge of their activities (e.g., “Do your parents know what you do with your friends?”). Responses to all items were coded on a 4-point scale (YES, yes, no, NO). Attachment to parents was measured as the sum of adolescents’ responses to 28 items (α = .95) from the Inventory of Parent and Peer Attachment (Armsden and Greenberg, 1987). Parental norms were based on one item assessing adolescents’ beliefs about whether their parents think it is okay for them to drink alcohol regularly. On the “YES, yes, no, NO” scale, only “NO” responses indicated a strong norm against regular alcohol consumption and were coded 1 (otherwise coded 0). Parental guidelines were assessed with the mean of eight items (α = .80) that measure parental agreement on a 4-point scale with statements about rules and consequences of substance use (e.g., “I have clear and specific rules about my teen’s use of tobacco, alcohol, and illegal drugs”). Consistent discipline was assessed by the mean of seven items (α = .77) indicating parental responses to questions such as, “How often do you and your spouse/partner disagree about the rules for your child?” Higher scores reflect more consistent discipline. Parental alcohol use was coded as present (1) if a primary caregiver reported drinking any alcohol during the past month (otherwise coded 0).
Individual variables (10th grade).
Religious conservatism was measured based on the extensive work done in this area by Wallace et al. (2003b) while adjusting for the level of exposure to conservative religious doctrine. Religious affiliation (e.g., Catholic, Methodist) was rated on a 4-point scale (Wallace et al., 2003b). Individuals who endorsed the most conservative religious affiliations were further stratified. Those with at least weekly attendance received a higher rating; thus, higher scores reflect more conservative religiosity. Ethnic identity was assessed using two subscales of the self-report Multigroup Ethnic Identity Measure: exploration (four items, α = .71), and affirmation, belonging, and commitment (“affirmation”; six items, α = .90). Adapting the work of Roberts et al. (1999), response options were on the “YES, yes, no, NO” scale and were averaged. Higher scores indicate greater identification with one’s ethnic group or greater exploration of one’s ethnic group. Self-reported delinquency was calculated as the total count of 12 behaviors in the past year (α = .77), including violent (e.g., hit someone) and nonviolent (e.g., theft) acts but not substance-related behavior.
Analytic strategy
After confirming that more Whites in this sample reported heavy drinking than did Blacks, we conducted two-step agglomerative hierarchical cluster analyses using SPSS (Version 19), which allowed for both categorical and continuous clustering variables. Clustering variables were the three measures of drinking behavior: HED, alcohol problems, and drunkenness. In the current sample, HED and drunkenness were highly correlated (age 20, r = .69; age 22, r = .59). When two (or more) clustering variables are highly correlated, they become disproportionately weighted in the analysis and can bias the resulting groups. Thus, we conducted analyses using (a) HED and alcohol problems and (b) drunkenness and alcohol problems as clustering variables in separate analyses.
Cluster analyses were conducted in two phases. Blacks and Whites were analyzed together to explore groups of individuals with unique drinking behaviors that may not necessarily align with race differences in HED rates. Next, the sample was divided by race, and cluster analyses were conducted separately to explore whether different patterns of drinking behavior would emerge for Blacks and Whites.
Because we did not have specific hypotheses about the number of resulting clusters, we used the auto-clustering function, which returns an optimal solution based on the Bayesian information criterion and distance change for each additional cluster in a solution (SPSS, 2001). After determining a solution, SPSS produces a silhouette measure of cluster cohesion and separation, which is a goodness-of-fit statistic that takes into account the distances between each observation and its cluster center, as well as other cluster centers (Mooi and Sarstedt, 2011; SPSS, 2001). It reveals how much overlap exists among the clusters (too much overlap suggests that clusters are not distinct); solution quality is then rated as “good,” “fair,” or “poor” (based on Kaufman and Rousseeuw’s [1990] criteria).
After a cluster solution is derived, relationships between external or validation variables and cluster membership are often tested to ascertain whether the clusters are meaningful and to shed light on associations of interest (Aldenderfer and Blashfield, 1984). We tested the association between membership in drinking clusters in young adulthood and family and individual factors measured in adolescence using analyses of variance and chi-square. If significant, post hoc analyses identified which groups were higher or lower than all other groups combined.
Because some participants received a substance use prevention program and others did not, we examined the relationship between intervention group and drinking cluster membership across and within race and found that none was significant. Likewise, because of the large income disparity by race, we examined the relationship between income and cluster membership across and within race. Differences were detected in mean income between clusters across the full sample, consistent with the race makeup of the clusters (and race differences in HED prevalence). However, no significant relationship was found between income and cluster membership when examined within each race group. Given this pattern of results, we did not control for intervention assignment or income in post hoc analyses of relationships between cluster membership and family and individual factors.
Results
Race differences in rates of drinking behavior
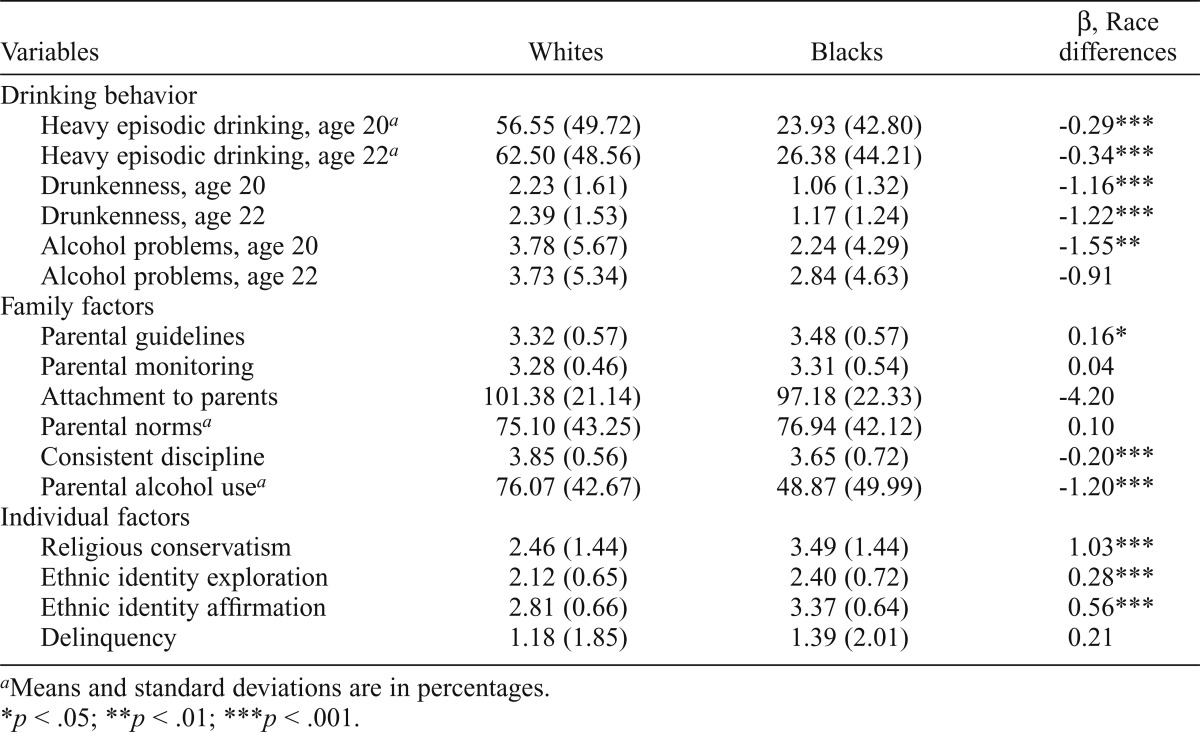
Table 2 displays the rates of HED among Whites and Blacks as well as descriptive information on family and individual factors. Consistent with past research, Whites in this sample reported much higher rates of HED than did Blacks at both ages. Frequency of drunkenness follows a similar race pattern, but there were no significant differences in alcohol problems between Blacks and Whites at age 22. As expected, some race differences emerged in family and individual factors. Blacks had lower scores on parental drinking and consistent discipline and higher scores on conservative religiosity and both ethnic identity factors than did Whites.
Table 2.
Means (SD) by race with tests of differences in clustering and validation variables
| Variables | Whites | Blacks | β, Race differences |
| Drinking behavior | |||
| Heavy episodic drinking, age 20a | 56.55 (49.72) | 23.93 (42.80) | -0.29*** |
| Heavy episodic drinking, age 22a | 62.50 (48.56) | 26.38 (44.21) | -0.34*** |
| Drunkenness, age 20 | 2.23 (1.61) | 1.06 (1.32) | -1.16*** |
| Drunkenness, age 22 | 2.39 (1.53) | 1.17 (1.24) | -1. 22*** |
| Alcohol problems, age 20 | 3.78 (5.67) | 2.24 (4.29) | -1.55** |
| Alcohol problems, age 22 | 3.73 (5.34) | 2.84 (4.63) | -0.91 |
| Family factors | |||
| Parental guidelines | 3.32 (0.57) | 3.48 (0.57) | 0.16* |
| Parental monitoring | 3.28 (0.46) | 3.31 (0.54) | 0.04 |
| Attachment to parents | 101.38 (21.14) | 97.18 (22.33) | -4.20 |
| Parental normsa | 75.10 (43.25) | 76.94 (42.12) | 0.10 |
| Consistent discipline | 3.85 (0.56) | 3.65 (0.72) | -0.20*** |
| Parental alcohol usea | 76.07 (42.67) | 48.87 (49.99) | -1.20*** |
| Individual factors | |||
| Religious conservatism | 2.46 (1.44) | 3.49 (1.44) | 1.03*** |
| Ethnic identity exploration | 2.12 (0.65) | 2.40 (0.72) | 0.28*** |
| Ethnic identity affirmation | 2.81 (0.66) | 3.37 (0.64) | 0.56*** |
| Delinquency | 1.18 (1.85) | 1.39 (2.01) | 0.21 |
Means and standard deviations are in percentages.
p < .05;
p < .01;
p < .001.
Cluster analyses with heavy episodic drinking
Full sample analyses.
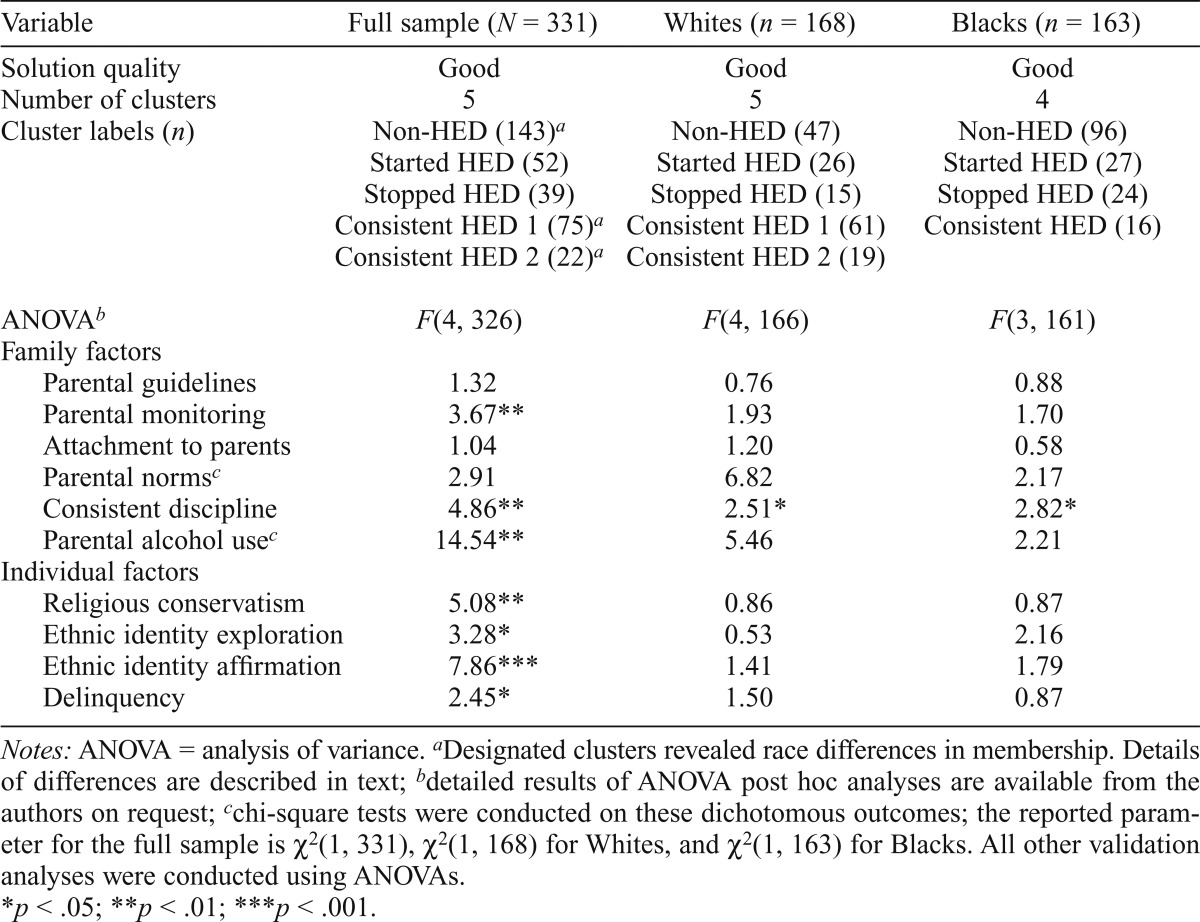
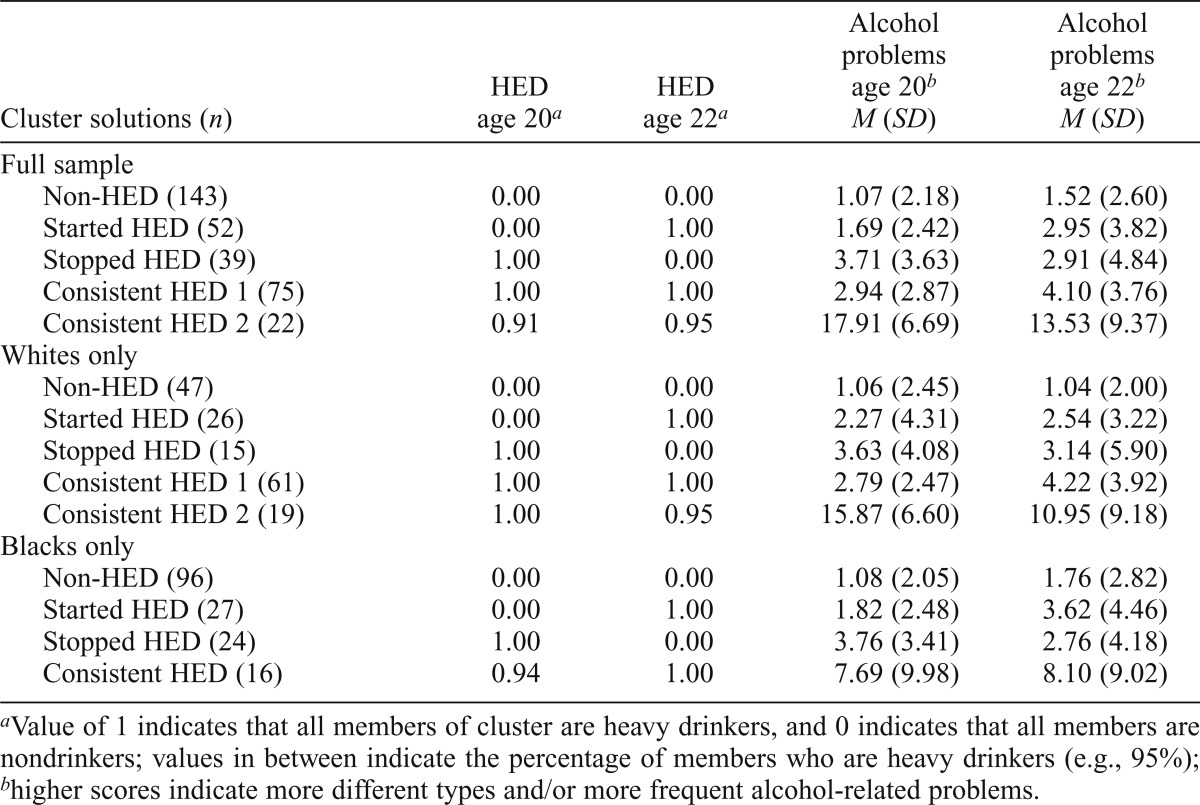
As noted earlier, we conducted two sets of cluster analyses. The first included HED and alcohol problems at ages 20 and 22 as the four clustering variables. On the full sample, the optimal solution, rated as “good” quality, contained five clusters (Table 3). The clusters were labeled to reflect the drinking behavior of their members across the two periods. For example, “Started HED” was predominantly composed of individuals who were not heavy drinkers at age 20 but were at age 22. Mean levels of alcohol problems for each cluster generally corresponded to the cluster’s average HED behavior (e.g., the Non-HED group displayed the lowest levels of problems). However, the two clusters with consistent HED behavior were differentiated by the level of alcohol problems: The Consistent HED 1 group, the larger group, had considerably fewer problems relative to the Consistent HED 2 group. Table 4 displays the mean values of each cluster on the clustering variables.
Table 3.
Cluster analyses based on heavy episodic drinking (HED) and alcohol problems at ages 20 and 22
| Variable | Full sample (N = 331) | Whites (n = 168) | Blacks (n = 163) |
| Solution quality | Good | Good | Good |
| Number of clusters | 5 | 5 | 4 |
| Cluster labels (n) | Non-HED (143)a | Non-HED (47) | Non-HED (96) |
| Started HED (52) | Started HED (26) | Started HED (27) | |
| Stopped HED (39) | Stopped HED (15) | Stopped HED (24) | |
| Consistent HED 1 (75)a | Consistent HED 1 (61) | Consistent HED (16) | |
| Consistent HED 2 (22)a | Consistent HED 2 (19) | ||
| ANOVAb | F(4, 326) | F(4, 166) | F(3, 161) |
| Family factors | |||
| Parental guidelines | 1.32 | 0.76 | 0.88 |
| Parental monitoring | 3.67** | 1.93 | 1.70 |
| Attachment to parents | 1.04 | 1.20 | 0.58 |
| Parental normsc | 2.91 | 6.82 | 2.17 |
| Consistent discipline | 4.86** | 2.51* | 2.82* |
| Parental alcohol usec | 14.54** | 5.46 | 2.21 |
| Individual factors | |||
| Religious conservatism | 5.08** | 0.86 | 0.87 |
| Ethnic identity exploration | 3.28* | 0.53 | 2.16 |
| Ethnic identity affirmation | 7.86*** | 1.41 | 1.79 |
| Delinquency | 2.45* | 1.50 | 0.87 |
Notes: ANOVA = analysis of variance.
Designated clusters revealed race differences in membership. Details of differences are described in text;
detailed results of ANOVA post hoc analyses are available from the authors on request;
chi-square tests were conducted on these dichotomous outcomes; the reported parameter for the full sample is χ2(l, 331), χ2(l, 168) for Whites, and χ2(1, 163) for Blacks. All other validation analyses were conducted using ANOVAs.
p < .05;
p < .01;
p < .001.
Table 4.
Mean values of clusters from analyses with heavy episodic drinking (HED) and alcohol problems
| Cluster solutions (n) | HED age 20a | HED age 22a | Alcohol problems age 20b M (SD) | Alcohol problems age 22b M (SD) |
| Full sample | ||||
| Non-HED (143) | 0.00 | 0.00 | 1.07 (2.18) | 1.52 (2.60) |
| Started HED (52) | 0.00 | 1.00 | 1.69 (2.42) | 2.95 (3.82) |
| Stopped HED (39) | 1.00 | 0.00 | 3.71 (3.63) | 2.91 (4.84) |
| Consistent HED 1 (75) | 1.00 | 1.00 | 2.94 (2.87) | 4.10 (3.76) |
| Consistent HED 2 (22) | 0.91 | 0.95 | 17.91 (6.69) | 13.53 (9.37) |
| Whites only | ||||
| Non-HED (47) | 0.00 | 0.00 | 1.06 (2.45) | 1.04 (2.00) |
| Started HED (26) | 0.00 | 1.00 | 2.27 (4.31) | 2.54 (3.22) |
| Stopped HED (15) | 1.00 | 0.00 | 3.63 (4.08) | 3.14 (5.90) |
| Consistent HED 1 (61) | 1.00 | 1.00 | 2.79 (2.47) | 4.22 (3.92) |
| Consistent HED 2 (19) | 1.00 | 0.95 | 15.87 (6.60) | 10.95 (9.18) |
| Blacks only | ||||
| Non-HED (96) | 0.00 | 0.00 | 1.08 (2.05) | 1.76 (2.82) |
| Started HED (27) | 0.00 | 1.00 | 1.82 (2.48) | 3.62 (4.46) |
| Stopped HED (24) | 1.00 | 0.00 | 3.76 (3.41) | 2.76 (4.18) |
| Consistent HED (16) | 0.94 | 1.00 | 7.69 (9.98) | 8.10 (9.02) |
Value of 1 indicates that all members of cluster are heavy drinkers, and 0 indicates that all members are nondrinkers; values in between indicate the percentage of members who are heavy drinkers (e.g., 95%);
higher scores indicate more different types and/or more frequent alcohol-related problems.
Chi-square tests indicated that the clusters differed by race. The Consistent HED 1 and HED 2 groups contained more Whites than did other clusters, χ2(1, 331) = 50.04, p < .001; χ2(l, 331) = 4.55, p < .05, respectively, and the Non-HED group contained more Blacks than other clusters, χ2(1, 331) = 32.23, p < .001. This finding is consistent with higher rates of White than Black drinking.
We compared the five clusters on early family and individual factors (Table 3). The clusters differ on 10th-grade parental monitoring, discipline, parental alcohol use, religious conservatism, ethnic identity exploration and affirmation, and delinquency. Post hoc results indicated that the Non-HED group was higher than others on monitoring, and the Consistent HED 2 group was lower on monitoring. The Started HED group was higher than others on consistent discipline, whereas the Stopped HED group was lower on discipline. The Consistent HED 1 cluster (predominantly White) had higher parental alcohol use, whereas the Non-HED cluster (predominantly Black) had lower parental use.
The Consistent HED 1 cluster (predominantly White) had lower religious conservatism, whereas the Non-HED cluster (predominantly Black) had higher religious conservatism. Furthermore, youth in the Stopped HED group were higher than others on ethnic identity exploration and affirmation (along with the Non-HED group for the latter). The Consistent HED 2 group was higher on delinquency than others.
Analyses by race.
The analysis with Whites yielded five clusters that were similar to those in the full sample (Table 3). The analysis with Blacks yielded four clusters with only one small Consistent HED group. Despite good-quality solutions in both cases, only consistent parental discipline differentiated among clusters for both Whites, F(4, 163) = 2.51, p < .05, and Blacks, F(3, 159) = 2.82, p < .05. However, the results were different by race. For Whites, individuals in the Started HED and Consistent HED 2 groups had higher levels of parental discipline than other White clusters. For Blacks, individuals in the Stopped HED group had lower scores on discipline than other Black clusters.
Cluster analyses with drunkenness
Full sample analyses.
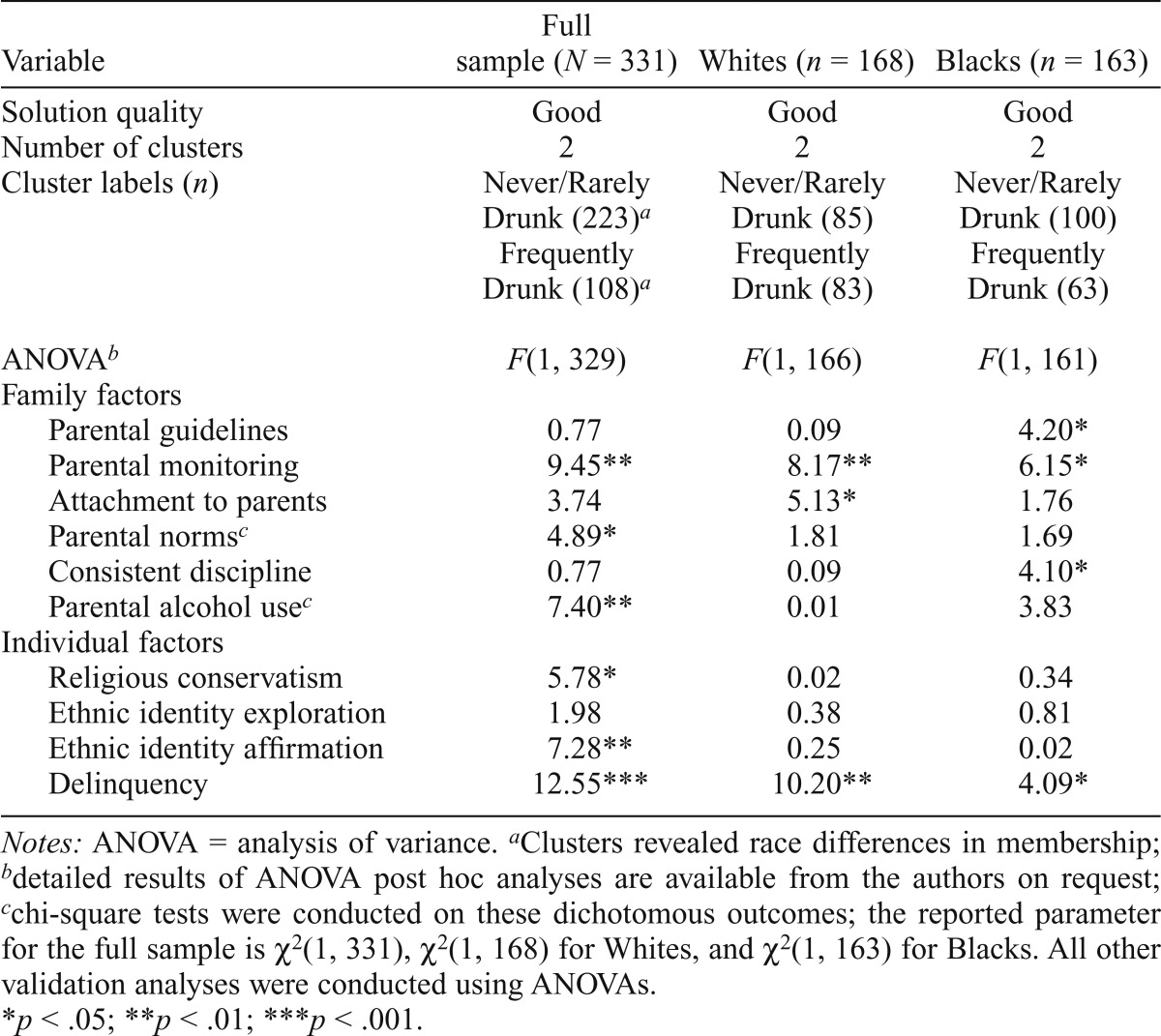
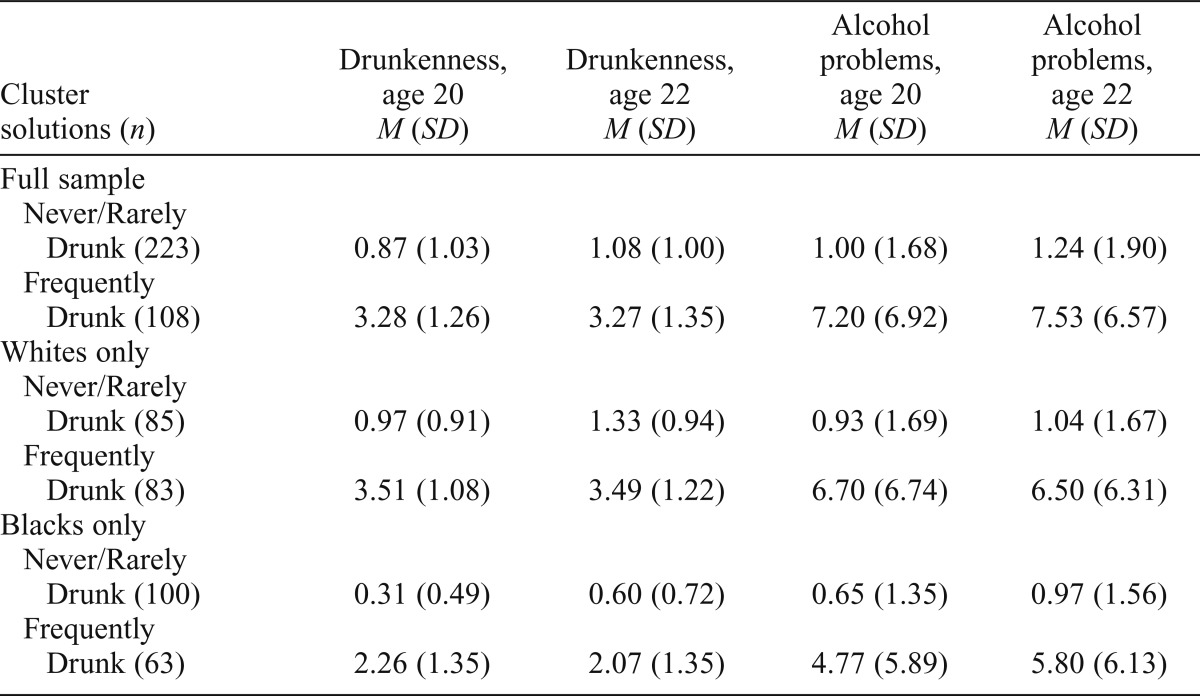
The four clustering variables included drunkenness and alcohol problems at ages 20 and 22. The optimal solution for the full sample showed “good” quality and produced two clusters: Frequently Drunk (n = 108) and Never or Rarely Drunk (n = 223; Table 5). Participants in the Frequently Drunk cluster reported greater frequency of drunkenness at both ages, as well as much higher levels of alcohol problems at both times (Table 6).
Table 5.
Cluster analyses based on drunkenness and alcohol problems at ages 20 and 22
| Variable | Full sample (N = 331) | Whites (n = 168) | Blacks (n = 163) |
| Solution quality | Good | Good | Good |
| Number of clusters | 2 | 2 | 2 |
| Cluster labels (n) | Never/Rarely Drunk (223)a | Never/Rarely Drunk (85) | Never/Rarely Drunk (100) |
| Frequently Drunk (108)a | Frequently Drunk (83) | Frequently Drunk (63) | |
| ANOVAb | F(1, 329) | F(1, 166) | F(1, 161) |
| Family factors | |||
| Parental guidelines | 0.77 | 0.09 | 4.20* |
| Parental monitoring | 9.45** | 8.17** | 6.15* |
| Attachment to parents | 3.74 | 5.13* | 1.76 |
| Parental normsc | 4.89* | 1.81 | 1.69 |
| Consistent discipline | 0.77 | 0.09 | 4.10* |
| Parental alcohol usec | 7.40** | 0.01 | 3.83 |
| Individual factors | |||
| Religious conservatism | 5.78* | 0.02 | 0.34 |
| Ethnic identity exploration | 1.98 | 0.38 | 0.81 |
| Ethnic identity affirmation | 7.28** | 0.25 | 0.02 |
| Delinquency | 12.55*** | 10.20** | 4.09* |
Notes: ANOVA = analysis of variance.
Clusters revealed race differences in membership;
detailed results of ANOVA post hoc analyses are available from the authors on request;
chi-square tests were conducted on these dichotomous outcomes; the reported parameter for the full sample is χ2(1, 331), χ2(1, 168) for Whites, and χ2(1, 163) for Blacks. All other validation analyses were conducted using ANOVAs.
p < .05;
p < .01;
p < .001.
Table 6.
Mean values of clusters from analyses with drunkenness and alcohol problems
| Cluster solutions (n) | Drunkenness, age 20 M (SD) | Drunkenness, age 22 M (SD) | Alcohol problems, age 20 M (SD) | Alcohol Problems, age 22 M (SD) |
| Full sample | ||||
| Never/Rarely Drunk (223) | 0.87 (1.03) | 1.08 (1.00) | 1.00 (1.68) | 1.24 (1.90) |
| Frequently Drunk (108) | 3.28 (1.26) | 3.27 (1.35) | 7.20 (6.92) | 7.53 (6.57) |
| Whites only | ||||
| Never/Rarely Drunk (85) | 0.97 (0.91) | 1.33 (0.94) | 0.93 (1.69) | 1.04 (1.67) |
| Frequently Drunk (83) | 3.51 (1.08) | 3.49 (1.22) | 6.70 (6.74) | 6.50 (6.31) |
| Blacks only | ||||
| Never/Rarely Drunk (100) | 0.31 (0.49) | 0.60 (0.72) | 0.65 (1.35) | 0.97 (1.56) |
| Frequently Drunk (63) | 2.26 (1.35) | 2.07 (1.35) | 4.77 (5.89) | 5.80 (6.13) |
Association of the cluster solution with early family and individual factors is presented in Table 5. Clusters differed by six variables: post hoc analyses revealed that the Never or Rarely Drunk cluster had more parental monitoring, stricter norms, less parental alcohol use, greater religious conservatism, higher ethnic identity affirmation, and less delinquency in adolescence. Race differed significantly by cluster, χ2(1, 331) = 24.68, p < .001, indicating that drunkenness clusters are consistent with higher rates of heavy drinking by Whites. The cluster differences in parental alcohol use, religious conservatism, and ethnic identity affirmation are consistent with race differences in these variables, which suggests that these cluster differences may be attributable to the race makeup of the groups.
Analyses by race.
Two similar clusters emerged for Blacks and Whites separately (Table 5). For Blacks, the Frequently Drunk cluster includes 39% of the sample, whereas the corresponding cluster for Whites includes 49% of that sample. Small clusters often indicate an extreme or deviant group, but the small number of Blacks in the Frequently Drunk cluster report lower drunkenness and alcohol problems scores than does the larger corresponding cluster for Whites (Table 6).
Early parental monitoring and delinquency were associated with cluster membership for both Blacks and Whites (greater monitoring and less delinquency were associated with less frequent drunkenness). In addition, within-race analyses revealed different relationships between family factors and cluster membership. Attachment to parents is significantly higher in the Never/Rarely Drunk cluster than in the Frequently Drunk cluster among Whites but not Blacks. Alternately, parental guidelines and consistent discipline are significantly higher in the Never/Rarely Drunk cluster than the Frequently Drunk cluster for Blacks but not Whites.
Clusters and college attendance
It is possible that race differences in drinking clusters are primarily attributable to race differences in college attendance; thus, relationships between college attendance at ages 20 and 22 (two variables) and cluster solutions were tested. For the HED clusters, chi-squares were significant, age 20: χ2(1, 331) = 23.72, p < .001; age 22: χ2(1, 331) = 17.52, p < .01, and consistent with race differences in cluster membership (e.g., at both ages, there were more college students in the Consistent HED 1 cluster [predominantly White] and fewer students in the Non-HED cluster [predominantly Black]). This pattern suggests that race differences in drinking may be explained by college attendance. However, when analyzed separately by race, college attendance was not associated with HED cluster [Whites age 20 χ2(1, attendance: χ2(1, 168) = 5.26, p = .26; age 22: χ2(1, 168) = 6.22, p = .18; Blacks age 20 attendance: χ2(1, 163) = 2.08, p = .56; age 22: χ2(1, 163) = 3.87, p = .28]. For the drunkenness clusters, the chi-square analyses were nonsignificant (age 20, p = .44; age 22, p = .80), indicating that college attendance is unrelated to belonging in the Frequently Drunk cluster.
Discussion
As expected, young Blacks engaged in significantly less heavy drinking than did young Whites. In our sample, there were far fewer Blacks than Whites who were classified as consistent heavy episodic drinkers in young adulthood and far more Blacks than Whites who were consistent non–heavy drinkers. Similarly, more Whites than Blacks reported a pattern of frequent drunkenness.
The inclusion of alcohol problems as a defining characteristic of drinking patterns provided additional information. Black young adults generally belonged to clusters in which alcohol problems were minimal; however, even those Blacks who were heavier drinkers reported fewer alcohol problems than their White counterparts. This finding extends previous work with students to a more general population. We note, however, that the negative consequences measured here do not include aspects such as involvement with the legal system (e.g., arrests), serious morbidity (e.g., cirrhosis of the liver), and mortality, which are problems that disproportionately affect Blacks (Beckett et al., 2006; Chartier and Caetano, 2010; Galea and Vlahov, 2002; Gary, 1986; Herd, 1985).
Our analyses identified one group of very high-risk White young adults who engage in extensive heavy drinking and experience especially serious negative consequences. This group is similar to the high-risk college students, identified by Mallett and colleagues (2011), who incur multiple and repeated negative consequences because of their drinking. Our investigation suggests that it is not only students who exhibit this dangerous behavior; therefore, intervening only on college campuses may not be sufficient to disrupt the downward trajectories of most of these individuals. We also found no relationship with income, suggesting that Whites with the most severe drinking patterns were not the most or least affluent. In fact, if low-income Whites were as likely to avoid heavy drinking as Blacks, we might conclude that lack of disposable income explains the relatively protected position of Blacks with regard to heavy drinking. However, we did not find that to be the case.
Several early family factors appear to be important for young adults of both races. Chief among them is parental monitoring, which has also been shown to be a strong predictor of young adult drinking in variable-centered research. In our study, monitoring differentiated among different drinking patterns, whether defined by HED or drunkenness, which suggests the robustness of this particular parenting practice. Consistent discipline also differentiated drinking groups of both races for HED, and parental norms differentiated groups for drunkenness. It is possible that different family dynamics serve to prevent different types of drinking behavior. For instance, strict parental norms may focus on the dangers and unacceptability of losing control, and therefore deter youth from getting drunk (or reporting that they get drunk). On the other hand, discipline may be initiated upon discovering that the teen has already been drinking and focus on deterring any further drinking, thereby preventing HED. Future research on the mechanisms by which parenting practices during adolescence affect young adult drinking may elucidate whether different family factors influence different drinking behaviors and how.
Overall, these findings speak to the importance of adolescent family dynamics, frequently the targets of intervention, for young adult drinking. Several studies have shown that Black adolescents experience stricter parental norms for substance use, more discipline, and more intense monitoring of their behavior than do White adolescents (Catalano et al., 1992; Gillmore et al., 1990; Giordano et al., 1993; Peterson et al., 1994; Wallace and Muroff, 2002). Through these dynamics, Black families may be exerting positive influences on their children even after they leave the home. Of importance, these protective parenting behaviors may stem from perceived dangers associated with experiences outside the home (e.g., greater police involvement, greater difficulty recovering from alcohol-related consequences), which differ by race (Elder et al., 1995).
When drunkenness (as opposed to HED) was examined, interesting race differences in early factors were observed. For Whites, drunkenness was uniquely associated with low scores on the support dimension of parenting (attachment), whereas for Blacks it was more influenced by high levels of parental behavioral control (monitoring and discipline). These differences may signify that drunkenness in particular may constitute a distinct experience for Blacks and Whites. Further support for this difference may be evident among individuals in our study who reported frequent drunkenness, with Whites reporting getting drunk more often and experiencing more consequences than did their Black counterparts.
Several analyses pointed to ethnic identity processes in adolescence as potentially important contributors to HED in young adulthood. Exploration and affirmation differentiated between groups of heavy drinkers among youth of both races. Of note, more exploration and affirmation in 10th grade was associated with stopping drinking or not engaging in heavy drinking at all in young adulthood, indicating that in mid-adolescence both the process of considering or discovering one’s identity as well as feeling a sense of belonging are protective. Because ethnic identity is the only component of identity formation we considered, we cannot say whether it uniquely influences drinking or is an indicator of identity formation more generally. Such identity processes may be precursors of young adult identity consolidation and specifically the resolution of an adult identity, which are predictive of less heavy drinking (Schwartz et al., 2010).
Limitations
One weakness of this study is a relatively small sample size with reduced statistical power for finding moderate to weak effects. This issue may have been especially problematic for the post hoc analyses with single-race subsamples. For example, ethnic identity exploration and affirmation predicted group membership for the full-sample HED analyses but not for Blacks and Whites separately. On closer examination, however, similar patterns were observed in the subsamples. Second, the variability in the income of Black participants is more restricted than that of Whites: Black participants were almost exclusively low income, whereas White participants ranged from working class to upper middle class. Thus, the current analyses do not take into account very low-income Whites or middle- to high-income Blacks.
Future directions
As person-centered approaches in the study of alcohol consumption gain traction (e.g., Cleveland et al., 2013; Huh et al., 2013; Varvil-Weld et al., 2013), more research is needed to identify distinct subgroups of young adults at risk for dysfunctional drinking behaviors. As part of this effort, more attention must be paid to race and other differences that may signify different levels of risk, as well as potentially unique mechanisms by which to prevent heavy drinking. We recommend further exploration of family factors to better understand how different parenting behaviors may influence different aspects of drinking. Of importance, this study supports the need for parent- or family-based interventions, even in late adolescence, as a way to prevent heavy drinking during the peak of the early 20s. Programs that train parents in effective monitoring (based on open communication with adolescents), consistent and appropriate discipline, and strict norms against alcohol may be especially successful in deterring future heavy drinking.
Acknowledgments
The authors thank the Seattle School District for their collaboration in this study and the dedicated families who participated.
Footnotes
This study was supported by National Institute on Drug Abuse Grant #R01 DA021737 (to Kevin P. Haggerty, principal investigator). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funding agency.
References
- Alati R, Najman JM, Kinner SA, Mamun AA, Williams GM, O’Callaghan M, Bor W. Early predictors of adult drinking: A birth cohort study. American Journal of Epidemiology. 2005;162:1098–1107. doi: 10.1093/aje/kwi320. [DOI] [PubMed] [Google Scholar]
- Aldenderfer MS, Blashfield RK. Cluster analysis. Beverly Hills, CA: Sage; 1984. [Google Scholar]
- Aquilino WS, Supple AJ. Long-term effects of parenting practices during adolescence on well-being outcomes in young adulthood. Journal of Family Issues. 2001;22:289–308. [Google Scholar]
- Armsden GC, Greenberg MT. The Inventory of Parent and Peer Attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence. 1987;16:427–454. doi: 10.1007/BF02202939. [DOI] [PubMed] [Google Scholar]
- Arria AM, Kuhn V, Caldeira KM, O’Grady KE, Vincent KB, Wish ED. High school drinking mediates the relationship between parental monitoring and college drinking: A longitudinal analysis. Substance Abuse Treatment, Prevention, and Policy. 2008;3(6) doi: 10.1186/1747-597X-3-6. Retrieved from http://www.substanceabusepolicy.com/content/3/1/6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnes GM, Hoffman JH, Welte JW, Farrell MP, Dintcheff BA. Effects of parental monitoring and peer deviance on substance use and delinquency. Journal of Marriage and Family. 2006;68:1084–1104. [Google Scholar]
- Beckett K, Nyrop K, Pfingst L. Race, drugs, and policing: Understanding disparities in drug delivery arrests. Criminology. 2006;44:105–137. [Google Scholar]
- Brook JS, Pahl K. The protective role of ethnic and racial identity and aspects of an Africentric orientation against drug use among African American young adults. Journal of Genetic Psychology. 2005;166:329–345. doi: 10.3200/GNTP.166.3.329-345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brook JS, Whiteman M, Balka EB, Win PT, Gursen MD. Similar and different precursors to drug use and delinquency among African Americans and Puerto Ricans. Journal of Genetic Psychology. 1998;159:13–29. doi: 10.1080/00221329809596131. [DOI] [PubMed] [Google Scholar]
- Catalano RF, Morrison DM, Wells EA, Gillmore MR, Iritani B, Hawkins JD. Ethnic differences in family factors related to early drug initiation. Journal of Studies on Alcohol. 1992;53:208–217. doi: 10.15288/jsa.1992.53.208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chartier K, Caetano R. Ethnicity and health disparities in alcohol research. Alcohol Research & Health. 2010;33:152–160. [PMC free article] [PubMed] [Google Scholar]
- Chassin L, Flora DB, King KM. Trajectories of alcohol and drug use and dependence from adolescence to adulthood: The effects of familial alcoholism and personality. Journal of Abnormal Psychology. 2004;113:483–498. doi: 10.1037/0021-843X.113.4.483. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pitts SC, Prost J. Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: Predictors and substance abuse outcomes. Journal of Consulting and Clinical Psychology. 2002;70:67–78. [PubMed] [Google Scholar]
- Chen CM, Dufour MC, Yi HY. Alcohol consumption among young adults ages 18-24 in the United States: Results from the 2001-2002 NESARC survey. Alcohol Research & Health. 2004;28:269–280. [Google Scholar]
- Clarke N, Kim SY, White HR, Jiao Y, Mun EY. Associations between alcohol use and alcohol-related negative consequences among Black and White college men and women. Journal of Studies on Alcohol and Drugs. 2013;74:521–31. doi: 10.15288/jsad.2013.74.521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleveland MJ, Mallett KA, White HR, Turrisi R, Favero S. Patterns of alcohol use and related consequences in non-college-attending emerging adults. Journal of Studies on Alcohol and Drugs. 2013;74:84–93. doi: 10.15288/jsad.2013.74.84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courtney KE, Polich J. Binge drinking in young adults: Data, definitions, and determinants. Psychological Bulletin. 2009;135:142–156. doi: 10.1037/a0014414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elder GH, Jr, Eccles JS, Ardelt M, Lord S. Inner-city parents under economic pressure: Perspectives on the strategies of parenting. Journal of Marriage and Family. 1995;57:771–784. [Google Scholar]
- Galea S, Vlahov D. Social determinants and the health of drug users: Socioeconomic status, homelessness, and incarceration. Public Health Reports. 2002;117(Supplement 1):S135–S145. [PMC free article] [PubMed] [Google Scholar]
- Gary LE. Drinking, homicide, and the Black male. Journal of Black Studies. 1986;17:15–31. [Google Scholar]
- Gillmore MR, Catalano RF, Morrison DM, Wells EA, Iritani B, Hawkins JD. Racial differences in acceptability and availability of drugs and early initiation of substance use. American Journal of Drug and Alcohol Abuse. 1990;16:185–206. doi: 10.3109/00952999009001583. [DOI] [PubMed] [Google Scholar]
- Giordano PC, Cernkovich SA, DeMaris A. The family and peer relations of Black adolescents. Journal of Marriage and Family. 1993;55:277–287. [Google Scholar]
- Graham JW. Missing data: Analysis and design. New York, NY: Springer; 2012. [Google Scholar]
- Greenfield TK, Room R. Situational norms for drinking and drunkenness: Trends in the US adult population, 1979-1990. Addiction. 1997;92:33–47. [PubMed] [Google Scholar]
- Guo J, Hawkins JD, Hill KG, Abbott RD. Childhood and adolescent predictors of alcohol abuse and dependence in young adulthood. Journal of Studies on Alcohol. 2001;62:754–762. doi: 10.15288/jsa.2001.62.754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haggerty KP, Skinner ML, MacKenzie EP, Catalano RF. A randomized trial of Parents Who Care: Effects on key outcomes at 24-month follow-up. Prevention Science. 2007;8:249–260. doi: 10.1007/s11121-007-0077-2. [DOI] [PubMed] [Google Scholar]
- Harford TC, Muthén BO. Adolescent and young adult antisocial behavior and adult alcohol use disorders: A fourteen-year prospective follow-up in a national survey. Journal of Studies on Alcohol. 2000;61:524–528. doi: 10.15288/jsa.2000.61.524. [DOI] [PubMed] [Google Scholar]
- Hawkins DF, Laub JH, Lauritsen JL, Cothern L. Race, ethnicity, and serious and violent juvenile offending. Juvenile Justice Bulletin. 2000, June Retrieved from https://www.ncjrs.gov/html/ojjdp/2000_6_1/contents.html. [Google Scholar]
- Herd D. Migration, cultural transformation and the rise of Black liver cirrhosis mortality. British Journal of Addiction. 1985;80:397–410. doi: 10.1111/j.1360-0443.1985.tb03011.x. [DOI] [PubMed] [Google Scholar]
- Huh J, Huang Z, Liao Y, Pentz M, Chou CP. Transitional life events and trajectories of cigarette and alcohol use during emerging adulthood: Latent class analysis and growth mixture modeling. Journal of Studies on Alcohol and Drugs. 2013;74:727–735. doi: 10.15288/jsad.2013.74.727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humphrey JA, Stephens V, Allen DF. Race, sex, marihuana use and alcohol intoxication in college students. Journal of Studies on Alcohol. 1983;44:733–738. doi: 10.15288/jsa.1983.44.733. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Demographic subgroup trends among adolescents for fifty-one classes of licit and illicit drugs, 1975–2012 (Monitoring the Future Occasional Paper No. 79) Ann Arbor, MI: Institute for Social Research; 2013. Retrieved from http://www.monitoringthefuture.org/pubs/occpapers/mtf-occ79.pdf. [Google Scholar]
- Kandel DB. Drugs and drinking behavior among youth. Annual Review of Sociology. 1980;6:235–285. [Google Scholar]
- Kaufman L, Rousseeuw P. Finding groups in data. New York, NY: Wiley & Sons; 1990. [Google Scholar]
- King KM, Chassin L. A prospective study of the effects of age of initiation of alcohol and drug use on young adult substance dependence. Journal of Studies on Alcohol and Drugs. 2007;68:256–265. doi: 10.15288/jsad.2007.68.256. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Turner AP, Mallett KA, Geisner IM. Predicting drinking behavior and alcohol-related problems among fraternity and sorority members: Examining the role of descriptive and injunctive norms. Psychology of Addictive Behaviors. 2004;18:203–212. doi: 10.1037/0893-164X.18.3.203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Locke TF, Newcomb MD. Adolescent predictors of young adult and adult alcohol involvement and dysphoria in a prospective community sample of women. Prevention Science. 2004;5:151–168. doi: 10.1023/b:prev.0000037639.78352.3c. [DOI] [PubMed] [Google Scholar]
- Maggs JL, Frome PM, Eccles JS, Barber BL. Psychosocial resources, adolescent risk behaviour and young adult adjustment: Is risk taking more dangerous for some than others? Journal of Adolescence. 1997;20:103–119. doi: 10.1006/jado.1996.0067. [DOI] [PubMed] [Google Scholar]
- Mallett KA, Marzell M, Varvil-Weld L, Turrisi R, Guttman K, Abar C. One-time or repeat offenders? An examination of the patterns of alcohol-related consequences experienced by college students across the freshman year. Addictive Behaviors. 2011;36:508–511. doi: 10.1016/j.addbeh.2010.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason WA, Hitch JE, Kosterman R, McCarty CA, Herrenkohl TI, Hawkins JD. Growth in adolescent delinquency and alcohol use in relation to young adult crime, alcohol use disorders, and risky sex: A comparison of youth from low- versus middle-income backgrounds. Journal of Child Psychology and Psychiatry. 2010;51:1377–1385. doi: 10.1111/j.1469-7610.2010.02292.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merline A, Jager J, Schulenberg JE. Adolescent risk factors for adult alcohol use and abuse: Stability and change of predictive value across early and middle adulthood. Addiction, 103, Supplement. 2008;1:84–99. doi: 10.1111/j.1360-0443.2008.02178.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Midanik LT. Drunkenness, feeling the effects and 5+ measures. Addiction. 1999;94:887–897. doi: 10.1046/j.1360-0443.1999.94688711.x. [DOI] [PubMed] [Google Scholar]
- Mooi E, Sarstedt M. A concise guide to market research: The process, data and methods using IBM SPSS statistics. Berlin, Germany: Springer; 2011. [Google Scholar]
- Oesterle S, Hill KG, Hawkins JD, Guo J, Catalano RF, Abbott RD. Adolescent heavy episodic drinking trajectories and health in young adulthood. Journal of Studies on Alcohol. 2004;65:204–212. doi: 10.15288/jsa.2004.65.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson PL, Hawkins JD, Abbott RD, Catalano RF. Disentangling the effects of parental drinking, family management, and parental alcohol norms on current drinking by Black and White adolescents. Journal of Research on Adolescence. 1994;4:203–227. [Google Scholar]
- Presley CA. Alcohol and drugs on American college campuses: Use, consequences, and perceptions of the campus environment: Volume III: 1991-93. Carbondale, IL: Southern Illinois University; 1996. [Google Scholar]
- Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. The Lancet. 2009;373:2223–2233. doi: 10.1016/S0140-6736(09)60746-7. [DOI] [PubMed] [Google Scholar]
- Roberts RE, Phinney JS, Masse LC, Chen YR, Roberts CR, Romero A. The structure of ethnic identity of young adolescents from diverse ethnocultural groups. Journal of Early Adolescence. 1999;19:301–322. [Google Scholar]
- Roche KM, Ahmed S, Blum RW. Enduring consequences of parenting for risk behaviors from adolescence into early adulthood. Social Science and Medicine. 2008;66:2023–2034. doi: 10.1016/j.socscimed.2008.01.009. [DOI] [PubMed] [Google Scholar]
- Rostosky SS, Danner F, Riggle EDB. Is religiosity a protective factor against substance use in young adulthood? Only if you’re straight! Journal of Adolescent Health. 2007;40:440–447. doi: 10.1016/j.jadohealth.2006.11.144. [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Forthun LF, Ravert RD, Zamboanga BL, Umaña-Taylor AJ, Filton BJ, Hudson M. Identity consolidation and health risk behaviors in college students. American Journal of Health Behavior. 2010;34:214–224. [PMC free article] [PubMed] [Google Scholar]
- SPSS, Inc. The SPSS TwoStep Cluster Component: A scalable component enabling more efficient customer segmentation [Technical Report] Chicago, IL: Author; 2001. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Results from the 2011 National Survey on Drug Use and Health (Summary of National Findings, NSDUH Series H-44, HHS Publication No. [SMA] 12–4713) Rockville, MD: Author; 2012a. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Table 2.44B—Alcohol Use, Binge Alcohol Use, and Heavy Alcohol Use in the Past Month among Persons Aged 18 to 25, by Demographic Characteristics: Percentages, 2010 and 2011. Results from the 2011 National Survey on Drug Use and Health (Summary of National Findings, NSDUH Series H-44, HHS Publication No. [SMA] 12–4713) 2012b. Retrieved from http://www.samhsa.gov/data/NSDUH/2011SummNatFindDetTables/NSDUH-DetTabsPDFWHTML2011/2k11DetailedTabs/Web/HTML/NSDUH-DetTabsSect2peTabs43to84-2011.htm#Tab2.44B. [Google Scholar]
- Turner AP, Larimer ME, Sarason IG. Family risk factors for alcohol-related consequences and poor adjustment in fraternity and sorority members: Exploring the role of parent-child conflict. Journal of Studies on Alcohol. 2000;61:818–826. doi: 10.15288/jsa.2000.61.818. [DOI] [PubMed] [Google Scholar]
- Varvil-Weld L, Mallett KA, Turrisi R, Abar CC. Using parental profiles to predict membership in a subset of college students experiencing excessive alcohol consequences: Findings from a longitudinal study. Journal of Studies on Alcohol and Drugs. 2012;73:434–443. doi: 10.15288/jsad.2012.73.434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varvil-Weld L, Mallett KA, Turrisi R, Cleveland MJ, Abar CC. Are certain college students prone to experiencing excessive alcohol-related consequences? Predicting membership in a high-risk subgroup using pre-college profiles. Journal of Studies on Alcohol and Drugs. 2013;74:542–551. doi: 10.15288/jsad.2013.74.542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voas RB, Torres P, Romano E, Lacey JH. Alcohol-related risk of driver fatalities: An update using 2007 data. Journal of Studies on Alcohol and Drugs. 2012;73:341–350. doi: 10.15288/jsad.2012.73.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace JM., Jr Explaining race differences in adolescent and young adult drug use: The role of racialized social systems. Drugs & Society. 1998;14:21–36. [Google Scholar]
- Wallace JM, Jr, Brown TN, Bachman JG, Laveist TA. The influence of race and religion on abstinence from alcohol, cigarettes and marijuana among adolescents. Journal of Studies on Alcohol. 2003a;64:843–848. doi: 10.15288/jsa.2003.64.843. [DOI] [PubMed] [Google Scholar]
- Wallace JM, Jr, Brown TN, Bachman JG, Laveist TA. Religion, race, and abstinence from drug use among American adolescents (Monitoring the Future Occasional Paper No. 58) Ann Arbor, MI: Institute for Social Research; 2003b. [Google Scholar]
- Wallace JM, Jr, Muroff JR. Preventing substance abuse among African American children and youth: Race differences in risk factor exposure and vulnerability. Journal of Primary Prevention. 2002;22:235–261. [Google Scholar]
- Wechsler H, Dowdall GW, Davenport A, Rimm EB. A gender-specific measure of binge drinking among college students. American Journal of Public Health. 1995;85:982–985. doi: 10.2105/ajph.85.7.982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White HR. Longitudinal stability and dimensional structure of problem drinking in adolescence. Journal of Studies on Alcohol. 1987;48:541–550. doi: 10.15288/jsa.1987.48.541. [DOI] [PubMed] [Google Scholar]
- White HR, Fleming CB, Kim MJ, Catalano RF, McMorris BJ. Identifying two potential mechanisms for changes in alcohol use among college-attending and non-college-attending emerging adults. Developmental Psychology. 2008;44:1625–1639. doi: 10.1037/a0013855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- White HR, McMorris BJ, Catalano RF, Fleming CB, Haggerty KP, Abbott RD. Increases in alcohol and marijuana use during the transition out of high school into emerging adulthood: The effects of leaving home, going to college, and high school protective factors. Journal of Studies on Alcohol. 2006;67:810–822. doi: 10.15288/jsa.2006.67.810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiesner M, Kim HK, Capaldi DM. Developmental trajectories of offending: Validation and prediction to young adult alcohol use, drug use, and depressive symptoms. Development and Psychopathology. 2005;17:251–270. doi: 10.1017/s0954579405050133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Windle M, Mun EY, Windle RC. Adolescent-to-young adulthood heavy drinking trajectories and their prospective predictors. Journal of Studies on Alcohol. 2005;66:313–322. doi: 10.15288/jsa.2005.66.313. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Switzerland. Author; 2011. Global status report on alcohol and health. Geneva. Retrieved from http://www.who.int/substance_abuse/publications/global_alcohol_report/en. [Google Scholar]
- Zucker RA. Anticipating problem alcohol use developmentally from childhood into middle adulthood: What have we learned? Addiction, 103, Supplement. 2008;1:100–108. doi: 10.1111/j.1360-0443.2008.02179.x. [DOI] [PMC free article] [PubMed] [Google Scholar]